
The Use of 360-Degree Video to Reduce Anxiety and Increase Confidence in Mental Health Nursing Students: A Mixed Methods Preliminary Study
Abstract
1. Introduction
1.1. Cognitive Reappraisal
1.2. VERA and Solution-Focused Strategies
1.3. Aims
- ○
- RQ1: What was the impact of VR as an educational tool and learning experience?
- ○
- RQ2: How did student mental health nurses perceive their abilities to develop a therapeutic nurse/client relationship in a stressful clinical situation?
- ○
- RQ3: Did working through a process of cognitive reappraisal and clinical supervision help students to envisage how they might cope better with a stressful interaction, in terms of increased confidence and reduced anxiety?
1.4. Study Design
2. Materials and Methods
2.1. Methods
2.2. Materials
- Scene 1: In a corridor, Mary is beginning to show signs of stress, asking to go home, and in frustration, she throws tea from a cup she is holding towards the viewer.
- Scene 2: Mary is seen crying in her bedroom and is clearly very distressed.
- Scene 3: Mary is showing frustration whilst interacting with two men in the dayroom.
2.3. Process
- ○
- RQ1: What was the impact of VR as an educational tool and learning experience?
- ○
- RQ2: How did student mental health nurses perceive their abilities to develop a therapeutic nurse/client relationship in a stressful clinical situation?
- ○
- In the video, the service user is talking to someone. In your view, who was that person?
- ○
- How did you feel whilst watching the scenario?
- ○
- How able were you to relate to the service user?
- ○
- How did you feel overall about the 360-degree video experience?
- ○
- RQ3: Did working through a process of cognitive reappraisal and clinical supervision help students to envisage how they might cope better with a stressful interaction, in terms of increased confidence and reduced anxiety?
- ○
- Identify emotions: as part of the process of cognitive reappraisal, each student was asked to describe their feelings after watching the scenario and rate the intensity of their emotional responses.
- ○
- Evaluate thoughts and rate how strongly they held these beliefs.
- ○
- Rate their levels of confidence and anxiety.
- ○
- What did you do then to successfully manage the situation?
- ○
- What did you say, keep in mind, feel, or remember that helped you solve the situation in a positive way?
2.4. Data Analyses
3. Results
3.1. Summary of Qualitative Findings
- Theme 1: strong presence effects/high levels of empathy;
- Theme 2: voyeuristic stance/strong emotional response but restricted agency;
- Theme 3: detached from distress/reduced emotions and agency;
- Theme 4: perceptions of risk.
- ‘I feel kind of sad that she was being neglected. That is person is supposed to be looking after me and is ignoring me. That is disrespectful, so I can’t get the best from that place. So, it makes me feel unhappy putting myself in that position…’
- ‘It’s like she weren’t being heard so even though she was directing it all at me I could… I felt the same at the same time’.
- ‘I wanted to intervene, but I wasn’t really sure. The woman was distressed, and I think she needed to talk to someone, or somebody needed to speak to her, but I couldn’t really communicate, and when I did there was no response back— one way traffic. Initially it was like…if I was to use to word strange or shocked, I couldn’t really…it was, Oh, what do I do? What do I say? What’s going on?’.
- ‘I still feel guilty, if I was, if that was a scenario like in real life, you know, I wouldn’t go over and see, I wouldn’t…Yes, it’s probably now I’m actually getting things out, it’s actually making me really disappointed’.
- ‘So, how intense were your feelings during the experience?’
- ‘Probably about a 5 maybe. I think because I’ve done it before, unfortunately I’ve probably seen it. So, to someone that hasn’t seen it, it would be more upsetting, wouldn’t it? Not that I’ve been desensitised to it, but yeah’.
- ‘What might happen? Hurt herself…hurt somebody else. She was trying to break through a door so she might have broken through the door or smashed a window…or upset one of the men that were in the room because, by the sounds of it, they weren’t very well either so she could have got hurt.’
- ‘Actually, when I was looking there and I saw the two guys, I was a bit distressed because I was thinking one is going to attack the other. So I was anticipating something bad might happen so that was distressing me more. And the last being distressed wasn’t as distressing as compared to when I was anticipating bad’.
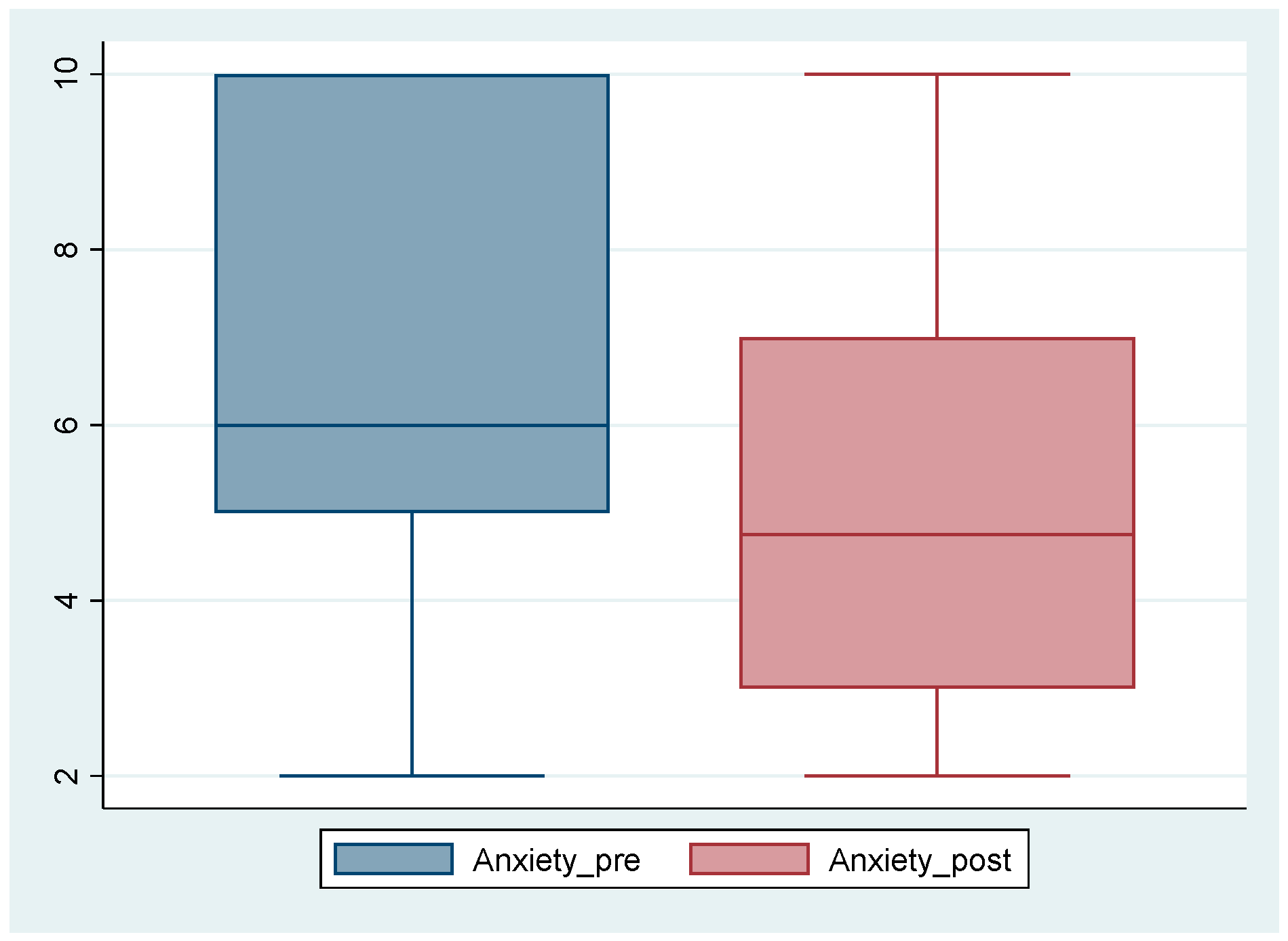
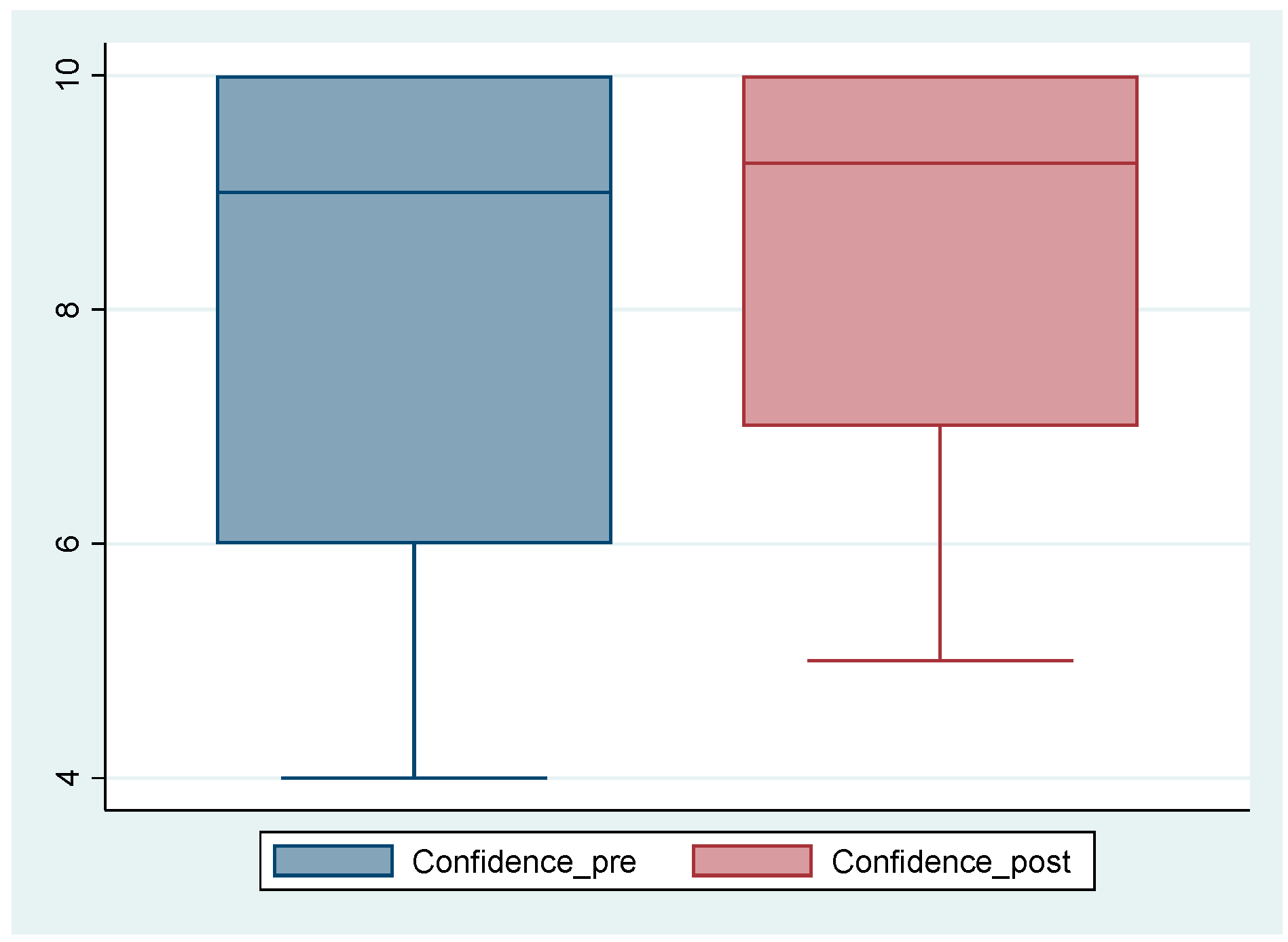
3.2. Clinical Supervision: Subgroup: Self-Reported Emotions and Thoughts and Ratings of Confidence and Anxiety Pre and Post Clinical Supervision
- ‘Yes, I was feeling anxious, because you know I couldn’t do anything. And if I could probably that would have reduced the anxiety and everything else. And probably at the beginning of it I just didn’t’ know what to expect, and I was just looking at these walls and these doors around me, I just didn’t know what was going to come out or what was going to happen. So that was a bit intense. It’s for Mary yeah, but especially when she was in the room, and she was really upset. And nobody bothered to actually go in there and find out what was going on. Why she was so distressed and upset. And the other thing is I feel really angry because the door she couldn’t get out of—that room—if she wanted to go for a walk or if she went to try to open the door, and the door was locked.
- ‘How anxious did you feel when viewing this situation on a scale of 0–10?’
- ‘I was very anxious because the first thing is, “Okay, who do I talk to? Who can help me?” I looked around. Then that’s when I asked, “Can you talk? Can you talk to us?’
- ‘To be honest I didn’t feel anxious, because I’ve seen worse. However, I think this lady in particular, she’s not causing a problem, so because I’ve seen worse, so I wasn’t anxious or anything. I just feel that maybe she was; maybe she was being neglected. She’s not young as well, I don’t know, because its very difficult you know. If she is always someone that’s seeking attention who [inaudible] or whatever she would do something, maybe I’d understand better and think, “Okay, this is the reason”. Maybe she would hurst somebody or slap somebody or whatever, but I don’t know that.”
4. Discussion
4.1. What Was the Impact of VR as an Educative Tool and Learning Experience?
4.2. How Did Student Mental Health Nurses Perceive Their Abilities to Develop a Nurse/Client Relationship in a Stressful Clinical Situation?
4.3. Strong Presence Effects/High Levels of Empathy
4.4. Voyeuristic Stance/Strong Emotional Response but Restricted Agency
4.5. Detached from Distress/Reduced Emotions and Agency
4.6. A Need for Increased Focus on Reducing Anxiety and Promoting Confidence, or a Wider Mental Health Concern?
4.7. Did Working Through a Process of Cognitive Reappraisal and Clinical Supervision Help Students to Imagine How to Cope Better with a Stressful Interaction, in Terms of Increased Confidence and Reduced Anxiety?
4.8. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
- Aim: in this study patient involvement was embedded and one service user contributed to some elements of the study design and process, as a valued member of the research team.
- Methods: The scenario depicting a distressed service user in a ward was conceptualized with the support of our service user colleague, who also acted in the role of the distressed service user, during the video. Following the creation of the video our service user colleague was invited to team meetings and contributed to discussions about the impact of the 360-degree video. Reported on page 4, Section 2.2. Materials.
- Study results: the 360-degree video was impactful. Reported on page 7, Section 3.1. Summary of Qualitative Findings.
- Discussion and conclusions: service user involvement in the design and development of the 360-degree video was essential to ensure an authentic experience for the student. Reported on page 11, Section 4.1. What Was the Impact of VR as an Educative Tool and Learning Experience?
- Reflections/critical perspective: as outlined above in discussion section [47].
Guidelines and Standards Statement
Use of Artificial Intelligence
Conflicts of Interest
References
- NHS Survey Coordination Centre. NHS Staff Surveys; NHS Coordination Centre: Oxford, UK, 2022. [Google Scholar]
- Aiken, L.H.; Sloane, D.M.; Ball, J.; Bruyneel, L.; Rafferty, A.M.; Griffiths, P. Patient satisfaction with hospital care and nurses in England: An observational study. BMJ Open 2018, 8, e019189. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Windle, G.; Bennet, K.M.; Noyes, J. A methodological review of resilience measurement scales. Health Qual. Life Outcomes 2011, 9, 8. [Google Scholar] [CrossRef]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal and Coping; Springer: New York, NY, USA, 2006. [Google Scholar]
- Maples-Keller, J.L.; Bunnell, B.E.; Kim, S.J.; Rothbaum, B.O. The Use of Virtual Reality Technology in the Treatment of Anxiety and Other Psychiatric Disorders. Harv. Rev. Psychiatry 2017, 25, 103–113. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bowman, D.A.; McMahan, R.P. Virtual Reality: How Much Immersion Is Enough? Computer 2007, 40, 36–43. [Google Scholar] [CrossRef]
- Jerdan, S.W.; Grindle, M.; van Woerden, H.C.; Kamel Boulos, M.N. Head-Mounted Virtual Reality and Mental Health: Critical Review of Current Research. JMIR Serious Games 2018, 6, e14. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gerber, S.M.; Jeitziner, M.M.; Wyss, P.; Chesham, A.; Urwyler, P.; Müri, R.M.; Jakob, S.M.; Nef, T. Visuo-acoustic stimulation that helps you to relax: A virtual reality setup for patients in the intensive care unit. Sci. Rep. 2017, 7, 13228. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kim, H.; Kim, D.J.; Kim, S.; Chung, W.H.; Park, K.A.; Kim, J.D.K.; Kim, D.; Kim, M.J.; Kim, K.; Jeon, H.J. Effect of Virtual Reality on Stress Reduction and Change of Physiological Parameters Including Heart Rate Variability in People with High Stress: An Open Randomized Crossover Trial. Front. Psychiatry 2021, 12, 614539. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Turton, W. Honing cognitive behaviour therapy skills through experiential learning. Ment. Health Pract. 2012, 15, 33. Available online: https://search.proquest.com/docview/1030130490 (accessed on 12 March 2021). [CrossRef]
- Beck, A.T. Cognitive Therapy: Nature and Relation to Behavior Therapy—Republished Article. Behav. Ther. 2016, 47, 776–784. [Google Scholar] [CrossRef] [PubMed]
- Barlow, D.H.; Farchione, T.J.; Bullis, J.R.; Gallagher, M.W.; Murray-Latin, H.; Sauer-Zavala, S.; Bentley, K.H.; Thompson-Hollands, J.; Conklin, L.R.; Boswell, J.F.; et al. The Unified Protocol for Transdiagnostic Treatment of Emotional Disorders Compared with Diagnosis-Specific Protocols for Anxiety Disorders: A Randomized Clinical Trial. JAMA Psychiatry 2017, 74, 875–884. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Einstein, D. Innovations and Advances in Cognitive Behaviour Therapy, 1st ed.; Australian Academic Press: Brisbane, Australia, 2008. [Google Scholar]
- Miu, A.; Crisan, L. Cognitive reappraisal reduces the susceptibility to the framing effect in economic decision making. Personal. Individ. Differ. 2011, 51, 478–482. [Google Scholar] [CrossRef]
- Bond, F.; Dryden, W. Handbook of Brief Cognitive Behaviour Therapy; John Wiley & Sons Ltd. Online: Hoboken, NJ, USA, 2002; ISBN 9780470713020. [Google Scholar] [CrossRef]
- Gross, J.J. Antecedent and response-focused emotion regulation: Divergent consequences for experience, expression, and psychology. J. Personal. Soc. Psychol. 1998, 74, 224–237. [Google Scholar] [CrossRef]
- Ochsner, K.N.; Bunge, S.A.; Gross, J.J.; Gabrielli, J.D.E. Rethinking feelings: An fMRI study of the cognitive regulation of emotion. J. Cogn. Neurosci. 2022, 14, 1215–1229. [Google Scholar] [CrossRef]
- Mauss, I.B.; Cook, C.L.; Cheng, J.Y.J.; Gross, J.J. Individual differences in cognitive reappraisal: Experiential and physiological responses to an anger provocation. Int. J. Psychophysiol. 2007, 66, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Gross, J.J.; John, O.P. Individual differences in two emotion regulation processes: Implications for affect, relationships and well-being. J. Personal. Soc. Psychol. 2003, 85, 348–362. [Google Scholar] [CrossRef] [PubMed]
- De Shazer, S. Putting Difference to Work; Norton: Tempe, AZ, USA, 1991. [Google Scholar]
- Hawkes, D. Solution Focused Therapy: A Handbook for Health Care Professionals; Butterworth-Heinemann: Oxford, UK, 1998. [Google Scholar]
- De Shazer, S.; Dolan, Y.; Korman, H.; McCollum, E.; Trepper, T.; Berg, I.K. More than Miracles: The State of the Art of Solution-Focused Brief Therapy; Haworth Press: Philadelphia, PA, USA, 2007. [Google Scholar]
- Hawkes, D. Heidegger undisclosed: Is Heidegger and phenomenology hiding or hidden from Solution Focus? Interact. J. Solut. Focus Organ. 2011, 3, 28–31. [Google Scholar]
- Ratner, H.; George, E.; Iveson, C. Solution Focused Brief Therapy; Routledge: London, UK, 2012. [Google Scholar]
- De Jong, P.; Berg, I.K. Interviewing for Solutions; Thomson Brooks/Cole Publishing, Co.: Monterey, CA, USA, 1998. [Google Scholar]
- Blackhall, A.; Hawkes, D.; Hingley, D.; Wood, S. VERA framework: Communicating with people who have dementia. Nurs. Stand. 2011, 26, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Hawkes, D.; Hingley, D.; Wood, S.; Blackhall, A. Evaluating the VERA framework for communication. Nurs. Stand. (RCN) 2015, 30, 44–48. [Google Scholar] [CrossRef]
- Laker, C.; Knight-Davidson, P.; Hawkes, D.; Driver, P.; Nightingale, M.; Winter, A.; McVicar, A. The Use of 360-Degree Video in Developing Emotional Coping Skills (Reduced Anxiety and Increased Confidence) in Mental Health Nursing Students: A Protocol Paper. Nurs. Rep. 2022, 12, 536–544. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Trivedi, P.; Wykes, T. From passive subjects to equal partners: Qualitative review of use involvement in research. Br. J. Psychiatry 2003, 181, 468–472. [Google Scholar] [CrossRef]
- Weng, H.; Fox, A.; Shackman, A.; Stodola, D.; Caldwell, J.; Olson, M.; Rogers, G.; Davidson, R. Compassion Training Alters Altrusim and Neural Responses to Suffering. Psychol. Sci. 2013, 24, 1171–1180. [Google Scholar] [CrossRef]
- Flick, U. An Introduction to Qualitative Research, 7th ed.; Freie Universtität: Berlin, Germany, 2023. [Google Scholar]
- Boyatzis, R. Transforming Qualitative Information: Thematic Analysis and Code Development; Sage: Thousand Oaks, CA, USA, 1998. [Google Scholar]
- Baxter, L.A. Content analysis. In Studying Interpersonal Interaction; Montgomery, B.M., Duck, S., Eds.; Guilford Press: New York, NY, USA, 1991; pp. 239–254. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Reflecting on reflexive thematic analysis. Qual. Res. Sport Exerc. Health 2019, 11, 589–597. [Google Scholar] [CrossRef]
- Chen, F.Q.; Leng, Y.F.; Ge, J.F.; Wang, D.W.; Li, C.; Chen, B.; Sun, Z.L. Effectiveness of Virtual Reality in Nursing Education: Meta-Analysis. J. Med. Internet Res. 2020, 22, e18290. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jicol, C.; Cheng, H.Y.; Petrini, K.; O’Neill, E. A predictive model for understanding the role of emotion for the formation of presence in virtual reality. PLoS ONE 2023, 18, e0280390. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- White, E.; Winstanley, J. Clinical supervision provided to mental health nurses in England. Br. J. Ment. Health Nurs. 2021, 10, 1–11. [Google Scholar] [CrossRef]
- Frijda, N.H. The laws of emotion. Am. Psychol. 1998, 43, 349. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, P.; Catarino, F.; Duarte, C.; Matos, M.; Kolts, R.; Stubbs, J.; Ceresatto, L.; Duarte, J.; Pinto-Gouveia, J.; Basran, J. The development of compassionate engagement and action scales for self and others. J. Compassionate Health Care 2017, 4, 4. [Google Scholar] [CrossRef]
- Klimecki, O.; Singer, T. Empathic distress fatigue rather than compassion fatigue? Integrating findings from empathy research in psychology and social neuroscience. In Pathological Altruism; Oakley, B., Knafo, A., Madhavan, G., Wilson, D.S., Eds.; Oxford University Press: Oxford, UK, 2012; pp. 368–383. [Google Scholar]
- Laker, C.; Rose, D.; Flach, C.; Csipke, E.; McCrone, P.; Craig, T.; Kelland, H.; Wykes, T. Views of the Therapeutic Environment (VOTE): Stakeholder involvement in measuring staff perceptions of acute in-patient care. Int. J. Nurs. Stud. 2012, 49, 1403–1410. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Menzies Lyth, I. Agency, Health and Social Survival: The Ecopolitics of Rival Psychologies; Taylor and Francis: London, UK, 1998. [Google Scholar]
- Rose, D.; Evans, E.; Laker, C.; Wykes, T. Life in acute mental health settings: Experiences and perceptions of service users and nurses. Epidemiol. Psychiatr. Sci. 2015, 24, 90–96. [Google Scholar] [CrossRef]
- Ford, M. Nursing Times survey reveals state of nurses’ mental health one year into pandemic. Nurs. Times 2021, 117, 6–7. [Google Scholar]
- Bakker, E.J.M.; Kox, J.H.A.M.; Boot, C.R.L.; Francke, A.L.; van der Beek, A.J.; Roelofs, P.D.D.M. Improving mental health of student and novice nurses to prevent dropout: A systematic review. J. Adv. Nurs. 2020, 76, 2494–2509. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Staniszewska, S.; Brett, J.; Simera, I.; Seers, K.; Mockford, C.; Goodlad, S.; Altman, D.G.; Moher, D.; Barber, R.; Denegri, S.; et al. GRIPP2 reporting checklists: Tools to improve reporting of patient and public involvement in research. BMJ 2017, 358, j3453. [Google Scholar] [CrossRef]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for Reporting Qualitative Research: A Synthesis of Recommendations. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Sample Data | Whole Group | Subgroup | |
|---|---|---|---|
| N 1 | 21 | 11 | |
| Gender | Male | 9 | 4 |
| Female | 12 | 7 | |
| Age | Ranges from | 21–63 | 30–56 |
| Ethnicity | Black African | 14 | 9 |
| White British | 5 | 2 | |
| Black British | 1 | 0 | |
|
Participants (N = 11) | How Anxious Were You on a Scale of 1–10? | |
|---|---|---|
| During the 360-Degree Video | After the Clinical Supervision | |
| 1 | 10 | 9 |
| 2 | 7 | Missing data |
| 3 | 2 | 3 |
| 4 | 6 | 6 |
| 5 | 10 | 10 |
| 6 | 3 | 2 |
| 7 | 5 | 4.5 |
| 8 | 9 | 3 |
| 9 | 6 | 4 |
| 10 | 5 | 5 |
| 11 | 10 | 7 |
| Participants (Intervention Group N = 11) | How Confident Were You on a Scale of 1–10? | |
|---|---|---|
| During the 360-Degree Video | After the Clinical Supervision Intervention | |
| 1 | 10 | 10 |
| 2 | 6 | No data |
| 3 | 10 | 7 |
| 4 | 6 | 7 |
| 5 | 10 | 10 |
| 6 | 4 | 5 |
| 7 | 9.5 | 9.5 |
| 8 | 8 | 9 |
| 9 | 9 | 10 |
| 10 | 8 | 8 |
| 11 | 10 | 10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laker, C.; Knight-Davidson, P.; McVicar, A. The Use of 360-Degree Video to Reduce Anxiety and Increase Confidence in Mental Health Nursing Students: A Mixed Methods Preliminary Study. Nurs. Rep. 2025, 15, 157. https://doi.org/10.3390/nursrep15050157
Laker C, Knight-Davidson P, McVicar A. The Use of 360-Degree Video to Reduce Anxiety and Increase Confidence in Mental Health Nursing Students: A Mixed Methods Preliminary Study. Nursing Reports. 2025; 15(5):157. https://doi.org/10.3390/nursrep15050157
Chicago/Turabian StyleLaker, Caroline, Pamela Knight-Davidson, and Andrew McVicar. 2025. "The Use of 360-Degree Video to Reduce Anxiety and Increase Confidence in Mental Health Nursing Students: A Mixed Methods Preliminary Study" Nursing Reports 15, no. 5: 157. https://doi.org/10.3390/nursrep15050157
APA StyleLaker, C., Knight-Davidson, P., & McVicar, A. (2025). The Use of 360-Degree Video to Reduce Anxiety and Increase Confidence in Mental Health Nursing Students: A Mixed Methods Preliminary Study. Nursing Reports, 15(5), 157. https://doi.org/10.3390/nursrep15050157