Which Surgical Hand Preparation Method Is More Effective? A Comparative Study of Hand Rub and Hand Scrub


Abstract
1. Introduction
2. Materials and Methods
2.1. Design and Setting
2.2. Population
2.3. Sample Size Calculation
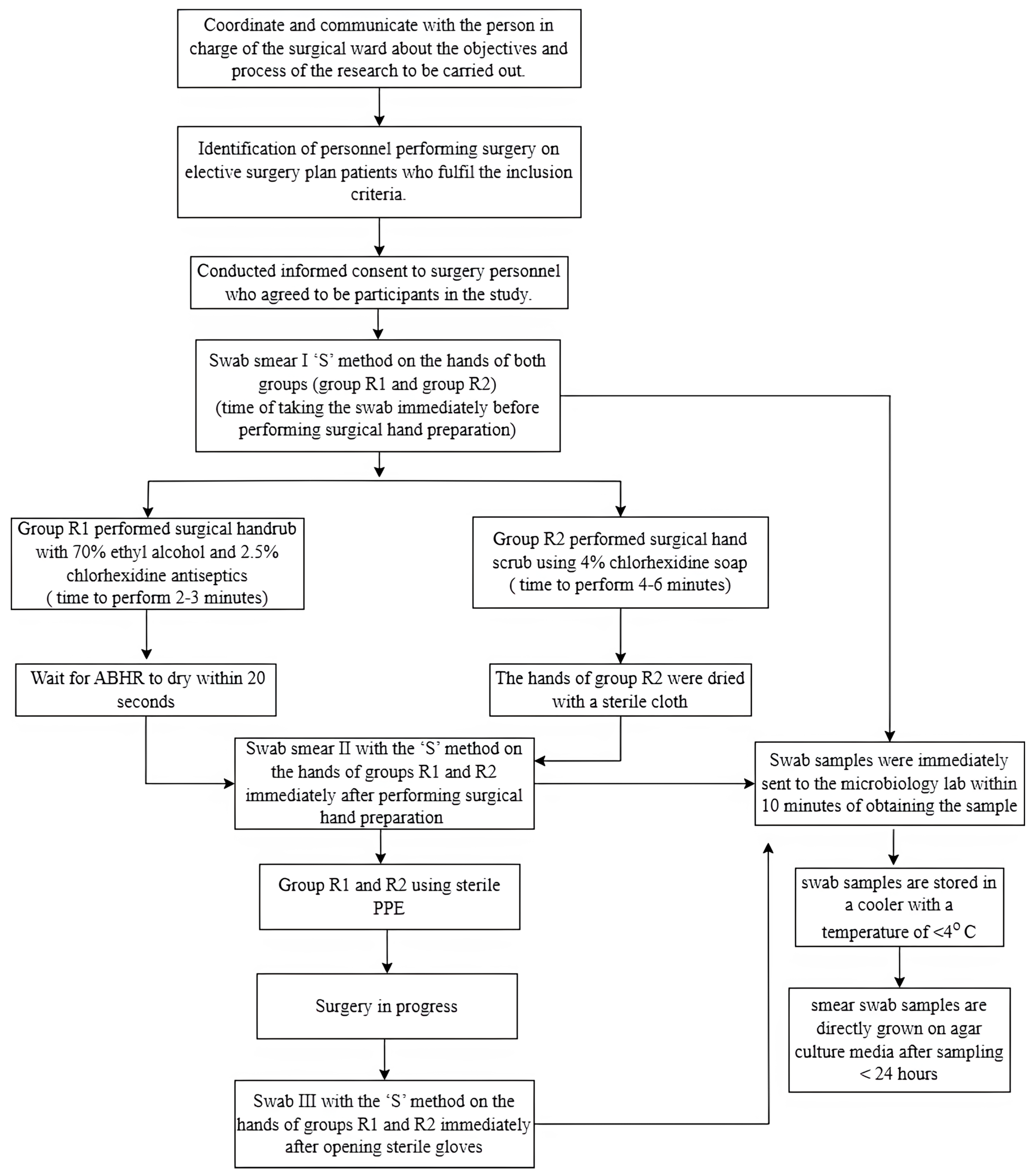
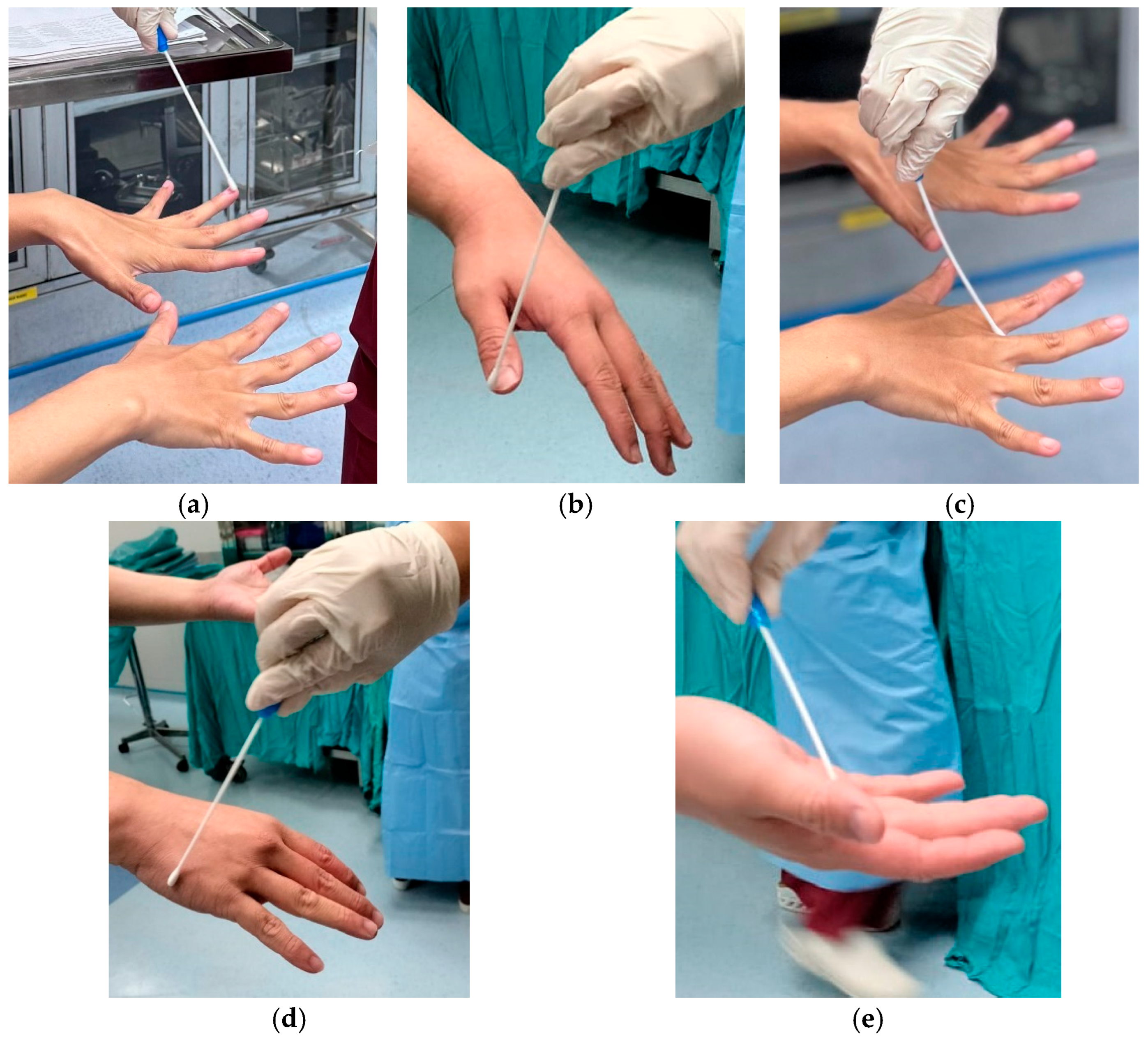
2.4. Data Collection
2.5. Data Analysis
2.6. Ethical Considerations
3. Results
3.1. Demographic Characteristics and Surgery
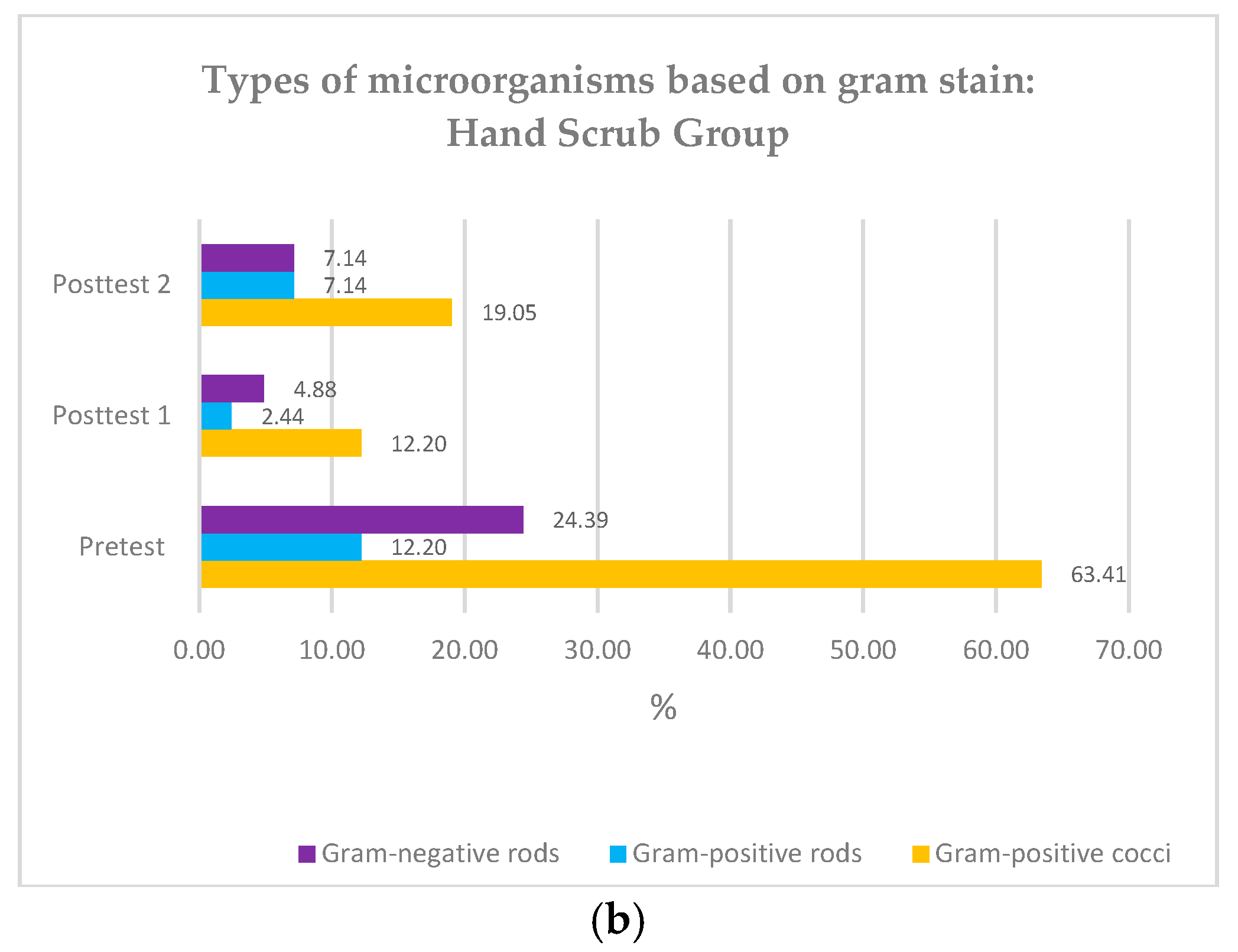
3.2. Types of Microorganisms Based on Gram Stain
3.3. Bacteria Colony Count in Surgical Hand Scrub and Surgical Hand Rub Groups
3.4. Comparison of the Difference in Bacterial Colonies of the Surgical Hand Scrub and Surgical Hand Rub Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
Guidelines and Standards Statement
Use of Artificial Intelligence
Acknowledgments
Conflicts of Interest
References
- National Collaborating Centre for Women’s and Children’s Health. Surgical Site Infection: Prevention and Treatment of Surgical Site Infection; RCOG Press: London, UK, 2020. [Google Scholar]
- Birhanu, A.; Amare, H.H.; Girma, T.; Tadesse, M.; Assefa, D.G. Magnitude of surgical site infection and determinant factors among postoperative patients, A cross sectional study. Ann. Med. Surg. 2022, 83, 104324. [Google Scholar] [CrossRef]
- Maraş, G.; Sürme, Y. Surgical Site Infections: Prevalence, Economic Burden, and New Preventive Recommendations. Explor. Res. Hypothesis Med. 2023, 8, 366–371. [Google Scholar] [CrossRef]
- Badia, J.M.; Casey, A.L.; Petrosillo, N.; Hudson, P.M.; Mitchell, S.A.; Crosby, C. Impact of surgical site infection on healthcare costs and patient outcomes: A systematic review in six European countries. J. Hosp. Infect. 2017, 96, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Gidey, K.; Gidey, M.T.; Hailu, B.Y.; Gebreamlak, Z.B.; Niriayo, Y.L. Clinical and economic burden of healthcare-associated infections: A prospective cohort study. PLoS ONE 2023, 18, e0282141. [Google Scholar] [CrossRef] [PubMed]
- Spagnolo, A.M.; Ottria, G.; Amicizia, D.; Perdelli, F.; Cristina, M.L. Operating theatre quality and prevention of surgical site infections. J. Prev. Med. Hyg. 2013, 54, 131–137. [Google Scholar]
- WHO. Surgical Site Infection Prevention Guidelines; Web Appendix 10. Guidelines; WHO: Geneva, Switzerland, 2016; pp. 1–18.
- Nthumba, P.M. Effective Hand Preparation for Surgical Procedures in Low- and Middle-Income Countries. Surg. Infect. 2020, 21, 495–500. [Google Scholar] [CrossRef]
- Allegranzi, B.; Pittet, D. Role of hand hygiene in healthcare-associated infection prevention. J. Hosp. Infect. 2009, 73, 305–315. [Google Scholar] [CrossRef]
- Singh, A.; Barnard, T.G. Health Science Students’ Perceptions of Hand Hygiene Education and Practice in a South African University: Introducing the University Hand Hygiene Improvement Model. Healthcare 2023, 11, 2553. [Google Scholar] [CrossRef]
- Soria, E.H.; Alou, L.; Martin-Villa, C.; Becerro-de-Bengoa-Vallejo, R.; Losa-Iglesias, M.; Sevillano, D. Alcohol-Based Chlorhexidine and Potassium Sorbate Rub Strengthens the Effectiveness of Traditional Hand scrubbing and Improves Long-Lasting Effectiveness—Evaluation of Hand Preparation Protocols According to EN 12791. Antibiotics 2024, 13, 470. [Google Scholar]
- WHO. Guidelines on Hand Hygiene in Health Care First Global Patient Safety Challenge Clean Care is Safer Care; WHO: Geneva, Switzerland, 2009.
- Asia Pacific Society of Infection Control. Pedoman APSIC Untuk Pencegahan Infeksi Daerah Operasi; Asia Pacific Society of Infection Control: Kuala Lumpur, Malaysia, 2018; pp. 1–58. [Google Scholar]
- Gaspar, G.G.; Menegueti, M.G.; Lopes, A.E.R.; Santos, R.O.C.; de Araújo, T.R.; Nassiff, A.; Ferreira, L.R.; Dallora, M.E.L.V.; Canini, S.R.M.S.; Bellissimo-Rodrigues, F. Alcohol-based surgical hand preparation: Translating scientific evidence into clinical practice. Antimicrob. Resist. Infect. Control 2018, 7, 80. [Google Scholar] [CrossRef]
- Shen, N.J.; Pan, S.C.; Sheng, W.H.; Tien, K.L.; Chen, M.L.; Chang, S.C.; Chen, Y.-C. Comparative antimicrobial efficacy of alcohol-based hand rub and conventional surgical scrub in a medical center. J. Microbiol. Immunol. Infect. 2015, 48, 322–328. [Google Scholar] [CrossRef] [PubMed]
- Brookes, Z.L.S.; Bescos, R.; Belfield, L.A.; Ali, K.; Roberts, A. Current uses of chlorhexidine for management of oral disease: A narrative review. J. Dent. 2020, 103, 103497. [Google Scholar] [CrossRef] [PubMed]
- Maeda, N.; Mori, N.; Shinjoh, M.; Komiyama, O.; Takahashi, T. Comparison of 0.5% chlorhexidine gluconate alcohol with 10% povidone-iodine for skin disinfection in children to prevent blood culture contamination. J. Infect. Chemother. 2021, 27, 1027–1032. [Google Scholar] [CrossRef]
- Feng, W.; Lin, S.; Huang, D.; Huang, J.; Chen, L.; Wu, W.; Hu, S.; Wei, Z.; Wang, X. Surgical hand rubbing versus surgical hand scrubbing: Systematic review and meta-analysis of efficacy. Injury 2020, 51, 1250–1257. [Google Scholar] [CrossRef]
- Gasson, S.; Solari, F.; Jesudason, E.P. Sustainable Hand Surgery: Incorporating Water Efficiency Into Clinical Practice. Cureus 2023, 15, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Mastracci, J.C.; Bonvillain, K.W.; Gaston, R.G. Surgical Hand Antisepsis: Environmental and Cost Impact in Hand Surgery. J. Hand Surg. 2024, 49, 923–926. [Google Scholar] [CrossRef]
- Iwakiri, K.; Kobayashi, A.; Seki, M.; Ando, Y.; Tsujio, T.; Hoshino, M.; Nakamura, H. Waterless Hand Rub Versus Traditional Hand scrub Methods for Preventing the Surgical Site Infection in Orthopedic Surgery. Spine 2017, 42, 1675–1679. [Google Scholar] [CrossRef]
- Martin-Villa, C.; Becerro-De-Bengoa-Vallejo, R.; Alou, L.; González, N.; Losa-Iglesias, M.; Gómez-Lus, M.L.; Sevillano, D. Comparing rubbing and scrubbing surgical hand antisepsis with propan-1-ol 60% in accordance with European regulation UNE-EN 12791:2016+A1:2018. Infect. Control Hosp. Epidemiol. 2021, 42, 1382–1384. [Google Scholar] [CrossRef]
- Santé, L.; Gómez-Lus, M.L.; Martin-Villa, C.; Becerro-De-Bengoa-Vallejo, R.; Alou, L.; Sevillano, D. Effect on the reduction of bacterial load after surgical hand antisepsis with triclosan 0.5% compared to triclosan 0.5% followed by 70% alcoholic solution. Infect. Control Hosp. Epidemiol. 2023, 44, 517–519. [Google Scholar] [CrossRef]
- de Bengoa Vallejo, R.B.; Fernandez, D.S.; Cervera, L.A.; Aragón, L.M.; Iglesias, M.E.L.; Yurrita, L.R.C.; Lopez, D.L. Effectiveness of surgical hand antisepsis using chlorhexidine digluconate and parachlorometaxylenol hand scrub: Cross-over trial. Medicine 2018, 97, e12831. [Google Scholar] [CrossRef]
- Akita, S.; Fujioka, M.; Akita, T.; Tanaka, J.; Masunaga, A.; Kawahara, T. Effects of Hand Hygiene Using 4% Chlorhexidine Gluconate or Natural Soap during Hand Rubbing Followed by Alcohol-Based 1% Chlorhexidine Gluconate Sanitizer Lotion in the Operating Room. Adv. Wound Care 2022, 11, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Akpokonyan, T.; Esan, O.; Ikem, I.; Ako-Nai, K.; Omo-Omorodion, B. Hand bacterial repopulation dynamics following two methods of surgical hand preparation during elective orthopedic surgeries. Niger. Med. J. 2020, 61, 241. [Google Scholar] [PubMed]
- Herruzo, R.; Vizcaino, M.J.; Yela, R. Surgical hand preparation with chlorhexidine soap or povidone iodine: New methods to increase immediate and residual effectiveness, and provide a safe alternative to alcohol solutions. J. Hosp. Infect. 2018, 98, 365–368. [Google Scholar] [CrossRef]
- Nieves, V.; Gundersen, T.; Mykkeltveit, I. The surgical team’s adherence to recommended guidelines for surgical hand preparation: A quantitative observation study. Sykepl. Forsk. 2024, 15, 123–130. [Google Scholar] [CrossRef]
- Sharif, B.O.; Edan, S.M.; Saeed, B.I.; Kaka, A.K. Evaluation of the Theater Staff Performance Regarding Surgical Hand scrub at Rania Teaching Hospital. Int. J. Med. Sci. Nurs. Res. 2022, 2, 18–24. [Google Scholar] [CrossRef]
- Hosseini, P.; Mundis, G.M.; Eastlack, R.; Nourian, A.; Pawelek, J.; Nguyen, S.; Akbarnia, B.A. Do Longer Surgical Procedures Result in Greater Contamination of Surgeons’ Hands? Clin. Orthop. Relat. Res. 2016, 474, 1707–1713. [Google Scholar] [CrossRef]
- Serra Neto, A.; Marques, S.G.; Bomfim, M.R.Q.; Monteiro, S.G.; de Souza, R.C.; Nunes, R.A. Microbiological Analysis of Surgeons’ Hands in a Public Hospital in São Luis, Maranhão State, Brazil: A Cross-Sectional Study. Microorganisms 2023, 11, 1895. [Google Scholar] [CrossRef]
- Gök, F. Surgical hand washing: A systematic review. Int. J. Antiseps. Disinfect. Steriliz. 2016, 1, 23–32. [Google Scholar] [CrossRef]
- Ho, Y.H.; Wang, Y.C.; Loh, E.W.; Tam, K.W. Antiseptic efficacies of waterless hand rub, chlorhexidine scrub, and povidone-iodine scrub in surgical settings: A meta-analysis of randomized controlled trials. J. Hosp. Infect. 2019, 101, 370–379. [Google Scholar] [CrossRef]
- Tsai, J.C.; Lin, Y.K.; Huang, Y.J.; Loh, E.W.; Wen, H.Y.; Wang, C.H.; Tsai, Y.-T.; Hsieh, W.-S.; Tam, K.-W. Antiseptic Effect of Conventional Povidone-Iodine Scrub, Chlorhexidine Scrub, and Waterless Hand Rub in a Surgical Room: A Randomized Controlled Trial. Infect. Control Hosp. Epidemiol. 2017, 38, 417–422. [Google Scholar] [CrossRef]
- CDC. Guideline for Disinfection and Sterilization in Healthcare Facilities: Updated 2017. Healthcare Infection Control Practices Advisory Committee. 2017. Available online: https://stacks.cdc.gov/view/cdc/47378 (accessed on 15 February 2017).
- Gold, N.A.; Avva, U. Alcohol Sanitizer; StatPearls: Tampa, FL, USA, 2018; pp. 1–8. [Google Scholar]
- Haque, M.; Sartelli, M.; McKimm, J.; Abu Bakar, M. Health care-associated infections—An overview. Infect. Drug Resist. 2018, 11, 2321–2333. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Surgical Hand Rub Group | Surgical Hand Scrub Group | p | |||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Participants Characteristics | |||||
| Working Experience | |||||
| 0–5 year | 1 | 2.9 | 1 | 2.8 | 0.026 |
| 6–10 year | 0 | 0 | 3 | 4.1 | |
| 11–15 year | 15 | 44.1 | 15 | 20.3 | |
| 16–20 year | 16 | 47.1 | 11 | 14.9 | |
| >20 year | 2 | 5.9 | 6 | 8.1 | |
| Mean | 13.46 ± 5.468 | 16.17 ± 6.474 | |||
| Age | |||||
| Mean (year) | 40.91 ± 5.711 | 39.19 ± 8.448 | 0.996 | ||
| Minimum (year) | 30 | 27 | |||
| Maximum (year) | 55 | 73 | |||
| Procedure Characteristic | |||||
| Duration of Surgery | |||||
| ≤60 min | 15 | 42.9 | 15 | 41.7 | 0.329 |
| 61–120 min | 11 | 31.4 | 10 | 27.8 | |
| ≥121 min | 9 | 25.7 | 11 | 30.6 | |
| Mean (SD) | 105 ± 67.47 | 113.75 ± 63.475 | |||
| Profession | |||||
| Nurse | 18 | 51.4 | 33 | 91.7 | 0.062 |
| Surgeon | 17 | 48.6 | 3 | 8.3 | |
| Type of Surgery | |||||
| Clean Surgery | 21 | 60 | 23 | 63.9 | 0.886 |
| Clean Contaminated Surgery | 14 | 40 | 13 | 36.1 | |
| Surgical Hand Rub Group (n = 33, %) | Surgical Hand Scrub Group (n = 41, %) | p (b) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Gram-positive cocci | Gram-positive rods | Gram-negative rods | Negative (−) | p (a) | Gram-positive cocci | Gram-positive rods | Gram-negative rods | Negative (−) | p (a) | ||
| Pre-test | 45.45 | 39.39 | 15.15 | 0 | 63.41 | 12.2 | 24.39 | 0 | 0.312 | ||
| Post-test1 | 3.03 | 3.03 | 0 | 93.94 | 0 | 12.2 | 2.44 | 4.88 | 80.49 | 0 | 0.104 |
| Post-test2 | 3.03 | 3.03 | 6.06 | 87.88 | 19.05 | 7.14 | 7.14 | 6.67 | 0.051 | ||
| Mean Rank | Mean (CFU/cm2) | SD | χ2 | p | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Surgical Hand Scrub Group | ||||||||||
| Pre-test | 2.89 | 0.202 | 0.295 | 53.397 | 0.00 | (pre-test vs. post-test 1: 0.00; pre-test vs. post-test 2: 0.00; post-test 1 vs. post-test 2: 0.218) | ||||
| Post-test 1 | 1.49 | 0.007 | 0.023 | |||||||
| Post-test 2 | 1.63 | 0.016 | 0.043 | |||||||
| Surgical Hand Rub Group | ||||||||||
| Pre-test | 2.81 | 0.163 | 0.218 | 53.109 | 0.00 | (pre-test vs. post-test 1: 0.00; pre-test vs. post-test 2: 0.00; post-test 1 vs. post-test 2: 0.317) | ||||
| Post-test 1 | 1.56 | 0.001 | 0.002 | |||||||
| Post-test 2 | 1.63 | 0.001 | 0.004 | |||||||
| Surgical Hand Scrub | Surgical Hand Rub | p-Value | |
|---|---|---|---|
| Delta 1 (pre-test and post-test 1) | 0.712 | ||
| Mean | 0.195 (0.295) | 0.162 (0.218) | |
| Std. Deviation | |||
| Delta 2 (pre-test and post-test 2) | 0.813 | ||
| Mean | 0.187 (0.284) | 0.162 (0.218) | |
| Std. Deviation | |||
| Delta 3 (post-test 1 and post-test 2) | 0.321 | ||
| Mean | −0.008 (0.046) | 0.000 (0.005) | |
| Std. Deviation |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olivia, C.; Ibrahim, K.; Kurniawan, T. Which Surgical Hand Preparation Method Is More Effective? A Comparative Study of Hand Rub and Hand Scrub. Nurs. Rep. 2025, 15, 242. https://doi.org/10.3390/nursrep15070242
Olivia C, Ibrahim K, Kurniawan T. Which Surgical Hand Preparation Method Is More Effective? A Comparative Study of Hand Rub and Hand Scrub. Nursing Reports. 2025; 15(7):242. https://doi.org/10.3390/nursrep15070242
Chicago/Turabian StyleOlivia, Claudia, Kusman Ibrahim, and Titis Kurniawan. 2025. "Which Surgical Hand Preparation Method Is More Effective? A Comparative Study of Hand Rub and Hand Scrub" Nursing Reports 15, no. 7: 242. https://doi.org/10.3390/nursrep15070242
APA StyleOlivia, C., Ibrahim, K., & Kurniawan, T. (2025). Which Surgical Hand Preparation Method Is More Effective? A Comparative Study of Hand Rub and Hand Scrub. Nursing Reports, 15(7), 242. https://doi.org/10.3390/nursrep15070242