
Factors Related to the Willingness of People with Mental Health Illnesses Living in Group Homes to Disclose Their Illness to Supporters during Disaster Evacuation: A Cross-Sectional Study


Abstract
1. Introduction
2. Materials and Methods
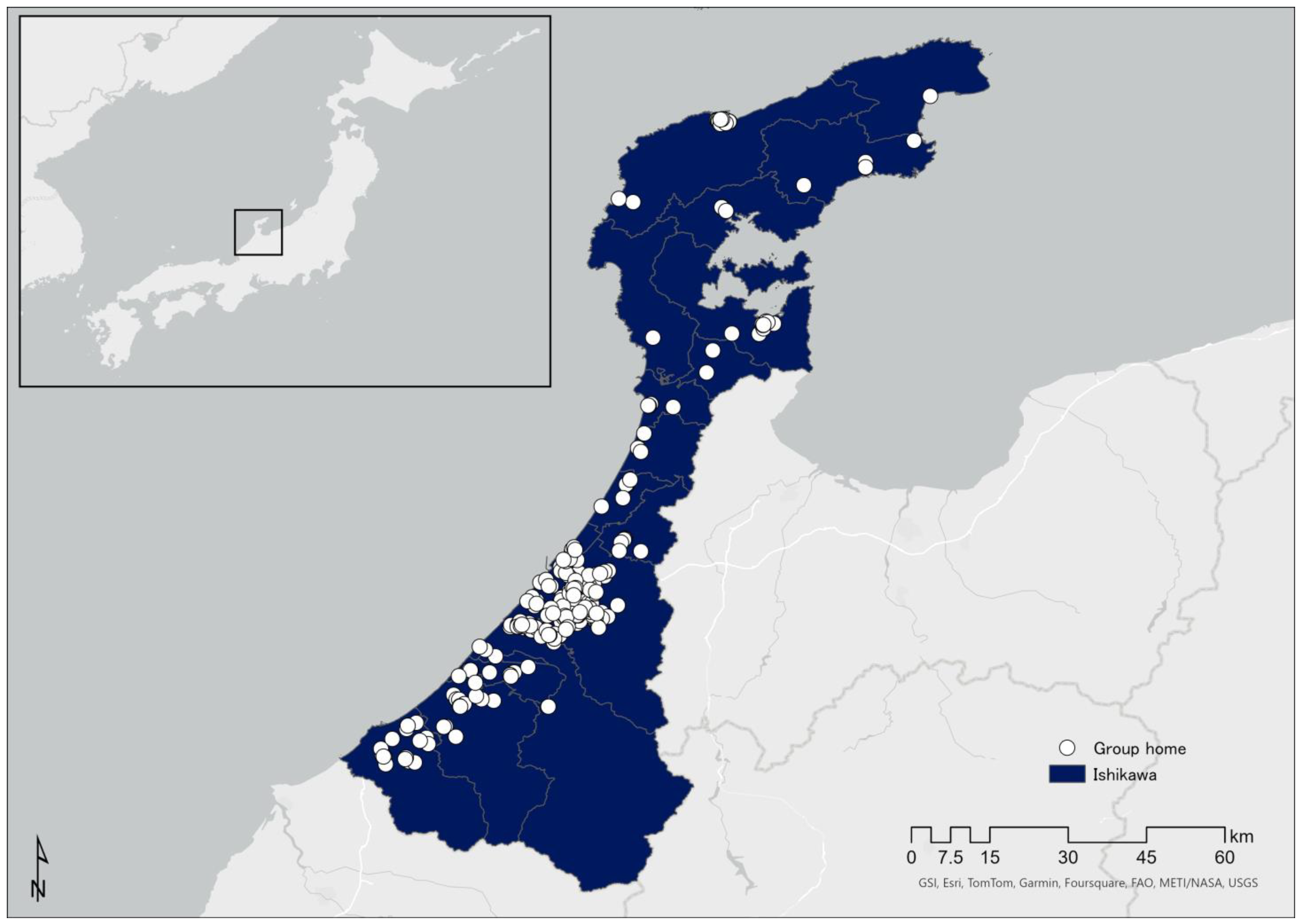
2.1. Research Location
2.2. Data Collection
2.3. Survey Contents
2.3.1. Participant Background Information
2.3.2. Services Used by Participating PMHI
2.3.3. Where Participants Lived before Hospitalization
2.3.4. Where Participants Obtained Information to Make Evacuation Decisions
2.3.5. Participants’ Typical Socializing Patterns
2.3.6. Assumptions about Evacuation from a Disaster
2.4. Analysis
2.5. Ethical Considerations
3. Results
3.1. Characteristics of Participants
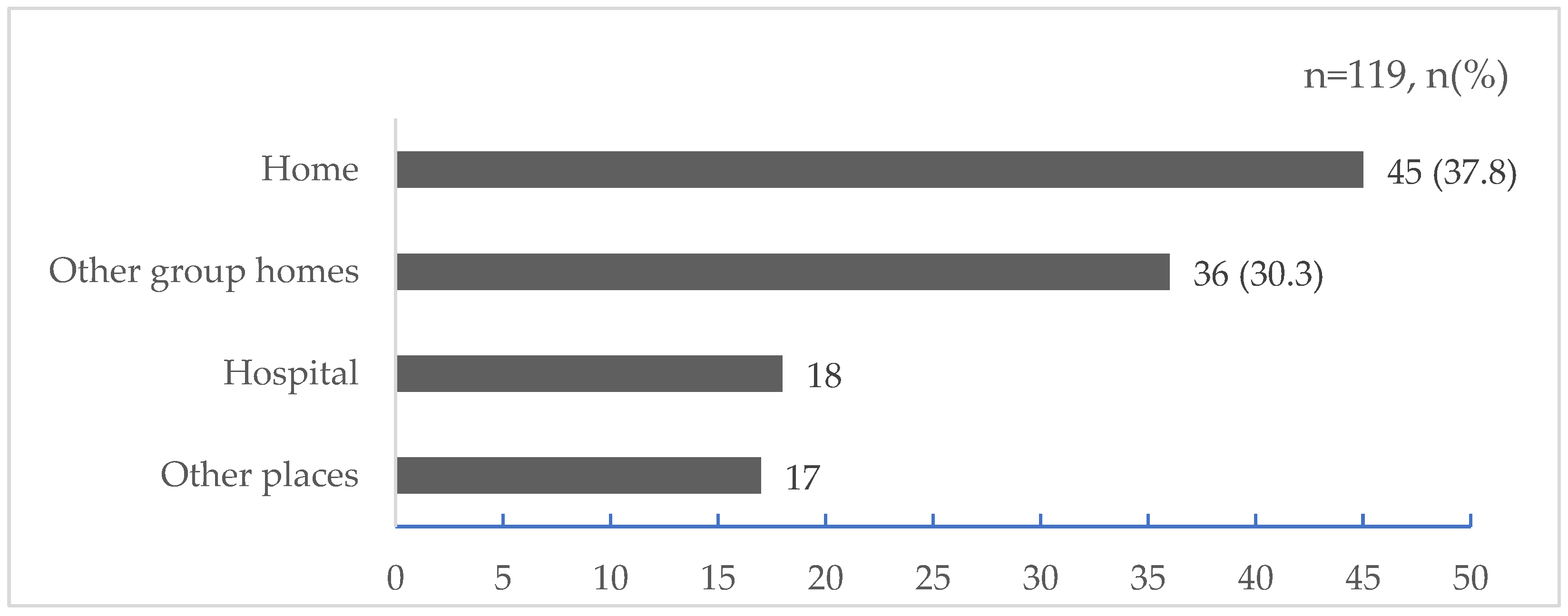
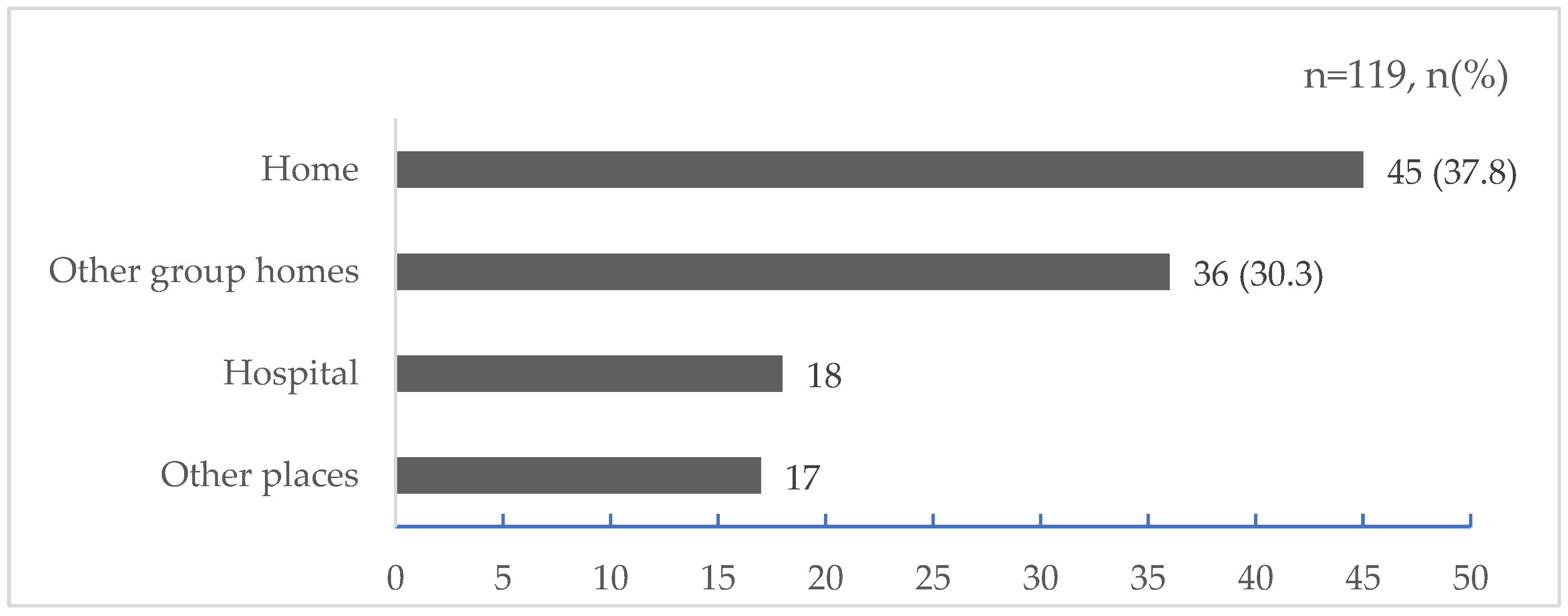
3.2. Whereabouts before Hospitalization
3.3. Sources of Information for Evacuation Decisions
3.4. Results of Cross-Tabulation of Responses to Each Item and “Disclosed My Illness to Supporters after the Evacuation”
3.5. Binary Logistic Regression Analysis Indicated Factors Associated with the Willingness to “Disclose My Illness to Supporters after Evacuation during a Disaster”
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
Guidelines and Standards Statement
Use of Artificial Intelligence
Acknowledgments
Conflicts of Interest
References
- Ministry of Health, Labour and Welfare Community Living Support Service Standards and Medical Fees. Available online: https://www.mhlw.go.jp/content/12401000/000670104.pdf (accessed on 15 November 2023). (In Japanese).
- Ministry of Health, Labour and Welfare Housing Support for People with Disabilities. Available online: https://www.mhlw.go.jp/content/12601000/000851065.pdf (accessed on 15 November 2023). (In Japanese).
- Enomoto, N.; Tsuzuki, S. Administration and Aging Problem of the Mentally–Disabled Person Group Home. J. Tokyo Online Univ. 2023, 5, 1–12. Available online: https://cir.nii.ac.jp/crid/1050858608274587264 (accessed on 31 March 2023).
- Ono, Y. A Study of Preferable Way of Community Care for Awareness of Aging of the Mental Disorders–From a Factfinding Survey of Users of Group Homes for the Mental Disorders. Bull. Tohoku Fukushi Univ. 2021, 45, 115–142. Available online: https://tfulib.repo.nii.ac.jp/records/786 (accessed on 18 March 2023). (In Japanese).
- Teruyuki, K. Quasi-Stationary Band-Shaped Precipitation Systems, Named “Senjo-Kousuitai”, Causing Localized Heavy Rainfall in Japan. J. Meteorol. Soc. Jpn. 2020, 98, 485–509. [Google Scholar] [CrossRef]
- Mori, N.; Takemi, T.; Tachikawa, Y.; Tatano, H.; Shimura, T.; Tanaka, T.; Fujimi, T.; Osakada, Y.; Webb, A.; Nakakita, E. Recent Nationwide Climate Change Impact Assessments of Natural Hazards in Japan and East Asia. Weather Clim. Extrem. 2021, 32, 100309. [Google Scholar] [CrossRef]
- Norris, F.H.; Friedman, M.J.; Watson, P.J.; Byrne, C.M.; Diaz, E.; Kaniasty, K. 60,000 Disaster Victims Speak: Part I. An Empirical Review of the Empirical Literature, 1981—2001. Psychiatry 2002, 65, 207–239. [Google Scholar] [CrossRef]
- Kessler, R.C.; McLaughlin, K.A.; Koenen, K.C.; Petukhova, M.; Hill, E.D. The Importance of Secondary Trauma Exposure for Post-Disaster Mental Disorder. Epidemiol. Psychiatr. Sci. 2012, 21, 35–45. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3465701/ (accessed on 16 October 2023). [CrossRef]
- Lancet, T. Can We End Stigma and Discrimination in Mental Health? Lancet 2022, 400, 1381. [Google Scholar] [CrossRef]
- Makwana, N. Disaster and Its Impact on Mental Health: A Narrative Review. J. Fam. Med. Prim. Care 2019, 8, 3090–3095. [Google Scholar] [CrossRef] [PubMed]
- Blake, D.; Pooley, S.; Lyons, A. Stigma and Disaster Risk Reduction among Vulnerable Groups: Considering People Receiving Opioid Substitution Treatment. Int. J. Disaster Risk Reduct. 2020, 48, 101588. [Google Scholar] [CrossRef]
- Rowe, O.; Nadkarni, A. Barriers and Facilitators to the Implementation of Mental Health and Psychosocial Support Programmes Following Natural Disasters in Developing Countries: A Systematic Review. Glob. Ment. Health 2023, 11, e5. [Google Scholar] [CrossRef]
- Schnall, A.H.; Hanchey, A.; Nakata, N.; Wang, A.; Jeddy, Z.; Alva, H.; Tan, C.; Boehmer, T.; Bayleyegn, T.; Casey-Lockyer, M. Disaster-Related Shelter Surveillance During the Hurricane Harvey Response–Texas 2017. Disaster Med. Public Health Prep. 2020, 14, 49–55. [Google Scholar] [CrossRef]
- Hori, A.; Sawano, T.; Nonaka, S.; Tsubokura, M. How to Deal With the Risk of Evacuation of Psychiatric Hospital in Nuclear Disaster: A Case Study. Disaster Med. Public Health Prep. 2023, 17, e332. [Google Scholar] [CrossRef]
- Mao, W.; Agyapong, V.I.O. The Role of Social Determinants in Mental Health and Resilience after Disasters: Implications for Public Health Policy and Practice. Front. Public Health 2021, 9. Available online: https://www.frontiersin.org/articles/10.3389/fpubh.2021.658528 (accessed on 16 October 2023). [CrossRef]
- Sasaki, Y.; Aida, J.; Tsuji, T.; Koyama, S.; Tsuboya, T.; Saito, T.; Kondo, K.; Kawachi, I. Pre-Disaster Social Support Is Protective for Onset of Post-Disaster Depression: Prospective Study from the Great East Japan Earthquake & Tsunami. Sci. Rep. 2019, 9, 19427. [Google Scholar] [CrossRef]
- North, C.S.; Pfefferbaum, B. Mental Health Response to Community Disasters: A Systematic Review. JAMA 2013, 310, 507–518. [Google Scholar] [CrossRef]
- Joachim, G.; Acorn, S. Stigma of Visible and Invisible Chronic Conditions. J. Adv. Nurs. 2000, 32, 243–248. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare Building a Regional Comprehensive Care System for Mental disorders. Available online: https://www.mhlw.go.jp/content/12201000/000307970.pdf (accessed on 25 October 2023). (In Japanese).
- Mavrodieva, A.V.; Shaw, R. Disaster and Climate Change Issues in Japan’s Society 5.0—A Discussion. Sustainability 2020, 12, 1893. [Google Scholar] [CrossRef]
- O’Brien, G.; O’Keefe, P.; Rose, J.; Wisner, B. Climate Change and Disaster Management. Disasters 2006, 30, 64–80. [Google Scholar] [CrossRef]
- Ishikawa Prefecture Overview of Ishikawa Prefecture. Available online: https://www.pref.ishikawa.lg.jp/sabou/1gaiyou/index.html (accessed on 16 October 2023). (In Japanese).
- Ishikawa Prefecture Ishikawa Plan for People with Disabilities in 2019. Available online: https://www.pref.ishikawa.lg.jp/fukusi/oshirase/documents/plan2019_book.pdf (accessed on 23 October 2023). (In Japanese).
- Ishikawa Prefecture List of Designated Disability Welfare Service Providers in Ishikawa Prefecture. Available online: https://www.pref.ishikawa.lg.jp/fukusi/jiritsushienfukushi/jigyousyashiteiichiran.html (accessed on 13 November 2023). (In Japanese).
- Ministry of Health, Labour and Welfare, Health Labour Sciences Research Grant Life after the Earthquake for People with Severe Mental disorders. 2014. Available online: https://www.ncnp.go.jp/nimh/chiiki/research/01/doc/01_28.pdf (accessed on 25 October 2023). (In Japanese).
- Japan Broadcasting Corporation Information for People with Disabilities during Disasters. Available online: https://www.nhk.or.jp/heart-net/saigai/ (accessed on 16 October 2023). (In Japanese).
- Ministry of Health, Labour and Welfare Life of Disabled People Using Group Homes. 2019. Available online: https://www.mhlw.go.jp/content/12200000/000521823.pdf (accessed on 15 November 2023). (In Japanese).
- Nagayama, Y.; Nakai, H. Community-Based Integrated Care System for People with Mental Illness in Japan: Evaluating Location Characteristics of Group Homes to Determine the Feasibility of Daily Life Skill Training. Challenges 2022, 13, 38. [Google Scholar] [CrossRef]
- Sakurai, M.; Murayama, Y. Information Technologies and Disaster Management–Benefits and Issues. Prog. Disaster Sci. 2019, 2, 100012. [Google Scholar] [CrossRef]
- Zahra, K.; Imran, M.; Ostermann, F.O. Automatic Identification of Eyewitness Messages on Twitter during Disasters. Inf. Process. Manag. 2020, 57, 102107. [Google Scholar] [CrossRef]
- Ministry of Internal Affairs and Communications Information and Communication Report in 2016. Available online: https://www.soumu.go.jp/johotsusintokei/whitepaper/h28.html (accessed on 16 October 2023). (In Japanese).
- Weathernews [Disaster Mitigation Survey 2022] People Turn to Smartphones to Obtain Information during Disasters; Younger People Are More Likely to Avoid Television and Radio. Available online: https://jp.weathernews.com/news/39375 (accessed on 16 October 2023). (In Japanese).
- Kawasaki, H.; Takeuchi, M.; Rahman, M.M.; Yamashita, K. Residents’ Concerns Regarding Schools Designated as Evacuation Shelters. Disaster Med. Public Health Prep. 2022, 16, 1587–1593. [Google Scholar] [CrossRef] [PubMed]
- Itamiya, T. VR/AR and Its Application to Disaster Risk Reduction. In Emerging Technologies for Disaster Resilience: Practical Cases and Theories; Springer: Singapore; pp. 63–79. [CrossRef]
- Kobayashi, K.; Saitoh, T.; Yoshie, I.; Sasaki, M.; Hirasawa, N. Health Needs and Community-Based Nursing Practice after a Disaster. Available online: https://niconurs.repo.nii.ac.jp/records/589 (accessed on 16 October 2023). (In Japanese).
- Disaster Management In Japan 5th Review Meeting on Evacuation Support for Persons Requiring Assistance in the Event of Disasters/Responses Depending on the Characteristics of People Requiring Assistance during Disasters. Available online: https://www.bousai.go.jp/taisaku/hisaisyagyousei/youengosya/h24_kentoukai/5/4.pdf (accessed on 25 October 2023).
- Cabinet Office, Government of Japan Aggregation of Messages from People with Disabilities (Mental Disorder). Available online: https://www8.cao.go.jp/shougai/kou-kei/toujisha/siryo07.html (accessed on 16 October 2023). (In Japanese).
- Nistor, G.; Dumitru, C.-L. Preventing School Exclusion of Students with Autism Spectrum Disorder (ASD) through Reducing Discrimination: Sustainable Integration through Contact-Based Education Sessions. Sustainability 2021, 13, 7056. [Google Scholar] [CrossRef]
- Ran, M.-S.; Hall, B.J.; Su, T.T.; Prawira, B.; Breth-Petersen, M.; Li, X.-H.; Zhang, T.-M. Stigma of Mental Illness and Cultural Factors in Pacific Rim Region: A Systematic Review. BMC Psychiatry 2021, 21, 8. [Google Scholar] [CrossRef]
- Aguirre Velasco, A.; Cruz, I.S.S.; Billings, J.; Jimenez, M.; Rowe, S. What Are the Barriers, Facilitators and Interventions Targeting Help-Seeking Behaviours for Common Mental Health Problems in Adolescents? A Systematic Review. BMC Psychiatry 2020, 20, 293. [Google Scholar] [CrossRef] [PubMed]
- Thornicroft, G. Stigma and Discrimination Limit Access to Mental Health Care. Epidemiol. Psychiatr. Sci. 2008, 17, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Clement, S.; Schauman, O.; Graham, T.; Maggioni, F.; Evans-Lacko, S.; Bezborodovs, N.; Morgan, C.; Rüsch, N.; Brown, J.S.L.; Thornicroft, G. What Is the Impact of Mental Health-Related Stigma on Help-Seeking? A Systematic Review of Quantitative and Qualitative Studies. Psychol. Med. 2015, 45, 11–27. [Google Scholar] [CrossRef] [PubMed]
- Henderson, C.; Evans-Lacko, S.; Thornicroft, G. Mental Illness Stigma, Help Seeking, and Public Health Programs. Am. J. Public Health 2013, 103, 777–780. [Google Scholar] [CrossRef]
- Corrigan, P.W.; Watson, A.C. Understanding the Impact of Stigma on People with Mental Illness. World Psychiatry 2002, 1, 16–20. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1489832/ (accessed on 16 October 2023).
- Morgan, A.J.; Wright, J.; Reavley, N.J. Review of Australian Initiatives to Reduce Stigma towards People with Complex Mental Illness: What Exists and What Works? Int. J. Ment. Health Syst. 2021, 15, 10. [Google Scholar] [CrossRef]
- Mann, F.; Bone, J.K.; Lloyd-Evans, B.; Frerichs, J.; Pinfold, V.; Ma, R.; Wang, J.; Johnson, S. A Life Less Lonely: The State of the Art in Interventions to Reduce Loneliness in People with Mental Health Problems. Soc. Psychiatry Psychiatr. Epidemiol. 2017, 52, 627–638. [Google Scholar] [CrossRef] [PubMed]
- Koyama, S.; Dohi, M. A Study on the Actual Conditions of Local Communication in the Group Homes of Mental Disturbed Persons. J. City Plannning Inst. Jpn. 2000, 35, 31–36. [Google Scholar] [CrossRef]
- Hoffmann, R.; Blecha, D. Education and Disaster Vulnerability in Southeast Asia: Evidence and Policy Implications. Sustainability 2020, 12, 1401. [Google Scholar] [CrossRef]
- Ronoh, S.; Gaillard, J.C.; Marlowe, J. Children with Disabilities and Disaster Risk Reduction: A Review. Int. J. Disaster Risk Sci. 2015, 6, 38–48. [Google Scholar] [CrossRef]
- Field, N.; Cohen, T.; Struelens, M.J.; Palm, D.; Cookson, B.; Glynn, J.R.; Gallo, V.; Ramsay, M.; Sonnenberg, P.; MacCannell, D.; et al. Strengthening the Reporting of Molecular Epidemiology for Infectious Diseases (STROME-ID): An Extension of the STROBE Statement. Lancet Infect. Dis. 2014, 14, 341–352. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Disclose My Illness to Supporters after the Evacuation | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Item | Category | Total | No | Yes | |||||
| n | % | n | % | n | % | p-Value | |||
| Participant background | |||||||||
| Sex | Male | 78 | 65.5 | 44 | 56.4 | 34 | 43.6 | 0.589 | a |
| Female | 41 | 34.5 | 21 | 51.2 | 20 | 48.8 | |||
| Age, median (SD) | 50.9 (15.4) | 65 | 54.6 | 54 | 45.4 | 0.168 | a | ||
| 10 s | 2 | 1.7 | 2 | 100.0 | 0 | 0.0 | |||
| 20 s | 13 | 10.9 | 4 | 30.8 | 9 | 69.2 | b | ||
| 30 s | 15 | 12.6 | 10 | 66.7 | 5 | 33.3 | |||
| 40 s | 20 | 16.8 | 11 | 55.0 | 9 | 45.0 | b | ||
| 50 s | 31 | 26.1 | 13 | 41.9 | 8 | 25.8 | |||
| 60 s | 25 | 21.0 | 15 | 60.0 | 10 | 40.0 | a | ||
| 70 s | 11 | 9.2 | 10 | 90.9 | 1 | 9.1 | |||
| 80 s | 2 | 1.7 | 0 | 0.0 | 2 | 100.0 | a | ||
| Age group | Under 65 years old | 92 | 77.3 | 46 | 50.0 | 46 | 50.0 | 0.062 | a |
| 65 years or older | 27 | 22.7 | 19 | 70.4 | 8 | 29.6 | |||
| Type of disability | Mental disability | 99 | 83.2 | 58 | 58.6 | 41 | 41.4 | 0.053 | a |
| Other disabilities | 20 | 16.8 | 7 | 35.0 | 13 | 65.0 | |||
| Mental disability and intellectual disability | 10 | 8.4 | |||||||
| Mental disability and physical disability | 7 | 5.9 | |||||||
| Intellectual disability | 2 | 1.7 | |||||||
| Mental disability, intellectual disability, and physical disability | 1 | 0.8 | |||||||
| Services used by PMHI (Multiple answers) | |||||||||
| Day services | No | 71 | 59.7 | 38 | 53.5 | 33 | 46.5 | 0.769 | a |
| Yes | 48 | 40.3 | 27 | 56.3 | 21 | 43.8 | |||
| Visiting services | No | 80 | 67.2 | 46 | 57.5 | 34 | 42.5 | 0.366 | a |
| Yes | 39 | 32.8 | 19 | 48.7 | 20 | 51.3 | |||
| Employment support services | No | 68 | 57.1 | 42 | 61.8 | 26 | 38.2 | 0.071 | a |
| Yes | 51 | 42.9 | 23 | 45.1 | 28 | 54.9 | |||
| Other services | No | 109 | 91.6 | 61 | 56.0 | 48 | 44.0 | 0.509 | b |
| Yes | 10 | 8.4 | 4 | 40.0 | 6 | 60.0 | |||
| Disclosed My Illness to Supporters after the Evacuation | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Item | Category | Total | No | Yes | |||||
| n | % | n | % | n | % | p-Value | |||
| Mobile device usage (Multiple answers) | |||||||||
| Smartphone | No | 58 | 48.7 | 35 | 60.3 | 23 | 39.7 | 0.221 | a |
| Yes | 61 | 51.3 | 30 | 49.2 | 31 | 50.8 | |||
| Feature phone | No | 104 | 87.4 | 57 | 54.8 | 47 | 45.2 | 0.915 | a |
| Yes | 15 | 12.6 | 8 | 53.3 | 7 | 46.7 | |||
| Computer | No | 111 | 93.3 | 61 | 55.0 | 50 | 45.0 | 1.000 | b |
| Yes | 8 | 6.7 | 4 | 50.0 | 4 | 50.0 | |||
| Tablet device | No | 113 | 95.0 | 63 | 55.8 | 50 | 44.2 | 0.409 | b |
| Yes | 6 | 5.0 | 2 | 33.3 | 4 | 66.7 | |||
| Group home phone | No | 88 | 73.9 | 48 | 54.5 | 40 | 45.5 | 0.978 | a |
| Yes | 31 | 26.1 | 17 | 54.8 | 14 | 45.2 | |||
| Socialize with people | |||||||||
| Socialize with group home PMHI | No | 64 | 53.8 | 40 | 62.5 | 24 | 37.5 | 0.063 | a |
| Yes | 55 | 46.2 | 25 | 45.5 | 30 | 54.5 | |||
| Socialize with neighbors | No | 97 | 81.5 | 60 | 61.9 | 37 | 38.1 | <0.001 | a |
| Yes | 22 | 18.5 | 5 | 22.7 | 17 | 77.3 | |||
| Sources of information for determining disaster experience and evacuation | |||||||||
| Experience of being affected by a natural disaster | No | 81 | 68.1 | 48 | 59.3 | 33 | 40.7 | 0.138 | a |
| Yes | 38 | 31.9 | 17 | 44.7 | 21 | 55.3 | |||
| Sources of information when deciding whether to evacuate (Multiple answers) | |||||||||
| TV | No | 52 | 43.7 | 32 | 61.5 | 20 | 38.5 | 0.182 | a |
| Yes | 67 | 56.3 | 33 | 49.3 | 34 | 50.7 | |||
| Radio | No | 95 | 79.8 | 54 | 56.8 | 41 | 43.2 | 0.333 | a |
| Yes | 24 | 20.2 | 11 | 45.8 | 13 | 54.2 | |||
| Smartphone (internet) | No | 71 | 59.7 | 41 | 57.7 | 30 | 42.3 | 0.405 | a |
| Yes | 48 | 40.3 | 24 | 50.0 | 24 | 50.0 | |||
| Feature phone | No | 112 | 94.1 | 62 | 55.4 | 50 | 44.6 | 0.700 | b |
| Yes | 7 | 5.9 | 3 | 42.9 | 4 | 57.1 | |||
| Computer | No | 118 | 99.2 | 64 | 54.2 | 54 | 45.8 | 1.000 | b |
| Yes | 1 | 0.8 | 1 | 100.0 | 0 | 0.0 | |||
| Local Government Staff | No | 105 | 88.2 | 59 | 56.2 | 46 | 43.8 | 0.347 | a |
| Yes | 14 | 11.8 | 6 | 42.9 | 8 | 57.1 | |||
| Group home staff | No | 44 | 37.0 | 24 | 54.5 | 20 | 45.5 | 0.990 | a |
| Yes | 75 | 63.0 | 41 | 54.7 | 34 | 45.3 | |||
| Assumptions about evacuations from a disaster | |||||||||
| My friends would support me if I had to evacuate | No | 91 | 76.5 | 51 | 56.0 | 40 | 44.0 | 0.574 | a |
| Yes | 28 | 23.5 | 14 | 50.0 | 14 | 50.0 | |||
| My family would support me if I had to evacuate | No | 71 | 59.7 | 39 | 54.9 | 32 | 45.1 | 0.935 | a |
| Yes | 48 | 40.3 | 26 | 54.2 | 22 | 45.8 | |||
| My group home staff would support me if I had to evacuate | No | 21 | 17.6 | 12 | 57.1 | 9 | 42.9 | 0.798 | a |
| Yes | 98 | 82.4 | 53 | 54.1 | 45 | 45.9 | |||
| I can imagine living in a public shelter | No | 81 | 68.1 | 53 | 65.4 | 28 | 34.6 | <0.001 | a |
| Yes | 38 | 31.9 | 12 | 31.6 | 26 | 68.4 | |||
| I want to stay in my room without evacuating | No | 41 | 34.5 | 20 | 48.8 | 21 | 51.2 | 0.353 | a |
| Yes | 78 | 65.5 | 45 | 57.7 | 33 | 42.3 | |||
| I can’t live in a shelter with many people | No | 62 | 52.1 | 33 | 53.2 | 29 | 46.8 | 0.750 | a |
| Yes | 57 | 47.9 | 32 | 56.1 | 25 | 43.9 | |||
| I am concerned about interpersonal relationships at the shelter | No | 34 | 28.6 | 21 | 61.8 | 13 | 38.2 | 0.322 | a |
| Yes | 85 | 71.4 | 44 | 51.8 | 41 | 48.2 | |||
| I am concerned about stigma from others at the shelter | No | 46 | 38.7 | 27 | 58.7 | 19 | 41.3 | 0.479 | a |
| Yes | 73 | 61.3 | 38 | 52.1 | 35 | 47.9 | |||
| Item | Category | OR | 95% CI | p-Value | |
|---|---|---|---|---|---|
| Lower Limit | Upper Limit | ||||
| Sex | Female/Male | 0.85 | 0.35 | 2.05 | 0.717 |
| Age group | 65 years or older/Under 65 years old | 0.34 | 0.12 | 1.01 | 0.052 |
| Type of disability | Mental disability/Mental disability and other disabilities | 2.69 | 0.86 | 8.46 | 0.091 |
| Experience of being affected by a natural disaster | No/Yes | 1.85 | 0.76 | 4.51 | 0.174 |
| I can imagine living in a public shelter | Yes/No | 4.50 | 1.78 | 11.43 | 0.002 |
| Socialize with neighbors | Yes/No | 5.63 | 1.74 | 18.22 | 0.004 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oe, M.; Nakai, H.; Nagayama, Y. Factors Related to the Willingness of People with Mental Health Illnesses Living in Group Homes to Disclose Their Illness to Supporters during Disaster Evacuation: A Cross-Sectional Study. Nurs. Rep. 2024, 14, 1014-1025. https://doi.org/10.3390/nursrep14020076
Oe M, Nakai H, Nagayama Y. Factors Related to the Willingness of People with Mental Health Illnesses Living in Group Homes to Disclose Their Illness to Supporters during Disaster Evacuation: A Cross-Sectional Study. Nursing Reports. 2024; 14(2):1014-1025. https://doi.org/10.3390/nursrep14020076
Chicago/Turabian StyleOe, Masato, Hisao Nakai, and Yutaka Nagayama. 2024. "Factors Related to the Willingness of People with Mental Health Illnesses Living in Group Homes to Disclose Their Illness to Supporters during Disaster Evacuation: A Cross-Sectional Study" Nursing Reports 14, no. 2: 1014-1025. https://doi.org/10.3390/nursrep14020076
APA StyleOe, M., Nakai, H., & Nagayama, Y. (2024). Factors Related to the Willingness of People with Mental Health Illnesses Living in Group Homes to Disclose Their Illness to Supporters during Disaster Evacuation: A Cross-Sectional Study. Nursing Reports, 14(2), 1014-1025. https://doi.org/10.3390/nursrep14020076