
The Reasons for Unfinished Nursing Care during the COVID-19 Pandemic: An Integrative Review



Abstract
1. Introduction
2. Materials and Methods
2.1. Identifying the Research Questions
2.2. Eligibility Criteria
2.3. Quality Appraisal
2.4. Data Extraction and Synthesis
3. Results
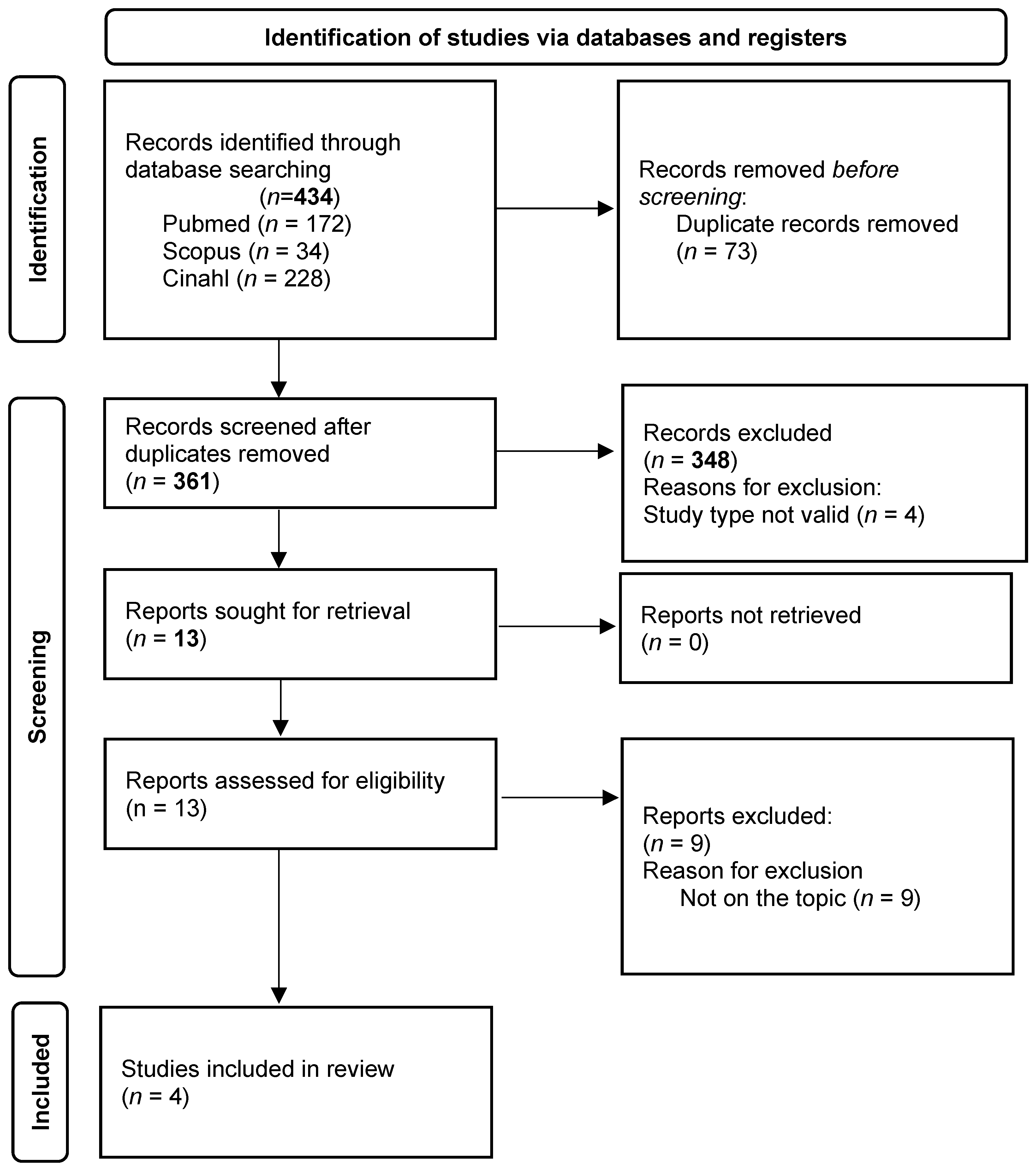
3.1. Study Characteristics
3.2. Reasons for UNC
3.2.1. System Level
- New priorities of the health system. The healthcare system has undergone major reorganisation, related to the drastic changes due to the COVID-19 pandemic, which has further reduced resources by exacerbating the pre-existing issues of the system [20,22] and leading to cost restraints in some sectors to rendering available resources to others [21].
- Pre-existing frailty of healthcare structures and processes. The inadequate environments, such as the old layouts of hospital buildings [21,22], as well as the discrepancies in the allocation of resources across units, have been seen as pre-existing frailties that have been exacerbated during the pandemic, thus increasing the risk of UNC. The structural and processual factors combined with an unbalanced workforce across units, and poor environments (e.g., distance between units), have been reported as leading to UNC [21].
- The poor support for nursing care. Systems causing a lack of nurses at the unit level [20,22], and not emphasising and/or communicating internally and externally the role and the value of nurses, have been documented as increasing the risk of UNC. Moreover, those systems not considering appropriately the early signs of poor-quality care (e.g., by analysing incident reports) have been perceived as insensitive towards UNC issues, neglecting its relevance and consequently strategies aimed at preventing it. In addition, some systems perpetuated some UNC factors when they did not invest in technologies facilitating nursing care [20]: the high level of bureaucratisation increased further during the pandemic (e.g., the need to collect certifications and to check issues) and led to time being wasted on administrative tasks leading nurses to postpone care [20,23].
- Increased challenges in leading nursing care. The fragmentation in the community of nurses as a profession and as a system has been reported as affecting its capacity to effectively address changes and policies, as an independent body, both at the political and institutional levels [22,23]. Similarly, the increased nursing turnover [23] has been reported as triggering UNC.
3.2.2. Unit Level
- Inadequate care environment. The environments within the units have been reported as inadequate in terms of their layouts, leading to time being wasted by nurses in getting to rooms or retrieving material. Moreover, with many patients being in the same room, the increased attention and processes needed to protect them from safety issues required more time and, when nurses experience a lack in resources, a greater occurrence of UNC. In some units, the perceived chaos and confusion distracted nurses while they were providing the necessary care [20].
- Insufficient human resources. The lack of human resources, reflected in the high nurse/patient ratio [20,21], due to the shortage of nurses [20,21,22,23] and nursing aides [20] has been documented. In addition, the absence of physicians (e.g., when they are outside the unit) also increased workloads, resulting in some care needs being missed [20].
- Ineffective shift design. An adequate presence of staff was not always planned during the day, at night and at weekends; the length of shifts was also a problem with shifts being too long. The idea that there are fewer care activities to provide at the weekend generated ineffective shift planning, reducing the number of nurses at the unit level during weekends [20,21]; on the other hand, excessively long shifts led to fatigue and lowered the standard of nursing work.
- Ineffective unit organization and work process. The mission of the unit and its continuing change have triggered uncertainty regarding the priorities [21]. Specifically, nurses were continuously called to review their work processes, redefining priorities and activities [20], due to continuous unexpected events [20] related to internal (e.g., emergencies) and/or external (e.g., COVID-19 patients) new conditions [23] such as the high number of discharges and admissions [20]. The continuous need to redefine care plans was also influenced by the high frequency of interruptions (e.g., answering the telephone) [20,21] and the disrupted routines due to changes imposed on the work processes in managing the pandemic [20,22]. The several competitive activities [20,21,22] have increased the occurrence of UNC. The high number of newly qualified nurses, deployed from other wards, prevented the possibility of working with shared procedures [20,22], leading to uncoordinated decisions, the wasting of time and ultimately UNC [20,21]. Expanding the capacity of the unit in response to the numerous unpredictable events was not always possible; therefore, with the same resources, all patients were cared for, but not all care needs were catered for, thereby increasing the occurrence of UNC.
- Ineffective models of nursing care. The delivery models did not support the personalisation of care expected both by patients and nurses. Specifically, the functional model in which tasks are fragmented, accompanied by the need to limit the exposure to patients due to the risk of contagion, have been reported as threatening care needs; also, handovers were incomplete or ineffective, due to the fragmentation of care, with failure to communicate patient needs ultimately leading to UNC [20].
- Ineffective inter- and intra-professional collaboration. The lack of collaboration and communication inside the nursing profession and across various professionals has been reported as causing tensions or interruptions in communication during the care process, thus increasing the risk of UNC [20,22].
3.2.3. Nurse Manager Level
3.2.4. Clinical Nurse Level
- Issues with nurses’ attitudes, competences and performances. The lack of empathy triggered poor communication and understanding of needs, and while working in a hurry prevented any contact with patients, thereby threatening the capacity to identify patients’ needs [21]. Moreover, reduced working abilities related to an increase in age [20], and a lack of work experience, knowledge and skills [20], as well as professional responsibility [20,21] and/or motivation [20,21,23], have also been reported as increasing the occurrence of UNC. Furthermore, the tiredness caused by high workloads [20,21,23] and the poor ability to manage time, to attribute priorities [20] or to delegate [20,21] have generated UNC. Errors in care planning (for example, scheduling of unnecessary interventions) have also been underlined as leading to UNC [20,22].
- Weaknesses in education: incomplete training or mentoring [20,23] led to long periods of time being needed to work effectively as an independent nurse among those just introduced into the unit. An increased risk of missing under-recognised needs was also reported. On the other hand, excessive burden among some more experienced nurses has been documented as causing a high nursing turnover, which implied the need to support new colleagues [20].
- Poor humanistic vision of the patient. Nursing care not centred on the person, but rather on the activities/tasks to be provided, forced by the extreme working conditions experienced, have reduced the capacity to consider all needs (for example emotional ones) that have been missed [20].
3.2.5. Patient Level
- Increased demand for patient care. During the pandemic, an increased number of patients were in unstable conditions [20,23], with highly complex and/or worse clinical conditions [20], many with co-morbidities [22,23], and elderly people with cognitive decline [20,22] and living alone [20]. These patients required more care, as they were not always able to communicate their needs, and above all, they were not supported by caregivers [20,22,23].
- Increased nursing care needs and expectations. In some contexts, patients became more demanding; they also resisted treatments because they did not believe that the pandemic and the need for treatment were truthful; for example, they rejected educational interventions regarding vaccinations [20,21].
4. Discussion
The Reasons for UNC
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
Guidelines and Standards Statement
Use of Artificial Intelligence
Conflicts of Interest
References
- Jones, T.L.; Hamilton, P.; Murry, N. Unfinished nursing care, missed care, and implicitly rationed care: State of the science review. Int. J. Nurs. Stud. 2015, 52, 1121–1137. [Google Scholar] [CrossRef] [PubMed]
- Jones, T.; Willis, E.; Amorim-Lopes, M.; Drach-Zahavy, A. RANCARE Consortium COST-CA 15208 Advancing the science of unfinished nursing care: Exploring the benefits of cross-disciplinary knowledge exchange, knowledge integration and transdisciplinarity. J. Adv. Nurs. 2019, 75, 905–917. [Google Scholar] [CrossRef] [PubMed]
- Bassi, E.; Tartaglini, D.; Valpiani, G.; Grassetti, L.; Palese, A. Unfinished Nursing Care Survey: A development and validation study. J. Nurs. Manag. 2020, 28, 2061–2071. [Google Scholar] [CrossRef] [PubMed]
- Moura, E.C.C.; Lima, M.B.; Peres, A.M.; Lopez, V.; Batista, M.E.M.; Braga, F.D.C.S.A.G. Relationship between the implementation of primary nursing model and the reduction of missed nursing care. J. Nurs. Manag. 2020, 28, 2103–2112. [Google Scholar] [CrossRef] [PubMed]
- Chiappinotto, S.; Papastavrou, E.; Efstathiou, G.; Andreou, P.; Stemmer, R.; Ströhm, C.; Schubert, M.; de Wolf-Linder, S.; Longhini, J.; Palese, A. Antecedents of unfinished nursing care: A systematic review of the literature. BMC Nurs. 2022, 21, 137. [Google Scholar] [CrossRef]
- von Vogelsang, A.C.; Göransson, K.E.; Falk, A.C.; Nymark, C. Missed nursing care during the COVID-19 pandemic: A comparative observational study. J. Nurs. Manag. 2021, 29, 2343–2352. [Google Scholar] [CrossRef] [PubMed]
- Falk, A.C.; Nymark, C.; Göransson, K.E.; von Vogelsang, A.C. Missed nursing care in the critical care unit, before and during the COVID-19 pandemic: A comparative cross-sectional study. Intensive Crit. Care Nurs. 2022, 72, 103276. [Google Scholar] [CrossRef] [PubMed]
- Alfuqaha, O.A.; Alhalaiqa, F.N.; Alqurneh, M.K.; Ayed, A. Missed nursing care before and during the COVID-19 pandemic: A comparative cross-sectional study. Int. Nurs. Rev. 2023, 70, 100–110. [Google Scholar] [CrossRef] [PubMed]
- Gurková, E.; Bartoníčková, D.; Mikšová, Z.; Labudíková, M.; Chocholková, D. Důvody nedokončené ošetřovatelské péče z pohledu sester z okresních a fakultních nemocnic. Kontakt 2021, 23, 281–288. [Google Scholar] [CrossRef]
- Cengia, M.G.; Di Falco, A.; Allegrini, E.; Ambrosi, E.; Brugnaro, L.; Zambon, A.; Saiani, L.; Grassetti, L.; Palese, A. Occurrence and reasons for unfinished nursing care between COVID-19 and non-COVID-19 patients. Int. Nurs. Rev. 2022, 69, 420–431. [Google Scholar] [CrossRef] [PubMed]
- Kakemam, E.; Chegini, Z.; Rouhi, A.; Ahmadi, F.; Majidi, S. Burnout and its relationship to self-reported quality of patient care and adverse events during COVID-19: A cross-sectional online survey among nurses. J. Nurs. Manag. 2021, 29, 1974–1982. [Google Scholar] [CrossRef] [PubMed]
- Rezaei-Shahsavarloo, Z.; Atashzadeh-Shoorideh, F.; Ebadi, A.; Gobbens, R.J.J. Factors affecting missed nursing care in hospitalized frail older adults in the medical wards: A qualitative study. BMC Geriatr. 2021, 21, 555. [Google Scholar] [CrossRef] [PubMed]
- Papastavrou, E.; Suhonen, R. Impacts of Rationing and Missed Nursing Care: Challenges and Solutions: RANCARE Action, 1st ed.; Springer: New York, NY, USA, 2021. [Google Scholar]
- Whittemore, R.; Knafl, K. The integrative review: Updated methodology. J. Adv. Nurs. 2005, 52, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Coronavirus Disease (COVID-19) Pandemic. 2021. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 5 March 2024).
- Critical Appraisal Skills Programme CASP (Qualitative) Checklist. 2018. Available online: https://casp-uk.net/images/checklist/documents/CASP-Qualitative-Studies-Checklist/CASP-Qualitative-Checklist-2018_fillable_form.pdf (accessed on 5 March 2024).
- Hong, Q.N.; Pluye, P.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; et al. Mixed Methods Appraisal Tool (MMAT), Version 2018; Registration of Copyright; Canadian Intellectual Property Office, Industry Canada: Gatineau, QC, Canada, 2018; p. 1148552. [Google Scholar]
- Chiappinotto, S.; Palese, A. Unfinished nursing care reasons as perceived by nurses at different levels of nursing services: Findings of a qualitative study. J. Nurs. Manag. 2022, 30, 3393–3405. [Google Scholar] [CrossRef]
- Chiappinotto, S.; Coppe, A.; Palese, A. What are the reasons for unfinished nursing care as perceived by hospitalized patients? Findings from a qualitative study. Health Expect. 2023, 26, 256–267. [Google Scholar] [CrossRef] [PubMed]
- Safdari, A.; Rassouli, M.; Elahikhah, M.; Ashrafizadeh, H.; Barasteh, S.; Jafarizadeh, R.; Khademi, F. Explanation of factors forming missed nursing care during the COVID-19 pandemic: A qualitative study. Front. Public Health 2023, 11, 989458. [Google Scholar] [CrossRef] [PubMed]
- Hackman, P.; Hult, M.; Häggman-Laitila, A. Unfinished nursing care in nursing homes. Geriatr. Nurs. 2023, 51, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Ludlow, K.; Churruca, K.; Mumford, V.; Ellis, L.A.; Testa, L.; Long, J.C.; Braithwaite, J. Unfinished Care in Residential Aged Care Facilities: An Integrative Review. Gerontologist 2021, 61, e61–e74. [Google Scholar] [CrossRef] [PubMed]
- Galanis, P.; Moisoglou, I.; Katsiroumpa, A.; Vraka, I.; Siskou, O.; Konstantakopoulou, O.; Meimeti, E.; Kaitelidou, D. Increased Job Burnout and Reduced Job Satisfaction for Nurses Compared to Other Healthcare Workers after the COVID-19 Pandemic. Nurs. Rep. 2023, 13, 1090–1100. [Google Scholar] [CrossRef]
- Baldassini Rodriguez, S.; Bardacci, Y.; El Aoufy, K.; Bazzini, M.; Caruso, C.; Giusti, G.D.; Mezzetti, A.; Lucchini, A.; Iozzo, P.; Guazzini, A.; et al. Sleep Quality and Its Relationship to Anxiety and Hardiness in a Cohort of Frontline Italian Nurses during the First Wave of the COVID-19 Pandemic. Nurs. Rep. 2023, 13, 1203–1215. [Google Scholar] [CrossRef]
- Kalisch, B.J.; Williams, R.A. Development and psychometric testing of a tool to measure missed nursing care. J. Nurs. Adm. 2009, 39, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Palese, A.; Bassi, E.; Bayram, A.; Dal Molin, A.; Chiappinotto, S. Misurare le missed nursing care in tempi di COVID-19: Riflessioni di metodo [Measuring missed nursing care during the Covid-19 pandemic: Methodological reflections]. AIR 2023, 42, 98–102. [Google Scholar] [CrossRef] [PubMed]
- Hugelius, K.; Harada, N.; Marutani, M. Consequences of visiting restrictions during the COVID-19 pandemic: An integrative review. Int. J. Nurs. Stud. 2021, 121, 104000. [Google Scholar] [CrossRef] [PubMed]
- Stemmer, R.; Bassi, E.; Ezra, S.; Harvey, C.; Jojo, N.; Meyer, G.; Özsaban, A.; Paterson, C.; Shifaza, F.; Turner, M.B.; et al. A systematic review: Unfinished nursing care and the impact on the nurse outcomes of job satisfaction, burnout, intention-to-leave and turnover. J. Adv. Nurs. 2022, 78, 2290–2303. [Google Scholar] [CrossRef]
- Lobão, C.; Coelho, A.; Parola, V.; Neves, H.; Sousa, J.P.; Gonçalves, R. Changes in Clinical Training for Nursing Students during the COVID-19 Pandemic: A Scoping Review. Nurs. Rep. 2023, 13, 378–388. [Google Scholar] [CrossRef]
- Zurzycka, P.Z.; Czyżowicz, K.; Musiał, Z.; Puto, G. Moral distress w pielęgniarstwie psychiatrycznym. Piel. Pol. 2023, 4, 135–140. [Google Scholar] [CrossRef]
- Benazzi, B.; Bevilacqua, S.; De Togni, S.; Milani, E.; Perdomini, M.; Laquintana, D. Prepararsi alle emergenze: Strategie per aumentare l’offerta di posti letto e di competenze intensive avanzate [Preparedness for emergencies: Strategies to increase the supply of beds and advanced intensive skills]. Assist. Inferm. Ric. 2023, 42, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Labrague, L.J.; de Los Santos, J.A.A.; Fronda, D.C. Factors associated with missed nursing care and nurse-assessed quality of care during the COVID-19 pandemic. J. Nurs. Manag. 2022, 30, 62–70. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Level | Theme | Subtheme | Authors (Year) |
|---|---|---|---|
| System | New healthcare system priorities | Dramatic changes due to the COVID-19 pandemic | Chiappinotto et al. (2023) [21] Safdari et al. (2023) [22] |
| Cost restraints | Chiappinotto et al. (2023) [21] | ||
| Pre-existing frailty of healthcare facilities | Unsuitable environment layout | Chiappinotto et al. (2023) [21] Safdari et al. (2023) [22] | |
| Old technologies | Chiappinotto et al. (2023) [21] Safdari et al. (2023) [22] | ||
| Discrepancies in resource allocation across units | Chiappinotto et al. (2023) [21] | ||
| Poor support for nursing care | Lack of nurses and nursing care value | Chiappinotto & Palese (2022) [20] Safdari et al. (2023) [22] | |
| System insensitive to UNC issues | Chiappinotto & Palese, (2022) [20] | ||
| High bureaucratisation and lack of investments in electronic records | Chiappinotto & Palese, (2022) [20] Hackman et al. (2023) [23] | ||
| Challenges in leading nursing care | Lack of effective professional community | Hackman et al. (2023) [23] Safdari et al. (2023) [22] | |
| High turnover | Hackman et al. (2023) [23] | ||
| Unit | Inappropriate care environment | Layout of the environment | Chiappinotto & Palese, (2022) [20] |
| High number of patients in each room | Chiappinotto & Palese, (2022) [20] | ||
| Chaotic environment | Chiappinotto & Palese, (2022) [20] | ||
| Insufficient material resources | Material resources unavailable or limited | Chiappinotto & Palese, (2022) [20] | |
| Restrictions in furniture/equipment | Safdari et al. (2023) [22] | ||
| Insufficient human resources | Higher nurse/patient ratio | Chiappinotto & Palese, (2022) [20] Chiappinotto et al. (2023) [21] | |
| Nurse shortages | Chiappinotto & Palese, (2022) [20] Chiappinotto et al. (2023) [21] Safdari et al. (2023) [22] Hackman et al. (2023) [23] | ||
| Nursing aide shortages | Chiappinotto & Palese, (2022) [20] | ||
| Physicians unavailable (e.g., off the unit) | Chiappinotto & Palese, (2022) [20] | ||
| Ineffective inter- and intra-professional cooperation | Poor teamwork (lack of collaboration and communication/lack of in-group reflection on action) | Chiappinotto & Palese, (2022) [20] Safdari et al. (2023) [22] | |
| Tension or communication breakdowns between nurses and medical staff, nurses and nursing aides, nurses and ward managers, and nurses and patients | Chiappinotto & Palese, (2022) [20] Safdari et al. (2023) [22] | ||
| Ineffective shift design | Lack of staff during the day, nights, and weekends Excessive length of shifts | Chiappinotto & Palese, (2022) [20] Chiappinotto et al. (2023) [21] | |
| Ineffective unit organization and work process | Work process unpredictability due to unexpected internal (e.g., a new hospitalization, an urgency of a particular patient) or external (e.g., COVID-19) situations | Chiappinotto & Palese, (2022) [20] Hackman et al. (2023) [23] | |
| Mission of the ward (specialised wards have a greater focus on the individual needs of patients) | Chiappinotto et al. (2023) [21] | ||
| Large number of discharges and admissions | Chiappinotto & Palese, (2022) [20] | ||
| Overlapping activities | Chiappinotto & Palese, (2022) [20] Chiappinotto et al. (2023) [21] Safdari et al. (2023) [22] | ||
| Limited capacity to react to unpredictable events (admissions/emergencies) | Chiappinotto et al. (2023) [21] | ||
| Ineffective routine | Chiappinotto & Palese, (2022) [20] Safdari et al. (2023) [22] | ||
| Lack of shared procedures | Chiappinotto & Palese, (2022) [20] Safdari et al. (2023) [22] | ||
| Higher frequency of interruptions | Chiappinotto & Palese, (2022) [20] Chiappinotto et al. (2023) [21] | ||
| Ineffective models of nursing care delivery | Poor nursing care models of care delivery: functional nursing | Chiappinotto & Palese, (2022) [20] Chiappinotto et al. (2023) [21] | |
| Incomplete or ineffective handovers | Chiappinotto & Palese, (2022) [20] | ||
| Manager | Inadequate nurse manager’s leadership | Inadequate nurse manager’s leadership | Chiappinotto & Palese, (2022) [20] Chiappinotto et al. (2023) [21] |
| Nurse | Nurses’ attitudes, competences and performances | Being in a hurry | Chiappinotto et al. (2023) [21] |
| Reduced work capacity due to increased age | Chiappinotto & Palese, (2022) [20] | ||
| Lack of experience, knowledge, competences (e.g., empathic) | Chiappinotto & Palese, (2022) [20] | ||
| Lack of responsibility | Chiappinotto & Palese, (2022) [20] Chiappinotto et al. (2023) [21] | ||
| Low motivation | Chiappinotto & Palese, (2022) [20] Chiappinotto et al. (2023) [21] Hackman et al. (2023) [23] | ||
| Higher stress, fatigue | Chiappinotto & Palese, (2022) [20] Chiappinotto et al. (2023) [21] Hackman et al. (2023) [23] | ||
| Poor time management skills | Chiappinotto & Palese, (2022) [20] | ||
| Ineffective delegation skills | Chiappinotto & Palese, (2022) [20] Chiappinotto et al. (2023) [21] | ||
| Ineffective priority-setting skills | Chiappinotto & Palese, (2022) [20] | ||
| Wrong nursing care planning | Chiappinotto & Palese, (2022) [20] Safdari et al. (2023) [22] | ||
| Weaknesses in education | Incomplete training/mentoring (in the transition as a newly qualified graduate)/inadequate orientation of the new staff | Chiappinotto & Palese, (2022) [20] Hackman et al. (2023) [23] | |
| High turnover among nurses | Chiappinotto & Palese, (2022) [20] | ||
| Poor humanistic view of patient care | Nursing care not patient-centred | Chiappinotto & Palese, (2022) [20] | |
| Patient | Increased demand of patient care | Clinical instability | Chiappinotto & Palese, (2022) [20] Hackman et al. (2023) [23] |
| Complexity/needs Worse clinical conditions | Chiappinotto & Palese, (2022) [20] Hackman et al. (2023) [23] Safdari et al. (2023) [22] | ||
| Age | Safdari et al. (2023) | ||
| Cognitive impairments | Chiappinotto & Palese, (2022) [20] Safdari et al. (2023) [22] | ||
| Loneliness | Chiappinotto & Palese, (2022) [20] | ||
| Lack of carer support | The absence of relatives/caregivers Hospital restriction to relatives | Chiappinotto & Palese, (2022) [20] Safdari et al. (2023) [22] | |
| Increased nursing care needs and care expectations | Demanding patients | Chiappinotto & Palese, (2022) [20] Chiappinotto et al. (2023) [21] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sist, L.; Chiappinotto, S.; Messina, R.; Rucci, P.; Palese, A. The Reasons for Unfinished Nursing Care during the COVID-19 Pandemic: An Integrative Review. Nurs. Rep. 2024, 14, 753-766. https://doi.org/10.3390/nursrep14020058
Sist L, Chiappinotto S, Messina R, Rucci P, Palese A. The Reasons for Unfinished Nursing Care during the COVID-19 Pandemic: An Integrative Review. Nursing Reports. 2024; 14(2):753-766. https://doi.org/10.3390/nursrep14020058
Chicago/Turabian StyleSist, Luisa, Stefania Chiappinotto, Rossella Messina, Paola Rucci, and Alvisa Palese. 2024. "The Reasons for Unfinished Nursing Care during the COVID-19 Pandemic: An Integrative Review" Nursing Reports 14, no. 2: 753-766. https://doi.org/10.3390/nursrep14020058
APA StyleSist, L., Chiappinotto, S., Messina, R., Rucci, P., & Palese, A. (2024). The Reasons for Unfinished Nursing Care during the COVID-19 Pandemic: An Integrative Review. Nursing Reports, 14(2), 753-766. https://doi.org/10.3390/nursrep14020058