

Comparative Study of Audiovestibular Symptoms between Early and Late Variants of COVID-19

Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Questionnaire Design and Instrumentation
2.3. Data Analysis
3. Results
3.1. Demographic and Clinical Characteristics
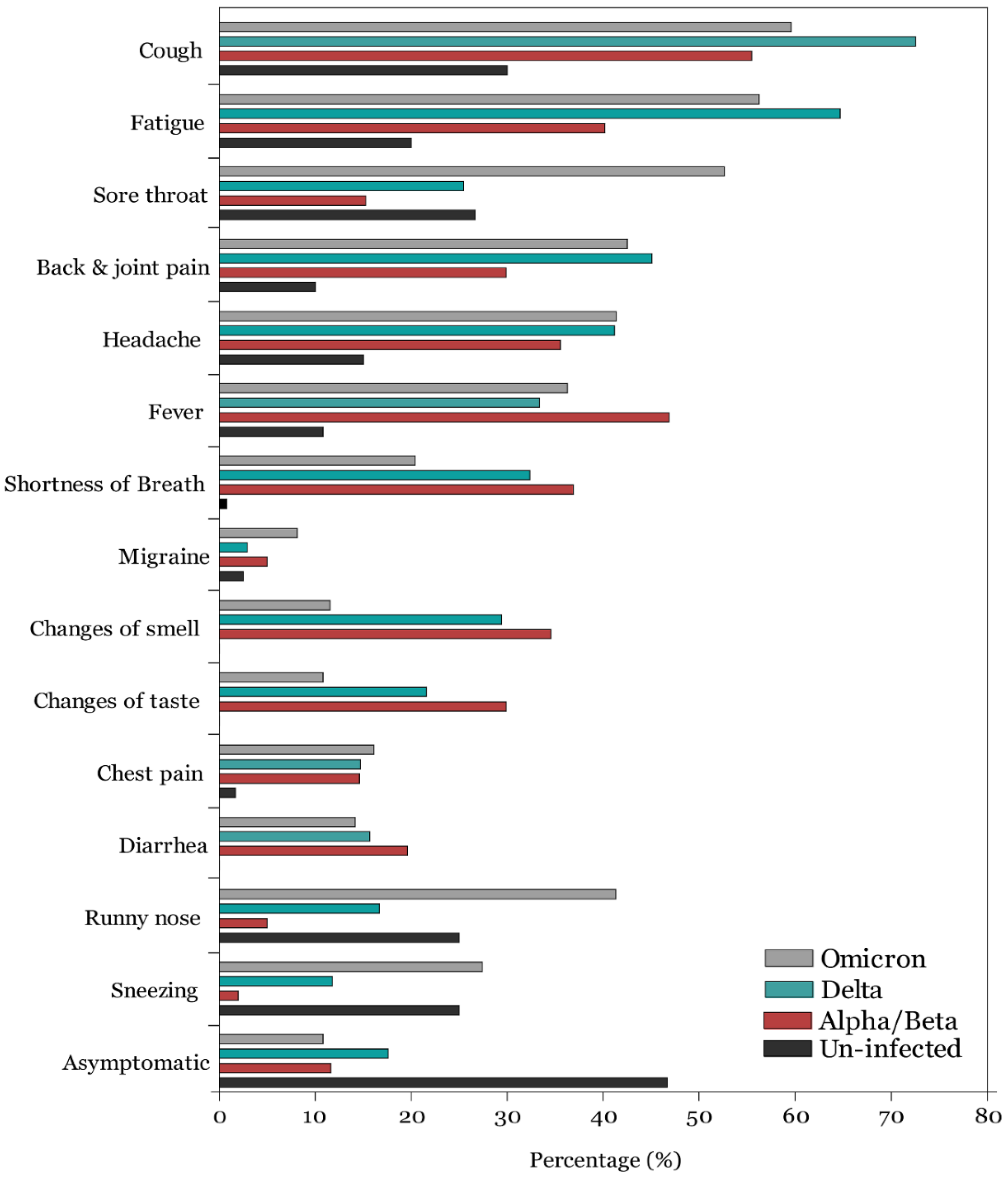
3.2. COVID-19 Symptoms
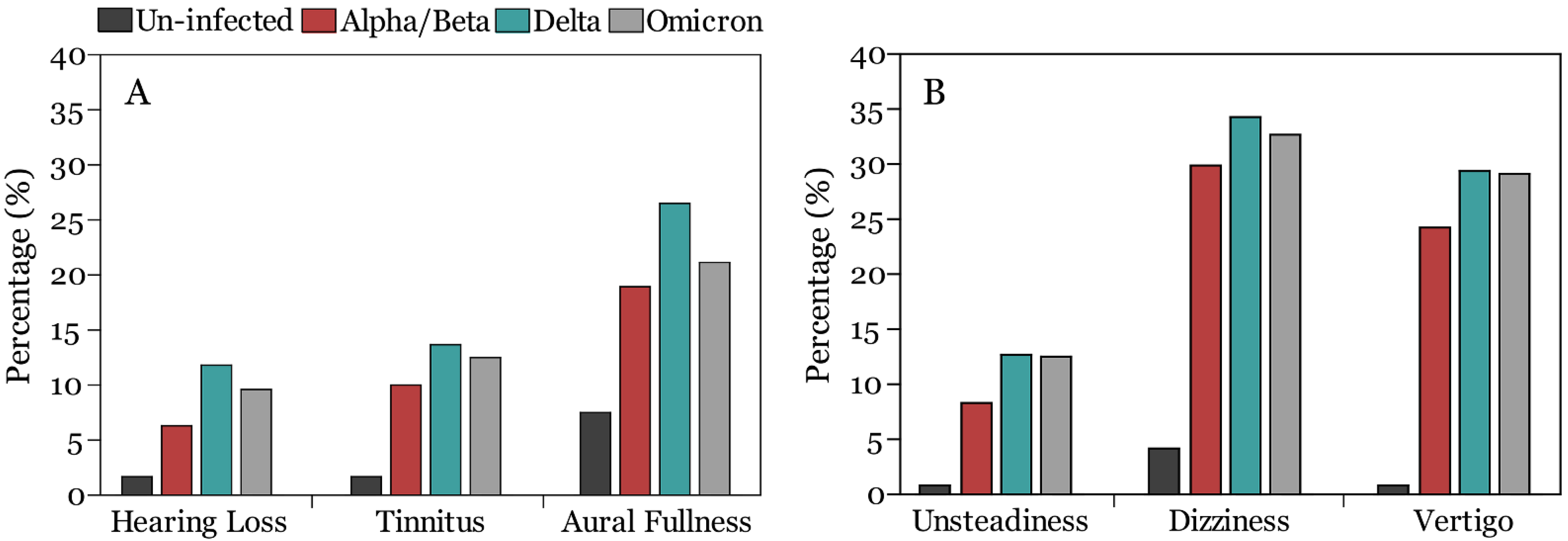
3.3. Auditory Symptoms
3.4. Vestibular Symptoms:
4. Discussion
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Campbell, F.; Archer, B.; Laurenson-Schafer, H.; Jinnai, Y.; Konings, F.; Batra, N.; Pavlin, B.; Vandemaele, K.; Van Kerkhove, M.D.; Jombart, T.; et al. Increased transmissibility and global spread of SARS-CoV-2 variants of concern as at June 2021. Eurosurveillance 2021, 26, 2100509. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Shaman, J.L. COVID-19 pandemic dynamics in South Africa and epidemiological characteristics of three variants of concern (Beta, Delta, and Omicron). medRxiv 2022. [Google Scholar] [CrossRef]
- Graham, M.S.; Sudre, C.H.; May, A.; Antonelli, M.; Murray, B.; Varsavsky, T.; Kläser, K.; Canas, L.S.; Molteni, E.; Modat, M.; et al. Changes in symptomatology, reinfection, and transmissibility associated with the SARS-CoV-2 variant B.1.1.7: An ecological study. Lancet Public Health 2021, 6, e335–e345. [Google Scholar] [CrossRef]
- Twohig, K.A.; Nyberg, T.; Zaidi, A.; Thelwall, S.; Sinnathamby, M.A.; Aliabadi, S.; Seaman, S.R.; Harris, R.J.; Hope, R.; Lopez-Bernal, J.; et al. Hospital admission and emergency care attendance risk for SARS-CoV-2 delta (B.1.617.2) compared with alpha (B.1.1.7) variants of concern: A cohort study. Lancet Infect. Dis. 2022, 22, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Nyberg, T.; Ferguson, N.M.; Nash, S.G.; Webster, H.H.; Flaxman, S.; Andrews, N.; Hinsley, W.; Bernal, J.L.; Kall, M.; Bhatt, S.; et al. Comparative analysis of the risks of hospitalisation and death associated with SARS-CoV-2 omicron (B.1.1.529) and delta (B.1.617.2) variants in England: A cohort study. Lancet 2022, 399, 1303–1312. [Google Scholar] [CrossRef]
- Mehta, O.P.; Bhandari, P.; Raut, A.; Kacimi, S.E.O.; Huy, N.T. Coronavirus Disease (COVID-19): Comprehensive Review of Clinical Presentation. Front. Public Health 2020, 8, 582932. [Google Scholar] [CrossRef]
- Liguori, C.; Pierantozzi, M.; Spanetta, M.; Sarmati, L.; Cesta, N.; Iannetta, M.; Ora, J.; Mina, G.G.; Puxeddu, E.; Balbi, O.; et al. Subjective neurological symptoms frequently occur in patients with SARS-CoV2 infection. Brain Behav. Immun. 2020, 88, 11–16. [Google Scholar] [CrossRef]
- Mao, L.; Jin, H.; Wang, M.; Hu, Y.; Chen, S.; He, Q.; Chang, J.; Hong, C.; Zhou, Y.; Wang, D.; et al. Neurologic Manifestations of Hospitalized Patients with Coronavirus Disease 2019 in Wuhan, China. JAMA Neurol. 2020, 77, 683–690. [Google Scholar] [CrossRef]
- Li, Z.; Liu, T.; Yang, N.; Han, D.; Mi, X.; Li, Y.; Liu, K.; Vuylsteke, A.; Xiang, H.; Guo, X. Neurological manifestations of patients with COVID-19: Potential routes of SARS-CoV-2 neuroinvasion from the periphery to the brain. Front. Med. 2020, 14, 533–541. [Google Scholar] [CrossRef]
- Almishaal, A.A.; Alrushaidan, A.A. Short- and Long-Term Self-Reported Audiovestibular Symptoms of SARS-CoV-2 Infection in Hospitalized and Nonhospitalized Patients. Audiol. Neurotol. 2022, 27, 297–311. [Google Scholar] [CrossRef]
- Menni, C.; Valdes, A.M.; Polidori, L.; Antonelli, M.; Penamakuri, S.; Nogal, A.; Louca, P.; May, A.; Figueiredo, J.C.; Hu, C.; et al. Symptom prevalence, duration, and risk of hospital admission in individuals infected with SARS-CoV-2 during periods of omicron and delta variant dominance: A prospective observational study from the ZOE COVID Study. Lancet 2022, 399, 1618–1624. [Google Scholar] [CrossRef]
- Vihta, K.-D.; Pouwels, K.B.; Peto, T.E.; Pritchard, E.; House, T.; Studley, R.; Rourke, E.; Cook, D.; Diamond, L.; Crook, D. Omicron-associated changes in SARS-CoV-2 symptoms in the United Kingdom. Clin. Infect. Dis. 2022. [Google Scholar] [CrossRef]
- Almufarrij, I.; Munro, K.J. One year on: An updated systematic review of SARS-CoV-2, COVID-19 and audio-vestibular symptoms. Int. J. Audiol. 2021, 60, 935–945. [Google Scholar] [CrossRef]
- AlMufarrij, I.; Uus, K.; Munro, K.J. Does coronavirus affect the audio-vestibular system? A rapid systematic review. Int. J. Audiol. 2020, 59, 487–491. [Google Scholar] [CrossRef]
- Bayat, A.; Saki, N.; Nikakhlagh, S.; Mirmomeni, G.; Raji, H.; Soleimani, H.; Rahim, F. Is COPD associated with alterations in hearing? A systematic review and meta-analysis. Int. J. Chronic Obstr. Pulm. Dis. 2019, 14, 149–162. [Google Scholar] [CrossRef]
- Degen, C.; Lenarz, T.; Willenborg, K. Acute Profound Sensorineural Hearing Loss After COVID-19 Pneumonia. Mayo Clin. Proc. 2020, 95, 1801–1803. [Google Scholar] [CrossRef]
- Koumpa, F.S.; Forde, C.T.; Manjaly, J.G. Sudden irreversible hearing loss post COVID-19. BMJ Case Rep. 2020, 13, e238419. [Google Scholar] [CrossRef]
- Lamounier, P.; Franco, V.; Ramos, H.V.L.; Gobbo, D.A.; Teixeira, R.P.; Dos Reis, P.C.; Fayez, B., Jr.; Cândido, C.C. A 67-Year-Old Woman with Sudden Hearing Loss Associated with SARS-CoV-2 Infection. Am. J. Case Rep. 2020, 21, e927519. [Google Scholar] [CrossRef]
- Lang, B.; Hintze, J.; Conlon, B. Coronavirus disease 2019 and sudden sensorineural hearing loss. J. Laryngol. Otol. 2020, 134, 1026–1028. [Google Scholar] [CrossRef]
- Ricciardiello, F.; Pisani, D.; Viola, P.; Cristiano, E.; Scarpa, A.; Giannone, A.; Longo, G.; Russo, G.; Bocchetti, M.; Coppola, C.; et al. Sudden Sensorineural Hearing Loss in Mild COVID-19: Case Series and Analysis of the Literature. Audiol. Res. 2021, 11, 313–326. [Google Scholar] [CrossRef]
- AlJasser, A.; Alkeridy, W.; Munro, K.J.; Plack, C.J. Is COVID-19 associated with self-reported audio-vestibular symptoms? Int. J. Audiol. 2021, 832–840. [Google Scholar] [CrossRef] [PubMed]
- Micarelli, A.; Granito, I.; Carlino, P.; Micarelli, B.; Alessandrini, M. Self-perceived general and ear-nose-throat symptoms related to the COVID-19 outbreak: A survey study during quarantine in Italy. J. Int. Med. Res. 2020, 48, 300060520961276. [Google Scholar] [CrossRef] [PubMed]
- Munro, K.J.; Uus, K.; AlMufarrij, I.; Chaudhuri, N.; Yioe, V. Persistent self-reported changes in hearing and tinnitus in post-hospitalisation COVID-19 cases. Int. J. Audiol. 2020, 59, 889–890. [Google Scholar] [CrossRef] [PubMed]
- Savtale, S.; Hippargekar, P.; Bhise, S.; Kothule, S. Prevalence of Otorhinolaryngological Symptoms in Covid 19 Patients. Indian J. Otolaryngol. Head Neck Surg. 2021, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Viola, P.; Ralli, M.; Pisani, D.; Malanga, D.; Sculco, D.; Messina, L.; Laria, C.; Aragona, T.; Leopardi, G.; Ursini, F.; et al. Tinnitus and equilibrium disorders in COVID-19 patients: Preliminary results. Eur. Arch. Otorhinolaryngol. 2020, 278, 3725–3730. [Google Scholar] [CrossRef] [PubMed]
- Mustafa, M. Audiological profile of asymptomatic COVID-19 PCR-positive cases. Am. J. Otolaryngol. 2020, 41, 102483. [Google Scholar] [CrossRef]
- de Sousa, F.A.; Costa, R.P.; Xará, S.; Pinto, A.N.; e Sousa, C.A. SARS-CoV-2 and hearing: An audiometric analysis of COVID-19 hospitalized patients. J. Otol. 2021, 16, 158–164. [Google Scholar] [CrossRef]
- Daikhes, N.; Карнеева, O.; Machalov, A.; Kuznetcov, A.; Sapozhnikov, Y.; Balakina, A.; Khulugurova, L.; Карпов, V. Audiological profile of patients with SARS-Co-V-2 PCR-positive cases. Vestnik Otorinolaringol. 2020, 85, 6–11. [Google Scholar] [CrossRef]
- Beukes, E.W.; Baguley, D.M.; Jacquemin, L.; Lourenco, M.P.C.G.; Allen, P.M.; Onozuka, J.; Stockdale, D.; Kaldo, V.; Andersson, G.; Manchaiah, V. Changes in Tinnitus Experiences During the COVID-19 Pandemic. Front. Public Health 2020, 8, 592878. [Google Scholar] [CrossRef]
- Öztürk, B.; Kavruk, H.; Aykul, A. Audiological findings in individuals diagnosed with COVID-19. Am. J. Otolaryngol. 2022, 43, 103428. [Google Scholar] [CrossRef]
- Tan, M.; Cengiz, D.U.; Demir, I.; Demirel, S.; Çolak, S.C.; Karakaş, O.; Bayındır, T. Effects of Covid-19 on the audio-vestibular system. Am. J. Otolaryngol. 2022, 43, 103173. [Google Scholar] [CrossRef]
- Kilic, O.; Kalcioglu, M.T.; Cag, Y.; Tuysuz, O.; Pektas, E.; Caskurlu, H.; Cetın, F. Could sudden sensorineural hearing loss be the sole manifestation of COVID-19? An investigation into SARS-CoV-2 in the etiology of sudden sensorineural hearing loss. Int. J. Infect. Dis. 2020, 97, 208–211. [Google Scholar] [CrossRef]
- Meng, X.; Wang, J.; Sun, J.; Zhu, K. COVID-19 and Sudden Sensorineural Hearing Loss: A Systematic Review. Front. Neurol. 2022, 13, 883749. [Google Scholar] [CrossRef]
- Davis, H.E.; Assaf, G.S.; McCorkell, L.; Wei, H.; Low, R.J.; Re’Em, Y.; Redfield, S.; Austin, J.P.; Akrami, A. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. medRxiv 2020, 38, 101019. [Google Scholar] [CrossRef]
- Lechien, J.R.; Chiesa-Estomba, C.M.; De Siati, D.R.; Horoi, M.; Le Bon, S.D.; Rodriguez, A.; Dequanter, D.; Blecic, S.; El Afia, F.; Distinguin, L.; et al. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): A multicenter European study. Eur. Arch. Otorhinolaryngol. 2020, 277, 2251–2261. [Google Scholar] [CrossRef]
- Zöger, S.; Svedlund, J.; Holgers, K.-M. Relationship Between Tinnitus Severity and Psychiatric Disorders. J. Psychosom. Res. 2006, 47, 282–288. [Google Scholar] [CrossRef]
- Falkenberg, E.-S.; Wie, O.B. Anxiety and Depression in Tinnitus Patients: 5-Year Follow-Up Assessment after Completion of Habituation Therapy. Int. J. Otolaryngol. 2012, 2012, 375460. [Google Scholar] [CrossRef]
- Krog, N.H.; Engdahl, B.; Tambs, K. The association between tinnitus and mental health in a general population sample: Results from the HUNT Study. J. Psychosom. Res. 2010, 69, 289–298. [Google Scholar] [CrossRef]
- Passos, L.; Prazeres, F.; Teixeira, A.; Martins, C. Impact on Mental Health Due to COVID-19 Pandemic: Cross-Sectional Study in Portugal and Brazil. Int. J. Environ. Res. Public Health 2020, 17, 6794. [Google Scholar] [CrossRef]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Glob. Health 2020, 16, 57. [Google Scholar] [CrossRef]
- Xia, L.; He, G.; Feng, Y.; Yu, X.; Zhao, X.; Yin, S.; Chen, Z.; Wang, J.; Fan, J.; Dong, C. COVID-19 associated anxiety enhances tinnitus. PLoS ONE 2021, 16, e0246328. [Google Scholar] [CrossRef] [PubMed]
- Lima, M.; Siokas, V.; Aloizou, A.-M.; Liampas, I.; Mentis, A.-F.A.; Tsouris, Z.; Papadimitriou, A.; Mitsias, P.D.; Tsatsakis, A.; Bogdanos, D.P.; et al. Unraveling the Possible Routes of SARS-COV-2 Invasion into the Central Nervous System. Curr. Treat. Options Neurol. 2020, 22, 37. [Google Scholar] [CrossRef] [PubMed]
- Giacomelli, A.; Pezzati, L.; Conti, F.; Bernacchia, D.; Siano, M.; Oreni, L.; Rusconi, S.; Gervasoni, C.; Ridolfo, A.L.; Rizzardini, G.; et al. Self-reported Olfactory and Taste Disorders in Patients with Severe Acute Respiratory Coronavirus 2 Infection: A Cross-sectional Study. Clin. Infect. Dis. 2020, 71, 889–890. [Google Scholar] [CrossRef] [PubMed]
- Frazier, K.M.; Hooper, J.E.; Mostafa, H.H.; Stewart, C.M. SARS-CoV-2 Virus Isolated from the Mastoid and Middle Ear: Implications for COVID-19 Precautions During Ear Surgery. JAMA Otolaryngol. Head Neck Surg. 2020, 146, 964. [Google Scholar] [CrossRef]
- Uranaka, T.; Kashio, A.; Ueha, R.; Sato, T.; Bing, H.; Ying, G.; Kinoshita, M.; Kondo, K.; Yamasoba, T. Expression of ACE2, TMPRSS2, and Furin in Mouse Ear Tissue, and the Implications for SARS-CoV-2 Infection. Laryngoscope 2020, 131, E2013–E2017. [Google Scholar] [CrossRef]
- Meinhardt, J.; Radke, J.; Dittmayer, C.; Franz, J.; Thomas, C.; Mothes, R.; Laue, M.; Schneider, J.; Brünink, S.; Greuel, S.; et al. Olfactory transmucosal SARS-CoV-2 invasion as a port of central nervous system entry in individuals with COVID-19. Nat. Neurosci. 2021, 24, 168–175. [Google Scholar] [CrossRef]
- Tao, Z.; Xu, J.; Chen, W.; Yang, Z.; Xu, X.; Liu, L.; Chen, R.; Xie, J.; Liu, M.; Wu, J.; et al. Anemia is associated with severe illness in COVID-19: A retrospective cohort study. J. Med. Virol. 2021, 19, 1478–1488. [Google Scholar] [CrossRef]
- Trune, D.R.; Nguyen-Huynh, A. Vascular Pathophysiology in Hearing Disorders. Semin. Heart 2012, 33, 242–250. [Google Scholar] [CrossRef]
- Zanon, A.; Sorrentino, F.; Franz, L.; Brotto, D. Gender-related hearing, balance and speech disorders: A review. Heart Balance Commun. 2019, 17, 203–212. [Google Scholar] [CrossRef]
- Smith, P.F.; Agrawal, Y.; Darlington, C.L. Sexual dimorphism in vestibular function and dysfunction. J. Neurophysiol. 2019, 121, 2379–2391. [Google Scholar] [CrossRef]
- Hülse, R.; Biesdorf, A.; Hörmann, K.; Stuck, B.; Erhart, M.; Hülse, M.; Wenzel, A. Peripheral Vestibular Disorders: An Epidemiologic Survey in 70 Million Individuals. Otol. Neurotol. 2019, 40, 88–95. [Google Scholar] [CrossRef]
- Formeister, E.J.; Rizk, H.G.; Kohn, M.A.; Sharon, J.D. The Epidemiology of Vestibular Migraine: A Population-based Survey Study. Otol. Neurotol. 2018, 39, 1037–1044. [Google Scholar] [CrossRef]
- Cha, Y.-H.; Cui, Y.Y.; Baloh, R.W. Comprehensive Clinical Profile of Mal De Debarquement Syndrome. Front. Neurol. 2018, 9, 261. [Google Scholar] [CrossRef]
- Saud, A.; Naveen, R.; Aggarwal, R.; Gupta, L. COVID-19 and Myositis: What We Know So Far. Curr. Rheumatol. Rep. 2021, 23, 63. [Google Scholar] [CrossRef]
- Helbostad, J.L.; Sturnieks, D.L.; Menant, J.; Delbaere, K.; Lord, S.R.; Pijnappels, M. Consequences of lower extremity and trunk muscle fatigue on balance and functional tasks in older people: A systematic literature review. BMC Geriatr. 2010, 10, 56. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Un-Infected (N = 120) | Alpha/Beta (N = 301) | Delta Variant (N = 102) | Omicron Variant (N = 416) | p-Value | |
|---|---|---|---|---|---|
| N (%) | N (%) | N (%) | N (%) | ||
| Age | |||||
| Median | 34 | 35 | 36 | 36 | 0.380 |
| Interquartile Range | (26, 42) | (27, 44) | (28.5, 44) | (30, 42) | |
| Sex | <0.001 | ||||
| Male | 83 (69.17) | 211 (70.10) | 53 (52) | 143 (34.38) | <0.001 |
| Female | 37 (30.83) | 90 (29.90) | 49 (48) | 273 (65.63) | <0.001 |
| Comorbidities | |||||
| No Comorbidities | 83 (69.17) | 207 (68.77) | 47 (46.08) | 312 (75) | <0.001 |
| Diabetes mellitus | 8 (6.76) | 39 (12.96) | 13 (12.75) | 21 (5.05) | 0.001 |
| Hypertension | 8 (6.67) | 35 (11.63) | 12 (11.76) | 26 (6.25) | 0.041 |
| Heart diseases | 1 (0.83) | 6 (1.99) | 5 (4.90) | 1 (0.24) | 0.003 |
| Chronic respiratory diseases | 4 (3.33) | 14 (4.65) | 9 (8.82) | 30 (7.21) | 0.064 |
| Anemia | 5 (4.17) | 15 (4.98) | 9 (8.82) | 24 (5.77) | 0.442 |
| Head trauma | 0 | 2 (0.66) | 0 | 2 (0.48) | 0.744 |
| Antiviral drugs | <0.001 | ||||
| Hydroxychloroquine | - | 55 (18.27) | 4 (3.19) | 4 (0.96) | <0.001 |
| Favipiravir | - | 40 (13.29) | 4 (3.19) | 1 (0.42) | <0.001 |
| Remdesivir | - | 3 (0.99) | 1 (0.98) | 2 (0.48) | >0.05 |
| Dexamethasone | - | 10 (3.32) | 3 (2.94) | 3 (0.72) | 0.001 |
| Control | Alpha/Beta | Delta | Omicron | COVID-19 Total | Total | |
|---|---|---|---|---|---|---|
| Auditory symptoms | 11 (9.2%) a | 68 (22.6%) b | 29 (28.4%) b | 99 (23.8%) b | 196 (24.02%) | 207 (22%) |
| Hearing Loss | 2 (1.7%) a | 19 (6.3%) a,b | 12 (11.8%) b | 40 (9.6%) b | 71 (8.7%) | 73 (7.8%) |
| Tinnitus | 2 (1.7%) a | 30 (10%) b | 14 (13.7%) b | 52 (12.5%) b | 94 (11.7%) | 98 (10.4%) |
| Aural Fullness | 9 (7.5%) a | 57 (18.9%) b | 27 (26.5%) b | 88 (21.2%) b | 172 (21%) | 181 (19.3%) |
| Vestibular symptoms | 7 (5.8%) a | 105 (34.9%) b | 37 (36.3%) b | 147 (35.3%) b | 289 (35.3%) | 296 (31.5%) |
| Unsteadiness | 1 (0.8%) a | 25 (8.3%) b | 13 (12.7%) b | 52 (12.5%) b | 90 (11%) | 91 (9.7%) |
| Dizziness | 5 (4.2%) a | 90 (29.9%) b | 35 (34.3%) b | 136 (29.1%) b | 261 (31.9%) | 266 (28.3%) |
| Vertigo | 1 (0.8%) a | 73 (24.3%) b | 30 (29.4%) b | 121 (29.1%) b | 216 (27.2%) | 224 (23.9%) |
| Univariate Regression | Multivariate Regression | |||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Group (R-Control) | 0.004 * | 0.415 | ||
| Alpha/Beta | 2.89 (1.47–5.69) | 0.002 * | 1.71 (0.83–3.53) | 0.150 |
| Delta | 3.94 (1.85–8.37) | <0.001 * | 1.98 (0.88–4.46) | 0.097 |
| Omicron | 3.09 (1.60–5.99) | 0.001 * | 1.63 (0.81–3.28) | 0.175 |
| Gender (R-Male) | 1.45 (1.7–1.98) | 0.018 * | 1.09 (0.77–1.56) | 0.616 |
| Age | 1 (0.99–1.02) | 0.970 | - | - |
| Diabetes | 0.86 (0.49–1.52) | 0.303 | - | - |
| Hypertension | 0.93 (0.54–1.63) | 0.810 | - | - |
| Cardiovascular | 1.58 (0.48–5.19) | 0.449 | - | - |
| Respiratory diseases | 1.47 (0.82–2.64) | 0.197 | - | - |
| Anemia | 1.89 (1.5–3.42) | 0.034 * | 1.43 (0.75–2.72) | 0.274 |
| Head injury | 1.18 (0.12–11.4) | 0.887 | - | - |
| Cough | 1.60 (1.16–2.21) | 0.004 * | 0.96 (0.66–1.38) | 0.817 |
| Shortness of breath | 1.44 (1.02–2.02) | 0.039 * | 0.86 (0.58–1.29) | 0.476 |
| Fatigue | 2.55 (1.85–3.52) | <0.001 * | 1.39 (0.95–2.04) | 0.094 |
| Fever | 1.93 (1.41–2.64) | <0.001 * | 1.23 (0.85–1.77) | 0.267 |
| Headache | 2.16 (1.58–2.96) | <0.001 * | 1.36 (0.95–1.95) | 0.099 |
| Migraine | 2.13 (1.20–378) | 0.010 * | 1.51 (0.82–2.79) | 0.194 |
| Loss of smell | 2.33 (1.63–3.32) | <0.001 * | 1.73 (1.01–2.95) | 0.044 * |
| Loss of taste | 1.86 (1.27–2.72) | 0.001 * | 0.86 (0.49–1.52) | 0.611 |
| Chest pain | 2.46 (1.65–3.66) | <0.001 * | 1.58 (1.00–2.49) | 0.048 * |
| Diarrhea | 1.63 (1.08–2.44) | 0.019 * | 0.96 (0.61–1.50) | 0.842 |
| Back and joint pain | 3.11 (2.26–4.27) | <0.001 * | 1.94 (1.34–2.80) | <0.001 * |
| Sore throat | 1.37 (0.99–1.89) | 0.051 * | - | - |
| Runny nose | 1.26 (0.89–1.77) | 0.191 | - | - |
| Sneezing | 1.25 (0.84–1.85) | 0.271 | - | - |
| Antiviral drugs | 0.86 (0.67–1.09) | 0.223 | - | - |
| Univariate Regression | Multivariate Regression | |||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Group (R-Control) | 1.31 (1.16–1.49) | <0.001 * | 1.15 (0.98–1.35) | 0.094 |
| Alpha/Beta | 8.65 (3.89–19.23) | <0.001 * | 5.58 (2.36–13.21) | <0.001 * |
| Delta | 9.22 (3.78–22.54) | <0.001 * | 4.25 (1.69–10.65) | 0.002 * |
| Omicron | 8.82 (4.01–19.43) | <0.001 * | 4.12 (1.81–9.39) | 0.001 * |
| Gender (R-Male) | 1.89 (1.43–2.51) | <0.001 * | 1.48 (1.06–2.06) | 0.020 * |
| Age | 1.01 (0.99–1.02) | 0.163 | - | - |
| Diabetes | 0.91 (0.51–1.49) | 0.701 | - | - |
| Hypertension | 0.79 (0.48–1.32) | 0.378 | - | - |
| Cardiovascular | 1.88 (0.63–5.64) | 0.260 | - | - |
| Respiratory | 1.22 (0.70–2.11) | 0.488 | - | - |
| Anemia | 2.03 (1.16–3.54) | 0.013 * | 1.56 (0.84–2.91) | 0.158 |
| Head injury | 0.78 (0.08–6.98) | 0.779 | - | - |
| Cough | 2.04 (1.53–2.72) | <0.001 * | 1.09 (0.78–1.54) | 0.605 |
| Shortness of breath | 2.45 (1.80–3.33) | <0.001 * | 1.49 (1.05–2.15) | 0.028 * |
| Fatigue | 3.46(2.58–4.63) | <0.001 * | 1.83 (1.38–2.76) | 0.001 * |
| Fever | 2.22 (1.67–2.95) | <0.001 * | 1.92 (0.88–1.73) | 0.215 |
| Headache | 2.82 (2.12–3.75) | <0.001 * | 1.57 (1.15–2.23) | 0.005 * |
| Migraine | 1.89 (1.09–3.27) | 0.024 * | 1.22 (0.63–2.14) | 0.640 |
| Loss of smell | 2.27 (1.63–3.16) | <0.001 * | 1.53 (0.85–2.29) | 0.192 |
| Loss of taste | 1.98 (1.39–2.81) | <0.001 * | 0.88 (0.53–1.51) | 0.675 |
| Chest pain | 2.4. (1.65–3.51) | <0.001 * | 1.15 (0.68–1.62) | 0.828 |
| Diarrhea | 1.75 (1.21–2.55) | 0.003 * | 0.96 (0.59–1.36) | 0.606 |
| Back and joint pain | 2.81 (2.11–3.74) | <0.001 * | 1.31 (0.97–1.92) | 0.074 |
| Sore throat | 1.58 (1.188–2.09) | 0.002 * | 1.06 (0.77–1.57) | 0.606 |
| Runny nose | 1.34 (0.99–1.82) | 0.060 | - | - |
| Sneezing | 1.58 (1.12–2.45) | 0.010 * | 1.28 (0.84–1.99) | 0.244 |
| Antiviral drugs | 1.08 (0.88–1.31) | 0.444 | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almishaal, A.A. Comparative Study of Audiovestibular Symptoms between Early and Late Variants of COVID-19. Audiol. Res. 2022, 12, 680-695. https://doi.org/10.3390/audiolres12060065
Almishaal AA. Comparative Study of Audiovestibular Symptoms between Early and Late Variants of COVID-19. Audiology Research. 2022; 12(6):680-695. https://doi.org/10.3390/audiolres12060065
Chicago/Turabian StyleAlmishaal, Ali A. 2022. "Comparative Study of Audiovestibular Symptoms between Early and Late Variants of COVID-19" Audiology Research 12, no. 6: 680-695. https://doi.org/10.3390/audiolres12060065
APA StyleAlmishaal, A. A. (2022). Comparative Study of Audiovestibular Symptoms between Early and Late Variants of COVID-19. Audiology Research, 12(6), 680-695. https://doi.org/10.3390/audiolres12060065