

Comparative Effectiveness of Active and Reactive Mattresses in Pressure Injury Healing for Older People in Their Own Homes: A Pragmatic Equivalence Randomised-Controlled Study



Abstract
1. Introduction
Research Questions
- Is a reactive mattress equivalent to an active mattress in healing an existing pressure injury when used in the domiciliary setting?
- What is the acceptability of different mattresses to users in a domiciliary setting
2. Materials and Methods
2.1. Participants
2.2. Intervention
2.3. Outcomes
2.4. Sample
2.5. Statistical Analysis
2.6. Trial Registration and Ethics
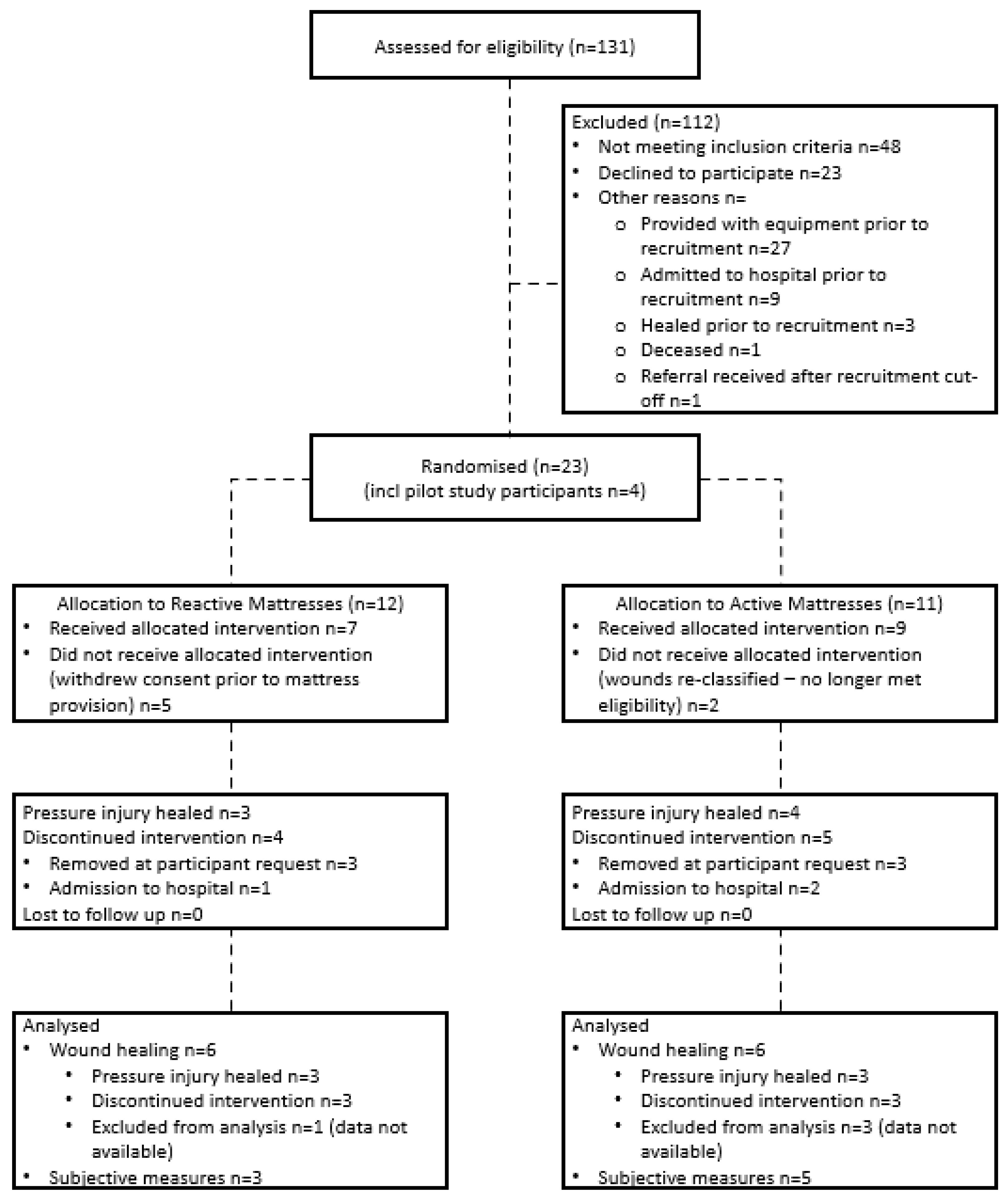
3. Results
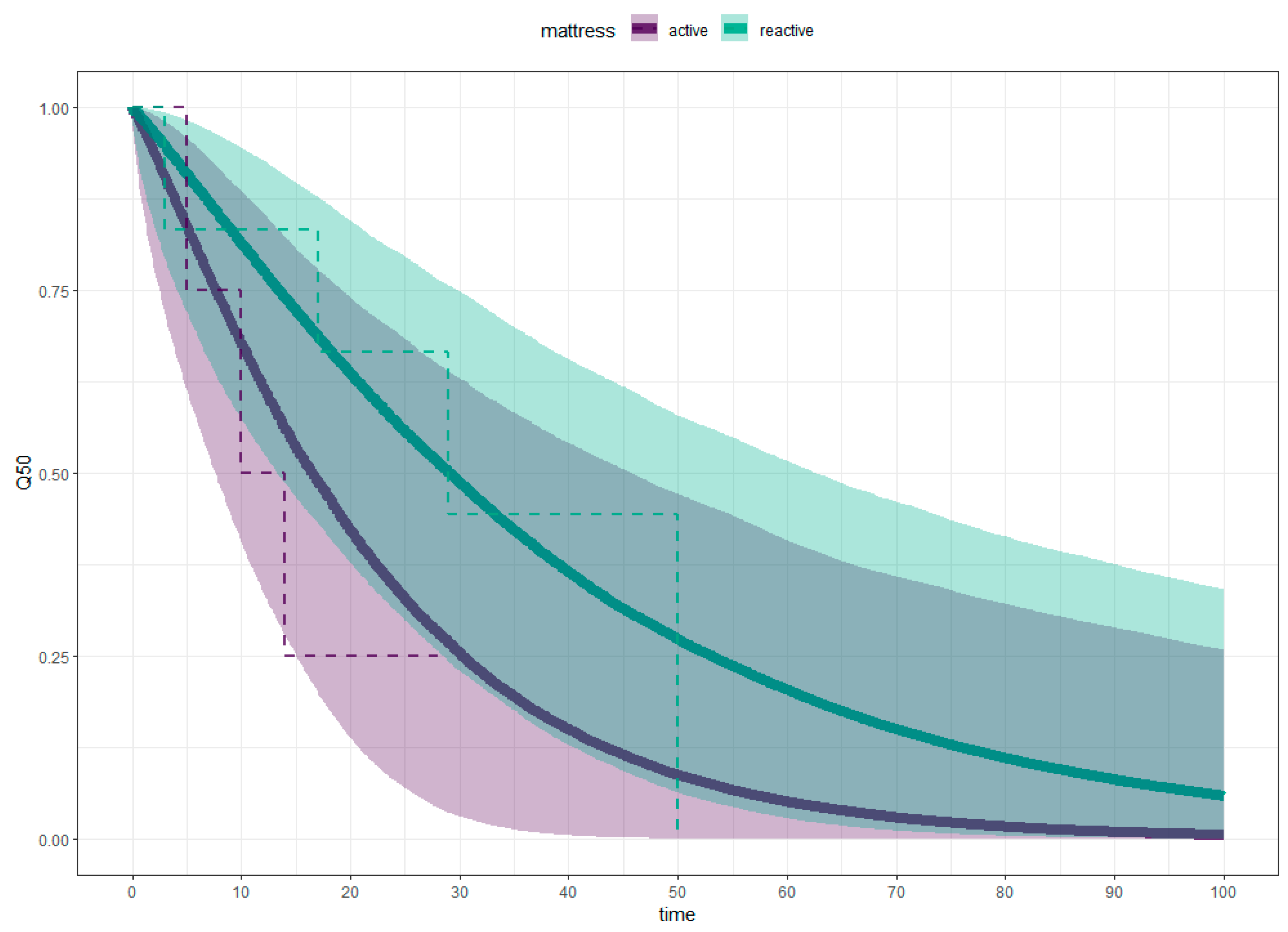
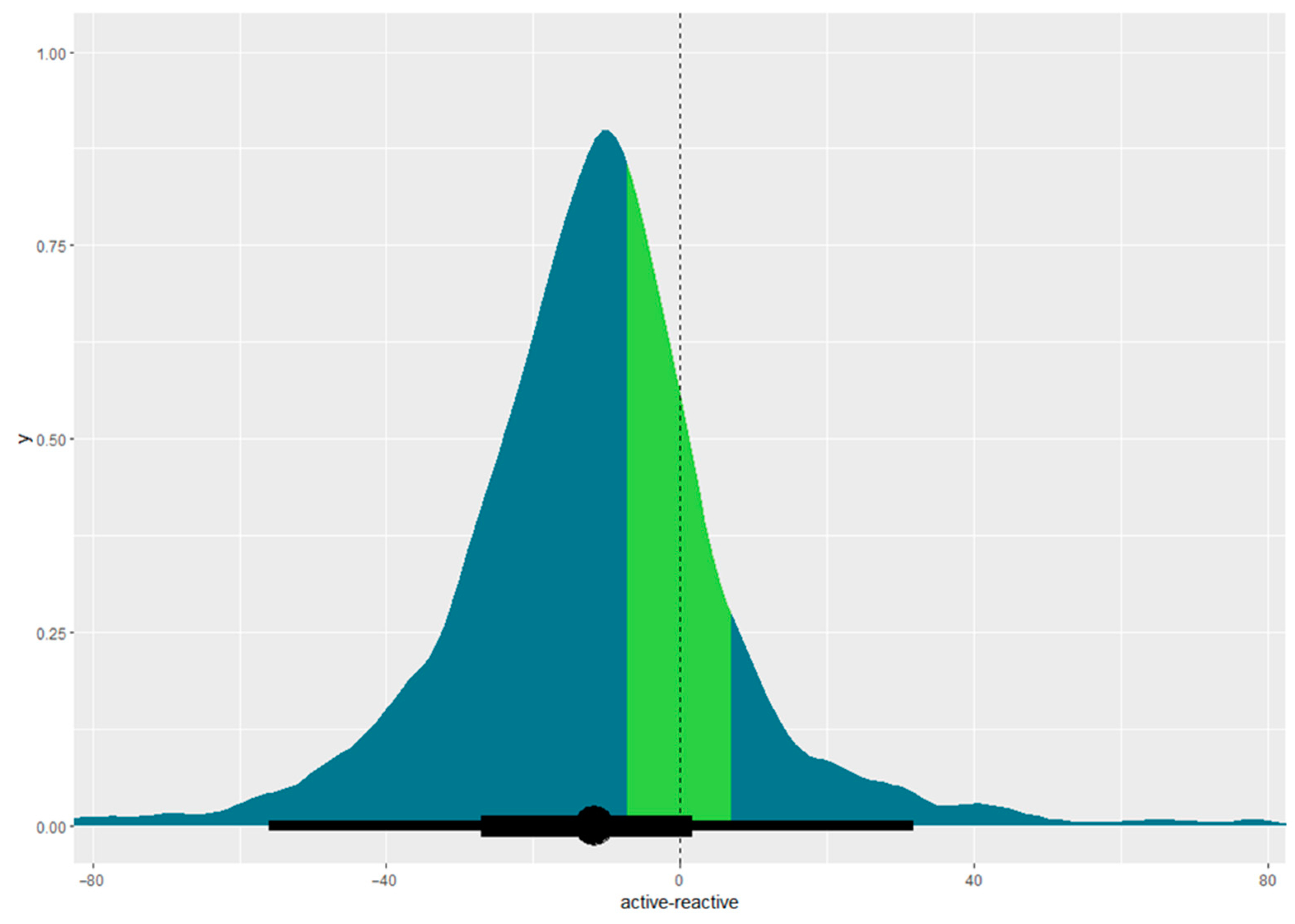
3.1. Comparative Mattress Effectiveness for Pressure Injury Healing
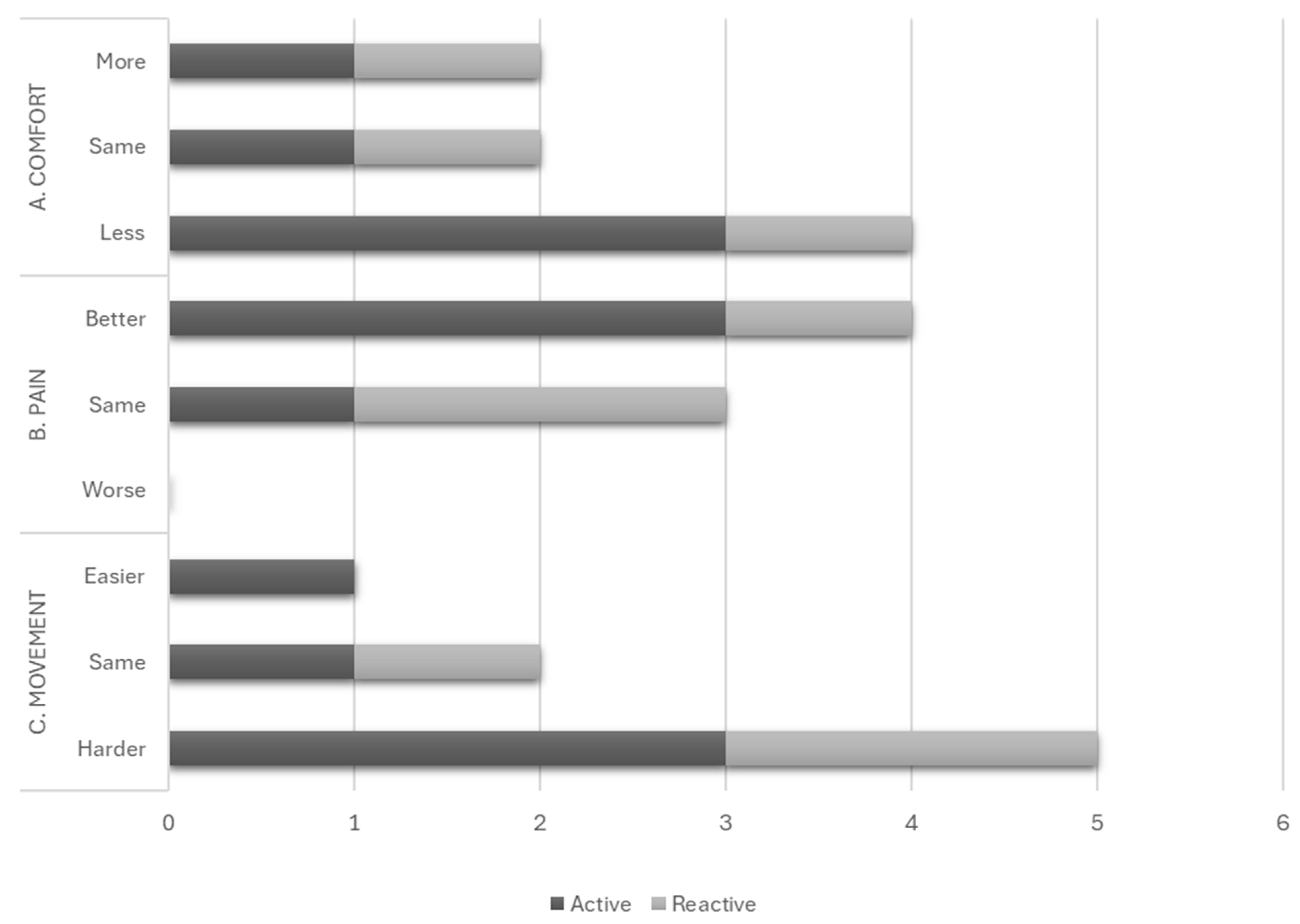
3.2. Comparative Mattress Effectiveness for User Acceptability
“The sound of the pump woke me frequently … When the changes in the pressure inside the mattress happened, there were noises that woke me.”(Participant X4)
“It takes up too much room on our double bed, making hardly any room for my husband”(Participant 16)
“I found it cold to sleep on, so put a sheepskin and blanket on top.”(Participant 2P)
4. Discussion
4.1. Equivalence of Mattress Types
4.2. User Acceptability
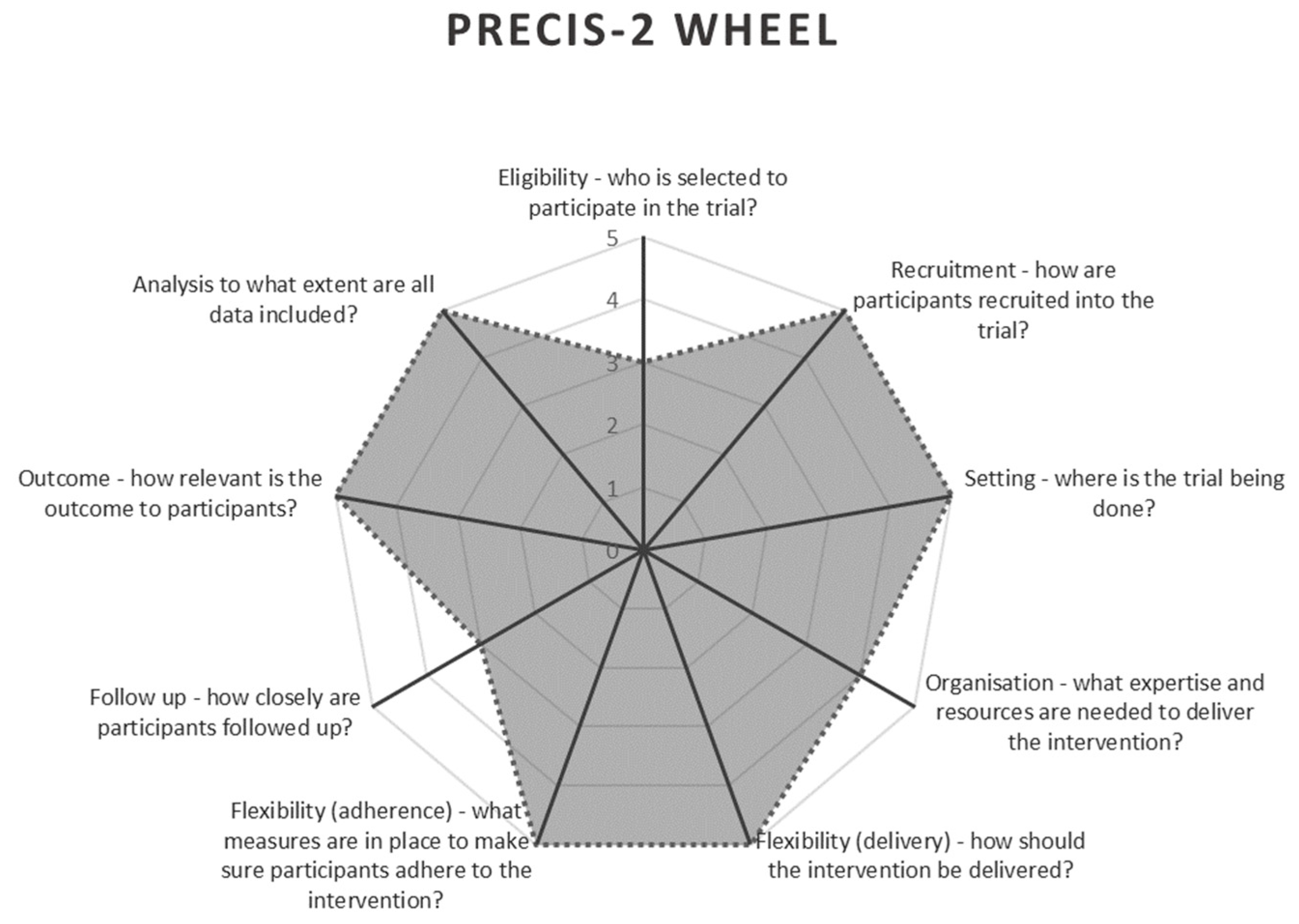
4.3. Pragmatic Considerations
4.3.1. Practice Context
4.3.2. Recruitment
4.3.3. Data Collection
4.3.4. Data Analysis
4.4. Limitations
4.5. Recommendations for Future Research
- Aligning study protocols with clinical practice is crucial for maintaining adherence, especially when competing priorities exist [29,63]. “Trials that are embedded in routine care and require limited additional activities pose fewer barriers for health care professionals and patients to participate” [6], p. 177. For example, if infrared technology for early identification of pressure injuries is not standard at the study site, its inclusion could hinder protocol adherence and limit transferability to settings without such technology.
- Consider data collection by treating clinician or research team. While data collection by research teams improves protocol adherence, it is resource-intensive, particularly when operating over multiple research sites [6]. Conversely, clinician-led data collection is more time-efficient; however, it may have lower adherence due to competing care priorities and less familiarity with the protocol [6]. Balancing these factors is essential for pragmatic studies in complex health care systems [6]. The degree of variation from the clinical practice of the settings can guide decision on who should collect data.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
Guidelines and Standards Statement
Use of Artificial Intelligence
Acknowledgments
Conflicts of Interest
References
- Glasgow, R.E. What does it mean to be pragmatic? Pragmatic methods, measures, and models to facilitate research translation. Health Educ. Behav. 2013, 40, 257–265. [Google Scholar] [CrossRef]
- Eckardt, P.; Erlanger, A.E. Lessons learned in methods and analyses for pragmatic studies. Nurs. Outlook 2018, 66, 446–454. [Google Scholar] [CrossRef]
- Kanzler, K.E.; McGeary, D.D.; McGeary, C.; Blankenship, A.E.; Young-McCaughan, S.; Peterson, A.L.; Buhrer, J.C.; Cobos, B.A.; Dobmeyer, A.C.; Hunter, C.L.; et al. Conducting a Pragmatic Trial in Integrated Primary Care: Key Decision Points and Considerations. J. Clin. Psychol. Med. Settings 2022, 29, 185–194. [Google Scholar] [CrossRef] [PubMed]
- Zuidgeest, M.G.P.; Goetz, I.; Groenwold, R.H.H.; Irving, E.; van Thiel, G.J.M.W.; Grobbee, D.E. Series: Pragmatic trials and real world evidence: Paper 1. Introduction. J. Clin. Epidemiol. 2017, 88, 7–13. [Google Scholar] [CrossRef]
- Bothwell, L.E.; Greene, J.A.; Podolsky, S.H.; Jones, D.S. Assessing the Gold Standard—Lessons from the History of RCTs. N. Engl. J. Med. 2016, 374, 2175–2181. [Google Scholar] [CrossRef] [PubMed]
- Rengerink, K.O.; Kalkman, S.; Collier, S.; Ciaglia, A.; Worsley, S.D.; Lightbourne, A.; Eckert, L.; Groenwold, R.H.H.; Grobbee, D.E.; Irving, E.A. Series: Pragmatic trials and real world evidence: Paper 3. Patient selection challenges and consequences. J. Clin. Epidemiol. 2017, 89, 173–180. [Google Scholar] [CrossRef]
- European Pressure Ulcer Advisory Panel; National Pressure Injury Advisory Panel; Pan Pacific Pressure Injury Alliance. Prevention and Treatment of Pressure Ulcers/Injuries: Clinical Practice Guideline. The International Guideline; Haesler, E., Ed.; EPUAP/NPIAP/PPPIA: Helsinki, Finland, 2019. Available online: https://static1.squarespace.com/static/6479484083027f25a6246fcb/t/6553d3440e18d57a550c4e7e/1699992399539/CPG2019edition-digital-Nov2023version.pdf (accessed on 28 December 2024).
- Fernando-Canavan, L.; Gust, A.; Hsueh, A.; Tran-Duy, A.; Kirk, M.; Brooks, P.; Knight, J. Measuring the economic impact of hospital-acquired complications on an acute health service. Aust. Health Rev. 2021, 45, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Demarré, L.; Van Lancker, A.; Van Hecke, A.; Verhaeghe, S.; Grypdonck, M.; Lemey, J.; Annemans, L.; Beeckman, D. The cost of prevention and treatment of pressure ulcers: A systematic review. Int. J. Nurs. Stud. 2015, 52, 1754–1774. [Google Scholar] [CrossRef]
- Padula, W.V.; Delarmente, B.A. The national cost of hospital-acquired pressure injuries in the United States. Int. Wound J. 2019, 16, 634–640. [Google Scholar] [CrossRef]
- Rodgers, K.; Sim, J.; Clifton, R. Systematic review of pressure injury prevalence in Australian and New Zealand hospitals. Collegian 2021, 28, 310–323. [Google Scholar] [CrossRef]
- Zhang, C.; Cai, E.; Qi, X.; Ge, X.; Xiang, Y.; Wang, J.; Li, Y.; Lv, L.; Zheng, H.; Qian, Y.; et al. Immunomodulatory gallium/glycyrrhizic acid hydrogels for treating multidrug-resistant Pseudomonas aeruginosa-infected pressure ulcers. Chem. Eng. J. 2024, 487, 150756. [Google Scholar] [CrossRef]
- Nghiem, S.; Campbell, J.; Walker, R.M.; Byrnes, J.; Chaboyer, W. Pressure injuries in Australian public hospitals: A cost of illness study. Int. J. Nurs. Stud. 2022, 130, 104191. [Google Scholar] [CrossRef]
- Australian Commission on Safety and Quality in Health Care. National Safety and Quality Health Service Standards, 2nd ed.; Australian Commission on Safety and Quality in Health Care: Sydney, Australia, 2021. [Google Scholar]
- Gefen, A.; Brienza, D.M.; Cuddigan, J.; Haesler, E.; Kottner, J. Our contemporary understanding of the aetiology of pressure ulcers/pressure injuries. Int. Wound J. 2022, 19, 692–704. [Google Scholar] [CrossRef]
- Gefen, A.; Soppi, E. What is new in our understanding of pressure injuries: The inextricable association between sustained tissue deformations and pain and the role of the support surface. Wound Pract. Res. 2020, 28, 58–65. [Google Scholar] [CrossRef]
- Rae, K.E.; Isbel, S.; Upton, D. Support surfaces for the treatment and prevention of pressure ulcers: A systematic literature review. J. Wound Care 2018, 27, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Beeckman, D.; Serraes, B.; Anrys, C.; Van Tiggelen, H.; Van Hecke, A.; Verhaeghe, S. A multicentre prospective randomised controlled clinical trial comparing the effectiveness and cost of a static air mattress and alternating air pressure mattress to prevent pressure ulcers in nursing home residents. Int. J. Nurs. Stud. 2019, 97, 105–113. [Google Scholar] [CrossRef]
- Nixon, J.; Cranny, G.; Iglesias, C.; Nelson, E.A.; Hawkins, K.; Phillips, A.; Torgerson, D.; Mason, S.; Cullum, N. Randomised, controlled trial of alternating pressure mattresses compared with alternating pressure overlays for the prevention of pressure ulcers: PRESSURE (pressure relieving support surfaces) trial. Br. Med. J. 2006, 332, 1413–1415. [Google Scholar] [CrossRef] [PubMed]
- Corbett, L.Q.; Funk, M.; Fortunato, G.; O’Sulllivan, D.M. Pressure injury in a community population: A descriptive study. J. Wound Ostomy Cont. Nurs. 2017, 44, 221–227. [Google Scholar] [CrossRef]
- Lumbers, M. Challenges in wound care for community nurses: A case review. Br. J. Community Nurs. 2019, 24, S25–S27. [Google Scholar] [CrossRef]
- Aloweni, F.; Gunasegaran, N.; Lim, S.H.; ZXin Leow, B.W.; Agus, N.; Qi Goh, I.H.; Ang, S.Y. Socio-economic and environmental factors associated with community-acquired pressure injuries: A mixed method study. J. Tissue Viability 2024, 33, 27–42. [Google Scholar] [CrossRef]
- Fletcher, J.; Tite, M.; Clark, M. Real-world evidence from a large-scale multisite evaluation of a hybrid mattress. Wounds UK 2016, 12, 54–61. [Google Scholar]
- Federici, S.; Borsci, S. The Use and Non-Use of Assistive Technology in Italy: Preliminary Data; Assistive Technology Research Series; IOS Press: Amsterdam, The Netherlands, 2011; Volume 29, pp. 979–986. [Google Scholar]
- Loudon, K.; Treweek, S.; Sullivan, F.; Donnan, P.; Thorpe, K.E.; Zwarenstein, M. The PRECIS-2 tool: Designing trials that are fit for purpose. BMJ Br. Med. J. 2015, 350, h2147. [Google Scholar] [CrossRef] [PubMed]
- Walker, E.; Nowacki, A.S. Understanding equivalence and noninferiority testing. J. Gen. Intern. Med. 2010, 26, 192–196. [Google Scholar] [CrossRef]
- Zuidgeest, M.G.P.; Welsing, P.M.J.; van Thiel, G.J.M.W.; Ciaglia, A.; Alfonso-Cristancho, R.; Eckert, L.; Eijkemans, M.J.C.; Egger, M. Series: Pragmatic trials and real world evidence: Paper 5. Usual care and real life comparators. J. Clin. Epidemiol. 2017, 90, 92–98. [Google Scholar] [CrossRef]
- Bond, J.; Atkinson, A.; Gregson, B.A.; Newell, D.J. Pragmatic and explanatory trials in the evaluation of the experimental National Health Service nursing homes. Age Ageing 1989, 18, 89–95. [Google Scholar] [CrossRef]
- Worsley, S.D.; Rengerink, K.O.; Irving, E.; Lejeune, S.; Mol, K.; Collier, S.; Groenwold, R.H.H.; Enters-Weijnen, C.; Egger, M.; Rhodes, T. Series: Pragmatic trials and real world evidence: Paper 2. Setting, sites, and investigator selection. J. Clin. Epidemiol. 2017, 88, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Lake, I. ACT Health and Calvary Health Care ACT: Pressure Injury Prevalence Survey 2015; ACT Health: Canberra, Australia, 2015. [Google Scholar]
- Nixon, J.; Brown, S.; Smith, I.L.; McGinnis, E.; Vargas-Palacios, A.; Nelson, E.A.; Brown, J.; Coleman, S.; Collier, H.; Fernandez, C.; et al. Comparing alternating pressure mattresses and high-specification foam mattresses to prevent pressure ulcers in high-risk patients: The PRESSURE 2 RCT. Health Technol. Assess. 2019, 23, 1–176. [Google Scholar] [CrossRef]
- Alderden, J.; Zhao, Y.; Zhang, Y.; Thomas, D.; Butcher, R.; Zhang, Y.; Cummins, M.R. Outcomes Associated with Stage 1 Pressure Injuries: A Retrospective Cohort Study. Am. J. Crit. Care 2018, 27, 471–476. [Google Scholar] [CrossRef] [PubMed]
- Brealey, G.; James, E.; Hay, K. Pressure cushions in a home environment: How effective are they at reducing interface pressure and does chair surface count? A pilot study. Wound Pract. Res. 2017, 25, 180–187. [Google Scholar]
- Shi, C.; Dumville, J.C.; Cullum, N.; Rhodes, S.; Jammali-Blasi, A.; Ramsden, V.; McInnes, E. Beds, overlays and mattresses for treating pressure ulcers. Cochrane Database Syst. Rev. 2021, CD013624. [Google Scholar] [CrossRef]
- Smet, S.; Probst, S.; Holloway, S.; Fourie, A.; Beele, H.; Beeckman, D. The measurement properties of assessment tools for chronic wounds: A systematic review. Int. J. Nurs. Stud. 2021, 121, 103998. [Google Scholar] [CrossRef] [PubMed]
- Thompson, N.; Gordey, L.; Bowles, H.; Parslow, N.; Houghton, P. Reliability and validity of the Revised Photographic Wound Assessment Tool on digital images taken of various types of chronic wounds. Adv. Ski. Wound Care 2013, 26, 360–373. [Google Scholar] [CrossRef] [PubMed]
- Waterlow, J. Pressure sores: A risk assessment card. Nurs. Times 1985, 81, 49–55. [Google Scholar]
- Field, A. Discovering Statistics Using IBM SPSS Statistics, 4th ed.; SAGE: London, UK, 2013. [Google Scholar]
- Welsing, P.M.; Rengerink, K.O.; Collier, S.; Eckert, L.; van Smeden, M.; Ciaglia, A.; Nachbaur, G.; Trelle, S.; Taylor, A.J.; Egger, M.; et al. Series: Pragmatic trials and real world evidence: Paper 6. Outcome measures in the real world. J. Clin. Epidemiol. 2017, 90, 99–107. [Google Scholar] [CrossRef]
- Cumming, G. The new statistics: Why and how. Psychol. Sci. 2014, 25, 7–29. [Google Scholar] [CrossRef]
- Kruschke, J.K.; Liddell, T.M. The Bayesian New Statistics: Hypothesis testing, estimation, meta-analysis, and power analysis from a Bayesian perspective. Psychon. Bull. Rev. 2018, 25, 178–206. [Google Scholar] [CrossRef]
- Kruschke, J.K. Doing Bayesian Data Analysis: A Tutorial with R, JAGS, and Stan, 2nd ed.; Elsevier: Amsterdam, The Netherlands, 2015. [Google Scholar]
- Greene, C.J.; Morland, L.A.; Durkalski, V.L.; Frueh, B.C. Noninferiority and equivalence designs: Issues and implications for mental health research. J. Trauma. Stress 2008, 21, 433–439. [Google Scholar] [CrossRef]
- Tripepi, G.; Chesnaye, N.C.; Dekker, F.W.; Zoccali, C.; Jager, K.J. Intention to treat and per protocol analysis in clinical trials. Nephrology 2020, 25, 513–517. [Google Scholar] [CrossRef] [PubMed]
- Rae, K.E.; Barker, J.; Isbel, S.; Upton, D. A pilot study comparing the effectiveness of active and reactive mattresses in pressure injury healing in a domiciliary setting. J. Wound Care 2024, 33, S13–S18. [Google Scholar] [CrossRef]
- Holtrop, J.S.; Glasgow, R.E. Pragmatic research: An introduction for clinical practitioners. Fam. Pract. 2020, 37, 424–428. [Google Scholar] [CrossRef]
- Shi, C.; Dumville, J.C.; Cullum, N.; Rhodes, S.; Jammali-Blasi, A.; McInnes, E. Alternating pressure (active) air surfaces for preventing pressure ulcers. Cochrane Database Syst. Rev. 2021, 2021, CD013620. [Google Scholar] [CrossRef]
- Shi, C.; Dumville, J.C.; Cullum, N.; Rhodes, S.; Leung, V.; McInnes, E. Reactive air surfaces for preventing pressure ulcers. Cochrane Database Syst. Rev. 2021, CD013622. [Google Scholar] [CrossRef]
- Lesaffre, E. Superiority, equivalence, and non-inferiority trials. Bull. NYU Hosp. Jt. Dis. 2008, 66, 150–154. [Google Scholar] [PubMed]
- Kruschke, J.K.; Liddell, T.M. Bayesian data analysis for newcomers. Psychon. Bull. Rev. 2018, 25, 155–177. [Google Scholar] [CrossRef] [PubMed]
- Ledger, L.; Worsley, P.; Hope, J.; Schoonhoven, L. Patient involvement in pressure ulcer prevention and adherence to prevention strategies: An integrative review. Int. J. Nurs. Stud. 2020, 101, 103449. [Google Scholar] [CrossRef]
- Foster, N.; Little, P. Methodological issues in pragmatic trials of complex interventions in primary care. Br. J. Gen. Pract. 2012, 62, 10–11. [Google Scholar] [CrossRef]
- Pawson, R. The “pragmatic trial”: An essentially contested concept? J. Eval. Clin. Pract. 2019, 25, 943–954. [Google Scholar] [CrossRef]
- Meinecke, A.-K.; Welsing, P.; Kafatos, G.; Burke, D.; Trelle, S.; Kubin, M.; Nachbaur, G.; Egger, M.; Zuidgeest, M. Series: Pragmatic trials and real world evidence: Paper 8. Data collection and management. J. Clin. Epidemiol. 2017, 91, 13–22. [Google Scholar] [CrossRef]
- London Group of the National Back Exchange. Moving and handling strategy—Standards for handling people and objects in health and social care. In Section G Specialist and Unusual Situations; London Group of the National Back Exchange: London, UK, 2013. [Google Scholar]
- Beyene, R.T.; Derryberry, S.L., Jr.; Barbul, A. The Effect of Comorbidities on Wound Healing. Surg. Clin. N. Am. 2020, 100, 695–705. [Google Scholar] [CrossRef]
- Baumgarten, M.; Margolis, D.J.; Selekof, J.L.; Moye, N.; Jones, P.S.; Shardell, M. Validity of pressure ulcer diagnosis using digital photography. Wound Repair Regen. 2009, 17, 287–290. [Google Scholar] [CrossRef]
- McGinnis, E.; Brown, S.; Collier, H.; Faulks, P.; Gilberts, R.; Greenwood, C.; Henderson, V.; Muir, D.; Nelson, A.; Nixon, J.; et al. Pressure relieving support surfaces: A randomised evaluation 2 (PRESSURE 2) photographic validation sub-study: Study protocol for a randomised controlled trial. Trials 2017, 18, 132. [Google Scholar] [CrossRef] [PubMed]
- Houghton, P.E.; Kincaid, C.B.; Campbell, K.E.; Woodbury, M.G.; Keast, D.H. Photographic assessment of the appearance of chronic pressure and leg ulcers. Ostomy Wound Manag. 2000, 46, 20–30. [Google Scholar]
- Peternelli, L.A.; Tomaz, F.S.C.; Bernardes, D.P.; da Silva, G.F.; Lacerda, F.G. An alternative method for assessing the equivalence among treatments in survival analysis. Ciência Rural 2013, 43, 1553–1560. [Google Scholar] [CrossRef]
- Carroll, K.J. On the use and utility of the Weibull model in the analysis of survival data. Control. Clin. Trials 2003, 24, 682–701. [Google Scholar] [CrossRef] [PubMed]
- Frieden, T.R. Evidence for Health Decision Making—Beyond Randomized, Controlled Trials. N. Engl. J. Med. 2017, 377, 465–475. [Google Scholar] [CrossRef]
- Gamerman, V.; Cai, T.; Elsäßer, A. Pragmatic randomized clinical trials: Best practices and statistical guidance. Health Serv. Outcomes Res. Methodol. 2018, 2019, 23–35. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Active Mattresses | Reactive Mattresses | Cushions |
|---|---|---|
| Novis BetterLiving APMBL-101 (MO) Novis Premier Digital 5 (MO) CuroCell A4 CX16 (MR) Novis Premium 9 (MR) | ROHO (MO) Softform Premier (MR) Novis Cairmax (MR) | High profile ROHO single valve High profile Star single valve |
| Characteristics | Active Group (n = 9) | Reactive Group (n = 7) |
|---|---|---|
| Age (mean, (standard deviation)) Gender (male:female) | 82.89 years (9.83) 7:2 | 79.00 years (4.83) 4:3 |
Medical Co-morbidities (n, (%))
| 6 (66.67%) 1 (11.11%) 3 (33.3%) 3 (33.33%) 5 (55.57%) 2 (22.22%) 4 (44.44%) | 6 (85.71%) 3 (42.86%) 2 (28.57%) 1 (14.29%) 1 (14.29%) 2 (28.57%) 4 (57.14%) |
Pressure injury location (n)
| 6 1 2 | 3 2 2 |
Pressure injury Stage (n)
| 7 1 1 | 6 0 1 |
Waterlow Scores (mean (standard deviation))
| 19.33 (7.40) 1.78 (1.30) 1.78 (1.30) | 19.71 (4.54) 3.00 (1.53) 1.71 (1.60) |
Pressure Injury Prevention
| 7.33 h (3.39) o o + | 9.20 h (1.92) o + + |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rae, K.E.; Barker, J.; Upton, D.; Isbel, S. Comparative Effectiveness of Active and Reactive Mattresses in Pressure Injury Healing for Older People in Their Own Homes: A Pragmatic Equivalence Randomised-Controlled Study. Nurs. Rep. 2025, 15, 111. https://doi.org/10.3390/nursrep15030111
Rae KE, Barker J, Upton D, Isbel S. Comparative Effectiveness of Active and Reactive Mattresses in Pressure Injury Healing for Older People in Their Own Homes: A Pragmatic Equivalence Randomised-Controlled Study. Nursing Reports. 2025; 15(3):111. https://doi.org/10.3390/nursrep15030111
Chicago/Turabian StyleRae, Katherine E., Judith Barker, Dominic Upton, and Stephen Isbel. 2025. "Comparative Effectiveness of Active and Reactive Mattresses in Pressure Injury Healing for Older People in Their Own Homes: A Pragmatic Equivalence Randomised-Controlled Study" Nursing Reports 15, no. 3: 111. https://doi.org/10.3390/nursrep15030111
APA StyleRae, K. E., Barker, J., Upton, D., & Isbel, S. (2025). Comparative Effectiveness of Active and Reactive Mattresses in Pressure Injury Healing for Older People in Their Own Homes: A Pragmatic Equivalence Randomised-Controlled Study. Nursing Reports, 15(3), 111. https://doi.org/10.3390/nursrep15030111