

Pilot Study of SATELLITE Education on Nurses’ Knowledge and Confidence toward Assessing and Caring for Female Victims of Sexual Violence

 , ,
, ,
Abstract
1. Background
2. Method
2.1. Design
2.2. Setting and Sample
2.3. Instruments
2.3.1. SATELLITE Education Program
2.3.2. SATELLITE Knowledge/Confidence Instrument
2.4. Data Collection
2.5. Data Analysis
2.6. Procedure and Ethical Considerations
3. Results
3.1. Feasibility: Can the SATELLITE Education Program Be Implemented as Planned? Is the Instrument Reliable?
3.2. Acceptability: Will Key Stakeholders Embrace the Education?
3.3. Efficacy: Does the Education Produce the Desired Effects on RNs’ Knowledge and Confidence in SV Assessment and Care Provision for SV Victims?
3.4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
Guidelines and Standards Statement
Use of Artificial Intelligence
Conflicts of Interest
References
- Rape, Abuse, & Incest National Network. Types of Sexual Violence; Rape, Abuse, & Incest National Network: Washington, DC, USA, 2024; Available online: https://www.rainn.org/types-sexual-violence#:~:text=The%20term%20%22sexual%20violence%22%20is,vary%20from%20state%20to%20state (accessed on 4 May 2024).
- Centers for Disease Control and Prevention. Fast Facts: Preventing Sexual Violence; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2022. Available online: https://www.cdc.gov/violenceprevention/sexualviolence/fastfact.html#:~:text=Sexual%20violence%20is%20sexual%20activity,experience%20or%20perpetrate%20sexual%20violence (accessed on 4 May 2024).
- International Justice Mission. The Problem: Sexual Violence; International Justice Mission: Washington, DC, USA, 2024; Available online: https://www.ijm.org/our-work/violence-women-children/sexual-violence (accessed on 4 May 2024).
- World Health Organization. Devastatingly Pervasive: 1 in 3 Women Globally Experience Violence; World Health Organization: Geneva, Switzerland, 2021; Available online: https://www.who.int/news/item/09-03-2021-devastatingly-pervasive-1-in-3-women-globally-experience-violence (accessed on 4 May 2024).
- Rape, Abuse, & Incest National Network. Victims of Sexual Violence: Statistics; Rape, Abuse, & Incest National Network: Washington, DC, USA, 2024; Available online: https://www.rainn.org/statistics/victims-sexual-violence (accessed on 4 May 2024).
- Ross, R.; Stidham, A.W.; Saenyakul, P.; Creswell, J.W. Intimate partner violence, emotional support, and health outcomes among Thai women: A mixed methods study. J. R. Thai Army Nurses 2015, 16, 14–24. Available online: https://he01.tci-thaijo.org/index.php/JRTAN/article/view/35131 (accessed on 4 May 2024).
- Leemis, R.W.; Friar, N.; Khatiwada, S.; Chen, M.S.; Kresnow, M.; Smith, S.G.; Caslin, S.; Basile, K.C. The National Intimate Partner and Sexual Violence Survey: 2016/2017 Report on Intimate Partner Violence; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2022. Available online: https://www.cdc.gov/violenceprevention/pdf/nisvs/nisvsreportonipv_2022.pdf (accessed on 4 May 2024).
- Farahi, N.; McEachern, M. Sexual assault of women. Am. Fam. Physician 2021, 103, 168–176. Available online: https://www.aafp.org/pubs/afp/issues/2021/0201/p168.html (accessed on 4 May 2024). [PubMed]
- Peterson, C.; DeGue, S.; Florence, C.; Lokey, C. Lifetime economic burden of rape among U.S. adults. Am. J. Prev. Med. 2017, 52, 691–701. [Google Scholar] [CrossRef] [PubMed]
- Hailes, H.P.; Yu, R.; Danese, A.; Fazel, S. Long-term outcomes of childhood sexual abuse: An umbrella review. Lancet Psychiatry 2019, 6, 830–839. [Google Scholar] [CrossRef] [PubMed]
- Holliday, R.; Nichter, B.; Holder, N.; Hill, M.L.; Monteith, L.L.; Norman, S.B.; Pietrzak, R.H. Childhood sexual abuse and military sexual trauma interact to increase suicide risk: Results from a nationally representative veteran sample. J. Interpers. Violence 2023, 38, 5354–5369. [Google Scholar] [CrossRef] [PubMed]
- Strizzi, J.M.; Mortensen, E.L.; Hegelund, E.R.; Wimmelmann, C.L.; Folker, A.P.; Flensborg-Madsen, T. Experience of sexual violence and satisfaction with life: A 20-year prospective cohort study. J. Sex. Aggress. 2022, 28, 316–330. [Google Scholar] [CrossRef]
- Letourneau, E.J.; Brown, D.S.; Fang, X.; Hassan, A.; Mercy, J.A. The economic burden of child sexual abuse in the United States. Child Abus. Negl. 2018, 79, 413–422. [Google Scholar] [CrossRef] [PubMed]
- The National Academies of Sciences, Engineering, and Medicine. The Future of Nursing 2020–2030: Charting a Path to Achieve Health Equity; The National Academies Press: Washington, DC, USA, 2021. [Google Scholar] [CrossRef]
- American Nurses Association. Nursing: Scope and Standards of Practice, 4th ed.; American Nurses Association, Nursing Knowledge Center: Silver Spring, MD, USA, 2021; Available online: https://www.nursingworld.org/nurses-books/nursing-scope-and-standards-of-practice-4th-edit/ (accessed on 4 May 2024).
- ACOG Committee Opinion No. 777: Sexual Assault. Obstet. Gynecol. 2019, 133, e296–e302. [CrossRef] [PubMed]
- Baird, K.; Creedy, D.K.; Saito, A.S.; Eustace, J. Longitudinal evaluation of a training program to promote routine antenatal enquiry for domestic violence by midwives. Women Birth 2018, 31, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Poreddi, V.; Gandhi, S.; Reddy, S.N.; Palaniappan, M.; BadaMath, M. Effectiveness of nurses training in routine screening of violence against women with mental illness: A randomized controlled trail. Arch. Psychiatr. Nurs. 2020, 3, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Miller, C.J.; Adjognon, O.L.; Brady, J.E.; Dichter, M.E.; Iverson, K.M. Screening for intimate partner violence in healthcare settings: An implementation-oriented systematic review. Implement. Res. Pract. 2021, 2. [Google Scholar] [CrossRef] [PubMed]
- Basile, K.C.; Hertz, M.F.; Back, S.E. Intimate Partner Violence and Sexual Violence Victimization Assessment Instruments for Use in Healthcare Settings: Version 1; Centers for Disease Control and Prevention, National Center for Injury Prevention and Control: Atlanta, GA, USA, 2016. [Google Scholar]
- Tavrow, P.; Bloom, B.E.; Withers, M.H. Intimate partner violence screening practices in California after passage of the Affordable Care Act. Violence Against Women 2017, 23, 871–886. [Google Scholar] [CrossRef] [PubMed]
- Feder, G.; Ramsay, J.; Dunne, D.; Rose, M.; Arsene, C.; Norman, R.; Kuntze, S.; Spencer, A.; Bacchus, L.; Hague, G.; et al. How far does screening women for domestic (partner) violence in different health-care settings meet criteria for a screening programme? Systematic reviews of nine UK National Screening Committee criteria. Health Technol. Assess. 2009, 13, 1–349. [Google Scholar] [CrossRef] [PubMed]
- O’doherty, L.J.; Taft, A.; Hegarty, K.; Ramsay, J.; Davidson, L.L.; Feder, G. Screening women for intimate partner violence in health care settings: Abridged Cochrane systematic review and meta-analysis. BMJ 2014, 348, 2913. [Google Scholar] [CrossRef] [PubMed]
- Ross, R.; Draucker, C.B.; Martsolf, D.; Adamle, K.; Chiang-Hanisko, L.; Lewandowski, W. The bridge: Providing nursing care for survivors of sexual violence. J. Am. Acad. Nurse Pract. 2010, 22, 361–368. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Physician Assistants. PA Training and Skills to Work with Survivors of Sexual Violence: Trends and Implications for PAs. 2020. Available online: https://www.aapa.org/wp-content/uploads/2020/04/PA-Training-and-Skills-to-Work-With-Survivors-of-Sexual-Violence.pdf (accessed on 4 May 2024).
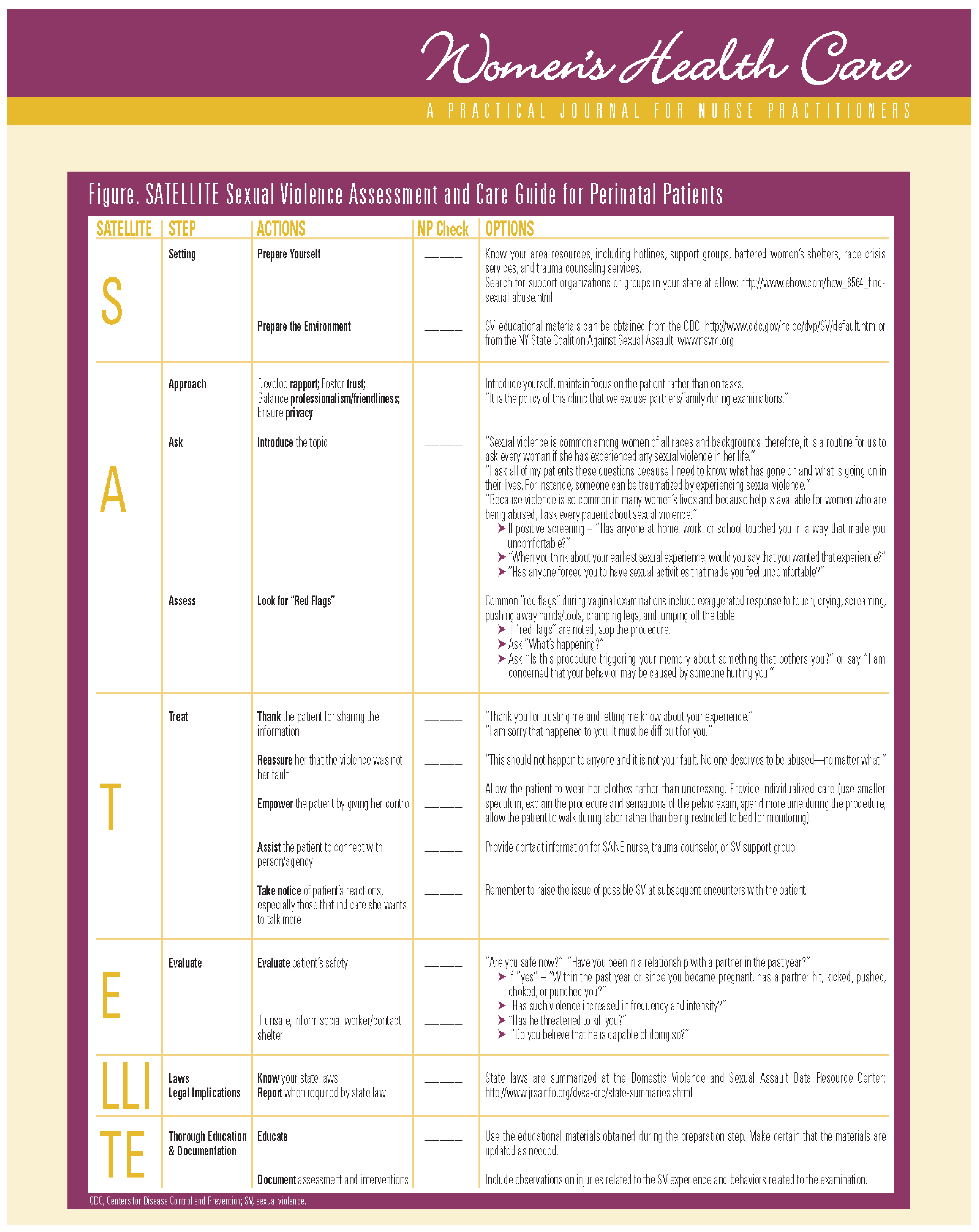
- Ross, R.; Roller, C.; Rusk, T.; Martsolf, D.; Draucker, C. The SATELLITE sexual violence assessment and care guide for perinatal patients. Women’s Health Care 2009, 8, 25–31. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3324818/ (accessed on 4 May 2024).
- Cash, J.C.; Glass, C.A. (Eds.) Adult-Gerontology Practice Guidelines; Springer: Berlin/Heidelberg, Germany, 2023. [Google Scholar] [CrossRef]
- Cash, J.C.; Glass, C.A. (Eds.) Family Practice Guidelines, 4th ed.; Springer Publishing Company, LLC.: New York, NY, USA, 2017. [Google Scholar]
- Ward, S.L.; Hisley, S.M.; Kennedy, A.M. (Eds.) Maternal-Child Nursing Care: Optimizing Outcomes for Mothers, Children, and Families, 2nd ed.; F.A. Davis Company: Philadelphia, PA, USA, 2015. [Google Scholar]
- Centers for Disease Control and Prevention. Understanding the Training of Trainers Model; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2019. Available online: https://www.cdc.gov/healthyschools/tths/train_trainers_model.htm (accessed on 4 May 2024).
- Knowles, M. The Adult Learners: A Neglected Species; Gulf Publishing: Houston, TX, USA, 1990. [Google Scholar]
- New England Institute of Technology. What Is Adult Learning Theory? New England Institute of Technology: East Greenwich, RI, USA, 2021; Available online: https://www.neit.edu/blog/what-is-adult-learning-theory (accessed on 4 May 2024).
- Strangroom, J. Social Science Statistics Effect Size Calculator for T-test. 2021. Available online: https://www.socscistatistics.com/effectsize/default3.aspx (accessed on 4 May 2024).
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis, 7th ed.; Prentice Hall: Englewood Cliffs, NJ, USA, 2010. [Google Scholar]
- Centers for Disease Control and Prevention. Training Effectiveness; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2021. Available online: https://www.cdc.gov/training/development/evaluate/training-effectiveness.html (accessed on 4 May 2024).
- Centers for Disease Control and Prevention. Violence Prevention: Preventing Sexual Violence; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2020. Available online: https://www.cdc.gov/violenceprevention/sexualviolence/fastfact.html#:~:text=Sexual%20violence%20is%20sexual%20activity,experience%20or%20perpetrate%20sexual%20violence (accessed on 4 May 2024).
- Ramsey, J.; Rivas, C.; Feder, G. Interventions to Reduce Violence and Promote the Physical and Psychosocial Well-Being of Women Who Experience Partner Abuse: A Systematic Review of Controlled Evaluations; Department of Health: London, UK, 2005; Available online: https://www.endvawnow.org/uploads/browser/files/Interventions%20to%20Reduce%20Violence.pdf (accessed on 4 May 2024).

{kind=link}
| Item | Before M (SD) | After | t | p | Cohen-d |
|---|---|---|---|---|---|
| 1. I know how to screen for my patients’ sexual violence experiences. | 3.38 (1.06) | 4.50 (0.53) | 3.22 | 0.015 ** | 1.34 (large) |
| 2. I know where to look for sexual violence support organizations or groups in my geographical area. | 3.25 (1.03) | 4.75 (0.46) | 3.97 | 0.005 ** | 1.56 (large) |
| 3. I know where to retrieve sexual violence educational materials. | 3.25 (0.88) | 4.88 (0.35) | 5.02 | 0.002 ** | 2.41 (large) |
| 4. I can introduce sexual violence topics to my patients. | 3.63 (1.06) | 4.38 (0.51) | 2.39 | 0.048 ** | 0.90 (large) |
| 5. I can care for patients who have experienced sexual violence. | 3.75 (1.28) | 4.13 (0.64) | 1.16 | 0.285 | 0.37 (~towards medium) |
| 6. I know what “red flags” are for patients who have experienced sexual violence. | 3.25 (1.03) | 4.38 (0.51) | 3.81 | 0.007 ** | 1.37 (large) |
| 7. I know what to say or do when my patients reveal their sexual violence experiences. | 3.31 (1.16) | 4.25 (0.46) | 2.62 | 0.034 * | 1.07 (large) |
| 8. I know how to evaluate my patients’ safety after they reveal their sexual violence experiences. | 3.50 (1.19) | 4.25 (0.70) | 1.82 | 0.111 | 0.76 (~large) |
| 9. I know my state laws and regulations related to sexual violence. | 2.88 (0.64) | 4.00 (0.75) | 3.21 | 0.015 * | 1.61 (large) |
| 10. I know how to educate my patients about sexual violence. | 3.00 (1.06) | 4.25 (0.462) | 3.04 | 0.019 * | 1.52 (large) |
| 11. I know how to document my patients’ sexual violence experiences. | 3.13 (0.99) | 4.25 (0.70) | 4.97 | 0.002 ** | 1.31 (large). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ross, R.; Sheppard, F.H.; Almotairy, M.M.; Hirst, J.; Jenkins, M. Pilot Study of SATELLITE Education on Nurses’ Knowledge and Confidence toward Assessing and Caring for Female Victims of Sexual Violence. Nurs. Rep. 2024, 14, 1287-1296. https://doi.org/10.3390/nursrep14020097
Ross R, Sheppard FH, Almotairy MM, Hirst J, Jenkins M. Pilot Study of SATELLITE Education on Nurses’ Knowledge and Confidence toward Assessing and Caring for Female Victims of Sexual Violence. Nursing Reports. 2024; 14(2):1287-1296. https://doi.org/10.3390/nursrep14020097
Chicago/Turabian StyleRoss, Ratchneewan, Francine Hebert Sheppard, Monir M. Almotairy, Joelle Hirst, and Marjorie Jenkins. 2024. "Pilot Study of SATELLITE Education on Nurses’ Knowledge and Confidence toward Assessing and Caring for Female Victims of Sexual Violence" Nursing Reports 14, no. 2: 1287-1296. https://doi.org/10.3390/nursrep14020097
APA StyleRoss, R., Sheppard, F. H., Almotairy, M. M., Hirst, J., & Jenkins, M. (2024). Pilot Study of SATELLITE Education on Nurses’ Knowledge and Confidence toward Assessing and Caring for Female Victims of Sexual Violence. Nursing Reports, 14(2), 1287-1296. https://doi.org/10.3390/nursrep14020097