
Examining the Contribution of Nurse Practitioners to Geriatric and Palliative Care in Israel

 ,
,  ,
,
Abstract
1. Introduction
Demographic Changes and Their Impact on the Israeli Health System
- To examine the perceptions of palliative and geriatric care NPs regarding their unique contribution to the health system and where this contribution can be made, as well as the differences between the groups.
- To examine how the nurses believe their role in these areas can be developed.
2. Materials and Methods
Data Analysis
3. Results
3.1. Demographic and Occupational Characteristics
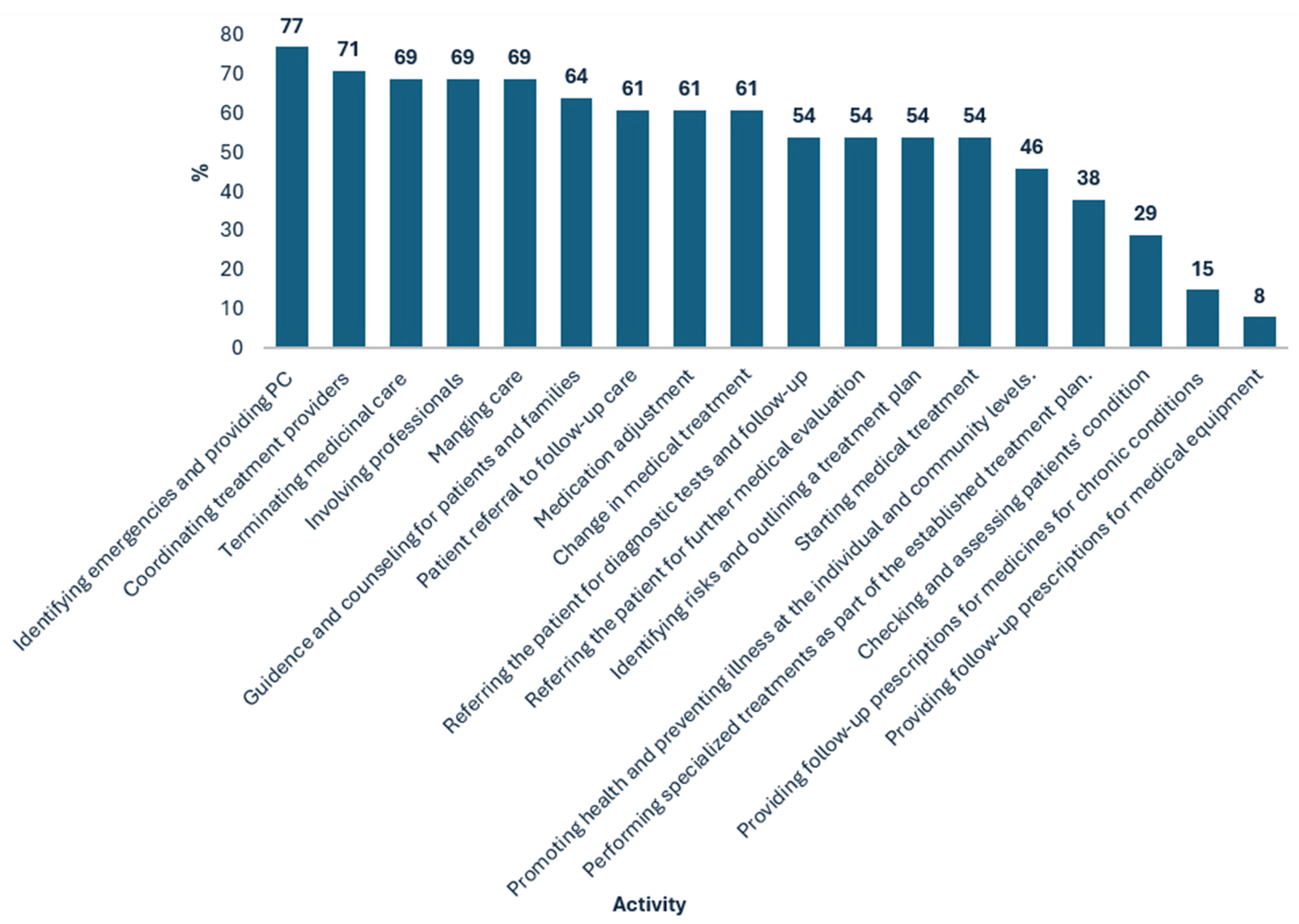
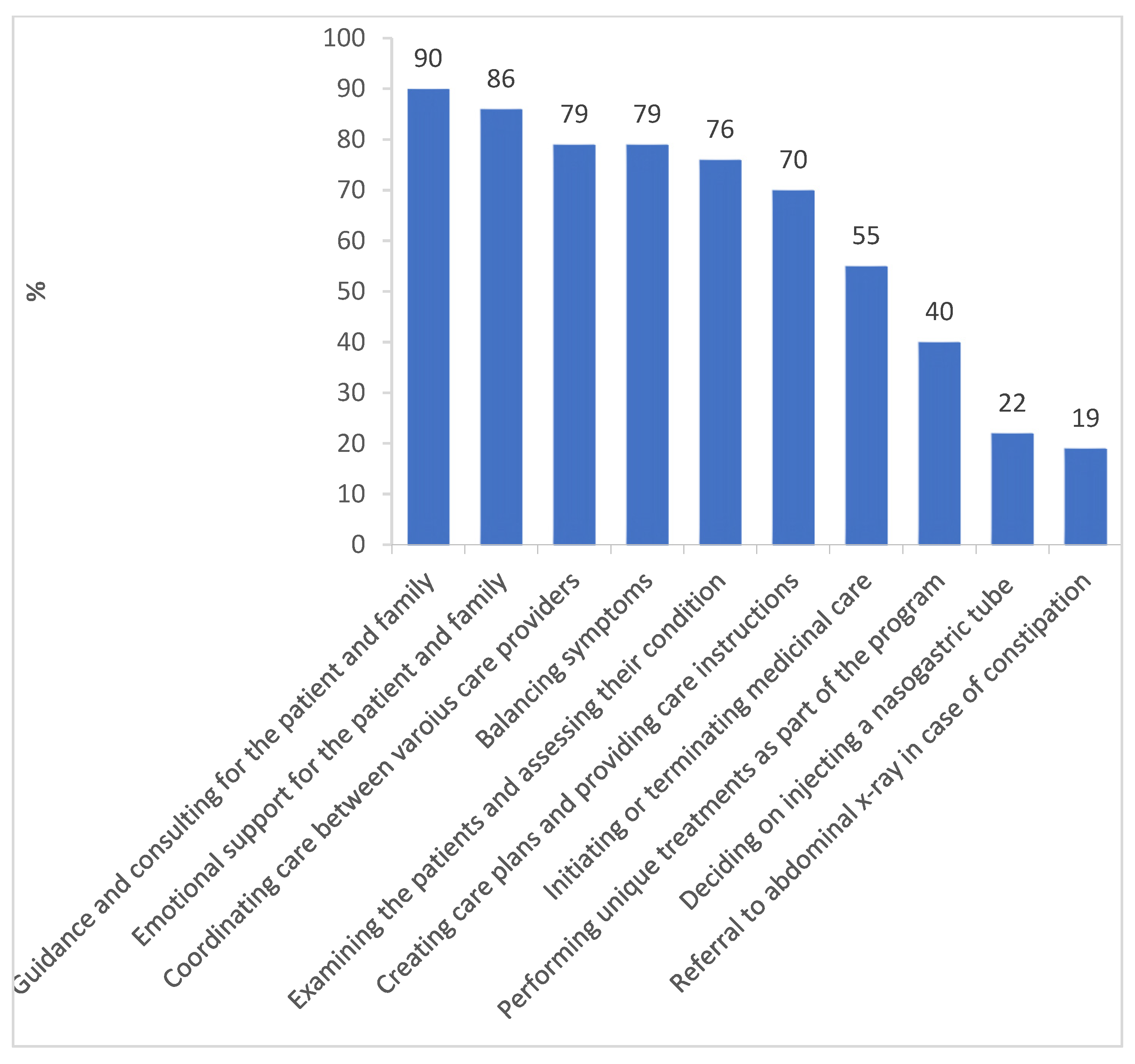
3.2. The Nurse Practitioners’ Reported Activities
3.3. The Nurse Practitioners’ Fourfold Impact
3.3.1. Circle of Influence 1: The Patient
I can also evaluate the patient on my own […]. In fact, I’m working on it write now, patients aged 65–75 who are still healthy without repeated hospitalizations […] still high functioning.(Interviewee #10, geriatric NP)
The mandate of an NP is truly comprehensive, including the physical, familia, and social aspects, and the broader characteristics… You look at the next step, where he goes from here, whether it’s to the community or to hospitalization. I am constantly preoccupied with predicting the next challenges that would have to be dealt with and with trying to provide a far more comprehensive response, which is medical, and also social, and also emotional. And that is something that an ordinary nurse does not have the time and usually not the ability [to do].(#9, palliative NP)
3.3.2. Circle of Influence 2: The Family
Today, in order to talk to a doctor, the family members have to wait for a long time… An NP can contact the family to provide them with answers, because she’s in a fulltime position, and that’s very important. The family needs to know that there’s a professional, with superb professional level, not just good, who can provide clear and serious answers. That will reduce much of the families’ disquiet.(#19, nursing home manager)
3.3.3. Circle of Influence 3: Professionals
The NP is actually the doctor’s substitute in daily life… She has good diagnostic skills and her shoulders are wide enough… She is the one who can help in the nursing area, and also make the right semi-medical decisions.(#19, nursing home manager)
3.3.4. Circle of Influence 4: The Health System
The NP will be able to follow up on them… In every clinic you have elderly patients with chronic illnesses, and if I want to take all these groups and monitor their illnesses and reach out to them and maintain their quality of life, I can save lots of hospital days.(#20, nursing school lecturer)
3.4. The Nurse Practitioners’ Status
3.4.1. Identity
[I’m] on the fence—one foot here, one foot there. I don’t see myself as belonging to either sector, “purely”. I cannot not be a nurse and see the nursing aspect, but I no longer view it strictly as a nurse, I only add the extra aspect… On the whole, I consider myself part of the medicine thing, because that’s what’s expected of me in the role definition… I sit in the doctors’ lounge, I don’t sit in the nursing”.(#4, geriatric NP and senior manager)
Our system is very hierarchic […]. They’re creating a hybrid creature here—the nurse is subordinate to the doctor under whom she works, but the administrative subordination is to nursing, and this creates difficulties.(#24, doctor in the community)
3.4.2. Professionalism
- Among the NPs, 70% reported their activity to the unit’s medical manager, and 53% to the nursing manager of their hospital or organization; in other words, there were quite a few instances of “multiple reporting”.
- Meanwhile, 24% of the NPs reported being subordinated to a single professional individual/entity in the system, 28% reported being subordinate to two, and 9% to three, while 1% even reported being subordinate to four.
- Among the nurses, 37% reported that one professional individual/entity decided on the identity of their patients, 18% reported two, 3% reported three, and 2% reported four.
3.5. Challenges in the Nurse Practitioner’s Role
3.5.1. Establishing the Nurse Practitioner’s Status
Another challenge is the public. They want doctors. They come for the department director, and that’s a difficult challenge.(#20, nursing school lecturer)
I’m against the idea of practitioner nurses, because here in Israel the objective is not to make life easier for the doctors, but to avoid adding doctors’ positions and letting nurses do the doctors’ work… How? At the expense of the patients. Our patients are old, they cannot shout that they want quality treatment, so it’s easy to provide them treatment with less-skilled staff.(#23, doctor and geriatric department director)
3.5.2. Training
3.5.3. Positions
3.5.4. Workload
3.5.5. Integrating Palliative Care into the Health System
3.6. The NPs’ View of the Future of Their Profession
3.7. Crosscutting Theme: Role Ambiguity
4. Discussion
4.1. Conclusions and Recommendations
- Providing a more precise definition of the NPs’ role and regulating their authorities.
- Aligning the NPs’ professional training with job requirements according to role factors, such as:
- Content expertise—knowledge on the content and subject of the role;
- Skill—mastery of skills required to perform the role and acquirement of the relevant toolset;
- Role identity—with emphasis on the NPs’ work in the community and developing abilities for ongoing knowledge refreshment.
- Strengthening the relationships and trust between the medical establishment and the NPs through dialogue and opportunities for professional encounters, such as conferences and peer forums for consultation.
- Emphasizing emotional support for palliative care NPs.
- Branding the NPs’ role using special badges and logos to highlight their uniqueness in the medical system.
Implications for Health Policy
- Increasing the number of training positions for NPs in geriatrics and palliative care.
- Developing clear guidelines for autonomous NP practice, especially in community settings.
- Implementing continuing education programs to maintain NPs’ skill currency.
- Creating financial incentives to attract more nurses to NP specializations.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
Guidelines and Standards Statement
Use of Artificial Intelligence
Conflicts of Interest
Abbreviations
| NP | Nurse practitioner |
References
- Shnoor, Y.; Cohen, Y. (Eds.) The 65+ Age Population in Israel—Statistical Abstract 2021; Myers-JDC-Brookdale Institute: Jerusalem, Israel, 2021. (In Hebrew) [Google Scholar]
- Rechel, B.; Grundy, E.; Robine, J.M.; Cylus, J.; Mackenbach, J.P.; Knai, C.; McKee, M. Ageing in the European union. Lancet 2013, 381, 1312–1322. [Google Scholar] [CrossRef]
- He, Y.; Wei, B.; Li, Y. The impact of using community home-based elderly care services on older adults’ self-reported health: Fresh evidence from China. Front. Public Health 2023, 11, 1257463. [Google Scholar] [CrossRef]
- Sela-Vilensky, Y.; Grinberg, K.; Nissanholtz-Gannot, R. Attracting Israeli nursing students to community nursing. Isr. J. Health Policy Res. 2020, 9, 44. [Google Scholar] [CrossRef] [PubMed]
- Haran Rosen, M.; Cohen, G.; Ramot-Nyska, T. Long-Term Care in Israel; Bank of Israel: Jerusalem, Israel, 2018; Available online: https://www.boi.org.il/en/economic-roles/research-and-publications/all-research/occasional-papers/long-term-care-in-israel/ (accessed on 24 April 2018). (In Hebrew)
- National Health Insurance Law. Israeli Book of Laws 5754; No. 1469; National Health Insurance Law: Jerusalem, Israel, 1994. (In Hebrew) [Google Scholar]
- Bentur, N. Education Programs and In-Service Training in Palliative Care in Israel—Current Situation; RR-762-17; Myers-JDC-Brookdale Institute: Jerusalem, Israel, 2017; Available online: https://brookdale.jdc.org.il/en/publication/education-programs-service-training-palliative-care-israel-current-situation/ (accessed on 17 January 2017). (In Hebrew)
- Hasson, Y.; Dagan-Buzaglo, N. The Care Deficit: What It Means and How It Can be Reduced; Adva Center: Tel Aviv, Israel, 2019. Available online: https://adva.org/en/care-deficit/ (accessed on 17 February 2019).
- Fisher-Reif, I.; Bentur, N.; Laxer, I. Recommendations for a National Plan for Palliative Care and Terminal Conditions; Ministry of Health: Jerusalem, Israel; JDC-Eshel: Jerusalem, Israel; Myers-Joint Brookdale Institute: Jerusalem, Israel, 2016. (In Hebrew) [Google Scholar]
- Hochwald, I.H.; Yakov, G.; Radomyslsky, Z.; Danon, Y.; Nissanholtz-Gannot, R. Ethical challenges in end-stage dementia: Perspectives of professionals and family care-givers. Nurs. Ethics 2021, 28, 1228–1243. [Google Scholar] [CrossRef] [PubMed]
- Adams, E.; Maier, C.B.; Buchan, J.; Cash-Gabison, L. Good Practice Brief: Advancing the Role of Nurses and Midwives in Ireland: Pioneering Transformation of the Health Workforce for no Communicable Diseases in Europe; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Delamaire, M.L.; Lafortune, G. Nurses in Advanced Roles: A Description and Evaluation of Experiences in 12 Developed Countries; OECD Health Working Paper; OECD Publishing: Paris, France, 2010. [Google Scholar]
- Maier, C.B.; Aiken, L.H.; Busse, R. Nurses in Advanced Roles: Policy Levers to Implementation; OECD Health Working Paper; OECD: Paris, France, 2017. [Google Scholar]
- Moons, P.; Callens, B.; Gut, C.; Lindpaintner, L. Introducing advanced practice nurses/nurse practitioners in health care systems: A framework for reflection and analysis. Swiss Med. Wkly. 2008, 138, 621–628. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Long, Q.; Jackson, S.L.; Rhee, M.K.; Tomolo, A.; Olson, D.; Phillips, L.S. Nurse practitioners, physician assistants, and physicians are comparable in managing the first five years of diabetes. Am. J. Med. 2018, 131, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. General Administration. In The Nurse Practitioner; Circular 9/2014; Ministry of Health: Jerusalem, Israel, 2014. Available online: https://www.health.gov.il/hozer/mk09_2014.pdf (accessed on 20 February 2014). (In Hebrew)
- Barton, T.D.; Bevan, L.; Moony, G. The development of advanced nursing roles. Nurs. Times 2012, 18, 18–20. [Google Scholar]
- Bryant-Lukosius, D.; Carter, N.; Kilpatrick, K.; Misener, R.M.; Donald, F.; Kaasalainen, S.; Hardman, P.; Bourgeault, I.; Alba, D. The clinical nurse specialist role in Canada [Special issue]. Nurs. Leadersh. 2010, 23, 140–166. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. Specialization in Palliative Care. 2024. Available online: https://www1.health.gov.il/nursing/study/specialization-studies/specialization-list/palliative-care (accessed on 10 December 2024). (In Hebrew)
- Csorba, S. The role of a nurse specialist in palliative care: An Israeli experience. Asia Pac. J. Oncol. Nurs. 2017, 4, 112–115. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Medical Division. Work Procedures for Geriatric Nursing Nurse Practitioners in the General Hospitalization System; Circular 8/2020; Ministry of Health: Jerusalem, Israel, 2021. Available online: https://www.gov.il/he/pages/mr08-2020 (accessed on 13 April 2021). (In Hebrew)
- Yang, B.K.; Johantgen, M.E.; Trinkoff, A.M.; Idzik, S.R.; Wince, J.; Tomlinson, C. State nurse practitioner practice regulations and US health care delivery outcomes: A systematic review. Med. Care Res. Rev. 2021, 78, 183–196. [Google Scholar] [CrossRef] [PubMed]
- Boeijen, E.R.K.; Peters, J.W.B.; van Vught, A.J.A.H. Nurse practitioners leading the way: An exploratory study on the added value of nurse practitioners in outpatient care in the Netherlands. J. Am. Assoc. Nurse Pract. 2020, 32, 800–808. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. Specialization in Geriatric Nursing. 2023. Available online: https://www1.health.gov.il/nursing/study/specialization-studies/specialization-list/geriatrics-specialization (accessed on 12 April 2023). (In Hebrew)
- Shkedi, A. Words of Meaning: Qualitative Research—Theory and Practice; Ramot: Tel Aviv, Israel, 2004. (In Hebrew) [Google Scholar]
- DesRoches, C.M.; Clarke, S.; Perloff, J.; O’Reilly-Jacob, M.; Buerhaus, P. The quality of primary care provided by nurse practitioners to vulnerable Medicare beneficiaries. Nurs. Outlook 2017, 65, 679–688. [Google Scholar] [CrossRef] [PubMed]
- Lovink, M.H.; Persoon, A.; Koopmans, R.T.C.M.; Van Vught, A.J.A.H.; Schoonhoven, L.; Laurant, M.G.H. Effects of substituting nurse practitioners, physician assistants or nurses for physicians concerning healthcare for the ageing population: A systematic literature review. J. Adv. Nurs. 2017, 73, 2084–2102. [Google Scholar] [CrossRef] [PubMed]
- Haron, Y.; Romem, A.; Greenberger, C. The role and function of the palliative care nurse practitioner in Israel. Int. J. Palliat. Nurs. 2019, 25, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Badawy, W.; Shaban, M. Exploring geriatric nurses’ perspectives on the adoption of AI in elderly care a qualitative study. Geriatr. Nurs. 2025, 61, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Callies, D. Augmenting Gerontology Education in Family Nurse Practitioner Curriculum. J. Nurse Pract. 2025, 21, 105249. [Google Scholar] [CrossRef]
- Feyereisen, S.; Goodrick, E. Examining variable nurse practitioner independence across jurisdictions: A case study of the United States. Int. J. Nurs. Stud. 2020, 118, 103633. [Google Scholar] [CrossRef] [PubMed]
- Hagan, J.; Curtis Sr, D.L. Predictors of nurse practitioner retention. J. Am. Assoc. Nurse Pract. 2018, 30, 280–284. [Google Scholar] [CrossRef] [PubMed]
- Coats, H.; Henrichs, K. The Role and Professional Standards of the Adult-Gerontology Nurse Practitioner in Hospice and Palliative Care. J. Hosp. Palliat. Nurs. 2024, 26, 116–121. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Total | Geriatrics | Palliative | |
|---|---|---|---|
| Respondents | |||
| n | 89 | 29 | 60 |
| % | 100 | 33 | 67 |
| Gender | |||
| M | 16 | 31 | 8 |
| F | 84 | 69 | 92 |
| Mage | 53 | 52 | 55 |
| Birthplace | |||
| Israel | 69 | 59 | 75 |
| Other | 31 | 41 | 25 |
| Nationality/Religion | |||
| Jewish | 88 | 86 | 88 |
| Muslim Arab | 8 | 10 | 7 |
| Christian Arab | 3 | 3 | 3 |
| Other | 1 | 0 | 2 |
| Total (N = 89) | Geriatrics (n = 29) | Palliative (n = 60) | |
|---|---|---|---|
| Experience as nurse (in years) | |||
| 10–20 | 20 | 28 | 17 |
| 21–30 | 38 | 37 | 38 |
| 31–50 | 42 | 35 | 45 |
| Currently employed as NP | 65 | 48 | 73 |
| Experience as NP (in years) | |||
| 1–4 | 53 | 43 | 56 |
| 5–10 | 37 | 57 | 30 |
| 10+ | 10 | - | 14 |
| Employment scope | |||
| Part time | 29 | 7 | 36 |
| Full time | 72 | 93 | 64 |
| Managerial role | 53 | 7 | 67 |
| Workplace | |||
| Dept. in general hospital | 9 | 5 | 7 |
| Consulting service in general hospital | 26 | - | 35 |
| Dept. in geriatric hospital | 22 | 64 | - |
| Consulting service in geriatric hospital | 2 | - | 4 |
| Hospital ambulatory clinic | 2 | 7 | - |
| Primary clinic in the community | 4 | - | 5 |
| Specialist clinic in the community | 4 | 7 | 2 |
| Consultation clinic in the community | 2 | - | 7 |
| Home visits in the community unit | 2 | - | 7 |
| Home hospitalization in the community | 5 | - | 5 |
| Hospice in hospital | 4 | - | 5 |
| Home hospice | - | - | - |
| Managerial staff unit/administration | 18 | 17 | 23 |
| No. of patients per week (full time) | |||
| 5–10 | 20 | - | 30 |
| 10–30 | 38 | 62 | 26 |
| +30 | 33 | 39 | 30 |
| Not providing direct care | 10 | - | 15 |
| Stakeholder | Contribution |
|---|---|
| Patient | Preventive medicine Holistic view of the patient Ability to treat complex and extreme cases |
| Family members | High availability |
| Professionals | Authority on medical consulting Reducing the physicians’ workload |
| Health system | Coordinating care Reducing the rates of hospitalization/institutionalization |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nissanholtz-Gannot, R.; Grinberg, K.; Goldberg, S.; Fighel, H.; Sela, Y.; Cohen, Y.; Hazoref, R.H. Examining the Contribution of Nurse Practitioners to Geriatric and Palliative Care in Israel. Nurs. Rep. 2025, 15, 101. https://doi.org/10.3390/nursrep15030101
Nissanholtz-Gannot R, Grinberg K, Goldberg S, Fighel H, Sela Y, Cohen Y, Hazoref RH. Examining the Contribution of Nurse Practitioners to Geriatric and Palliative Care in Israel. Nursing Reports. 2025; 15(3):101. https://doi.org/10.3390/nursrep15030101
Chicago/Turabian StyleNissanholtz-Gannot, Rachel, Keren Grinberg, Shoshy Goldberg, Hilla Fighel, Yael Sela, Yafit Cohen, and Rivka Hazan Hazoref. 2025. "Examining the Contribution of Nurse Practitioners to Geriatric and Palliative Care in Israel" Nursing Reports 15, no. 3: 101. https://doi.org/10.3390/nursrep15030101
APA StyleNissanholtz-Gannot, R., Grinberg, K., Goldberg, S., Fighel, H., Sela, Y., Cohen, Y., & Hazoref, R. H. (2025). Examining the Contribution of Nurse Practitioners to Geriatric and Palliative Care in Israel. Nursing Reports, 15(3), 101. https://doi.org/10.3390/nursrep15030101