
Value Propositions of Public Adult Hearing Rehabilitation in Denmark

 , , , , , , and
, , , , , , and
Abstract
1. Introduction
2. Materials and Methods—Harvesting Value Propositions
2.1. Participants
2.2. Data Collection
2.3. Inductive Thematic Analysis
2.4. Deductive Thematic Analysis
- 1.
- Read the headlines and the detailed descriptions of the value propositions to consider if any themes were missing from the headlines;
- 2.
- Consider merging value propositions;
- 3.
- Consider the wording of each value proposition;
- 4.
- Consider the degree of detail needed.
3. Results—Harvesting Value Propositions
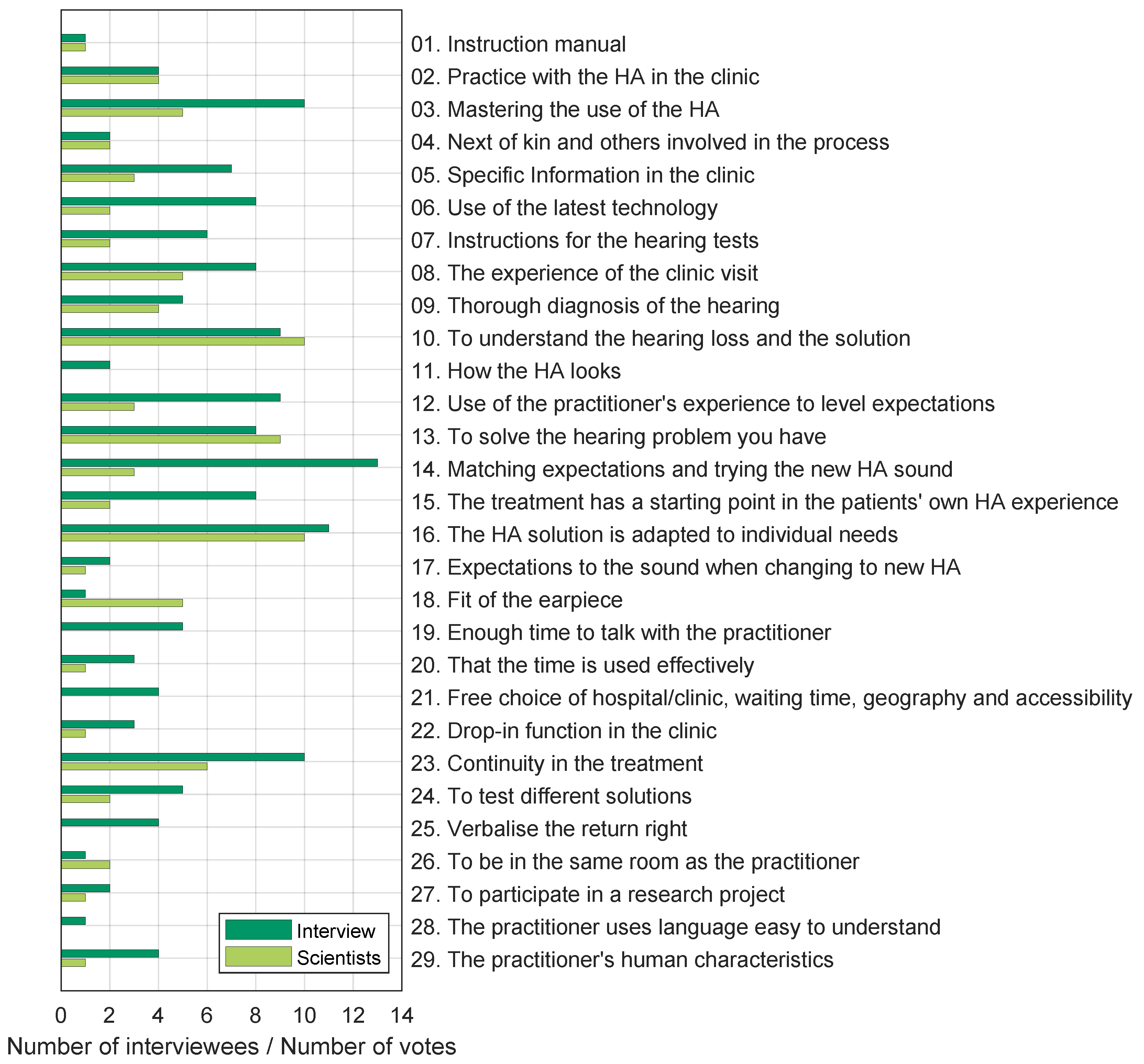
3.1. Value Propositions List
3.2. Selection of Value Propositions for Paired Comparisons
- A
- Will the subject be well-elucidated by being included in the test?
- B
- Is the subject a known and frequent factor in the literature and/or in general?
- C
- Is the subject represented in the scientists’ classification?
- D
- Is the subject represented in interview data?
4. Methods and Materials—Evaluation through Paired Comparisons
4.1. Participants
4.2. Data Collection
4.3. Response Reliability
4.4. Preference Model and Ratio Scale
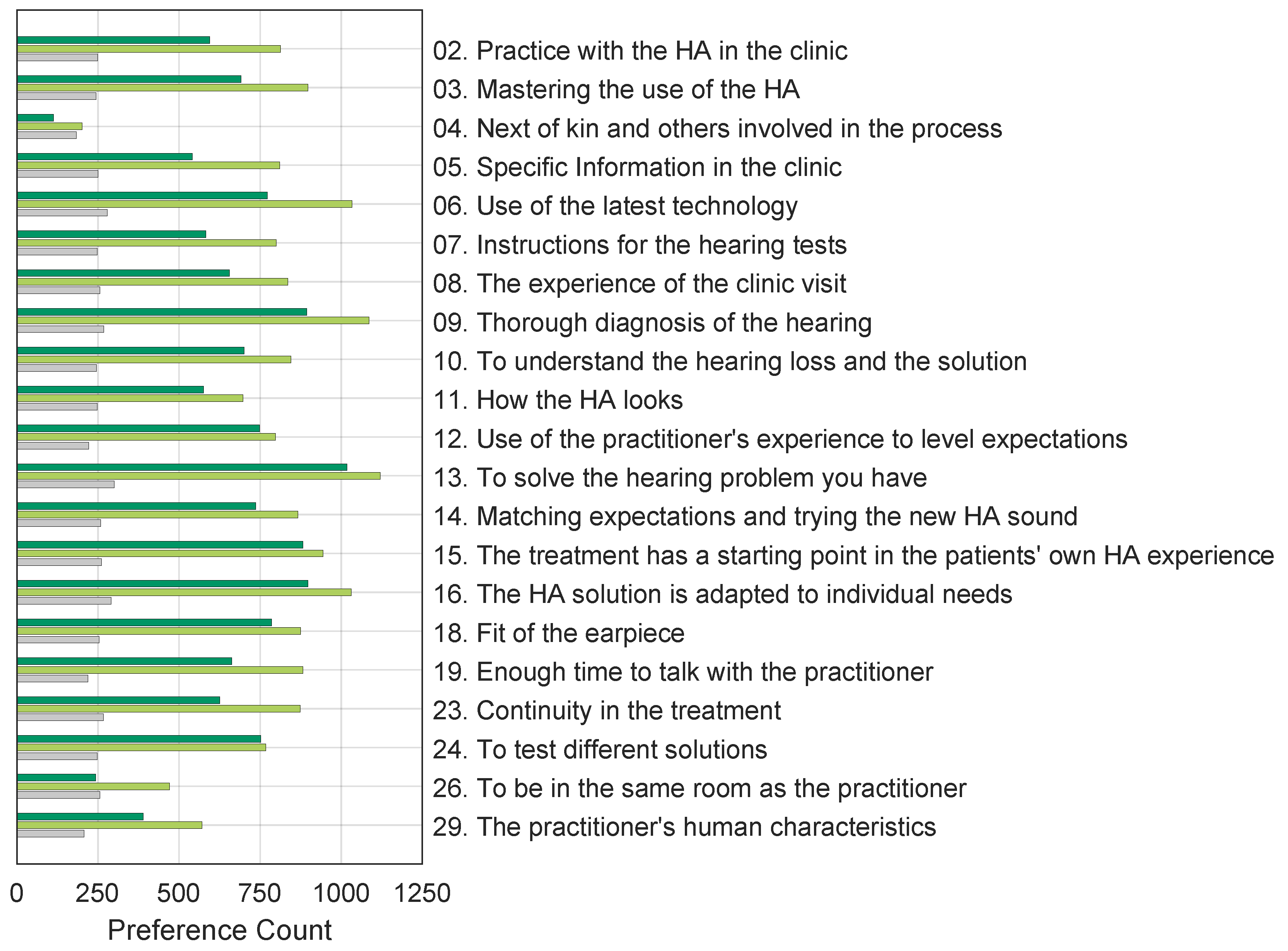
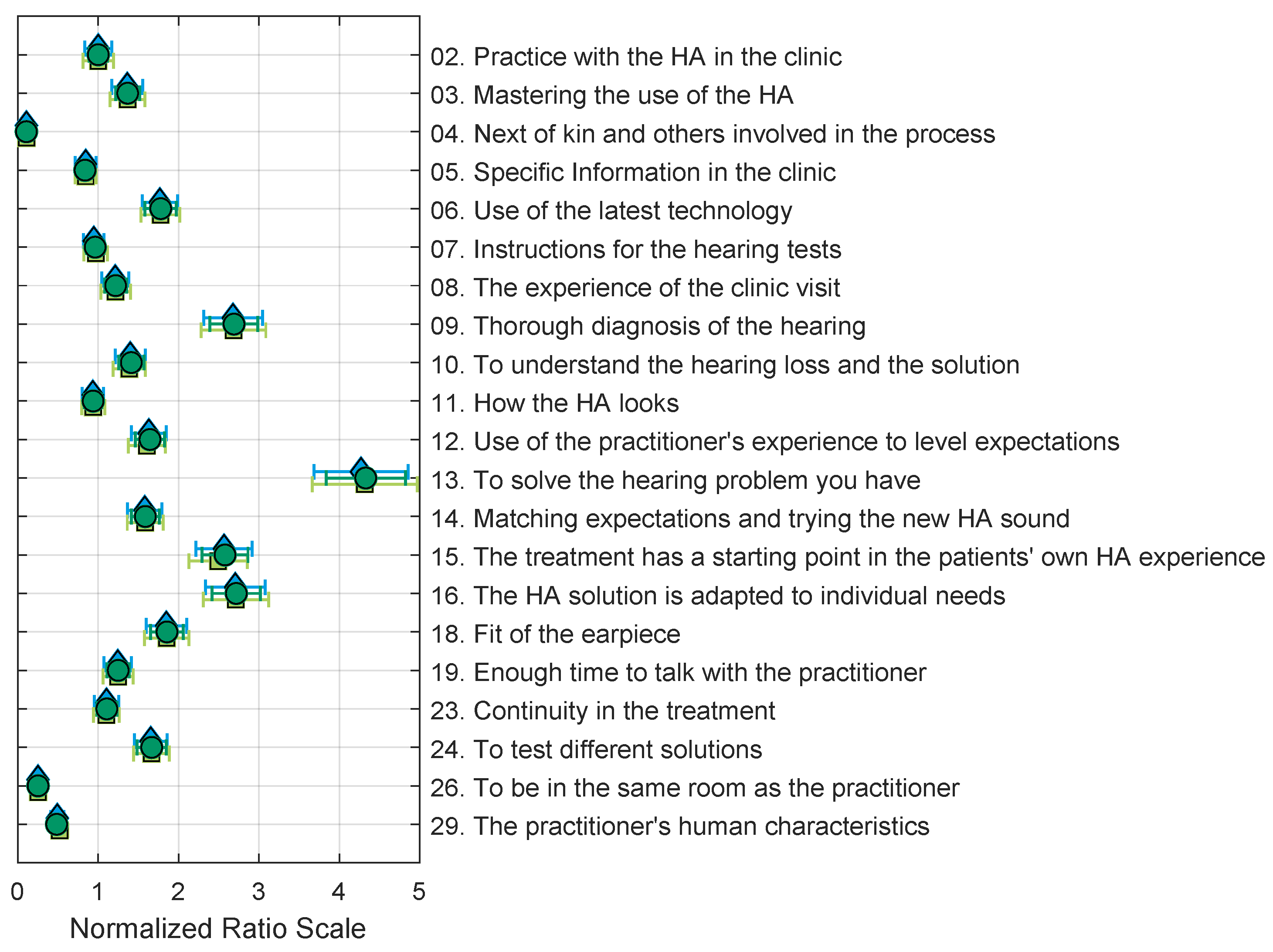
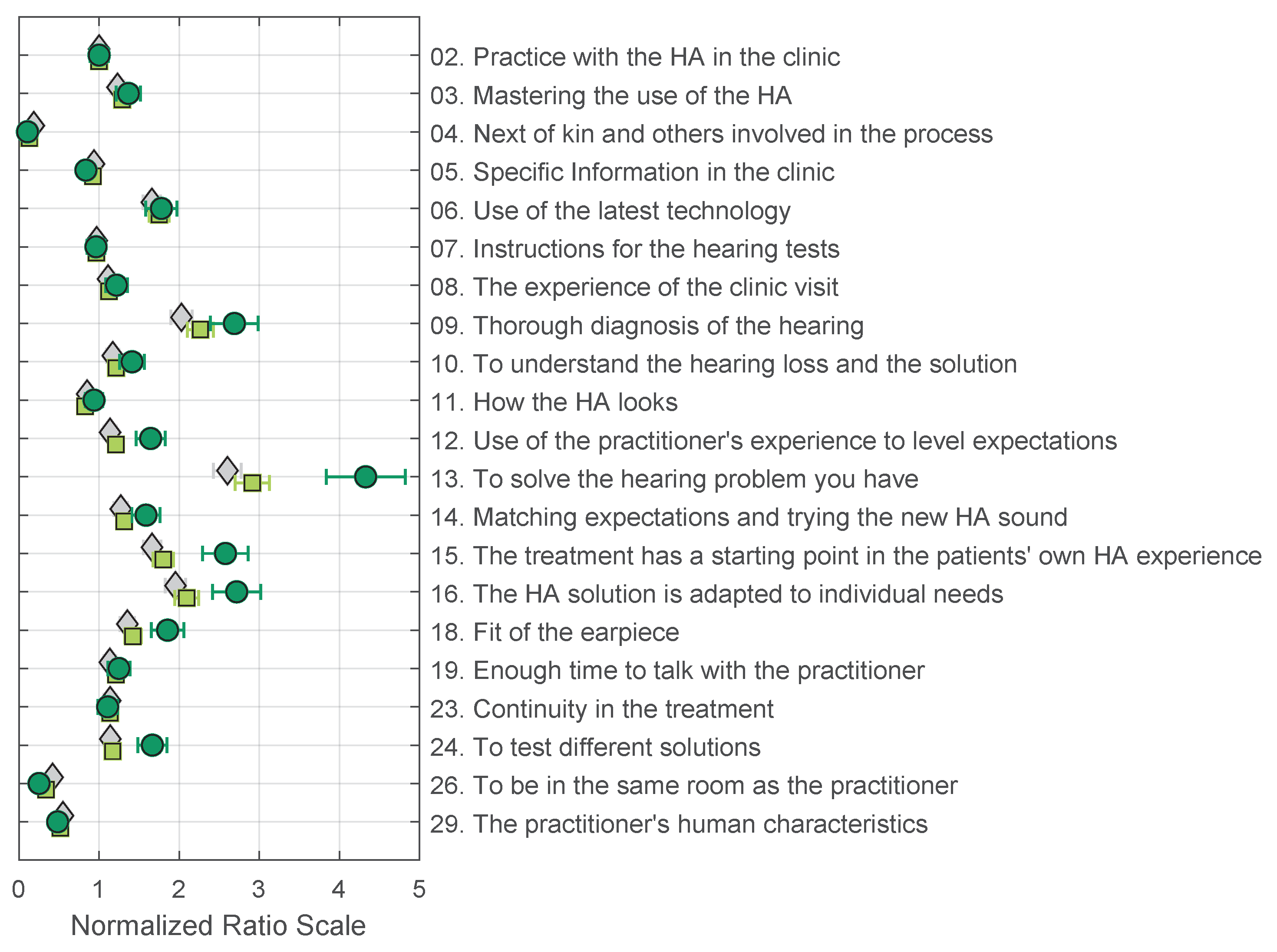
5. Results—Evaluation through Paired Comparisons
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviation
| HA | hearing aid |
References
- Skålén, P.; Gummerus, J.; von Koskull, C.; Magnusson, P.R. Exploring value propositions and service innovation: A service-dominant logic study. J. Acad. Mark. Sci. 2015, 43, 137–158. [Google Scholar] [CrossRef]
- Vargo, S.L.; Lusch, R.F. Service-dominant logic: Continuing the evolution. J. Acad. Mark. Sci. 2008, 36, 1–10. [Google Scholar] [CrossRef]
- Edvardsson, B.; Tronvoll, B.; Gruber, T. Expanding understanding of service exchange and value co-creation: A social construction approach. J. Acad. Mark. Sci. 2011, 39, 327–339. [Google Scholar] [CrossRef]
- Gummerus, J. Value creation processes and value outcomes in marketing theory. Mark. Theory 2013, 13, 19–46. [Google Scholar] [CrossRef]
- Humes, L.E. Dimensions of hearing aid outcome. J. Am. Acad. Audiol. 1999, 10, 26–39. [Google Scholar] [CrossRef] [PubMed]
- Arlinger, S.; Nordqvist, P.; Öberg, M. International outcome inventory for hearing aids: Data from a large Swedish quality register database. Am. J. Audiol. 2017, 26, 443–450. [Google Scholar] [CrossRef] [PubMed]
- Laplante-Lévesque, A.; Jensen, L.D.; Dawes, P.; Nielsen, C. Optimal hearing aid use: Focus groups with hearing aid clients and audiologists. Ear Hear. 2013, 34, 193–202. [Google Scholar] [CrossRef]
- Bennett, R.J.; Swanepoel, D.W.; Ratinaud, P.; Bailey, A.; Pennebaker, J.W.; Manchaiah, V. Hearing aid acquisition and ownership: What can we learn from online consumer reviews? Int. J. Audiol. 2021, 60, 917–926. [Google Scholar] [CrossRef]
- Bennett, R.J.; Meyer, C.J.; Eikelboom, R.H.; Atlas, M.D. Investigating the Knowledge, Skills, and Tasks Required for Hearing Aid Management: Perspectives of Clinicians and Hearing Aid Owners. Am. J. Audiol. 2018, 27, 67–84. [Google Scholar] [CrossRef]
- Sanchez-Lopez, R.R.; Fereczkowski, M.M.; Santurette, S.S.; Dau, T.T.; Neher, T.T. Towards Auditory Profile-Based Hearing-Aid Fitting: Fitting Rationale and Pilot Evaluation. Audiol. Res. 2021, 11, 10–21. [Google Scholar] [CrossRef] [PubMed]
- Hansen, F.T. Den Sokratiske Dialoggruppe: Et væRktøj til væRdiafklaring, 1st ed.; Gyldendal Uddannelse: Copenhagen, Denmark, 2000. [Google Scholar]
- Osterwalder, A.; Pigneur, Y.; Bernarda, G.; Smith, A. Value Proposition Design: How to Create Products and Services Customers Want; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2014. [Google Scholar]
- Houmøller, S.S.; Wolff, A.; Möller, S.; Narne, V.K.; Narayanan, S.K.; Godballe, C.; Hougaard, D.D.; Loquet, G.; Gaihede, M.; Hammershøi, D. Prediction of successful hearing aid treatment in first-time and experienced hearing aid users: Using the International Outcome Inventory for Hearing Aids. Int. J. Audiol. 2022, 61, 119–129. [Google Scholar] [CrossRef] [PubMed]
- Kendall, M.G.; Smith, B.B. On the Method of Paired Comparisons. Biometrika 1940, 31, 324–345. [Google Scholar] [CrossRef]
- Zimmer, K.; Ellermeier, W. Deriving ratio-scale measures of sound quality from preference judgements. J. Noise Control. Eng. 2005, 51, 210–215. [Google Scholar] [CrossRef]
- Bradley, R.A.; Terry, M.E. Rank Analysis of Incomplete Block Designs: I. The Method of Paired Comparisons. Biometrika 1952, 39, 324–345. [Google Scholar] [CrossRef]
- Luce, R.D. Individual Choice Behavior: A Theoretical Analysis; John Wiley & Sons, Inc.: New York, NY, USA, 1959. [Google Scholar]
- Tversky, A. Elimination by aspects: A theory of choice. Psychol. Rev. 1972, 79, 281–299. [Google Scholar] [CrossRef]
- Tversky, A.; Sattath, S. Preference trees. Psychol. Rev. 1979, 86, 542–573. [Google Scholar] [CrossRef]
- Wickelmaier, F.; Schmid, C. A Matlab function to estimate choice model parameters form paired-comparison data. Behav. Res. Methods, Instruments Comput. 2004, 36, 29–40. [Google Scholar] [CrossRef] [PubMed]
- Lund, K.; Rosenstand, C.A.F. Hvordan reducerer vi stress hos erhvervsaktive med høretab?- et dialogværktøj til at forstå og guide medarbejdere i et stressforløb (How do we reduce stress in a working population with hearing loss?—A dialog tool to understand and guide workers in a stress management course.). In Sammenhænge i Sundhedskommunikation (Context of Heath Communication); Frimann, S., Sørensen, M.B., Wentzer, H.S., Eds.; Aalborg Universitetsforlag: Aalborg, Denmark, 2015; Chapter 10. [Google Scholar]
- Amlani, A.M.; Schafer, E.C. Application of paired-comparison methods to hearing Aids. Trends Amplif. 2009, 13, 241–259. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number | English Translation | Original Danish |
|---|---|---|
| 01 | Instruction manual. It has value in that the hearing aid comes with a good instruction manual (printed and/or digital), which illustrates how one does various things and what one goes through in the clinic. It has to have pictures, be easy to use, manageable, and intuitive. | Brugsanvisning. Det har værdi, at der følger en god brugsanvisning med høreapparaterne (trykt og/eller digital), som illustrerer, hvordan man gør forskellige ting, og som bliver gennemgået i klinikken. Der skal være billeder og den skal være nem, overskuelig og intuitiv. |
| 02 | Practice with the hearing aid in the clinic. It has value in that, as a patient, you have the time and possibility to practice putting the hearing aid on and taking it off, and changing the filters, batteries, etc., while there is a competent person who can help. In the clinic, there should be the possibility to change programs and adjust the level if the hearing aid has such functions. | Øvelser med høreapparatet på klinikken. Det har værdi, at man som patient får tid og mulighed for at øve sig i at tage høreapparaterne af og på, skifte filtre og batterier og lignende, mens der er en fagperson, der kan hjælpe. I klinikken skal man også have mulighed for at prøve at skifte programmer og regulere på lydstyrken, hvis høreapparatet har den funktion. |
| 03 | Mastering the use of the hearing aid. It has value in that, as a patient, you feel able to handle the hearing aid on your own without feeling unsure or handicapped, because it is too small or difficult to manage. Even though the hearing aid is small and advanced, it should be easy to operate and cover the individual’s everyday hearing needs. | Mestring ift. håndtering af høreapparatet. Det har værdi, at man som patient føler, at man kan håndtere høreaparatet på egen hånd uden at føle sig usikker eller handicappet, fordi det er for småt eller for svært at håndtere. Selvom høreapparatet er lille og avanceret, skal det være let at betjene og dække hverdagens individuelle hørebehov. |
| 04 | Next of kin and others involved in the process. It has value in that you receive help to handle the hearing aid when at home. It can, for example, be a caregiver or a next of kin that has been with you to the hearing clinic, and can support you in remembering what was said, as well as help explain the hearing situation to the hearing care professional. | Pårørende og andre med i processen. Det har værdi, at man få hjælp til håndtering af høreapparatet, når man er hjemme. Det kan for eksempel være hjælp fra en hjemmehjælper eller en pårørende, der har været med på høreklinikken, og som kan støtte patienten i at huske, hvad der bliver sagt, samt forklare høresituationen til behandleren. |
| 05 | Specific Information in the clinic. It has value in that, as a patient, you receive sufficient (yet not too much) information at the clinic. The information should be oriented toward the needs of the patient. Important information should be repeated, and it should be cohesive with the written material that is taken home. The process in the clinic should be clearly explained from the start, so one can concentrate on one thing at a time, without having to speculate about what the next step is. | Målrettet information på klinikken. Det har værdi, at man som patient modtager tilstrækkelig, men heller ikke for meget, information på klinikken. Informationen skal være målrettet til patientens behov. Vigtig information skal gentages og hænge godt sammen med den skriftlige information, man får med hjem. Forløbet i klinikken skal være tydeligt forklaret fra start, så man kan koncentrere sig om én ting ad gangen uden at spekulere på, hvad næste skridt bliver. |
| 06 | Use of the latest technology. It has value in that the most advanced test methods are used for hearing tests. The hearing aids should use the latest technology and should be able to connect to the patient’s telephone and other equipment used every day. The batteries in the hearing aid should preferably be rechargeable so there is no need to change the batteries. | Anvendelse af ny teknologi. Det har værdi, at der under høreprøverne anvendes avancerede testmetoder. Høreapparaterne skal anvende den nyeste teknologi og skal kunne kobles op til patientens telefon og andre apparater i hverdagen. Batterierne i høreapparaterne skal helst være genopladelige, så man ikke skal skifte batterier. |
| 07 | Instructions for the hearing tests. It has value in that instructions for the hearing tests are clear and easy to understand and the practitioner explains to the patient (you) what you will experience so that you feel sure about the task. The practitioner should pay attention to you, so, if necessary, test instructions are repeated, and the objective of the test is explained. | Instruktion under høreprøverne. Det har værdi, at der er tydelig og let forståelig instruktion under høreprøverne, og at behandleren forklarer, hvad patienten kommer til at opleve, så man føler sig sikker på opgaven. Behandleren skal være opmærksom på patienten, så instruktioner om nødvendigt gentages og formålet med testen forklares. |
| 08 | The experience of the clinic visit. It has value in that the visit to the clinic is a good experience for the patient (you). You should feel comfortable so that it will be a positive experience to receive the hearing aid. You should not feel that you have failed during the hearing test. You should feel that you can operate the hearing aid when you leave the clinic and that you are satisfied with the sound in the hearing aid. | Oplevelsen af klinikbesøget. Det har værdi, at besøget på høreklinikken er en god oplevelse for patienten. Man skal føle sig godt tilpas, så det opleves positivt at få høreapparater. Man må ikke føle, at man har fejlet i høreprøverne. Man skal føle, at man kan betjene høreapparaterne, når man går fra klinikken, og man skal være tilfreds med lyden i høreapparaterne. |
| Number | English Translation | Original Danish |
|---|---|---|
| 09 | Thorough diagnosis of the hearing. It has value in that the hearing tests are thorough and test different aspects of the hearing, so that the patient feels that there is good correspondence between the hearing tests, hearing needs, and challenges in everyday life, and that the patient feels that all aspects of the hearing loss are tested and clarified, and you can rely on the treatment offered. | En omfattende undersøgelse af hørelsen. Det har værdi, at høreprøverne er grundige og tester forskellige aspekter af hørelsen så patienten føler, at der er god sammenhæng mellem høretests og de hørebehov og -udfordringer, der kan være i hverdagen. At man føler, at alle dele af høretabet bliver belyst, så man kan have tillid til den behandling, der bliver tilbudt. |
| 10 | To understand the hearing loss and the solution. It has value in that the hearing care professional at the clinic provides the patient with a basic understanding about hearing loss, regarding, for example, range of speech, discrimination loss, and normal hearing, and that the patient (through different hearing tests) understands how hearing works, so that the patient understands existing solutions. The treatment should help the patients understand the significance of their hearing loss (for themselves and their next of kin). | Forståelse af høreudfordringer og løsningsmuligheder. Det har værdi, at behandleren på klinikken giver patienten en grundlæggende forståelse af høretabet ift. fx taleområde, skelnetab og normal hørelse. At patienten via forskellige høretests får en forståelse af, hvordan hørelsen fungerer, så man forstår hvilke løsningsmuligheder, der er. Behandlingen skal hjælpe patienten med at forstå høretabets betydning, både for patienten selv og pårørende. |
| 11 | How the hearing aid looks. It has value in that the hearing aid does not look too big (the outer part and the plug in the ear). In terms of looks, it is important that you feel comfortable wearing the hearing aid. | Høreapparatets udseende. Det har værdi, at høreapparatet ikke ser for stort ud, hverken den ydre del eller proppen i øret. Rent udseendemæssig er det vigtig at man føler sig godt tilpas med at have sit høreapparat på. |
| 12 | Use of the practitioner’s experiences to level expectations. It has value in that the practitioners can put themselves in the place of the patients and use their own experiences to assess what works well in view of the patient’s hearing loss. The practitioner must explain what the patient can realistically expect to receive from the hearing aid treatment. It should be clear what types of hearing aids can be chosen from, and what can be expected of them. It should be clear what the best choice is according to the practitioner. | Anvendelse af behandlererfaring ved forventningsafstemning. Det har værdi, at behandleren kan sætte sig i patientens sted og bruge sin egen erfaring til at vurdere, hvad der virker godt ift. høretabet. Behandleren skal forklare, hvad man realistisk kan forvente at få ud af høreapparatbehandlingen. Det skal være tydeligt hvilke høreapparattyper, man kan vælge imellem, og hvad man kan forvente af dem. Det skal stå klart, hvad det bedste valg er set fra behandlerens synspunkt. |
| 13 | To solve the hearing problem you have. It has value in that the practitioner understands the patient’s hearing problem, and attempts to solve the problem by imitating the listening situation that the patient describes and wants to have changed. It is important that the patients feel that there is a solution to their hearing problems, so that they can do some of the things they have not been able to do. Likewise, it has value in that the problems that the next of kin experience (with respect to the patient’s hearing loss) are understood and addressed. | At man får løst det høreproblem, man har. Det har værdi, at behandleren forstår det høreproblem, patienten har, og forsøger at løse problemet ved at efterligne den lydsituation patienten beskriver og gerne vil have ændret på. Det er vigtigt at patienten føler, at der er en løsning på høreproblemet, så man kan nogle af de ting igen, man ikke har kunnet. Ligeledes har det værdi, at de problemer pårørende oplever ift. patientens hørelse bliver forstået og søgt løst. |
| 14 | Matching expectations and trying the new hearing aid sound. It has value in that, as a patient, you can hear and experience how the sound changes with the new hearing aid. The patient will be allowed to test how the hearing aid sounds in the clinic and talk to practitioners through different stages of the process (regarding the new sound). The practitioner will explain that it can take time to become accustomed to the new sound and that not all sounds will be experienced as good as in the beginning. | Forventningsafstemning og afprøvning af den nye høreapparatlyd. Det har værdi, at man som patient kan høre og opleve, hvordan lyden ændrer sig med de nye høreapparater. Patienten skal have lov til at afprøve lyden i klinikken og snakke med behandlere i forskellige dele af processen om den nye lyd. Behandleren skal forklare, at det kan tage tid at vænne sig til den nye lyd, og at ikke alle lyde vil opleves som gode til at starte med. |
| 15 | The treatment has a starting point in the patient’s own hearing aid experience. It has value in that the treatment in the clinic is based on the patient’s own hearing aid experiences. You (the patient) should have the opportunity to talk to the practitioner at some point, after having some experience with the hearing aid. This is both immediately after you have been fitted with the hearing aid in the clinic, and at follow-up (after a few months). | Behandlingen tager afsæt i patientens erfaringer med høreapparaterne. Det har værdi, at behandlingen i klinikken tager afsæt i patientens egne erfaringer med høreapparaterne. Man skal have mulighed for at snakke med behandleren på et tidspunkt, hvor man har gjort sig nogle erfaringer. Det er både lige efter, man har fået apparaterne på i klinikken, og ved opfølgning i klinikken efter nogle måneder. |
| Number | English Translation | Original Danish |
|---|---|---|
| 16 | The hearing aid solution is adapted to individual needs. It has value in that the practitioner has insight into the patient’s everyday life (and, thus, will be able to adapt the hearing aid to any of the patient’s special needs). This can be, for example, related to adjusting the hearing aid to fit the patient’s environment and specific needs. It can also involve connecting the hearing aid to devices such as a telecoil, telephone, or television. | Høreapparatløsningen tilpasses individuelle behov. Det har værdi, at behandleren har indsigt i patientens hverdag for at kunne tilpasse høreapparaterne til særlige behov. Det kan f.eks. dreje sig om en justering af høreapparaterne til patientens omgivelser og situation. Det kan også dreje sig om tilslutning af f.eks. teleslynge, telefon eller fjernsyn. |
| 17 | Expectations to the sound when changing to new hearing aids. It has value in that when changing hearing aids, the sound in the new hearing aid is as close as possible to the sound in the old hearing aid. | Forventninger til nye lyde ved høreapparat-skift. Det har værdi, at lyden i nye høreapparater ved skift er så lig lyden i de gamle apparater som mulig. |
| 18 | Fit of the earpiece. It has value in that the plug fits well in the ear (and it is not annoying). It is possible to obtain a molded plug that fits, and if a plug is annoying, you can have a new one or the existing one can be fixed, so that the discomfort stops. Likewise, treatment is offered if there is eczema or other nuisances from the plug. | Proppens pasform. Det har værdi, at proppen sidder godt i øret og ikke generer. At der er mulighed for at få lavet en støbt prop, der passer, og hvis en prop generer, at man kan få lavet en ny eller få den tilpasset, så generne ophører. Ligeledes, at der er tilbudt behandling, hvis der har været eksem eller andre gener skabt af proppen. |
| 19 | Enough time to talk with the practitioner. It has value in that the practitioners have plenty of time to talk about the treatment and explain possibilities and limitations with regard to hearing loss. The practitioner should have time to listen to and understand the patient’s hearing problems and pursue this to find the right solution. The patient shall have time and opportunity to ask questions. | Tid til samtale. Det har værdi, at personalet har god tid til at snakke om behandlingen og forklare muligheder og begrænsninger ift. høretabet. Behandleren skal have tid til at lytte til og forstå patientens høreproblemer og følge det for at finde den rigtige løsning. Patienten skal have tid og lejlighed til at stille spørgsmål. |
| 20 | The time is used effectively. It has value in that the practitioner is well-prepared and has everything ready, so that the time spent with the practitioner is used effectively, without wasting time; it does not take too long when one has to go to the clinic (parking, driving, waiting to obtain an appointment, and waiting time in the clinic). | At tiden bruges effektivt. Det har værdi, at behandleren har forberedt sig og gjort alt klar, så tiden hos behandleren udnyttes effektivt, og der ikke er spildtid. At det ikke tager for lang tid, når man skal på klinikken (parkering, kørsel, ventetid for at få en tid på klinikken, ventetid i klinikken). |
| 21 | Free choice of hospital/clinic, waiting time, geography, and accessibility. It has value in that you are informed about the waiting time and alternatives, and you can choose the clinic yourself (for example, if it is a university hospital) when you need a new hearing aid; the clinic is close by and accessible, there are good parking options, and transport is free of charge, if necessary. | Frit sygehus-/klinikvalg, ventetid, geografi og tilgængelighed. Det har værdi, at man bliver oplyst om ventetider og alternativer og på den baggrund selv kan vælge høreklinikken, man vil til (fx om det er et universitetshospital), når man skal have nye høreapparater. At klinikken er tæt på og nem at komme til, at der er gode parkeringsmuligheder, og at man kan blive transporteret gratis dertil, hvis man har brug for det. |
| 22 | Drop-in functions in the clinic. It has/will have value in that you can drop in to the clinic without an appointment or with short notice, when you need an adjustment or to fix a small problem with the hearing aid. | Drop-in funktion i klinikken. Det har værdi/vil have værdi, at man kan droppe ind i klinikken uden tidsbestilling eller med kort varsel, når man har brug for at få lavet en justering eller for hjælp til et mindre problem med høreapparaterne. |
| 23 | Continuity of the treatment. It has value in that there is continuity in the process before, during, and after the treatment in the clinic, as well as in the transition to the communication centre. This relation should be made clear to the patients when initiating the process. You (the patient) should have the same practitioner throughout the entire process, and the treatment should subsequently be at the same clinic. If you want, you you should be automatically invited to a follow-up and for hearing-aid renewal. Finally, the treatment shall be flexible and coherent with regard to individual needs, and you should be able to have earwax removed at the clinic. | Sammenhæng i behandlingen. Det har værdi, at der er sammenhæng i forløbet under og efter behandlingen på klinikken og ved overgangen til kommunikationscenter. Sammenhængen skal tydeliggøres for patienten ved opstart af behandlingsforløbet. Man skal have samme behandler igennem hele forløbet, og efterfølgende skal behandlingen foregå på samme klinik. Hvis patienten ønsker det, bliver man automatisk indkaldt til en opfølgning og til fornyelse af høreapparaterne. Endelig skal behandlingen være fleksibel og sammenhængende ift. individuelle behov som fx at man kan få fjernet ørevoks på klinikken. |
| Number | English Translation | Original Danish |
|---|---|---|
| 24 | To test different solutions. It has value in that you have the opportunity to test different types of hearing aids while at the clinic. In this way, you can experience the possibilities with respect to physical fit, the feeling of occlusion, etc., before deciding. | Afprøvning af forskellige løsninger. Det har værdi, at man har mulighed for at afprøve forskellige typer høreapparater, mens man er på klinikken. Dermed kan man opleve mulighederne med hensyn til pasform, følelsen af indelukkethed osv., inden man beslutter sig. |
| 25 | Verbalise the return right. It has value in that the practitioner verbalises your right to come back after having tried the hearing aid for a while, and that you have the right to return it or exchange it at a follow-up, and that the device can be repaired free of charge. | At man italesætter returretten. Det har værdi, at behandleren italesætter retten til at henvende sig efter at have afprøvet høreapparatet i en periode, og at man har mulighed for at returnere det og/eller få det byttet ved en opfølgning, samt at det kan blive repareret gratis. |
| 26 | To be in the same physical room as the practitioner. It has value in that you are in the same physical room as the practitioner, and the practitioner takes into consideration good communication so that you can hear and see each other clearly throughout the entire process. | At være i samme fysiske rum som behandleren. Det har værdi, at man befinder sig i samme fysiske rum som behandleren, og at behandleren tænker over god kommunikation, så man under hele forløbet kan høre og se hinanden tydeligt. |
| 27 | To participate in research projects. It has value in regard to participating in research projects because, as a patient, you are examined more thoroughly and can receive a better hearing-aid solution; it can be interesting to participate in research because it is for a greater purpose. | At deltage i forskningsprojekter. Det har værdi at deltage i forskningsprojekter, fordi man som patient bliver undersøgt grundigere og dermed forventer at få en bedre høreapparatløsning. At det er interessant at deltage i forskning, fordi der er et større formål. |
| 28 | The practitioner uses language that is easy to understand. It has value in that the practitioner informs you in a language that is easy for you to comprehend without using too many technical terms. | At behandleren bruger et letforståeligt sprog. Det har værdi, at behandleren informerer på et sprog, der er til at forstå, hvor der ikke bruges for mange fagtermer. |
| 29 | The practitioner’s human characteristics. It has value in that the practitioner is accommodating so that you experience good treatment and service. The tone should be warm and preferably humorous. The patient should feel that the practitioner is interested in helping. The practitioner should be polite, keep the patient informed about the process, be pedagogical in their approach, and show empathy. | Behandlernes menneskelige egenskaber. Det har værdi, at behandleren er imødekommende, så man oplever en god behandling og service. Omgangstonen skal være varm og gerne humoristisk. Patienten skal opleve, at behandleren er interesseret i at hjælpe. Behandleren skal være høflig, holde patienten orienteret om forløbet, være pædagogisk i sin tilgang samt udvise empati. |
| Model | Parameters | Value Propositions |
|---|---|---|
| BTL | One for each stimulus | – |
| EBA | One for each stimulus | – |
| Self-understanding / Confidence | 02, 03, 04, 07, 08, 10 | |
| Information and communication | 05, 07, 10, 12, 15, 23, 29 | |
| Technology and practice | 02, 03, 06, 14, 24 | |
| PT | One for each stimulus | – |
| Good communication with the practitioner | 10, 12, 14 | |
| Clear and concise information | 05, 07 | |
| Technology and practice | 02, 03, 06, 24 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lund, K.; Ordoñez, R.; Nielsen, J.B.; Christiansen, S.; Houmøller, S.S.; Schmidt, J.H.; Gaihede, M.; Hammershøi, D. Value Propositions of Public Adult Hearing Rehabilitation in Denmark. Audiol. Res. 2023, 13, 254-270. https://doi.org/10.3390/audiolres13020023
Lund K, Ordoñez R, Nielsen JB, Christiansen S, Houmøller SS, Schmidt JH, Gaihede M, Hammershøi D. Value Propositions of Public Adult Hearing Rehabilitation in Denmark. Audiology Research. 2023; 13(2):254-270. https://doi.org/10.3390/audiolres13020023
Chicago/Turabian StyleLund, Katja, Rodrigo Ordoñez, Jens Bo Nielsen, Stine Christiansen, Sabina Storbjerg Houmøller, Jesper Hvass Schmidt, Michael Gaihede, and Dorte Hammershøi. 2023. "Value Propositions of Public Adult Hearing Rehabilitation in Denmark" Audiology Research 13, no. 2: 254-270. https://doi.org/10.3390/audiolres13020023
APA StyleLund, K., Ordoñez, R., Nielsen, J. B., Christiansen, S., Houmøller, S. S., Schmidt, J. H., Gaihede, M., & Hammershøi, D. (2023). Value Propositions of Public Adult Hearing Rehabilitation in Denmark. Audiology Research, 13(2), 254-270. https://doi.org/10.3390/audiolres13020023