
Caregiver Contribution to Self-Care of Chronic Illness Inventory: Evaluation of Measurement Properties in a Middle-Income Country

 ,
,  ,
,  ,
,  , , , , , and
, , , , , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants and Setting
2.3. Data Collection
2.4. Measurements
2.5. Ethical Considerations
2.6. Data Analysis
3. Results
3.1. Characteristics of the Sample
3.2. Item Descriptive Analysis
3.3. Testing the Structural Validity of the CC-SC-CII Albanian Version
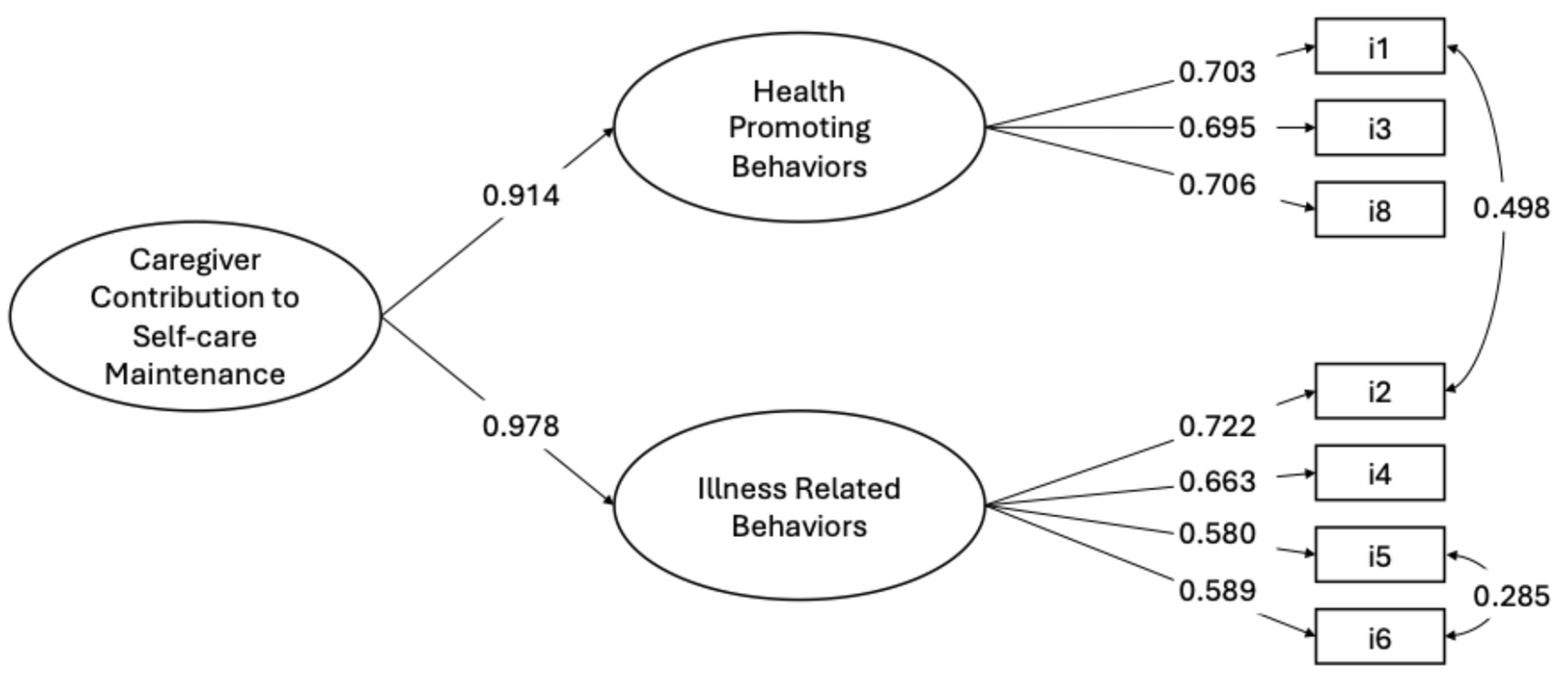
3.3.1. Caregiver Contribution to Self-Care Maintenance Scale
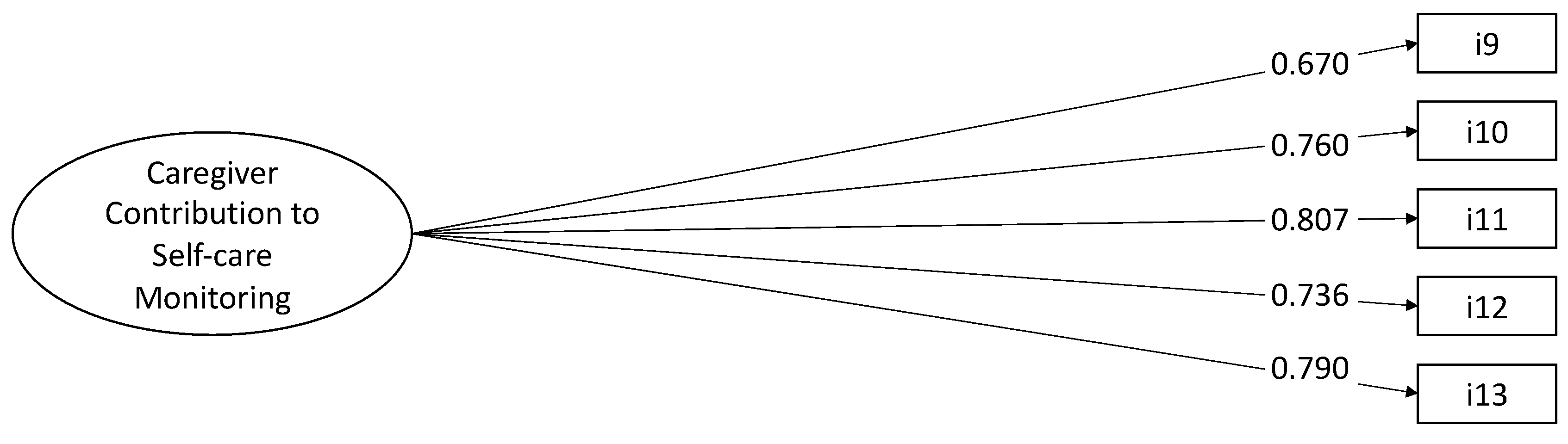
3.3.2. Caregiver Contribution to Self-Care Monitoring Scale
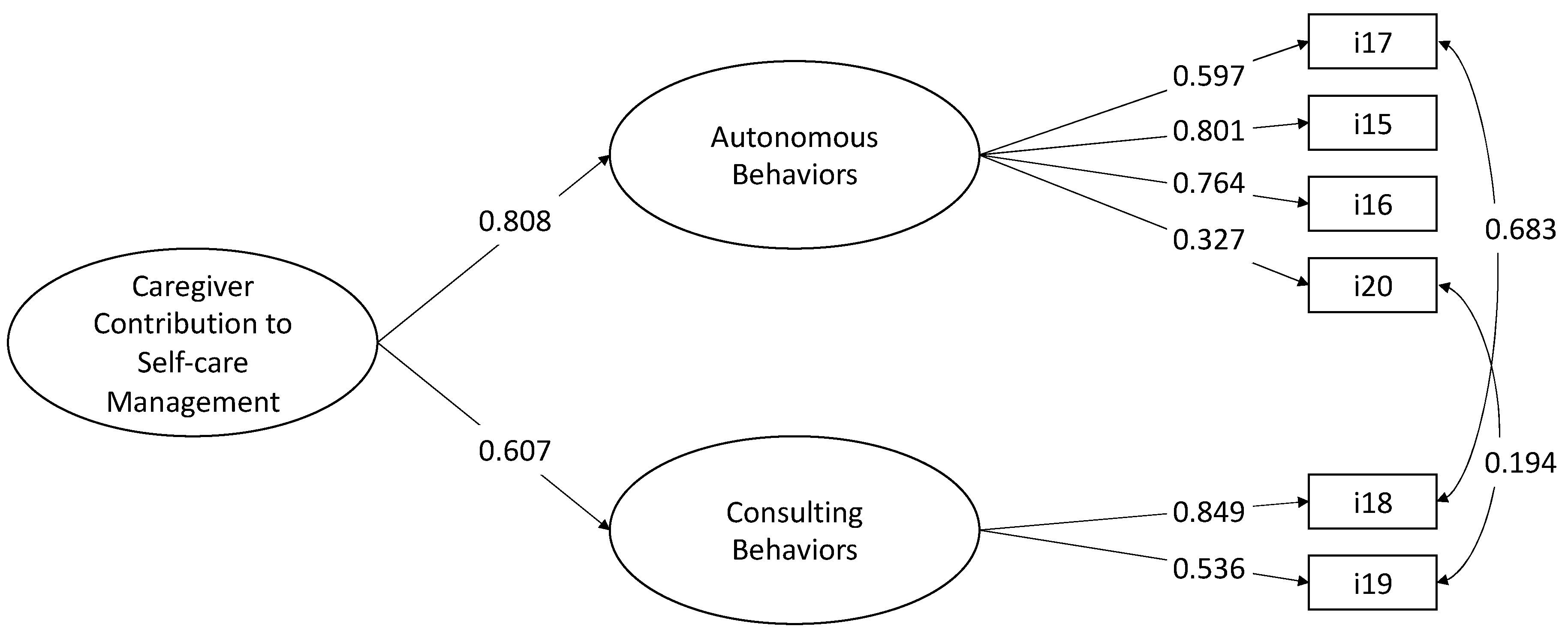
3.3.3. Caregiver Contribution to Self-Care Management Scale
3.3.4. Construct Validity
3.4. Testing the Reliability of the CC-SC-CII Albanian Version
3.4.1. Internal Consistency Reliability
3.4.2. Stability
3.5. Testing the Measurement Errors of the CC-SC-CII Albanian Version
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
Guidelines and Standards Statement
Use of Artificial Intelligence
Conflicts of Interest
References
- World Health Organization. Noncommunicable Diseases. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 10 August 2024).
- Group, W.B. The World Bank in Albania. Available online: https://www.worldbank.org/en/country/albania/overview (accessed on 10 August 2024).
- Kraja, F.; Kraja, B.; Mone, I.; Harizi, I.; Babameto, A.; Burazeri, G. Self-reported Prevalence and Risk Factors of Non-communicable Diseases in the Albanian Adult Population. Med. Arch. 2016, 70, 208–212. [Google Scholar] [CrossRef] [PubMed]
- GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef]
- Hajat, C.; Stein, E. The global burden of multiple chronic conditions: A narrative review. Prev. Med. Rep. 2018, 12, 284–293. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Guideline on Self-Care Interventions for Health and Well-Being, 2022 Revision; WHO Guidelines Approved by the Guidelines Review Committee; WHO: Geneva, Switzerland, 2022. [Google Scholar]
- Hearn, J.; Ssinabulya, I.; Schwartz, J.I.; Akiteng, A.R.; Ross, H.J.; Cafazzo, J.A. Self-management of non-communicable diseases in low- and middle-income countries: A scoping review. PLoS ONE 2019, 14, e0219141. [Google Scholar] [CrossRef]
- Riegel, B.; Jaarsma, T.; Stromberg, A. A middle-range theory of self-care of chronic illness. ANS Adv. Nurs. Sci. 2012, 35, 194–204. [Google Scholar] [CrossRef]
- World Health Organization. WHO Consolidated Guideline on Self-Care Interventions for Health: Sexual and Reproductive Health and Rights; WHO Guidelines Approved by the Guidelines Review Committee; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Jaarsma, T.; Cameron, J.; Riegel, B.; Stromberg, A. Factors Related to Self-Care in Heart Failure Patients According to the Middle-Range Theory of Self-Care of Chronic Illness: A Literature Update. Curr. Heart Fail. Rep. 2017, 14, 71–77. [Google Scholar] [CrossRef]
- Vellone, E.; Riegel, B.; Alvaro, R. A Situation-Specific Theory of Caregiver Contributions to Heart Failure Self-care. J. Cardiovasc. Nurs. 2019, 34, 166–173. [Google Scholar] [CrossRef]
- Chen, Y.; Zou, H.; Zhang, Y.; Fang, W.; Fan, X. Family Caregiver Contribution to Self-care of Heart Failure: An Application of the Information-Motivation-Behavioral Skills Model. J. Cardiovasc. Nurs. 2017, 32, 576–583. [Google Scholar] [CrossRef] [PubMed]
- Hooker, S.A.; Schmiege, S.J.; Trivedi, R.B.; Amoyal, N.R.; Bekelman, D.B. Mutuality and heart failure self-care in patients and their informal caregivers. Eur. J. Cardiovasc. Nurs. 2018, 17, 102–113. [Google Scholar] [CrossRef]
- Cassidy, L.; Hill, L.; Fitzsimons, D.; McGaughey, J. The impact of psychoeducational interventions on the outcomes of caregivers of patients with heart failure: A systematic review and meta-analysis. Int. J. Nurs. Stud. 2021, 114, 103806. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, R.B.; Bryson, C.L.; Udris, E.; Au, D.H. The influence of informal caregivers on adherence in COPD patients. Ann. Behav. Med. 2012, 44, 66–72. [Google Scholar] [CrossRef] [PubMed]
- De Maria, M.; Matarese, M.; Stromberg, A.; Ausili, D.; Vellone, E.; Jaarsma, T.; Osokpo, O.H.; Daus, M.M.; Riegel, B.; Barbaranelli, C. Cross-cultural assessment of the Self-Care of Chronic Illness Inventory: A psychometric evaluation. Int. J. Nurs. Stud. 2021, 116, 103422. [Google Scholar] [CrossRef] [PubMed]
- Riegel, B.; Barbaranelli, C.; Sethares, K.A.; Daus, M.; Moser, D.K.; Miller, J.L.; Haedtke, C.A.; Feinberg, J.L.; Lee, S.; Stromberg, A.; et al. Development and initial testing of the self-care of chronic illness inventory. J. Adv. Nurs. 2018, 74, 2465–2476. [Google Scholar] [CrossRef]
- Chen, D.D.; Zhang, H.; Cui, N.; Tang, L.; Shao, J.; Wang, X.; Wang, D.; Liu, N.; Ye, Z. Cross-cultural adaptation and validation of the caregiver contribution to self-care of chronic illness inventory in China: A cross-sectional study. BMJ Open 2021, 11, e048875. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Kim, E.; Chung, M.; Yeom, I. Validity and reliability of the Korean caregiver contribution to self-care chronic illness inventory. Sci. Rep. 2023, 13, 7808. [Google Scholar] [CrossRef]
- Vellone, E.; Lorini, S.; Ausili, D.; Alvaro, R.; Di Mauro, S.; De Marinis, M.G.; Matarese, M.; De Maria, M. Psychometric characteristics of the caregiver contribution to self-care of chronic illness inventory. J. Adv. Nurs. 2020, 76, 2434–2445. [Google Scholar] [CrossRef]
- Arapi, A.; Vellone, E.; Ivziku, D.; Duka, B.; Taci, D.; Notarnicola, I.; Stievano, A.; Prendi, E.; Rocco, G.; De Maria, M. Psychometric Characteristics of the Self-Care of Chronic Illness Inventory in Older Adults Living in a Middle-Income Country. Int. J. Environ. Res. Public Health 2023, 20, 4714. [Google Scholar] [CrossRef] [PubMed]
- McKown, S.; Acquadro, C.; Anfray, C.; Arnold, B.; Eremenco, S.; Giroudet, C.; Martin, M.; Weiss, D. Good practices for the translation, cultural adaptation, and linguistic validation of clinician-reported outcome, observer-reported outcome, and performance outcome measures. J. Patient Rep. Outcomes 2020, 4, 89. [Google Scholar] [CrossRef]
- Tarlow, B.J.; Wisniewski, S.R.; Belle, S.H.; Rubert, M.; Ory, M.G.; Gallagher-Thompson, D. Positive Aspects of Caregiving:Contributions of the REACH Project to the Development of New Measures for Alzheimer’s Caregiving. Res. Aging 2004, 26, 429–453. [Google Scholar] [CrossRef]
- Muthén, B.; Kaplan, D. A comparison of some methodologies for the factor analysis of non-normal Likert variables. Br. J. Math. Stat. Psychol. 1985, 38, 171–189. [Google Scholar] [CrossRef]
- Barbaranelli, C.; Lee, C.S.; Vellone, E.; Riegel, B. The problem with Cronbach’s Alpha: Comment on Sijtsma and van der Ark (2015). Nurs. Res. 2015, 64, 140–145. [Google Scholar] [CrossRef]
- Linden, W.J.v.d. Handbook of Item Response Theory; CRC Press, Taylor & Francis Group: Boca Raton, FL, USA, 2018. [Google Scholar]
- Meade, A.W.; Johnson, E.C.; Braddy, P.W. Power and sensitivity of alternative fit indices in tests of measurement invariance. J. Appl. Psychol. 2008, 93, 568–592. [Google Scholar] [CrossRef]
- Vandenberg, R.J.; Lance, C.E. A Review and Synthesis of the Measurement Invariance Literature: Suggestions, Practices, and Recommendations for Organizational Research. Organ. Res. Methods 2000, 3, 4–70. [Google Scholar] [CrossRef]
- Browne, M.W.; Cudeck, R. Alternative Ways of Assesssing Model Fit. Sociol. Methods Res. 1992, 21, 230–258. [Google Scholar] [CrossRef]
- Hu, L.t.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. A Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; L. Erlbaum Associates: Hillsdale, NJ, USA, 1988; p. xxi. 567p. [Google Scholar]
- Grant, G.; Nolan, M. Informal carers: Sources and concomitants of satisfaction. Health Soc. Care Community 1993, 1, 147–159. [Google Scholar] [CrossRef]
- Fornell, C.; Larcker, D.F. Evaluating Structural Equation Models with Unobservable Variables and Measurement Error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Trizano-Hermosilla, I.; Galvez-Nieto, J.L.; Alvarado, J.M.; Saiz, J.L.; Salvo-Garrido, S. Reliability Estimation in Multidimensional Scales: Comparing the Bias of Six Estimators in Measures With a Bifactor Structure. Front. Psychol. 2021, 12, 508287. [Google Scholar] [CrossRef]
- Bagozzi, R.P. Issues in the Application of Covariance Structure Analysis: A Further Comment. J. Consum. Res. 1983, 9, 449–450. [Google Scholar] [CrossRef]
- Thorndike, R.M. Book Review: Psychometric Theory (3rd ed.) by Jum Nunnally and Ira Bernstein New York: McGraw-Hill, 1994, xxiv + 752 pp. Appl. Psychol. Meas. 1995, 19, 303–305. [Google Scholar] [CrossRef]
- Brown, J.D. Standard error vs. Standard error of measurement. Shiken JALT Test. Eval. SIG Newsl. 1999, 3, 20–25. [Google Scholar]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 8th ed.; Muthén & Muthén: Los Angeles, CA, USA, 1998. [Google Scholar]
- Weijters, B.; Geuens, M.; Schillewaert, N. The proximity effect: The role of inter-item distance on reverse-item bias. Int. J. Res. Mark. 2009, 26, 2–12. [Google Scholar] [CrossRef]
- Fornell, C. Issues in the Application of Covariance Structure Analysis: A Comment. J. Consum. Res. 1983, 9, 443–448. [Google Scholar] [CrossRef]
- Besedovsky, L.; Lange, T.; Born, J. Sleep and immune function. Pflug. Arch 2012, 463, 121–137. [Google Scholar] [CrossRef]
- Barry, C.A.; Bradley, C.P.; Britten, N.; Stevenson, F.A.; Barber, N. Patients’ unvoiced agendas in general practice consultations: Qualitative study. BMJ 2000, 320, 1246–1250. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.C.; Suchyta, M.R.; Darowski, E.S.; Collar, E.M.; Kiehl, A.L.; Van, J.; Jackson, J.C.; Hopkins, R.O. Psychological Sequelae in Family Caregivers of Critically III Intensive Care Unit Patients. A Systematic Review. Ann. Am. Thorac. Soc. 2019, 16, 894–909. [Google Scholar] [CrossRef]
- Kertz, S.; Bigda-Peyton, J.; Bjorgvinsson, T. Validity of the Generalized Anxiety Disorder-7 scale in an acute psychiatric sample. Clin. Psychol. Psychother. 2013, 20, 456–464. [Google Scholar] [CrossRef] [PubMed]
- Lowe, B.; Decker, O.; Muller, S.; Brahler, E.; Schellberg, D.; Herzog, W.; Herzberg, P.Y. Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Med. Care 2008, 46, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Gabrani, J.; Schindler, C.; Wyss, K. Health Seeking Behavior Among Adults and Elderly With Chronic Health Condition(s) in Albania. Front. Public Health 2021, 9, 616014. [Google Scholar] [CrossRef] [PubMed]
- De Maria, M.; Ferro, F.; Ausili, D.; Buck, H.G.; Vellone, E.; Matarese, M. Characteristics of dyadic care types among patients living with multiple chronic conditions and their informal caregivers. J. Adv. Nurs. 2021, 77, 4768–4781. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variable | N (%) |
|---|---|
| Gender | |
| Female | 166 (66.40) |
| Male | 84 (33.60) |
| Marital Status | |
| Married | 207 (82.80) |
| Single | 35 (14.0) |
| Separated/Divorced/Widowed | 8 (3.20) |
| Education level (years) | |
| ≤8 | 242 (96.80) |
| >8 | 89 (3.20) |
| Income | |
| Enough to live | 200 (80.0) |
| More than necessary to live | 34 (12.80) |
| Lower than necessary to live | 18 (7.20) |
| Living with other people | |
| No | 2 (0.80) |
| 1 | 77 (30.80) |
| 2 | 58 (23.20) |
| ≥3 | 113 (45.20) |
| Living with patient | |
| Yes | 174 (69.60) |
| No | 76 (30.40) |
| Relationship patient–caregiver | |
| Sons/Daughter | 96 (38.40) |
| Husband/Wife | 78 (31.20) |
| Son/Daughter-in-law | 40 (16.0) |
| Nephew/Niece | 23 (9.20) |
| Brother/Sister | 5 (2.0) |
| Other | 8 (3.20) |
| Patient’s chronic conditions | |
| Hypertension | 219 (87.6) |
| Diabetes mellitus | 185 (74.0) |
| Heart failure | 112 (44.8) |
| COPD | 32 (12.8) |
| Kidney disease | 20 (8.0) |
| Arthritis | 20 (8.0) |
| Other | 28 (11.2) |
| (Mean ± DS) | |
| Age | 49.91 (15.59) |
| Caregiving hours per week | |
| 0–10 | 56 (22.40) |
| 11–20 | 95 (38.0) |
| 21–30 | 78 (31.20) |
| >30 | 21 (8.40) |
| Number of patients with chronic conditions | 2.49 (0.70) |
| Items | M | SD | Skewness | Kurtosis |
|---|---|---|---|---|
| How often do you recommend that the person you care for do the following things? | ||||
| 1. Get enough sleep | 4.43 | 0.80 | −1.45 | 2.15 |
| 2. Try to avoid getting sick (e.g., flu shot, wash their hands) | 4.55 | 0.73 | −1.71 | 2.90 |
| 3. Do physical activity (e.g., take a brisk walk, use the stairs) | 3.99 | 1.05 | −0.67 | −0.56 |
| 4. Eat a special diet | 4.14 | 0.93 | −0.66 | −0.61 |
| 5. See their healthcare provider for routine healthcare | 4.57 | 0.71 | −1.69 | 2.41 |
| 6. Take prescribed medicines without missing a dose | 4.74 | 0.58 | −2.78 | 9.71 |
| 8. Manage stress | 4.02 | 1.05 | −0.65 | −0.73 |
| How often do you do the following things? | ||||
| 9. Monitor the condition of the person for whom you care you care? | 4.50 | 0.67 | −0.99 | −0.23 |
| 10. Pay attention to changes in how the person for whom you care feels? | 4.31 | 0.82 | −1.07 | 0.70 |
| 11. Monitor for medication side-effects of the person for whom you care? | 4.13 | 0.88 | −0.57 | −0.59 |
| 12. Monitor whether the person for whom you care tires more than usual doing normal activities? | 4.15 | 0.89 | −0.65 | −0.63 |
| 13. Monitor for symptoms of the person for whom you care? | 4.24 | 0.84 | −0.78 | −0.35 |
| 15. When the person for whom you care has symptoms, how likely are you to recommend or actually change what he/she eats or drinks to make the symptom decrease or go away? | 4.13 | 0.85 | −0.64 | −0.17 |
| 16. When the person for whom you care has symptoms, how likely are you to recommend or actually change his/her activity level (e.g., slow down, rest)? | 4.26 | 0.80 | −0.71 | −0.50 |
| 17. When the person for whom you care has symptoms, how likely are you to recommend he/she take medicines to make the symptoms decrease or go away? | 4.43 | 0.76 | −1.13 | 0.78 |
| 18. When the person for whom you care has symptoms, how likely are you to recommend he/she tell his/her healthcare provider about the symptoms at the next office visit? | 4.53 | 0.71 | −1.38 | 1.25 |
| 19. When the person for whom you care has symptoms, how likely are you to recommend he/she call his/her healthcare provider for guidance? | 4.18 | 0.97 | −0.94 | 0.01 |
| 20. Think of a remedy you tried the last time the patient for whom you care had symptoms. Did the remedy make the person you care for feel better? | 3.51 | 1.16 | −0.70 | 0.56 |
| Variable | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|
| 1. CC Self-Care Maintenance | - | |||||
| 2. CC Self-Care Monitoring | 0.584 | |||||
| 3. CC Self-Care Management | 0.600 | 0.767 | ||||
| 4. Self-Care Maintenance | 0.342 | 0.250 | 0.191 | |||
| 5. Self-Care Monitoring | 0.273 | 0.393 | 0.233 | 0.600 | ||
| 6. Self-Care Management | 0.361 | 0.396 | 0.364 | 0.561 | 0.631 | |
| 7. PACs | 0.231 | 0.289 | 0.249 | 0.326 | 0.128 * | 0.233 |
| Variable | Single Factor Reliability | Multidimensional Model-Based Reliability | Cronbach’s Alpha |
|---|---|---|---|
| CC Self-Care Maintenance scale | 0.837 | 0.833 | |
| Health promoting behaviors factor | 0.893 | ||
| Illness-related behavior factor | 0.890 | ||
| CC Self-Care Monitoring scale | - | - | 0.866 |
| CC Self-Care Management scale | 0.756 | 0.728 | |
| Autonomous behavior factor | 0.825 | ||
| Consulting behavior factor | 0.901 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adëraj, S.; Arapi, A.; Mazzotta, R.; Stievano, A.; Taci, D.; Ivziku, D.; Bernalte-Martí, V.; Vellone, E.; Rocco, G.; De Maria, M. Caregiver Contribution to Self-Care of Chronic Illness Inventory: Evaluation of Measurement Properties in a Middle-Income Country. Nurs. Rep. 2025, 15, 42. https://doi.org/10.3390/nursrep15020042
Adëraj S, Arapi A, Mazzotta R, Stievano A, Taci D, Ivziku D, Bernalte-Martí V, Vellone E, Rocco G, De Maria M. Caregiver Contribution to Self-Care of Chronic Illness Inventory: Evaluation of Measurement Properties in a Middle-Income Country. Nursing Reports. 2025; 15(2):42. https://doi.org/10.3390/nursrep15020042
Chicago/Turabian StyleAdëraj, Sajmira, Alta Arapi, Rocco Mazzotta, Alessandro Stievano, Dasilva Taci, Dhurata Ivziku, Vicente Bernalte-Martí, Ercole Vellone, Gennaro Rocco, and Maddalena De Maria. 2025. "Caregiver Contribution to Self-Care of Chronic Illness Inventory: Evaluation of Measurement Properties in a Middle-Income Country" Nursing Reports 15, no. 2: 42. https://doi.org/10.3390/nursrep15020042
APA StyleAdëraj, S., Arapi, A., Mazzotta, R., Stievano, A., Taci, D., Ivziku, D., Bernalte-Martí, V., Vellone, E., Rocco, G., & De Maria, M. (2025). Caregiver Contribution to Self-Care of Chronic Illness Inventory: Evaluation of Measurement Properties in a Middle-Income Country. Nursing Reports, 15(2), 42. https://doi.org/10.3390/nursrep15020042