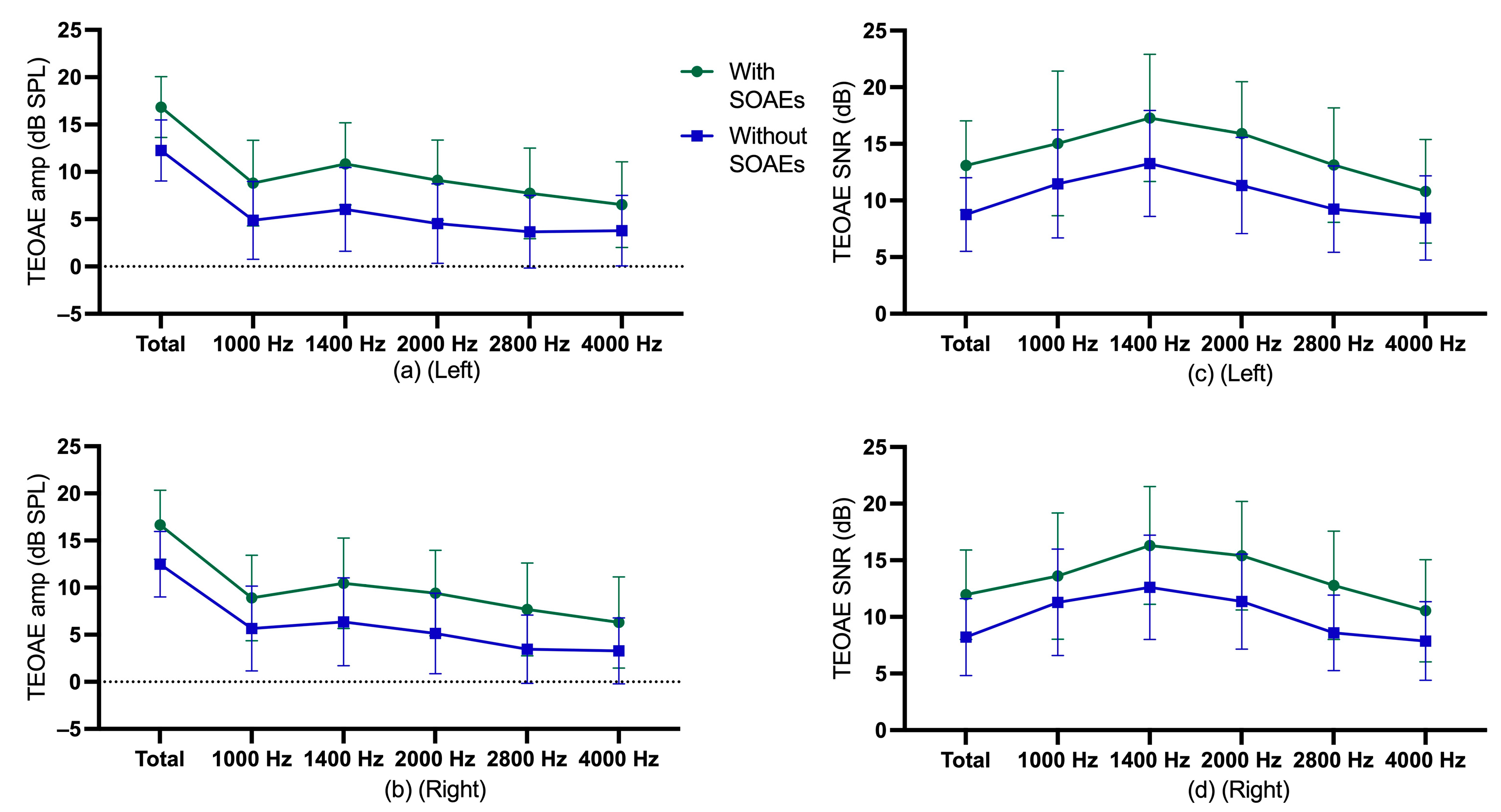
3.2. TEOAE Findings
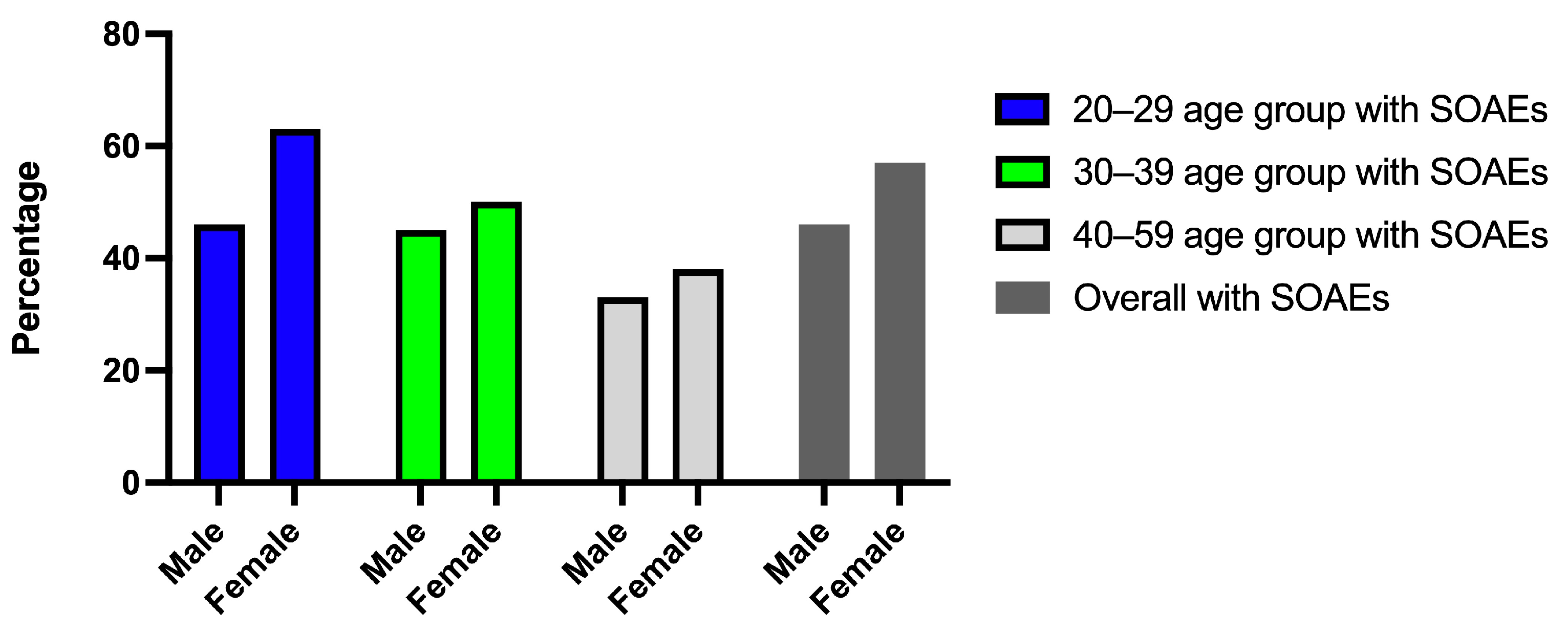
Descriptive statistics for TEOAE amplitude and SNR of participants with and without SOAEs are shown in
Figure 2, and descriptive statistics for gender and age group are shown in
Supplementary Figure S3.
For the left ears, multiple regressions were performed for TEOAE amplitude and SNR in terms of age, gender, and SOAE status. The multiple regression model showed statistically significant in examining TEOAE amplitude,
F = 77.71,
p < 0.0005, adj R
2 = 0.35. Age, gender, and SOAE status contributed statistically significantly to the model,
p < 0.001. The multiple regression model was statistically significant in examining TEOAE SNR,
F = 58.97,
p < 0.0005, adj R
2 = 0.29. Age, gender, and SOAE status contributed statistically significantly to the explanation,
p < 0.001. Regression coefficients and standard errors can be found in the
Supplementary Table S2.
For the right ears, multiple regressions were performed for TEOAE amplitude and SNR in terms of age, gender, and SOAE status. The multiple regression model was statistically significant in examining TEOAE amplitude,
F = 59.49,
p < 0.0005, adj R
2 = 0.28. Age, gender, and SOAE status contributed statistically significantly to the explanation,
p < 0.001. The multiple regression model was statistically significant in examining TEOAE SNR,
F = 42.36,
p < 0.0005, adj R
2 = 0.22. Age, gender, and SOAE status contributed statistically significantly to the explanation,
p < 0.001. Regression coefficients and standard errors can be found in the
Supplementary Table S3.
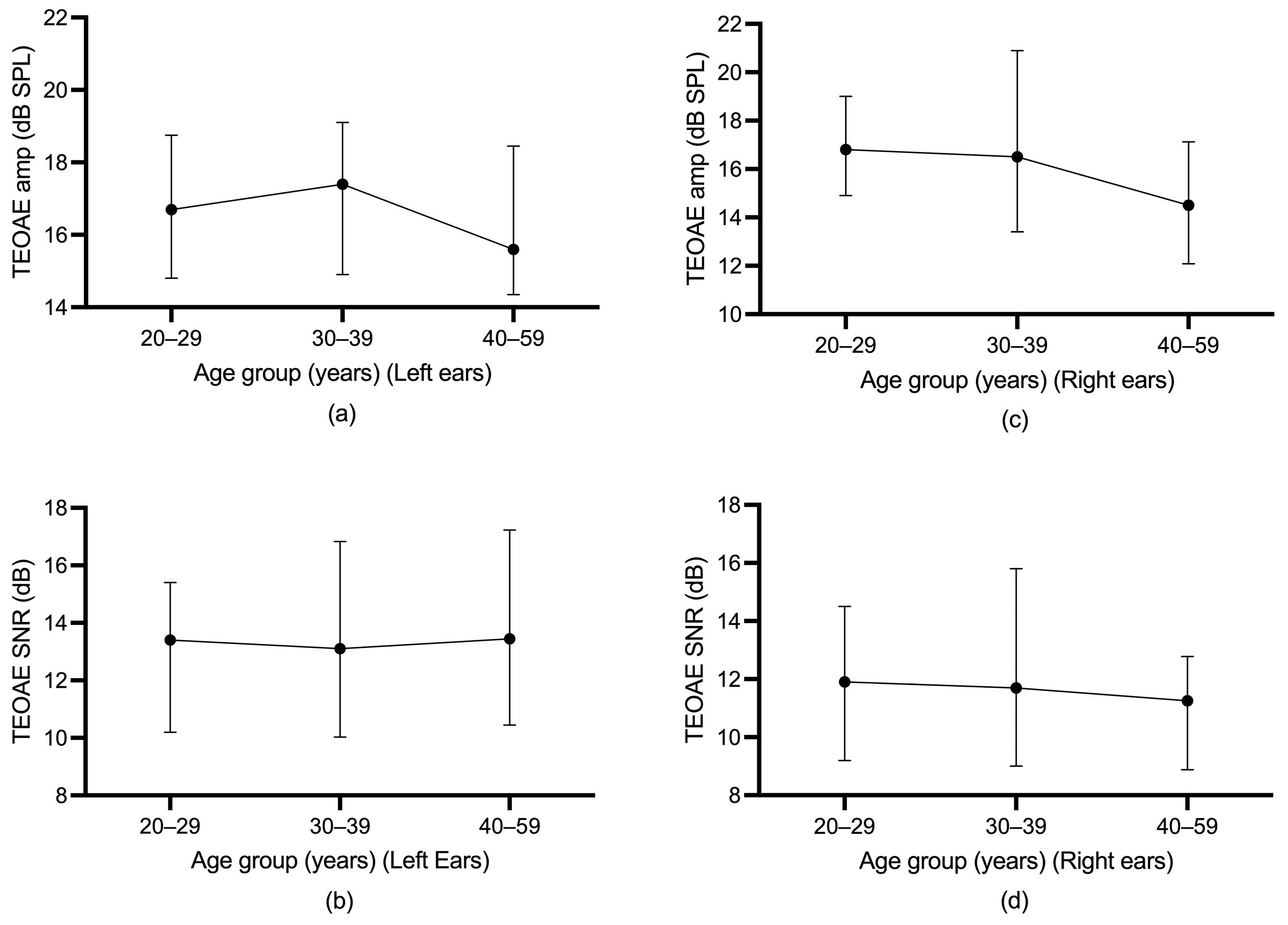
Differences in TEOAE parameters (amplitude and SNR) among the three age groups were evaluated using the Jonckheere–Terpstra test. For participants without SOAEs, a statistically significant downward trend in total TEOAE amplitude in the left ear was found across age groups,
p = 0.001, and the Spearman correlation between total TEOAE amplitude and age group was
r = −0.195. A statistically significant downward trend in total TEOAE SNR in the left ear was also found across age groups,
p < 0.0005, and the Spearman correlation between total TEOAE SNR and age group was
r = −0.236. For participants without SOAEs, a statistically significant downward trend in total TEOAE amplitude in the right ear was found across age groups,
p = 0.030), and the Spearman correlation between total TEOAE amplitude and age group was
r = −0.141. A statistically significant downward trend in total TEOAE SNR in the right ear was also found across age groups,
p = 0.004, and the Spearman correlation between total TEOAE SNR and age group was
r = −0.186. For participants with SOAEs, however, a statistically significant trend in total TEOAE amplitude and total SNR over age group was not found.
Figure 3 and
Figure 4 illustrate the age trends for participants with or without SOAEs.
A Spearman correlation test was conducted to determine the age effect for TEOAEs in participants with SOAEs or without SOAEs. In general, the Spearman correlation test did not find significant results for participants with SOAEs in the left ears. For right ears, no significant results were found for participants with SOAEs. However, for participants without SOAEs, the Spearman correlation test found a significant negative correlation in TEOAE test parameters in the left and right ears.
Supplementary Table S4 shows the results of the Spearman correlation test between TEOAEs and age for the left and right ears.
3.3. DPOAE Findings
Descriptive statistics for DPOAE amplitude and SNR of participants with and without SOAEs are shown in
Figure 5, and descriptive statistics for gender and age group are shown in
Supplementary Figures S4 and S5.
For the left ears, multiple regressions were performed for DPOAE amplitude and SNR at overall average frequency, low average frequency, middle average frequency, and high average frequency in terms of age, gender, and SOAE status. The multiple regression model was statistically significant in examining DPOAE amplitude (
F = 26.18,
p < 0.0005, adj R
2 = 0.15) and SNR (
F = 17.65,
p < 0.0005, adj R
2 = 0.10) at overall average frequency. Age and SOAE status contributed statistically significantly to the model,
p < 0.0005. Similarly, for low average frequency, the multiple regression model was statistically significant in examining DPOAE amplitude (
F = 22.94,
p < 0.0005, adj R
2 = 0.13) and SNR (
F = 11.98,
p < 0.0005, adj R
2 = 0.08). Age and SOAE status contributed statistically significantly to the model,
p < 0.01. For middle average frequency, the multiple regression model was statistically significant in examining DPOAE amplitude (
F = 28.92,
p < 0.0005, adj R
2 = 0.17) and SNR (
F = 23.06,
p < 0.0005, adj R
2 = 0.14). Age and SOAE status contributed statistically significantly to the model,
p < 0.0005. For high average frequency, the multiple regression model was statistically significant in examining DPOAE amplitude (
F = 4.52,
p = 0.004, adj R
2 = 0.04) and SNR (
F = 3.67,
p = 0.012, adj R
2 = 0.03). Age contributed statistically significantly to the model,
p < 0.0005. Regression coefficients and standard errors can be found in
Supplementary Table S5.
For the right ears, multiple regressions were performed for DPOAE amplitude and SNR at overall average frequency, low average frequency, middle average frequency, and high average frequency in terms of age, gender, and SOAE status. The multiple regression model was statistically significant in examining DPOAE amplitude (
F = 29.47,
p < 0.0005, adj R
2 = 0.16) and SNR (
F = 17.34,
p < 0.0005, adj R
2 = 0.10) at overall average frequency. Age and SOAE status contributed statistically significantly to the model,
p < 0.01. For low average frequency, the multiple regression model was statistically significant in examining DPOAE amplitude (
F = 20.35,
p < 0.0005, adj R
2 = 0.11), age and SOAE status contributed statistically significantly to the model,
p < 0.01. For DPOAE SNR at low average frequency, the multiple regression model was statistically significant in examining DPOAE SNR (
F = 9.23,
p < 0.0005, adj R
2 = 0.05), SOAE status contributed statistically significantly to the model,
p < 0.0005. For middle average frequency, the multiple regression model was statistically significant in examining DPOAE amplitude (
F = 27.59,
p < 0.0005, adj R
2 = 0.16) and SNR (
F = 19.95,
p < 0.0005, adj R
2 = 0.12). Age and SOAE status contributed statistically significantly to the model,
p < 0.01. For high average frequency, the multiple regression model was statistically significant in examining DPOAE amplitude (
F = 7.56,
p < 0.0005, adj R
2 = 0.05) and SNR (
F = 5.91,
p = 0.001, adj R
2 = 0.04). Age and SOAE status contributed statistically significantly to the model,
p < 0.05. Regression coefficients and standard errors can be found in
Supplementary Table S6.
Spearman correlation tests were conducted to determine the age effect for DPOAEs in participants with SOAEs or without SOAEs. In general, the Spearman correlation tests did not find significant results for participants with SOAEs in left ears. For participants with SOAEs in right ears, significant negative correlations were found for DPOAE amplitude and SNR at middle average frequencies and high average frequencies. However, for participants without SOAEs, Spearman correlation tests found significant negative correlations for most DPOAE parameters (amplitude and SNR) in left and right ears.
Table 1 and
Table 2 show the results of Spearman correlation tests between DPOAEs and age for left and right ears.
Age differences among the three age groups were evaluated using the Jonckheere–Terpstra test. The results of average frequency, average low frequency, average mid frequency and average high frequency are presented in
Table 3 and
Table 4. For participants without SOAEs, a statistically significant downward trend in average frequency, average low frequency, average mid-frequency and average high-frequency DPOAE amplitudes and SNR was found across age groups. However, for participants with SOAEs, a significant downward trend was found at only a few frequencies, and no statistically significant trends in DPOAE amplitudes and SNR were found at most frequencies across age groups.
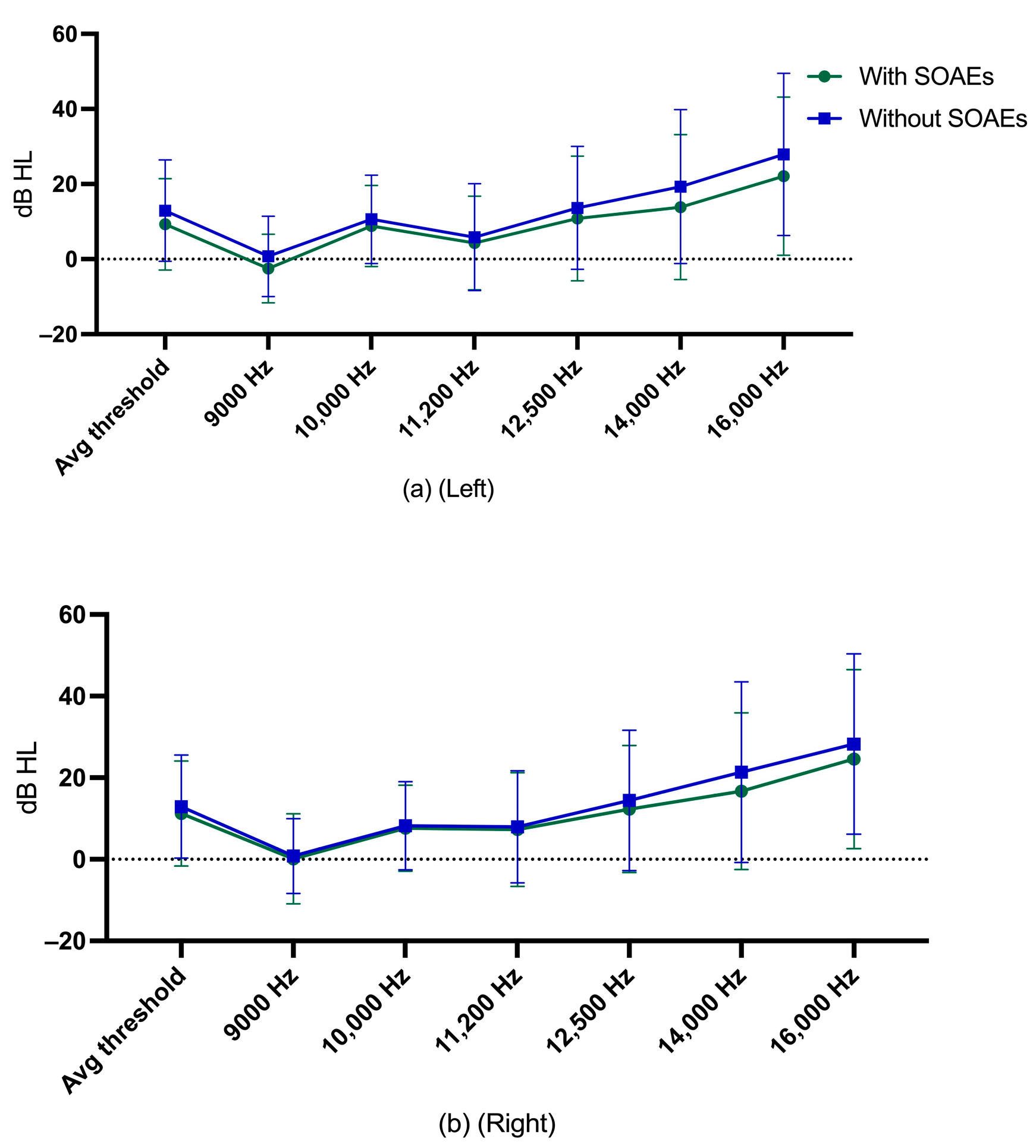
3.4. Extended High-Frequency Hearing Thresholds
Descriptive statistics for EHF hearing thresholds of participants with and without SOAEs are shown in
Figure 6.
Multiple regression was run separately for the left and right ears to examine average EHF hearing thresholds from age, gender, and SOAE status. The multiple regression model was statistically significant in examining average EHF hearing threshold in left ears,
F = 153.67,
p < 0.0005, adj R
2 = 0.50. Age contributed statistically significantly to the model,
p < 0.0005. For the right ears, the multiple regression model was statistically significant in examining average EHF hearing threshold,
F = 119.21,
p < 0.0005, adj R
2 = 0.44. Age contributed statistically significantly to the model,
p < 0.0005. Regression coefficients and standard errors can be found in
Supplementary Table S7.
Spearman’s correlation tests were used to examine the relationship between EHF hearing thresholds and age. All EHF hearing thresholds had a significant positive correlation with age. EHF hearing thresholds increased with age, regardless of the presence or absence of SOAEs.
Table 5 and
Table 6 show the results of Spearman’s correlation test for EHF hearing thresholds in left or right ears for participants with or without SOAEs.
Jonckheere–Terpstra tests were also used to assess trends across age groups in EHF hearing thresholds among participants with or without SOAEs. Findings were similar to Spearman’s correlation test results, with participants having higher EHF hearing thresholds with older age groups, regardless of whether they had SOAEs or not.
Table 7 and
Table 8 show the Jonckheere–Terpstra test results for participants with or without SOAEs in each EHF hearing threshold in left or right ears.







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}