
A Scoping Review of Educational and Training Interventions on Parkinson’s Disease for Staff in Care Home Settings
 , , , , ,
, , , , ,  ,
, 

Abstract
1. Introduction
- (1)
- Identify the existing literature on the education and training programs available for nursing and nursing assistant staff in care homes regarding PD.
- (2)
- Analyze the content and effectiveness of the PD education and training programs available to nursing and care staff in care home settings.
- (3)
- Propose recommendations for enhancing the quality and accessibility of education and training opportunities for nursing and care staff in care homes to improve the care of people living with PD in care homes.
2. Materials and Methods
2.1. Design
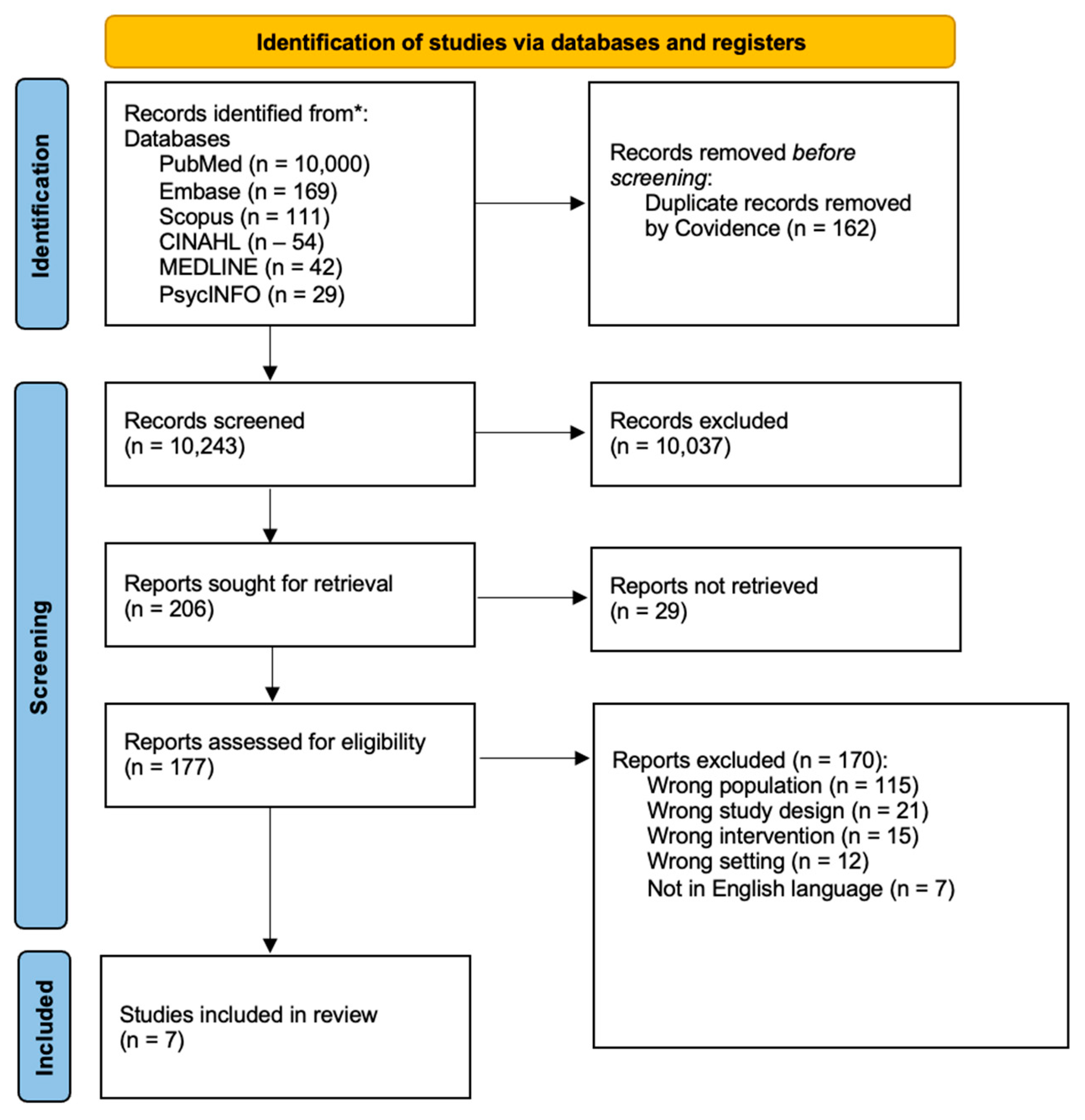
2.2. Search Strategy
2.3. Eligibility Criteria
2.4. Data Extraction
2.5. Data Analysis
3. Results
3.1. Characteristics of Included Studies
3.2. Quality Appraisal
3.3. Study Results
3.3.1. Theme One: Improvements in PD Knowledge and Confidence
3.3.2. Theme Two: Improvements in Care Practices and Outcomes
3.3.3. Theme Three: Lack of Specialist PD Education
3.3.4. Theme Four: The Incorporation of Communication Training
4. Discussion
4.1. Relevance to Nursing Practice
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
Guidelines and Standards Statement
Use of Artificial Intelligence
Acknowledgments
Conflicts of Interest
References
- DeMaagd, G.; Philip, A. Parkinson’s Disease and Its Management. Pharm. Ther. 2015, 40, 504–532. [Google Scholar]
- Ou, Z.; Pan, J.; Tang, S.; Duan, D.; Yu, D.; Nong, H.; Wang, Z. Global Trends in the Incidence, Prevalence, and Years Lived With Disability of Parkinson’s Disease in 204 Countries/Territories From 1990 to 2019. Front. Public Health 2021, 9, 776–847. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation (WHO). Parkinson Disease. Available online: https://www.who.int/news-room/fact-sheets/detail/parkinson-disease (accessed on 19 September 2024).
- National Institute for Health and Care Excellence (NICE). Parkinson’s Disease: How Common Is It? Available online: https://cks.nice.org.uk/topics/parkinsons-disease/background-information/prevalence/ (accessed on 29 September 2024).
- Reeve, A.; Simcox, E.; Turnbull, D. Ageing and Parkinson’s disease: Why is advancing age the biggest risk factor? Ageing Res. Rev. 2014, 14, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Nihtilä, E.K.; Martikainen, P.T.; Koskinen, S.V.P.; Reunanen, A.R.; Noro, A.M.; Häkkinen, U.T. Chronic conditions and the risk of long-term institutionalization among older people. Eur. J. Public Health 2008, 18, 77–84. [Google Scholar] [CrossRef]
- Salminen, M.; Vire, J.; Viikari, L.; Vahlberg, T.; Isoaho, H.; Lehtonen, A.; Viitanen, M.; Arve, S.; Eloranta, S. Predictors of institutionalization among home-dwelling older Finnish people: A 22-year follow-up study. Aging Clin. Exp. Res. 2017, 29, 499–505. [Google Scholar] [CrossRef]
- Weerkamp, N.J.; Tissingh, G.; Poels, P.J.E.; Zuidema, S.U.; Munneke, M.; Koopmans, R.T.C.M.; Bloem, B.R. Parkinson Disease in Long Term Care Facilities: A Review of the Literature. J. Am. Med. Dir. Assoc. 2014, 15, 90–94. [Google Scholar] [CrossRef]
- Hosking, A.; Hommel, A.A.L.J.; Lorenzl, S.; Coelho, M.; Ferreira, J.J.; Meissner, W.G.; Odin, P.; Bloem, B.R.; Dodel, R.; Schrag, A. Characteristics of Patients with Late-Stage Parkinsonism Who are Nursing Home Residents Compared with those Living at Home. J. Am. Med. Dir. Assoc. 2021, 22, 440–445.e2. [Google Scholar] [CrossRef]
- Copeland, S.; Anderson, T.; Carter, G.; Brown Wilson, C.; Stark, P.; Doumas, M.; Rodger, M.; O’Shea, E.; Creighton, L.; Craig, S.; et al. Experiences of People Living with Parkinson’s Disease in Care Homes: A Qualitative Systematic Review. Nurs. Rep. 2024, 14, 428–443. [Google Scholar] [CrossRef]
- Radder, D.L.M.; De Vries, N.M.; Riksen, N.P.; Diamond, S.J.; Gross, D.; Gold, D.R.; Heesakkers, J.; Henderson, E.; Hommel, A.L.A.J.; Lennaerts, H.H.; et al. Multidisciplinary care for people with Parkinson’s disease: The new kids on the block! Expert Rev. Neurother. 2019, 19, 145–157. [Google Scholar] [CrossRef]
- Fugita, T.; Iwaki, M.; Hatono, Y. The role of nurses for patients with Parkinson’s disease at home: A scoping review. BMC Nurs. 2024, 23, 318. [Google Scholar] [CrossRef]
- Sathyababu, R.; Chan, E.; Dhakam, Z. Management of Parkinson’s Disease medication in acutely admitted patients. BMJ Qual. Improv. Rep. 2012, 1, u473.w154. [Google Scholar] [CrossRef] [PubMed]
- Cohen, E.V.; Hagestuen, R.; González-Ramos, G.; Cohen, H.W.; Bassich, C.; Book, E.; Bradley, K.P.; Carter, J.H.; Di Minno, M.; Gardner, J.; et al. Interprofessional education increases knowledge, promotes team building, and changes practice in the care of Parkinson’s disease. Park. Relat. Disord. 2016, 22, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Crooks, S.; Stark, P.; Carlisle, S.; McMullan, J.; Copeland, S.; Wong, W.Y.A.; Blake, D.; Lyons, E.; Campbell, N.; Carter, G.; et al. Evaluation of a co-designed Parkinson’s awareness audio podcast for undergraduate nursing students in Northern Ireland. BMC Nurs. 2023, 22, 370. [Google Scholar] [CrossRef] [PubMed]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Davies, A. Carrying out systematic literature reviews: An introduction. Br. J. Nurs. 2019, 28, 1008–1014. [Google Scholar] [CrossRef]
- Bettany-Saltikov, J.; McSherry, R. How To Do a Systematic Literature Review in Nursing: A Step-by-Step Guide, 3rd ed.; McGraw-Hill Education: New York, NY, USA, 2024; ISBN 978-0-335-25115-5. [Google Scholar]
- Barker, T.; Habibi, N.; Aromataris, E.; Stone, J.; Leonardi-Bee, J.; Sears, K.; Hasanoff, S.; Klugar, M.; Tufanaru, C.; Moola, S.; et al. The revised JBI critical appraisal tool for the assessment of risk of bias quasi-experimental studies. JBI Evid. Synth. 2024, 22, 378–388. [Google Scholar] [CrossRef]
- Clarke, V.; Braun, V. Thematic analysis. J. Posit. Psychol. 2017, 12, 297–298. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Ashraf, S.; Datta-Chaudhuri, M.; Chattopadhyay, T.; Ngoma, P.; Wardle, A.; Datta, A. Impact of care home education programme on the care home staff and their practice. Age Ageing 2012, 41, 16. [Google Scholar]
- Chenoweth, L.; Sheriff, J.; McAnally, L.; Tait, F. Impact of the Parkinson’s disease medication protocol program on nurses’ knowledge and management of Parkinson’s disease medicines in acute and aged care settings. Nurse Educ. Today 2013, 33, 458–464. [Google Scholar] [CrossRef] [PubMed]
- Makoutonina, M.; Iansek, R.; Simpson, P. Optimizing care of residents with Parkinsonism in supervised facilities. Park. Relat. Disord. 2010, 16, 351–355. [Google Scholar] [CrossRef] [PubMed]
- Oates, L.L.; Hand, A.; Walker, R.W.; Gray, W.K. Barriers to Providing Quality Care for People with Parkinson’s Living in Care Homes in the UK: The Role of Staff Training. In Proceedings of the 2016 International Congress, Berlin, Germany, 19–23 June 2016. [Google Scholar]
- Wong, A.L.; Luthra, N. Bridging the gaps in Parkinson’s education for nurses in long term care facilities. J. Park. Dis. 2019, 9, 199. [Google Scholar]
- Eriksson, K.; Forsgren, E.; Hartelius, L.; Saldert, C. Communication partner training of enrolled nurses working in nursing homes with people with communication disorders caused by stroke or Parkinson’s disease. Disabil. Rehabil. 2016, 38, 187–203. [Google Scholar] [CrossRef] [PubMed]
- Coles, R.; Lester, R.; Bryan, K.; Maxim, J.; Jordan, L.; Kerr, J.; Rudd, T. Coping with communication disability in residential care. Int. J. Lang. Commun. Disord. 1995, 30, 384–388. [Google Scholar] [CrossRef]
- Bloem, B.R.; Henderson, E.J.; Dorsey, E.R.; Okun, M.S.; Okubadejo, N.; Chan, P.; Andrejack, J.; Darweesh, S.K.; Munneke, M. Integrated and patient-centred management of Parkinson’s disease: A network model for reshaping chronic neurological care. Lancet Neurol. 2020, 19, 623–634. [Google Scholar] [CrossRef]
- Bartlett, G.; Blais, R.; Tamblyn, R.; Clermont, R.J.; MacGibbon, B. Impact of patient communication problems on the risk of preventable adverse events in acute care settings. CMAJ 2008, 178, 1555–1562. [Google Scholar] [CrossRef]
- Pitts, E.; Wylie, K.; Loftus, A.M.; Cocks, N. Communication strategies used by Parkinson’s nurse specialists during healthcare interactions: A qualitative descriptive study. J. Adv. Nurs. 2022, 78, 1773–1786. [Google Scholar] [CrossRef]
- Carapellotti, A.M.; Stevenson, R.; Doumas, M. The efficacy of dance for improving motor impairments, non-motor symptoms, and quality of life in Parkinson’s disease: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0236820. [Google Scholar] [CrossRef]
- Fischer, F.; Helmer, S.; Rogge, A.; Arraras, J.I.; Buchholz, A.; Hannawa, A.; Horneber, M.; Kiss, A.; Rose, M.; Söllner, W.; et al. Outcomes and outcome measures used in evaluation of communication training in oncology—A systematic literature review, an expert workshop, and recommendations for future research. BMC Cancer 2019, 19, 808. [Google Scholar] [CrossRef]
- Smith, K.M.; Caplan, D.N. Communication impairment in Parkinson’s disease: Impact of motor and cognitive symptoms on speech and language. Brain Lang. 2018, 1, 38–46. [Google Scholar] [CrossRef]
- Crooks, S.; Mitchell, G.; Wynne, L.; Carter, G. Exploring the stigma experienced by people affected by Parkinson’s disease: A systematic review. BMC Public Health 2025, 25, 25. [Google Scholar] [CrossRef]

{kind=link}
| Population | Residential homes OR residential home OR Nursing homes OR nursing home OR Long term care facilities OR long-term care facility OR care home OR care homes OR aged care facility OR care home staff OR nursing home staff OR residential home staff |
| Exposure | Parkinsons OR Parkinson’s Disease OR Parkinsonian, Parkinsonian OR PD OR Progressive Supranuclear Palsy OR Multiple System Atrophy OR Corticobasal Degeneration OR Parkinson OR Movement Disorder |
| Outcome | Education OR Educational Activities OR Nursing Education OR Training OR Self-Directed Learning OR E-Learning OR Learning OR Staff Training OR CPD OR Continuing Professional Development OR educational intervention OR online education OR staff education OR staff development |
| Inclusion | Exclusion | |
|---|---|---|
| Study Characteristics | Empirical studies Literature reviews English language | |
| Population | Care home settings and staff (residential homes, nursing homes, long-term care facilities, aged care facilities, care homes) | Hospital settings, community settings other than care homes |
| Exposure | Parkinson’s disease, Parkinsonism, or movement disorders | |
| Outcome | Training, education, development, learning |
| Authors | Title | Sample Size | Age | Gender | Professional Background |
|---|---|---|---|---|---|
| Ashraf et al., 2012 [23] | Impact of Care Home Education Program on the Care Home Staff and their Practice | 15 | Not provided | Not provided | Care home staff (not specified if RN or social care staff) |
| Chenoweth et al., 2013 [24] | Impact of the PD medication protocol program on nurses’ knowledge and management of PD medicines in acute and aged care settings | 127 | 18–24—2% 25–34—17% 35–44—14% 45–54—35% 55+—32% | Female—95% Male—5% | RN: 67%; director of nursing: 1%; deputy director of nursing: 2%; clinical nurse specialist: 2%; nursing unit manager: 1%; enrolled nurse/trainee enrolled nurse: 2%; nurse assistant: 25% |
| Coles et al., 1995 [29] | Coping with communication disability in residential care | 150 | Not provided | Not provided | Social care staff |
| Eriksson et al., 2016 [28] | Communication partner training of enrolled nurses working in nursing homes with people with communication disorders caused by stroke or PD | 1 | 45 years old | Female | Enrolled Nurse in nursing home with 5 months experience caring for a person with communication difficulties related to PD |
| Makoutonina et al., 2010 [25] | Optimizing care for residents with Parkinsonism in supervised facilities | 118 | Not provided | Not provided | Residential facility staff |
| Oates et al., 2016 [26] | Barriers to providing quality care for people with Parkinson’s living in care homes in the UK: The role of staff training | 53 care home staff | Not provided | Not provided | Care home staff (not specified if RN or social care staff) |
| Wong and Luthra, 2019 [27] | Bridging the gaps in Parkinson’s education for nurses in long term care facilities | Not provided | Not provided | Not provided | Registered nurses in long-term care |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Finlay, S.; Anderson, T.; Henderson, E.; Wilson, C.B.; Stark, P.; Carter, G.; Rodger, M.; Doumas, M.; O’Shea, E.; Creighton, L.; et al. A Scoping Review of Educational and Training Interventions on Parkinson’s Disease for Staff in Care Home Settings. Nurs. Rep. 2025, 15, 20. https://doi.org/10.3390/nursrep15010020
Finlay S, Anderson T, Henderson E, Wilson CB, Stark P, Carter G, Rodger M, Doumas M, O’Shea E, Creighton L, et al. A Scoping Review of Educational and Training Interventions on Parkinson’s Disease for Staff in Care Home Settings. Nursing Reports. 2025; 15(1):20. https://doi.org/10.3390/nursrep15010020
Chicago/Turabian StyleFinlay, Stacey, Tara Anderson, Elizabeth Henderson, Christine Brown Wilson, Patrick Stark, Gillian Carter, Matthew Rodger, Mihalis Doumas, Emma O’Shea, Laura Creighton, and et al. 2025. "A Scoping Review of Educational and Training Interventions on Parkinson’s Disease for Staff in Care Home Settings" Nursing Reports 15, no. 1: 20. https://doi.org/10.3390/nursrep15010020
APA StyleFinlay, S., Anderson, T., Henderson, E., Wilson, C. B., Stark, P., Carter, G., Rodger, M., Doumas, M., O’Shea, E., Creighton, L., Craig, S., Crooks, S., Gillis, A., & Mitchell, G. (2025). A Scoping Review of Educational and Training Interventions on Parkinson’s Disease for Staff in Care Home Settings. Nursing Reports, 15(1), 20. https://doi.org/10.3390/nursrep15010020