
Neuropsychological Functions and Audiological Findings in Elderly Cochlear Implant Users: The Role of Attention in Postoperative Performance


 ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Study Design
2.2. Procedure
2.2.1. Audiological Assessment
2.2.2. Cognitive Assessment
2.3. Statistical Analysis
3. Results
3.1. Outcomes of Attention Assessment and Their Comparison with Audiological/Cognitive Data
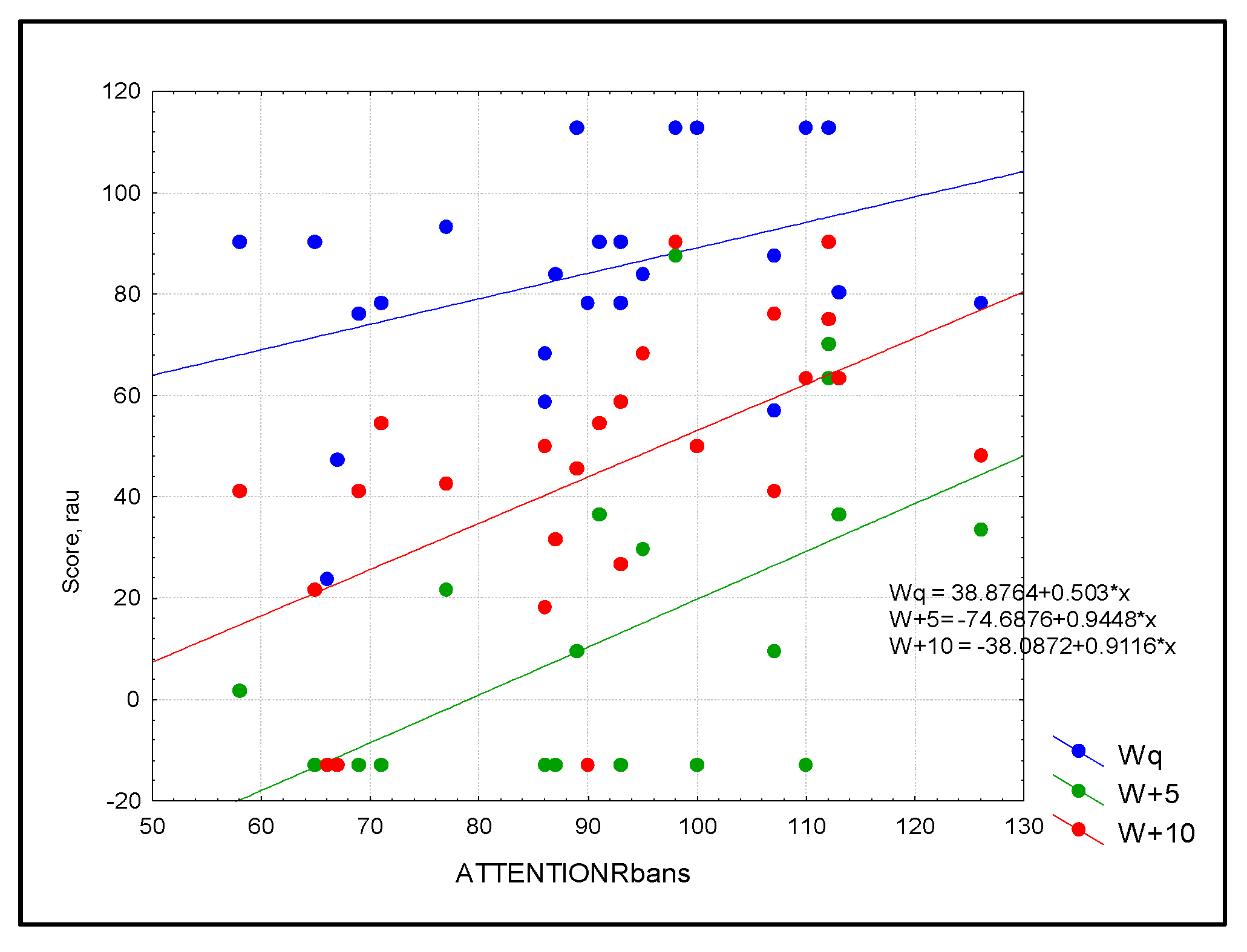
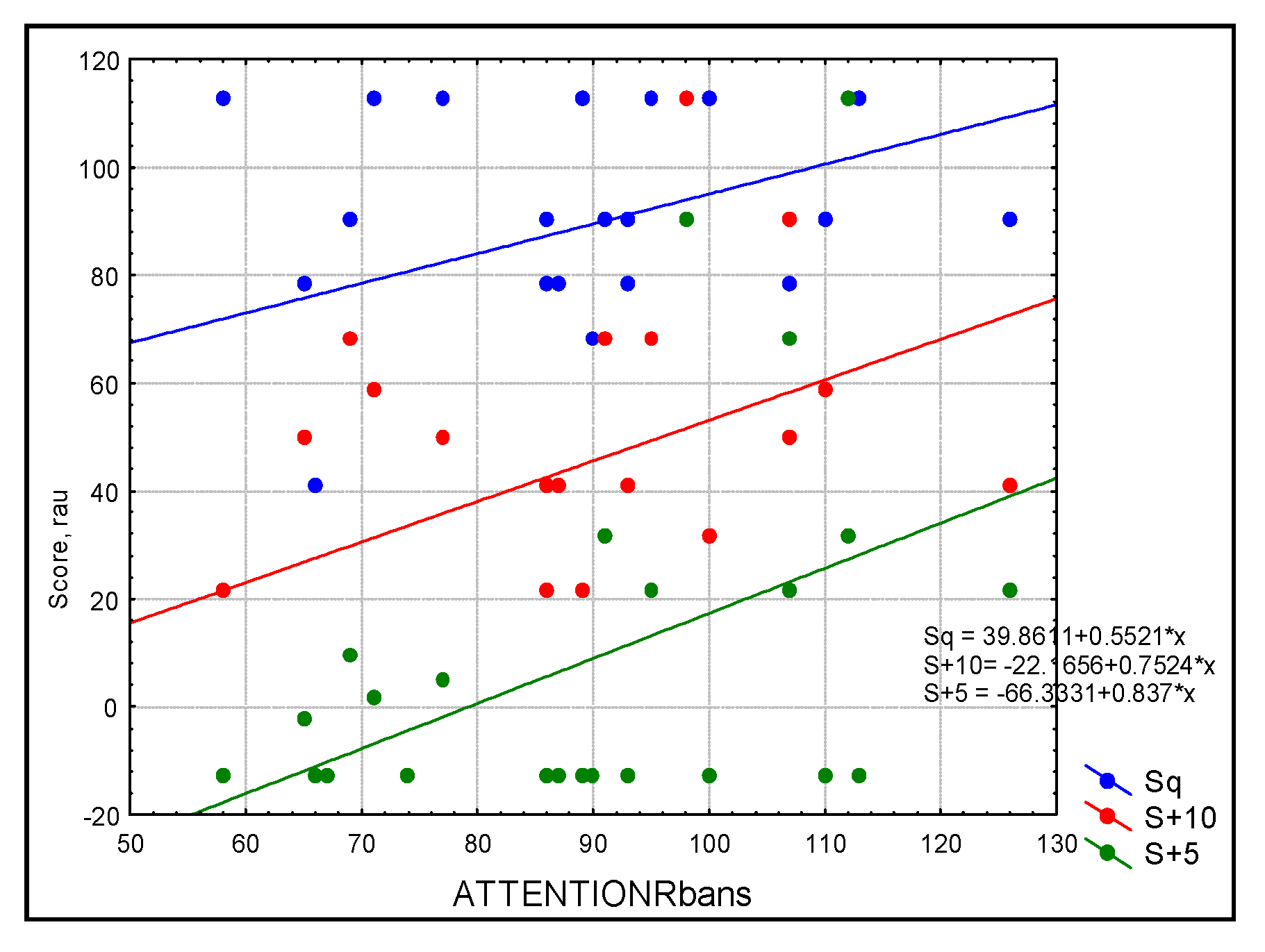
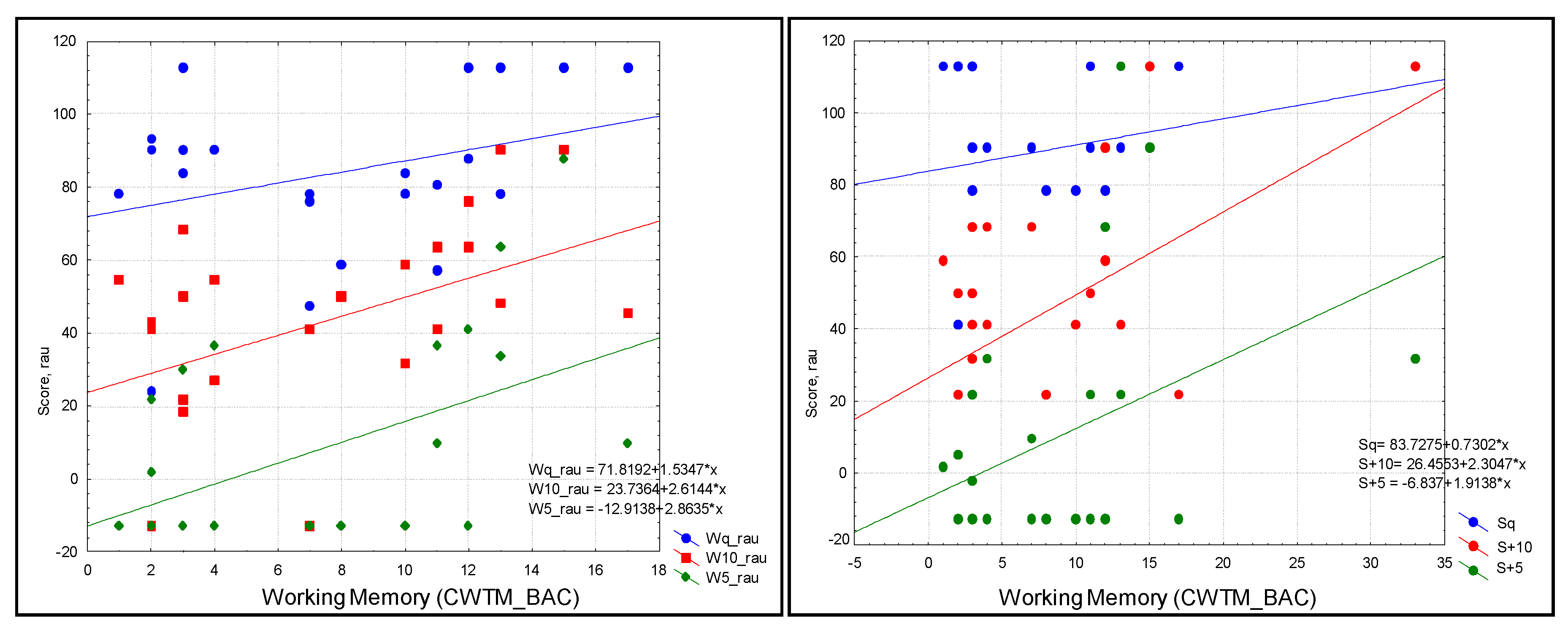
3.2. Correlations and Regressions
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Diao, T.; Ma, X.; Zhang, J.; Duan, M.; Yu, L. The Correlation between Hearing Loss, Especially High-Frequency Hearing Loss and Cognitive Decline Among the Elderly. Front. Neurosci. 2021, 15, 750874. [Google Scholar] [CrossRef] [PubMed]
- Livingston, G.; Sommerlad, A.; Orgeta, V.; Costafreda, S.G.; Huntley, J.; Ames, D.; Ballard, C.; Banerjee, S.; Burns, A.; Cohen-Mansfield, J.; et al. Dementia prevention, intervention, and care. Lancet 2017, 390, 2673–2734. [Google Scholar] [CrossRef] [PubMed]
- Calvino, M.; Sánchez-Cuadrado, I.; Gavilán, J.; Gutiérrez-Revilla, M.A.; Polo, R.; Lassaletta, L. Effect of cochlear implantation on cognitive decline and quality of life in younger and older adults with severe-to-profound hearing loss. Eur. Arch. Oto-Rhino-Laryngol. 2022, 279, 4745–4759. [Google Scholar] [CrossRef]
- Uchida, Y.; Sugiura, S.; Nishita, Y.; Saji, N.; Sone, M.; Ueda, H. Age-related hearing loss and cognitive decline—The potential mechanisms linking the two. Auris Nasus Larynx 2019, 46, 1–9. [Google Scholar] [CrossRef]
- Lin, F.R. Hearing loss and cognition among older adults in the United States. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2011, 66, 1131–1136. [Google Scholar] [CrossRef]
- Lin, F.R.; Ferrucci, L.; Metter, E.J.; An, Y.; Zonderman, A.B.; Resnick, S.M. Hearing loss and cognition in the Baltimore Longitudinal Study of Aging. Neuropsychology 2011, 25, 763–770. [Google Scholar] [CrossRef]
- Cherko, M.; Hickson, L.; Bhutta, M. Auditory deprivation and health in the elderly. Maturitas 2016, 88, 52–57. [Google Scholar] [CrossRef]
- Mudar, R.A.; Husain, F.T. Neural Alterations in Acquired Age-Related Hearing Loss. Front. Psychol. 2016, 7, 828. [Google Scholar] [CrossRef]
- Wayne, R.V.; Johnsrude, I.S. A review of causal mechanisms underlying the link between age-related hearing loss and cognitive decline. Ageing Res. Rev. 2015, 23, 154–166. [Google Scholar] [CrossRef]
- Peelle, J.E.; Troiani, V.; Grossman, M.; Wingfield, A. Hearing loss in older adults affects neural systems supporting speech comprehension. J. Neurosci. 2011, 31, 12638–12643. [Google Scholar] [CrossRef]
- Lin, F.R.; Yaffe, K.; Xia, J.; Xue, Q.L.; Harris, T.B.; Purchase-Helzner, E.; Satterfield, S.; Ayonayon, H.N.; Ferrucci, L.; Simonsick, E.M.; et al. Hearing loss and cognitive decline in older adults. JAMA Intern. Med. 2013, 173, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Lindenberger, U.; Baltes, P.B. Sensory functioning and intelligence in old age: A strong connection. Psychol. Aging 1994, 9, 339–355. [Google Scholar] [CrossRef] [PubMed]
- Moore, B.C. A review of the perceptual effects of hearing loss for frequencies above 3 kHz. Int. J. Audiol. 2016, 55, 707–714. [Google Scholar] [CrossRef] [PubMed]
- Kramer, S.; Vasil, K.J.; Adunka, O.F.; Pisoni, D.B.; Moberly, A.C. Cognitive Functions in Adult Cochlear Implant Users, Cochlear Implant Candidates, and Normal-Hearing Listeners. Laryngoscope Investig. Otolaryngol. 2018, 3, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Boisvert, I.; Reis, M.; Au, A.; Cowan, R.; Dowell, R.C. Cochlear implantation outcomes in adults: A scoping review. PLoS ONE 2020, 15, e0232421. [Google Scholar] [CrossRef]
- Völter, C.; Götze, L.; Bajewski, M.; Dazert, S.; Thomas, J.P. Cognition and Cognitive Reserve in Cochlear Implant Recipients. Front. Aging Neurosci. 2022, 14, 838214. [Google Scholar] [CrossRef]
- Miller, G.; Miller, C.; Marrone, N.; Howe, C.; Fain, M.; Jacob, A. The impact of cochlear implantation on cognition in older adults: A systematic review of clinical evidence. BMC Geriatr. 2015, 15, 16. [Google Scholar] [CrossRef]
- Mosnier, I.; Bebear, J.P.; Marx, M.; Fraysse, B.; Truy, E.; Lina-Granade, G.; Mondain, M.; Sterkers-Artières, F.; Bordure, P.; Robier, A.; et al. Improvement of cognitive function after cochlear implantation in elderly patients. JAMA Otolaryngol.-Head Neck Surg. 2015, 141, 442–450. [Google Scholar] [CrossRef]
- Cosetti, M.K.; Pinkston, J.B.; Flores, J.M.; Friedmann, D.R.; Jones, C.B.; Roland, J.T., Jr.; Waltzman, S.B. Neurocognitive testing and cochlear implantation: Insights into performance in older adults. Clin. Interv. Aging 2016, 11, 603–613. [Google Scholar] [CrossRef]
- Castiglione, A.; Benatti, A.; Velardita, C.; Favaro, D.; Padoan, E.; Severi, D.; Pagliaro, M.; Bovo, R.; Vallesi, A.; Gabelli, C.; et al. Aging, Cognitive Decline and Hearing Loss: Effects of Auditory Rehabilitation and Training with Hearing Aids and Cochlear Implants on Cognitive Function and Depression among Older Adults. Audiol. Neuro-Otol. 2016, 21 (Suppl. 1), 21–28. [Google Scholar] [CrossRef]
- Sonnet, M.H.; Montaut-Verient, B.; Niemier, J.Y.; Hoen, M.; Ribeyre, L.; Parietti-Winkler, C. Cognitive Abilities and Quality of Life After Cochlear Implantation in the Elderly. Otol. Neurotol. 2017, 38, e296–e301. [Google Scholar] [CrossRef] [PubMed]
- Sarant, J.; Harris, D.; Busby, P.; Maruff, P.; Schembri, A.; Dowell, R.; Briggs, R. The Effect of Cochlear Implants on Cognitive Function in Older Adults: Initial Baseline and 18-Month Follow up Results for a Prospective International Longitudinal Study. Front. Neurosci. 2019, 13, 789. [Google Scholar] [CrossRef]
- Völter, C.; Götze, L.; Haubitz, I.; Müther, J.; Dazert, S.; Thomas, J.P. Impact of Cochlear Implantation on Neurocognitive Subdomains in Adult Cochlear Implant Recipients. Audiol. Neuro-Otol. 2021, 26, 236–245. [Google Scholar] [CrossRef]
- Claes, A.J.; Van de Heyning, P.; Gilles, A.; Van Rompaey, V.; Mertens, G. Cognitive outcomes after cochlear implantation in older adults: A systematic review. Cochlear Implant. Int. 2018, 19, 239–254. [Google Scholar] [CrossRef] [PubMed]
- Ambert-Dahan, E.; Routier, S.; Marot, L.; Bouccara, D.; Sterkers, O.; Ferrary, E.; Mosnier, I. Cognitive Evaluation of Cochlear Implanted Adults Using CODEX and MoCA Screening Tests. Otol. Neurotol. 2017, 38, e282–e284. [Google Scholar] [CrossRef] [PubMed]
- Jayakody, D.M.P.; Friedland, P.L.; Nel, E.; Martins, R.N.; Atlas, M.D.; Sohrabi, H.R. Impact of cochlear implantation on cognitive functions of older adults: Pilot test results. Otol. Neurotol. 2017, 38, e289–e295. [Google Scholar] [CrossRef]
- Moberly, A.C.; Harris, M.S.; Boyce, L.; Nittrouer, S. Speech Recognition in Adults with Cochlear Implants: The Effects of Working Memory, Phonological Sensitivity, and Aging. J. Speech Lang. Hear. Res. JSLHR 2017, 60, 1046–1061. [Google Scholar] [CrossRef]
- Holden, L.K.; Finley, C.C.; Firszt, J.B.; Holden, T.A.; Brenner, C.; Potts, L.G.; Gotter, B.D.; Vanderhoof, S.S.; Mispagel, K.; Heydebrand, G.; et al. Factors affecting open-set word recognition in adults with cochlear implants. Ear Hear. 2013, 34, 342–360. [Google Scholar] [CrossRef]
- Kenway, B.; Tam, Y.C.; Vanat, Z.; Harris, F.; Gray, R.; Birchall, J.; Carlyon, R.; Axon, P. Pitch Discrimination: An Independent Factor in Cochlear Implant Performance Outcomes. Otol. Neurotol. 2015, 36, 1472–1479. [Google Scholar] [CrossRef]
- Moberly, A.C.; Vasil, K.J.; Wucinich, T.L.; Safdar, N.; Boyce, L.; Roup, C.; Holt, R.F.; Adunka, O.F.; Castellanos, I.; Shafiro, V.; et al. How does aging affect recognition of spectrally degraded speech? Laryngoscope 2018, 128, 1–44. [Google Scholar] [CrossRef]
- Völter, C.; Oberländer, K.; Carroll, R.; Dazert, S.; Lentz, B.; Martin, R.; Thomas, J.P. Nonauditory Functions in Low-performing Adult Cochlear Implant Users. Otol. Neurotol. 2021, 42, e543–e551. [Google Scholar] [CrossRef] [PubMed]
- Akeroyd, M.A. Are individual differences in speech reception related to individual differences in cognitive ability? A survey of twenty experimental studies with normal and hearing-impaired adults. Int. J. Audiol. 2008, 47 (Suppl. 2), S53–S71. [Google Scholar] [CrossRef] [PubMed]
- Pichora-Fuller, M.K.; Souza, P.E. Effects of aging on auditory processing of speech. Int. J. Audiol. 2003, 42 (Suppl. 2), 2S11–2S16. [Google Scholar] [CrossRef] [PubMed]
- Zhan, K.Y.; Lewis, J.H.; Vasil, K.J.; Tamati, T.N.; Harris, M.S.; Pisoni, D.B.; Kronenberger, W.G.; Ray, C.; Moberly, A.C. Cognitive Functions in Adults Receiving Cochlear Implants: Predictors of Speech Recognition and Changes after Implantation. Otol. Neurotol. 2020, 41, e322–e329. [Google Scholar] [CrossRef]
- Robinson, O.J.; Vytal, K.; Cornwell, B.R.; Grillon, C. The impact of anxiety upon cognition: Perspectives from human threat of shock studies. Front. Hum. Neurosci. 2013, 7, 203. [Google Scholar] [CrossRef]
- Bopp, K.L.; Verhaeghen, P. Aging and verbal memory span: A meta-analysis. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2005, 60, P223–P233. [Google Scholar] [CrossRef]
- Kumar, N.; Priyadarshi, B. Differential effect of aging on verbal and visuo-spatial working memory. Aging Dis. 2013, 4, 170–177. [Google Scholar]
- Nittrouer, S.; Lowenstein, J.H.; Wucinich, T.; Moberly, A.C. Verbal Working Memory in Older Adults: The Roles of Phonological Capacities and Processing Speed. J. Speech Lang. Hear. Res. JSLHR 2016, 59, 1520–1532. [Google Scholar] [CrossRef]
- Rönnberg, J.; Lunner, T.; Zekveld, A.; Sörqvist, P.; Danielsson, H.; Lyxell, B.; Dahlström, O.; Signoret, C.; Stenfelt, S.; Pichora-Fuller, M.K.; et al. The Ease of Language Understanding (ELU) model: Theoretical, empirical, and clinical advances. Front. Syst. Neurosci. 2013, 7, 31. [Google Scholar] [CrossRef]
- Angelopoulou, E.; Karabatzaki, Z.; Drigas, A. The Role of Working Memory and Attention in Older Workers’ Learning. Int. J. Adv. Corp. Learn. (IJAC) 2021, 14, 4–14. [Google Scholar] [CrossRef]
- Baddeley, A. Working memory. Curr. Biol. 2010, 20, R136–R140. [Google Scholar] [CrossRef]
- Tao, D.; Deng, R.; Jiang, Y.; Galvin, J.J., 3rd; Fu, Q.J.; Chen, B. Contribution of auditory working memory to speech understanding in mandarin-speaking cochlear implant users. PLoS ONE 2014, 9, e99096. [Google Scholar] [CrossRef] [PubMed]
- Oberauer, K. Working Memory and Attention—A Conceptual Analysis and Review. J. Cogn. 2019, 2, 36. [Google Scholar] [CrossRef]
- Chun, M.M.; Golomb, J.D.; Turk-Browne, N.B. A taxonomy of external and internal attention. Annu. Rev. Psychol. 2011, 62, 73–101. [Google Scholar] [CrossRef]
- Baroni, M.R. I Processi Psicologici Dell’Invecchiamento; Carocci Editore: Roma, Italy, 2010. [Google Scholar]
- Jurado, M.B.; Rosselli, M. The elusive nature of executive functions: A review of our current understanding. Neuropsychol. Rev. 2007, 17, 213–233. [Google Scholar] [CrossRef]
- Pliatsikas, C.; Veríssimo, J.; Babcock, L.; Pullman, M.Y.; Glei, D.A.; Weinstein, M.; Goldman, N.; Ullman, M.T. Working memory in older adults declines with age, but is modulated by sex and education. Q. J. Exp. Psychol. 2019, 72, 1308–1327. [Google Scholar] [CrossRef]
- Dazert, S.; Thomas, J.P.; Loth, A.; Zahnert, T.; StöverT. Cochlear Implantation. Dtsch. Arztebl. Int. 2020, 117, 690–700. [Google Scholar] [CrossRef]
- Cutugno, F.; Prosser, S.; Turrini, M. Audiometria Vocale; GN ReSound: Padova, Itay, 2000. [Google Scholar]
- Raven, J.C. Coloured Progressive Matrices; H.K. Lewis: London, UK, 1986. [Google Scholar]
- Belacchi, C.; Scalisi, T.G.; Cannoni, E.; Cornoldi, C. CPM—Coloured Progressive Matrices. Standardizzazione Italiana. Manuale; Giunti O.S.: Florence, Italy, 2008. [Google Scholar]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Santangelo, G.; Siciliano, M.; Pedone, R.; Vitale, C.; Falco, F.; Bisogno, R.; Siano, P.; Barone, P.; Grossi, D.; Santangelo, F.; et al. Normative data for the Montreal Cognitive Assessment in an Italian population sample. Neurol. Sci. 2015, 36, 585–591. [Google Scholar] [CrossRef]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.; Vagg, P.R.; Jacobs, G.A. Manual for the State-Trait Anxiety Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1983. [Google Scholar]
- Monaco, M.; Costa, A.; Caltagirone, C.; Carlesimo, G.A. Forward and backward span for verbal and visuo-spatial data: Standardization and normative data from an Italian adult population. Neurol. Sci. 2013, 34, 749–754. [Google Scholar] [CrossRef]
- De Beni, R.; Borella, E.; Carretti, C.; Marigo, C.; Nava, L. BAC. Benessere e Abilità Cognitive in Età Adulta ed Avanzata; Giunti Psychometrics: Florence, Italy, 2008. [Google Scholar]
- Randolph, C.; Tierney, M.C.; Mohr, E.; Chase, T.N. The Repeatable Battery for the Assessment of Neuropsychological Status (RBANS): Preliminary clinical validity. J. Clin. Exp. Neuropsychol. 1998, 20, 310–319. [Google Scholar] [CrossRef]
- Patton, D.E.; Duff, K.; Schoenberg, M.R.; Mold, J.; Scott, J.G.; Adams, R.L. RBANS index discrepancies: Base rates for older adults. Arch. Clin. Neuropsychol. 2006, 21, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, R.; Rubin, D.B. requivalent: A simple effect size indicator. Psychol. Methods 2003, 8, 492–496. [Google Scholar] [CrossRef] [PubMed]
- Studebaker, G.A. A “rationalized” arcsine transform. J. Speech Hear. Res. 1985, 28, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Strauss, D.J.; Francis, A.L. Toward a taxonomic model of attention in effortful listening. Cogn. Affect. Behav. Neurosci. 2017, 17, 809–825. [Google Scholar] [CrossRef] [PubMed]
- Mancini, P.; Dincer D’Alessandro, H.; Portanova, G.; Atturo, F.; Russo, F.Y.; Greco, A.; de Vincentiis, M.; Giallini, I.; De Seta, D. Bimodal cochlear implantation in elderly patients. Int. J. Audiol. 2021, 60, 469–478. [Google Scholar] [CrossRef]
- Dincer D’Alessandro, H.; Ballantyne, D.; Boyle, P.J.; De Seta, E.; DeVincentiis, M.; Mancini, P. Temporal Fine Structure Processing, Pitch, and Speech Perception in Adult Cochlear Implant Recipients. Ear Hear. 2018, 39, 679–686. [Google Scholar] [CrossRef]
- Boyle, P.J.; Nunn, T.B.; O’Connor, A.F.; Moore, B.C. STARR: A speech test for evaluation of the effectiveness of auditory prostheses under realistic conditions. Ear Hear. 2013, 34, 203–212. [Google Scholar] [CrossRef]
- Moran, M. Arguments for rejecting the sequential Bonferroni in ecological studies. OIKOS 2003, 100, 403–405. [Google Scholar] [CrossRef]
- Claes, A.J.; Van de Heyning, P.; Gilles, A.; Van Rompaey, V.; Mertens, G. Cognitive Performance of Severely Hearing-impaired Older Adults before and after Cochlear Implantation: Preliminary Results of a Prospective, Longitudinal Cohort Study Using the RBANS-H. Otol. Neurotol. 2018, 39, e765–e773. [Google Scholar] [CrossRef]
- Claes, A.J.; Van de Heyning, P.; Gilles, A.; Hofkens-Van den Brandt, A.; Van Rompaey, V.; Mertens, G. Impaired Cognitive Functioning in Cochlear Implant Recipients over the Age of 55 Years: A Cross-Sectional Study Using the Repeatable Battery for the Assessment of Neuropsychological Status for Hearing-Impaired Individuals (RBANS-H). Front. Neurosci. 2018, 12, 580. [Google Scholar] [CrossRef] [PubMed]
- Vasil, K.J.; Ray, C.; Lewis, J.; Stefancin, E.; Tamati, T.N.; Moberly, A.C. How Does Cochlear Implantation Lead to Improvements on a Cognitive Screening Measure? J. Speech Lang. Hear. Res. JSLHR 2021, 64, 1053–1061. [Google Scholar] [CrossRef]
- Oberauer, K. Design for a working memory. Psychol. Learn. Motiv. Adv. Res. Theory 2009, 51, 45–100. [Google Scholar] [CrossRef]
- Pichora-Fuller, M.K.; Schneider, B.A.; Daneman, M. How young and old adults listen to and remember speech in noise. J. Acoust. Soc. Am. 1995, 97, 593–608. [Google Scholar] [CrossRef] [PubMed]
- Wingfield, A.; Grossman, M. Language and the aging brain: Patterns of neural compensation revealed by functional brain imaging. J. Neurophysiol. 2006, 96, 2830–2839. [Google Scholar] [CrossRef] [PubMed]
- Pisoni, D.B.; Cleary, M. Measures of working memory span and verbal rehearsal speed in deaf children after cochlear implantation. Ear Hear. 2003, 24 (Suppl. 1), 106S–120S. [Google Scholar] [CrossRef]
- Choi, C.T.M.; Lee, Y. A Review of Stimulating Strategies for Cochlear Implants. In Cochlear Implant Research Updates; IntechOpen: London, UK, 2012. [Google Scholar] [CrossRef]
- Middlebrooks, J.C.; Bierer, J.A.; Snyder, R.L. Cochlear implants: The view from the brain. Curr. Opin. Neurobiol. 2005, 15, 488–493. [Google Scholar] [CrossRef]
- Kral, A.; O’Donoghue, G.M. Profound deafness in childhood. N. Engl. J. Med. 2010, 363, 1438–1450. [Google Scholar] [CrossRef]
- Rönnberg, J.; Rudner, M.; Foo, C.; Lunner, T. Cognition counts: A working memory system for ease of language understanding (ELU). Int. J. Audiol. 2008, 47 (Suppl. 2), S99–S105. [Google Scholar] [CrossRef]
- Lyxell, B.; Andersson, J.; Andersson, U.; Arlinger, S.; Bredberg, G.; Harder, H. Phonological representation and speech understanding with cochlear implants in deafened adults. Scand. J. Psychol. 1998, 39, 175–179. [Google Scholar] [CrossRef]
- Nicastri, M.; Giallini, I.; Inguscio, B.; Turchetta, R.; Guerzoni, L.; Cuda, D.; Portanova, G.; Ruoppolo, G.; Dincer D’Alessandro, H.; Mancini, P. The influence of auditory selective attention on linguistic outcomes in deaf and hard of hearing children with cochlear implants. Eur. Arch. Oto-Rhino-Laryngol. 2023, 280, 115–124. [Google Scholar] [CrossRef]
- McDermott, J.H. The cocktail party problem. Curr. Biol. CB 2009, 19, R1024–R1027. [Google Scholar] [CrossRef] [PubMed]
- Shinn-Cunningham, B.G. Object-based auditory and visual attention. Trends Cogn. Sci. 2008, 12, 182–186. [Google Scholar] [CrossRef]
- Zahodne, L.B.; Stern, Y.; Manly, J.J. Differing effects of education on cognitive decline in diverse elders with low versus high educational attainment. Neuropsychology 2015, 29, 649–657. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.S.; Yu, L.; Lamar, M.; Schneider, J.A.; Boyle, P.A.; Bennett, D.A. Education and cognitive reserve in old age. Neurology 2019, 92, e1041–e1050. [Google Scholar] [CrossRef]
- Stern, Y.; Arenaza-Urquijo, E.M.; Bartrés-Faz, D.; Belleville, S.; Cantilon, M.; Chetelat, G.; Ewers, M.; Franzmeier, N.; Kempermann, G.; Kremen, W.S.; et al. Whitepaper: Defining and investigating cognitive reserve, brain reserve, and brain maintenance. Alzheimer’s Dement. 2020, 16, 1305–1311. [Google Scholar] [CrossRef]
- Nucci, M.; Mapelli, D.; Mondini, S. Cognitive Reserve Index questionnaire (CRIq): A new instrument for measuring cognitive reserve. Aging Clin. Exp. Res. 2012, 24, 218–226. [Google Scholar] [CrossRef]
- Buonomano, D.V.; Merzenich, M.M. Cortical plasticity: From synapses to maps. Annu. Rev. Neurosci. 1998, 21, 149–186. [Google Scholar] [CrossRef]
- Lyxell, B.; Andersson, U.; Borg, E.; Ohlsson, I.S. Working-memory capacity and phonological processing in deafened adults and individuals with a severe hearing impairment. Int. J. Audiol. 2003, 42 (Suppl. 1), S86–S89. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| (a) Main Hypotheses for the Relationship between HL and Cognitive Decline | |
|---|---|
| Cognitive Load Hypothesis [4] | The cognitive load hypothesis suggests that HL leads to greater sensory-perceptual effort because of the incoming degraded auditory signal. The greater cognitive resources required for auditory perceptual processing have negative effects on cognitive, attentional, and mnemonic resources. In other words, cognitive decline in hearing-impaired adults might be a consequence of an overinvestment of brain activity in auditory and spoken language processing, resulting in a significant detriment to other cognitive processes. |
| Information Degradation Hypothesis [10] | The “information degradation hypothesis” suggests that degradation of stimuli (noisy environment, decrease in auditory sensitivity) requires an additional effort: as a consequence, cognitive resources used for signal codification are not available for cognitive functions. |
| Sensory Deprivation Hypothesis/Cascade Hypothesis [6,11] | According to the “sensory-deprivation hypothesis”, HL demands increased cognitive effort which results in depleting cognitive performance over time. Subsequently, cognitive performance deterioration leads to social isolation that in turn causes gradual cognitive decline. Cognitive decline is believed to be potentially remediable with rehabilitation. |
| Common Cause Hypothesis [12] | Presbycusis and cognitive impairment might be signs of a common neurodegenerative process. So, sensory functioning could be a strong late-life predictor of individual differences in intellectual functioning and could be seen as an indicator of the physiological integrity of the aging brain. |
| (b) Possible non-causal mechanisms linking HL to cognitive decline | |
| Testing bias [7,8,9,10] | Poor verbal communication associated with HL may confound cognitive testing. HL may influence neuropsychological testing more than cognition per se. HL may introduce a systematic bias into neuropsychological assessments that are mostly designed and validated for verbal instructions and/or the presentation of stimuli. Greater sensitivity of tests in one domain (hearing or cognition) could identify deficits in that domain prior to the other one, leading to the appearance of an illusory causal relationship. |
| Conceptual bias [7,8,9,10] | Upstream common causes with no conditions causally related to others. HL brings older adults to medical attention more often. |
| Personal Variables | Mean (sd) | |
|---|---|---|
| Age at test (years) | 73.4 (6.6) | |
| Duration of HL (years) | 36.7 (16.4) | |
| CI experience (years) | 8.6 (5.54) | |
| n (%) | ||
| CI listening mode | Unilateral | 15 (50.0) |
| Bilateral | 5 (16.7) | |
| Bimodal (CI/HA) | 10 (33.3) | |
| Gender | Male | 16 (53.3) |
| Female | 14 (46.7) | |
| Status | Married | 23 (76.7) |
| Unmarried | 2 (6.7) | |
| Widow | 5 (16.7) | |
| Living alone | 4 (20.0) | |
| Living with significant others | 16 (80.0) | |
| Educational level | Basic | 20 (66.7) |
| Intermediate | 8 (26.7) | |
| Advanced | 2(6.7) | |
| A. Cognitive Variables | LMAP Rank Sum | HAP Rank Sum | U | Z | p-Value | Effect Size |
|---|---|---|---|---|---|---|
| CWTM | 146.000 | 319.000 | 55.000 | 2.322 | 0.019 | 0.425 |
| FDS | 119.000 | 346.000 | 28.000 | 3.452 | 0.000 | 0.642 |
| BDS | 137.000 | 328.000 | 46.000 | 2.699 | 0.005 | 0.511 |
| B. Audiological Variables | LMAP Rank Sum | HAP Rank Sum | U | Z | p-Value | Effect Size |
| W quiet | 113.50 | 211.50 | 47.50 | 1.632 | 0.106 * | 0.320 |
| W+10 | 92.00 | 233.00 | 26.00 | 2.391 | 0.005 * | 0.470 |
| W+5 | 102.50 | 222.50 | 36.50 | 2.798 | 0.026 * | 0.550 |
| S quiet | 127.00 | 198.00 | 61.00 | 0.919 | 0.381 * | 0.180 |
| S +10 | 112.50 | 212.50 | 46.50 | 1.685 | 0.094 * | 0.330 |
| S +5 | 126.00 | 225.00 | 48.00 | 2.017 | 0.064 * | 0.400 |
| VARIABLES |
SF 250 Hz |
SF 500 Hz |
SF 1000 Hz |
SF 2000 Hz |
SF 4000 Hz | Wq | W+10 | W+5 | Sq | S+10 | S+5 |
Age at Test (yrs) | Education (yrs) |
HL duration (yrs) | Attention | CWTM | FDS | BDS |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age at test (yrs) | 0.43 * | 0.32 | 0.23 | 0.29 | 0.15 | −−0.25 | −0.47 * | −0.52 ** | −0.44 * | −0.15 | −0.27 | −− | −0.38 * | −0.27 | −0.34 | −0.30 | −0.07 | 0.002 |
| Education (yrs) | −0.56 ** | −0.40 * | −048 * | −0.42 * | −0.53 ** | 0.25 | 0.38 | 0.43 * | 0.37 | 0.1 | 0.25 | −0.37 | −− | −0.09 | 0.60 ** | 0.30 | 0.27 | 0.53 ** |
| HL duration (yrs) | 0.00 | −0.34 | −0.15 | −0.19 | −0.16 | 0.08 | 0.32 | 0.15 | 0.30 | 0.45 | 0.23 | −0.27 | −0.10 | −− | −0.12 | −0.00 | −0.27 | −0.05 |
| Attention | −0.58 ** | −0.40 * | −0.37 | −0.45 * | −0.47 * | 0.356 | 0.66 ** | 0.58 ** | 0.32 | 0.34 | 0.40 * | −0.34 | 0.60 ** | −0.19 | −− | 0.67 ** | 0.74 ** | 0.53 ** |
| CWTM | −0.50 * | −0.41 * | −0.33 | −0.38 | −0.28 | 0.31 | 0.50 * | 0.52 * | 0.07 | 0.28 | 0.33 | −0.31 | 0.31 | −0.00 | 0.66 ** | −− | 0.56 ** | 0.32 |
| FDS | −0.40 | −0.29 | −0.32 | −0.32 | −0.27 | 0.06 | 0.40 | 0.38 | −0.12 | 0.25 | 0.27 | −0.07 | 0.27 | −0.27 | 0.74 | 0.56 ** | −− | 0.46 * |
| BDS | −0.31 | −0.36 | −0.41 * | −0.39 | −0.54 ** | 0.07 | 0.27 | 0.25 | −0.06 | 0.27 | 0.22 | 0.00 | 0.53 | −0.05 | 0.53 ** | 0.32 | 0.46 * | −− |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giallini, I.; Inguscio, B.M.S.; Nicastri, M.; Portanova, G.; Ciofalo, A.; Pace, A.; Greco, A.; D’Alessandro, H.D.; Mancini, P. Neuropsychological Functions and Audiological Findings in Elderly Cochlear Implant Users: The Role of Attention in Postoperative Performance. Audiol. Res. 2023, 13, 236-253. https://doi.org/10.3390/audiolres13020022
Giallini I, Inguscio BMS, Nicastri M, Portanova G, Ciofalo A, Pace A, Greco A, D’Alessandro HD, Mancini P. Neuropsychological Functions and Audiological Findings in Elderly Cochlear Implant Users: The Role of Attention in Postoperative Performance. Audiology Research. 2023; 13(2):236-253. https://doi.org/10.3390/audiolres13020022
Chicago/Turabian StyleGiallini, Ilaria, Bianca Maria Serena Inguscio, Maria Nicastri, Ginevra Portanova, Andrea Ciofalo, Annalisa Pace, Antonio Greco, Hilal Dincer D’Alessandro, and Patrizia Mancini. 2023. "Neuropsychological Functions and Audiological Findings in Elderly Cochlear Implant Users: The Role of Attention in Postoperative Performance" Audiology Research 13, no. 2: 236-253. https://doi.org/10.3390/audiolres13020022
APA StyleGiallini, I., Inguscio, B. M. S., Nicastri, M., Portanova, G., Ciofalo, A., Pace, A., Greco, A., D’Alessandro, H. D., & Mancini, P. (2023). Neuropsychological Functions and Audiological Findings in Elderly Cochlear Implant Users: The Role of Attention in Postoperative Performance. Audiology Research, 13(2), 236-253. https://doi.org/10.3390/audiolres13020022