
Translation, Cross-Cultural Adaptation, and Psychometric Properties of the Persian Version of the Measure of Audiologic Rehabilitation Self-Efficacy for Hearing Aids (P-MARS-HA)


 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Inclusion Criteria
2.4. Research Instruments
- Measure of Audiologic Rehabilitation Self-Efficacy for Hearing Aids Questionnaire (MARS-HA)West and Smith (2007) designed the Measure of Audiologic Rehabilitation Self-Efficacy for Hearing Aids (MARS-HA) to assess current self-efficacy beliefs related to hearing aids [21]. This scale consists of 24 questions and 4 subscales: 1. Aided Listening (9 items): This subscale assesses an individual’s self-efficacy when listening with a hearing aid in a specific listening situation; for example, “I could understand a one-on-one conversation in a quiet place if I wore hearing aids”. 2. Basic Handling (7 items): This includes questions assessing an individual’s self-efficacy in the basic management of a hearing aid, for example, “I can insert a battery into a hearing aid with ease”. 3. Adjustment (3 items): Questions assessing an individual’s self-efficacy in adjusting to the hearing aid, for example, “I could get used to the sound quality of hearing aids”. 4. Advanced Handling (5 items): Questions assessing a hearing-aid user’s self-efficacy in performing advanced hearing aid tasks, for example, “I can troubleshoot a hearing aid when it stops working”. For scoring the questions, respondents should report how much confidence they have in their ability on a 10-unit interval scale (0, 10, 20...100 percent) for each question. If they feel they do not have the ability or skill, they score zero, and if they are completely confident in performing that skill, they consider a score of 100 for themselves. A higher score on this questionnaire indicates greater self-efficacy. According to West and Smith, if the average score of the questionnaire is higher than 80 percent, it indicates a sufficient level of self-efficacy. West and Smith reported the reliability of this instrument for experienced hearing-aid users, using Cronbach’s alpha coefficient for the total scale as 0.91, and for the subscales “Basic Handling”, “Advanced Handling”, “Adjustments”, and “Aided Listening” as 0.88, 0.67, 0.73, and 0.91, respectively. In addition, using the test–retest method, the reliability of the instrument was obtained as 0.88 [21].
- Satisfaction with Amplification in Daily Life (SADL)The Satisfaction with Amplification in Daily Life questionnaire is a valid instrument designed by Cox and Alexander (1999) [28]. This instrument assesses an individual’s satisfaction in various aspects of hearing-aid use and consists of 15 items and four subscales: Positive Effects, Services and Costs, Negative Features, and Personal Image. The average score obtained from each subscale assesses the individual’s range of satisfaction and forms the overall questionnaire score. The method of responding to questions is based on a 7-option Likert scale (from completely agree to completely disagree), such that in four questions (2, 4, 7, 13), scoring is reversed. In the research by Faraji Khiavi et al. (2014), the face and content validity of the Persian version of this tool were reviewed and confirmed by five experts, and its internal reliability was obtained as 0.8 through the calculation of Cronbach’s alpha index [29].
2.5. Description of the Procedure
- Phase (1): Translation and Localization
- Phase (2): Psychometric Properties
2.6. Data Analysis
3. Results
3.1. Floor and Ceiling Effects
3.2. Descriptive Results
3.3. Face Validity
3.4. Content Validity
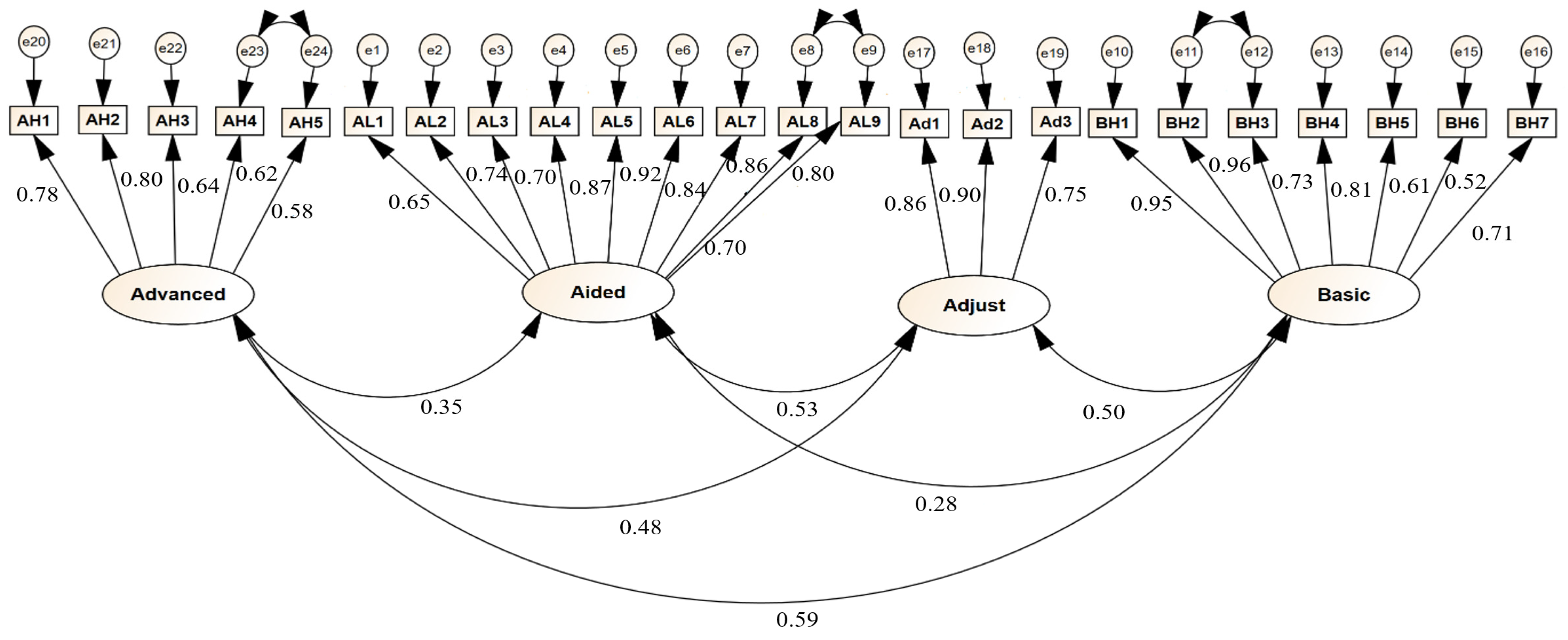
3.5. Construct Validity (Confirmatory Factor Analysis)
3.6. Criterion Validity
3.7. Reliability
4. Discussion
5. Conclusions
6. Clinical Applications
7. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Younis, N.M.; Ibrahim, R.M.; Ahmed, M.M. Health problems related to Quality of Life among Aging in Iraq. J. Curr. Med. Res. Opinion. 2024, 7, 3015–3024. [Google Scholar]
- Hajizadeh, A.; Albelbeisi, A.H.; Tajvar, M. Impacts of Population Ageing on the Functions of the Health System: A Systematic Review. Iran. J. Ageing. 2024, 19, 328–361. [Google Scholar] [CrossRef]
- Velaithan, V.; Tan, M.-M.; Yu, T.-F.; Liem, A.; Teh, P.-L.; Su, T.T. The association of self-perception of aging and quality of life in older adults: A systematic review. Gerontologist 2024, 64, gnad041. [Google Scholar] [CrossRef] [PubMed]
- Naseh, L.; Mohammadi-Shahboulaghi, F.; Khankeh, H.R.; Norouzi Tabrizi, K. Successful Aging: Concept Analysis with Walker and Avant’s Approach. Iran. J. Ageing. 2024, 19, 158–175. [Google Scholar] [CrossRef]
- Afrashteh, M.Y.; Majzoobi, M.R.; Janjani, P.; Forstmeier, S. The relationship between the meaning of life, psychological well-being, self-care, and social capital, with depression and death anxiety in the elderly living in nursing homes: The mediating role of loneliness. Heliyon 2024, 10, e30124. [Google Scholar] [CrossRef]
- Lin, F.R. Age-related hearing loss. N. Engl. J. Med. 2024, 390, 1505–1512. [Google Scholar] [CrossRef]
- Haile, L.M.; Orji, A.U.; Reavis, K.M.; Briant, P.S.; Lucas, K.M.; Alahdab, F.; Bärnighausen, T.W.; Bell, A.W.; Cao, C.; Dai, X.J.E.; et al. Hearing loss prevalence, years lived with disability, and hearing aid use in the United States from 1990 to 2019: Findings from the global burden of disease study. Ear Hear. 2024, 45, 257–267. [Google Scholar]
- Shukla, A.; Reed, N.S.; Armstrong, N.M.; Lin, F.R.; Deal, J.A.; Goman, A.M. Hearing Loss, Hearing Aid Use, and Depressive Symptoms in Older Adults-Findings from the Atherosclerosis Risk in Communities Neurocognitive Study (ARIC-NCS). J. Gerontol. Ser. B 2021, 76, 518–523. [Google Scholar] [CrossRef]
- Sanders, M.E.; Kant, E.; Smit, A.L.; Stegeman, I. The effect of hearing aids on cognitive function: A systematic review. PLoS ONE 2021, 16, e0261207. [Google Scholar] [CrossRef] [PubMed]
- Committee on Accessible and Affordable Hearing Health Care for Adults; Board on Health Sciences Policy; Health and Medicine Division; National Academies of Sciences, Engineering, and Medicine; Blazer, D.G.; Domnitz, S.; Liverman, C.T. (Eds.) The National Academies Collection: Reports funded by National Institutes of Health. In Hearing Health Care for Adults: Priorities for Improving Access and Affordability; National Academies Press (US): Washington, DC, USA, 2016. [Google Scholar]
- Lisan, Q.; Goldberg, M.; Lahlou, G.; Ozguler, A.; Lemonnier, S.; Jouven, X.; Zins, M.; Empana, J.-P. Prevalence of hearing loss and hearing aid use among adults in France in the CONSTANCES study. JAMA Netw. Open 2022, 5, e2217633. [Google Scholar] [CrossRef]
- Oosthuizen, I.; Manchaiah, V.; Launer, S.; Swanepoel, D.W. Hearing aid experiences of adult hearing aid owners during and after fitting: A systematic review of qualitative studies. Trends Hear. 2022, 26, 23312165221130584. [Google Scholar] [CrossRef] [PubMed]
- Houmøller, S.; Wolff, A.; Möller, S.; Narne, V.; Narayanan, S.; Godballe, C.; Hougaard, D.; Loquet, G.; Gaihede, M.; Hammershøi, D.J. Prediction of successful hearing aid treatment in first-time and experienced hearing aid users: Using the International Outcome Inventory for Hearing Aids. Int. J. Audiol. 2022, 61, 119–129. [Google Scholar] [CrossRef]
- Knoetze, M.; Manchaiah, V.; Mothemela, B.; Swanepoel, D.W. Factors influencing hearing help-seeking and hearing aid uptake in adults: A systematic review of the past decade. Trends Hear. 2023, 27, 23312165231157255. [Google Scholar] [CrossRef]
- Franks, I.; Timmer, B.H. Reasons for the non-use of hearing aids: Perspectives of non-users, past users, and family members. Int. J. Audiol. 2024, 63, 794–801. [Google Scholar] [CrossRef]
- Tavanai, E.; Khalili, M.E.; Shahidipour, Z.; Jalaie, S.; Ghahraman, M.A.; Rouhbakhsh, N.; Rahimi, V. Hearing handicaps, communication difficulties and depression in the older adults: A comparison of hearing aid users and non-users. Eur. Arch. Oto-Rhino-Laryngol. 2023, 280, 5229–5240. [Google Scholar] [CrossRef]
- Sarangi, L.; Johnson, J. An exploration of associations between hearing aid self-efficacy and other measurable characteristics of naïve and experienced hearing aid users. Int. J. Audiol. 2023, 62, 343–349. [Google Scholar] [CrossRef]
- Ferguson, M.A.; Woolley, A.; Munro, K.J. The impact of self-efficacy, expectations, and readiness on hearing aid outcomes. Int. J. Audiol. 2016, 55 (Suppl. 3), S34–S41. [Google Scholar] [CrossRef] [PubMed]
- Meyer, C.; Hickson, L.; Fletcher, A. Identifying the barriers and facilitators to optimal hearing aid self-efficacy. Int. J. Audiol. 2014, 53 (Suppl. 1), S28–S37. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Guide for constructing self-efficacy scales. Self-Effic. Beliefs Adolesc. 2006, 5, 307–337. [Google Scholar]
- West, R.L.; Smith, S.L. Development of a hearing aid self-efficacy questionnaire. Int. J. Audiol. 2007, 46, 759–771. [Google Scholar] [CrossRef]
- Johnson, J.; Sarangi, L. Shared experiences among successful hearing aid users with high hearing aid self-efficacy. Int. J. Audiol. 2024, 63, 579–586. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.E.; Jilla, A.M.; Danhauer, J.L.; Sullivan, J.C.; Sanchez, K.R. (Eds.) Benefits from, satisfaction with, and self-efficacy for advanced digital hearing aids in users with mild sensorineural hearing loss. In Seminars in Hearing; Thieme Medical Publishers: New York, NY, USA, 2018. [Google Scholar]
- Kelly-Campbell, R.J.; McMillan, A. The relationship between hearing aid self-efficacy and hearing aid satisfaction. Am. J. Audiol. 2015, 24, 529–535. [Google Scholar] [CrossRef]
- Fuentes-López, E.; Fuente, A.; Valdivia, G.; Luna-Monsalve, M. Does educational level predict hearing aid self-efficacy in experienced older adult hearing aid users from Latin America? Validation process of the Spanish version of the MARS-HA questionnaire. PLoS ONE 2019, 14, e0226085. [Google Scholar] [CrossRef]
- Vincent, C.; Gagné, J.-P.; Leroux, T.; Clothier, A.; Larivière, M.; Dumont, F.S.; Gendron, M. French-Canadian translation and validation of four questionnaires assessing hearing impairment and handicap. Int. J. Audiol. 2017, 56, 248–259. [Google Scholar] [CrossRef] [PubMed]
- Bakhtiyari, F.; Foroughan, M.; Fakhrzadeh, H.; Nazari, N.; Najafi, B.; Alizadeh, M.; Arzaghi, M.; Sharifi, F.; Shoaee, S.; Mostafa, Q.; et al. Validation of the persian version of Abbreviated Mental Test (AMT) in elderly residents of Kahrizak charity foundation. Iran. J. Diabetes Metab. 2014, 13, 487–494. [Google Scholar]
- Cox, R.M.; Alexander, G.C. hearing. Measuring satisfaction with amplification in daily life: The SADL scale. Ear Hear. 1999, 20, 306–320. [Google Scholar] [CrossRef] [PubMed]
- FarajiKhiavi, F.; Bayat, A.; Dashti, R.; Sameni, S.J. Hearing aid-related satisfaction based on type and degree of hearing loss in elderly. Bimon. Audiol.-Tehran Univ. Med. Sci. 2015, 23, 114–122. [Google Scholar]
- Mahomed-Asmail, F.; Graham, M.A.; Swanepoel, W.; Manchaiah, V.; Yerraguntla, K.; Karlsson, E. Predictors of hearing loss disability: A multinational study using the ICF core set. Int. J. Audiol. 2025, 1–8. [Google Scholar] [CrossRef]
- Gomez, R.; Ferguson, M. Improving self-efficacy for hearing aid self-management: The early delivery of a multimedia-based education programme in first-time hearing aid users. Int. J. Audiol. 2020, 59, 272–281. [Google Scholar] [CrossRef]

{kind=link}
| Variables | Frequency (%) | |
|---|---|---|
| Age | Mean (SD): | 71.38 (8.05) |
| Gender | Female | 152 (50.7%) |
| Male | 148 (49.3%) | |
| Education status | Illiterate | 45 (15%) |
| Primary | 66 (22%) | |
| Secondary | 65 (21.7%) | |
| Diploma | 77 (25.7%) | |
| Higher education | 47 (15.6%) | |
| Marital Status | Married | 211 (70.3%) |
| Widow | 71 (23.7%) | |
| Divorced | 18 (6%) | |
| Types of Hearing Aids | Digital | 243 (81%) |
| Programmable | 37 (12.3%) | |
| Analog | 20 (6.7%) | |
| Degree of hearing impairment (WEA) | ˂26 dB HL | 0 |
| 26–40 dB HL | 9 (3%) | |
| 41–55 dB HL | 82 (27.3%) | |
| 56–70 dB HL | 149 (49.7%) | |
| 71 dB HL | 60 (20%) | |
| Hearing aid fitting | Unilateral | 98 (32.7%) |
| Bilateral | 202 (67.3%) | |
| Style of hearing aid | Behind the ear (BTE) | 203 (67.7%) |
| In-the-ear (ITE) | 97 (32.3%) |
| Variables | Mean (SD) | Basic Handling | Advanced Handling | Adjustment | Aided Listening | Overall Score |
|---|---|---|---|---|---|---|
| Basic handling | 73.76 (21.94) | 1 | ||||
| Advanced handling | 40.03 (23.05) | 0.67 * | 1 | |||
| Adjustment | 67.01 (24.97) | 0.46 * | 0.45 * | 1 | ||
| Aided listening | 72.03 (17.39) | 0.29 * | 0.30 * | 0.48 * | 1 | |
| Overall score | 65.24 (15.94) | 0.81 * | 0.78 * | 0.71 * | 0.71 * | 1 |
| Reliability (Cronbach’s Alpha) | - | 0.90 | 0.83 | 0.87 | 0.93 | 0.93 |
| Variables. | Mean (SD) | T/F Statistic | p-Value | |
|---|---|---|---|---|
| Gender | Male | 64.77 (14.45) | −0.49 | 0.62 |
| Female | 65.69 (17.30) | |||
| Marital status | Single | 60.40 (17.05) | 4.75 | 0.009 * |
| Married | 66.48 (15.21) | |||
| Divorced or widowed | 69.76 (16.54) | |||
| Education | Illiterate | 60.37 (18.25) | 5.36 | 0.001 * |
| Primary | 60.19 (14.24) | |||
| Secondary | 67.05 (15.78) | |||
| Diploma | 66.94 (15.25) | |||
| Higher education | 71.70 (14.15) | |||
| Degree of hearing impairment (WEA) | 26–40 dB HL | 66.88 (21.56) | 4.91 | 0.002 * |
| 41–55 dB HL | 67.44 (13.34) | |||
| 56–70 dB HL | 66.74 (16.03) | |||
| 71 dB HL | 58.34 (16.63) | |||
| Hearing-aid fitting | Unilateral | 66.17 (16.92) | 0.7 | 0.48 |
| Bilateral | 64.79 (15.42) | |||
| Types of hearing aids | Digital | 66.61 (15.21) | 4.91 | 0.008 * |
| Programmable | 60.13 (18.54) | |||
| Analog | 58.12 (17.50) | |||
| Style of hearing aid | Behind the ear (BTE) | 62.14 (16.30) | 25.74 | 0.001 * |
| In-the-ear (ITE) | 71.73 (12.99) | |||
| Model | χ2/df | CFI | PCFI | RMSEA | GFI | IFI |
|---|---|---|---|---|---|---|
| Recommended value | ˂5 | ≥0.9 | ˃0.5 | <0.1 | ≥0.9 | 0–1 |
| P-MARS-HA | 4.02 | 0.93 | 0.67 | 0.09 | 0.901 | 0.89 |
| Path | Standardized Regression Coefficient | Standard Error | C.R Statistic | p Value | |
|---|---|---|---|---|---|
| 1 | AL1<— Aided listening | 0.64 | |||
| 2 | AL2<— Aided listening | 0.74 | 0.10 | 11.36 | 0.001 * |
| 3 | AL3<— Aided listening | 0.69 | 0.12 | 10.76 | 0.001 * |
| 4 | AL4<— Aided listening | 0.87 | 0.13 | 12.90 | 0.001 * |
| 5 | AL 5<— Aided listening | 0.92 | 0.14 | 13.45 | 0.001 * |
| 6 | AL 6<— Aided listening | 0.84 | 0.13 | 12.58 | 0.001 * |
| 7 | AL 7<— Aided listening | 0.85 | 0.13 | 12.73 | 0.001 * |
| 8 | AL8<— Aided listening | 0.79 | 0.13 | 12.09 | 0.001 * |
| 9 | AL 9<— Aided listening | 0.69 | 0.12 | 10.74 | 0.001 * |
| 10 | BH1<— Basic handling | 0.94 | 0.001 * | ||
| 11 | BH2<— Basic handling | 0.95 | 0.02 | 34.38 | 0.001 * |
| 12 | BH3<— Basic handling | 0.72 | 0.05 | 16.32 | 0.001 * |
| 13 | BH4<— Basic handling | 0.80 | 0.03 | 20.68 | 0.001 * |
| 14 | BH5<— Basic handling | 0.61 | 0.04 | 12.61 | 0.001 * |
| 15 | BH6<— Basic handling | 0.51 | 0.05 | 10.03 | 0.001 * |
| 16 | BH7<— Basic handling | 0.71 | 0.04 | 16.05 | 0.001 * |
| 17 | Ad1<— Adjustment | 0.86 | 0.001 * | ||
| 18 | Ad2<— Adjustment | 0.90 | 0.06 | 18.40 | 0.001 * |
| 19 | Ad3<— Adjustment | 0.74 | 0.05 | 14.74 | 0.001 * |
| 20 | AH1<— Advanced handling | 0.77 | 0.001 * | ||
| 21 | AH2<— Advanced handling | 0.79 | 0.07 | 12.76 | 0.001 * |
| 22 | AH3<— Advanced handling | 0.63 | 0.06 | 10.38 | 0.001 * |
| 23 | AH4<— Advanced handling | 0.62 | 0.08 | 10.31 | 0.001 * |
| 24 | AH5<— Advanced handling | 0.58 | 0.05 | 9.37 | 0.001 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jorbonyan, A.; Abolfathi Momtaz, Y.; Foroughan, M.; Mehrkian, S. Translation, Cross-Cultural Adaptation, and Psychometric Properties of the Persian Version of the Measure of Audiologic Rehabilitation Self-Efficacy for Hearing Aids (P-MARS-HA). Audiol. Res. 2025, 15, 31. https://doi.org/10.3390/audiolres15020031
Jorbonyan A, Abolfathi Momtaz Y, Foroughan M, Mehrkian S. Translation, Cross-Cultural Adaptation, and Psychometric Properties of the Persian Version of the Measure of Audiologic Rehabilitation Self-Efficacy for Hearing Aids (P-MARS-HA). Audiology Research. 2025; 15(2):31. https://doi.org/10.3390/audiolres15020031
Chicago/Turabian StyleJorbonyan, Abdolhakim, Yadollah Abolfathi Momtaz, Mahshid Foroughan, and Saeideh Mehrkian. 2025. "Translation, Cross-Cultural Adaptation, and Psychometric Properties of the Persian Version of the Measure of Audiologic Rehabilitation Self-Efficacy for Hearing Aids (P-MARS-HA)" Audiology Research 15, no. 2: 31. https://doi.org/10.3390/audiolres15020031
APA StyleJorbonyan, A., Abolfathi Momtaz, Y., Foroughan, M., & Mehrkian, S. (2025). Translation, Cross-Cultural Adaptation, and Psychometric Properties of the Persian Version of the Measure of Audiologic Rehabilitation Self-Efficacy for Hearing Aids (P-MARS-HA). Audiology Research, 15(2), 31. https://doi.org/10.3390/audiolres15020031