
The Otoprotective Effect of Ear Cryotherapy: Systematic Review and Future Perspectives
 ,
, 
Abstract
1. Introduction
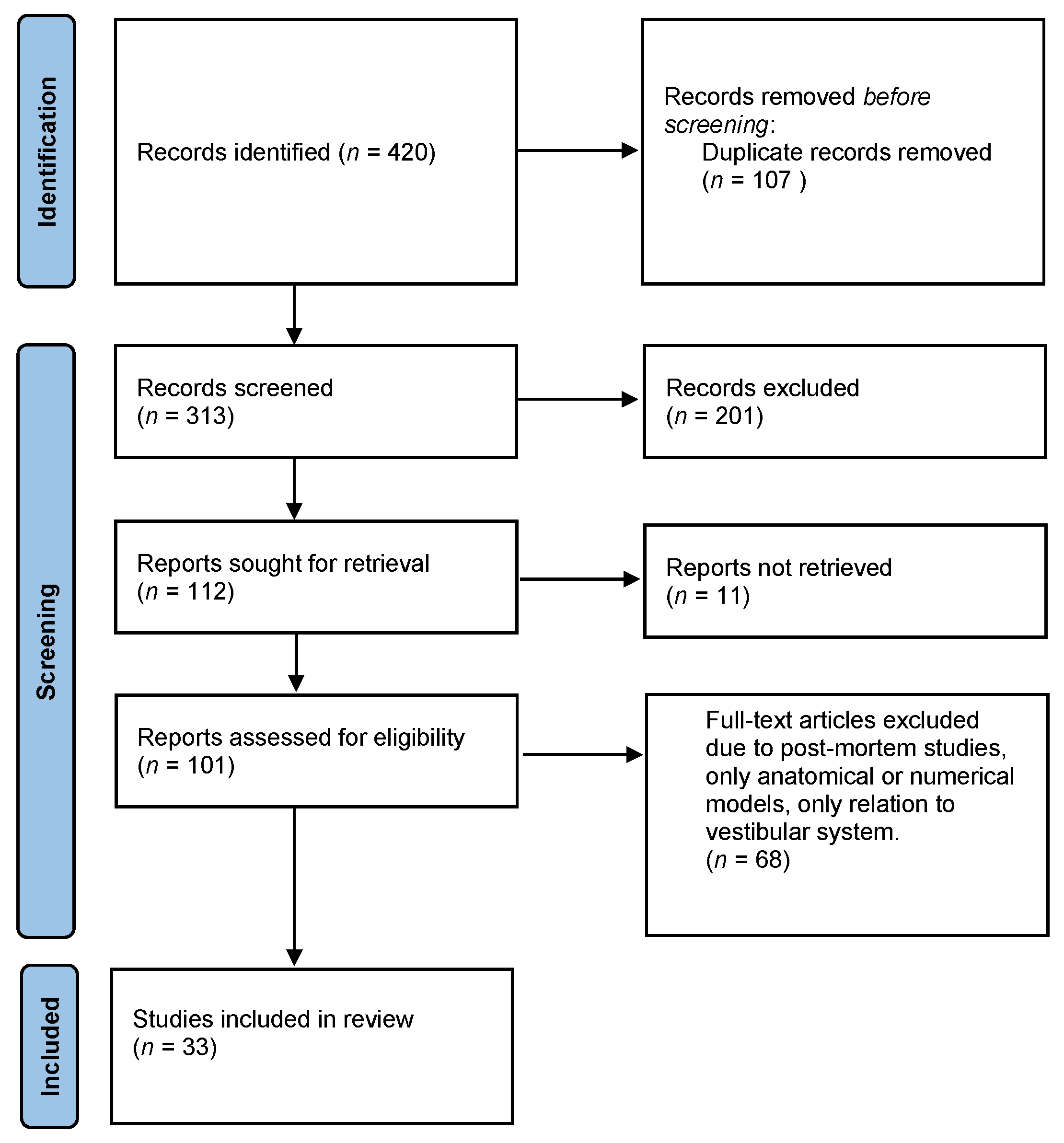
2. Methods
3. Results
3.1. Cooling Effects on Compound Action Potential
3.2. Cooling Effects on Endocochlear Potential and Single nerve Fibers
3.3. Cooling Effects on Otoacoustic Emissions
3.4. Other In Vivo Studies
3.5. Comparison of Cooling Administration
3.6. Cooling-Induced Otoacoustic and Temperature Changes in Human Studies
3.7. Evidence of Cryotherapy for Prevention and Therapy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dixon, P.R.; Feeny, D.; Tomlinson, G.; Cushing, S.; Chen, J.M.; Krahn, M.D. Health-Related Quality of Life Changes Associated With Hearing Loss. JAMA Otolaryngol. Neck Surg. 2020, 146, 630–638. [Google Scholar] [CrossRef]
- Mohr, P.E.; Feldman, J.J.; Dunbar, J.L.; McConkey-Robbins, A.; Niparko, J.K.; Rittenhouse, R.K.; Skinner, M.W. The societal costs of severe to profound hearing loss in the United States. Int. J. Technol. Assess. Health Care 2000, 16, 1120–1135. [Google Scholar] [CrossRef]
- Kellerhals, B. Pathogenesis of inner ear lesions in acute acoustic trauma. Acta. Otolaryngol. 1972, 73, 249–253. [Google Scholar] [CrossRef]
- Szczepek, A.J. Ototoxicity: Old and New Foes. In Advances in Clinical Audiology; Hatzopoulos, S., Ed.; InTech: London, UK, 2017. [Google Scholar]
- Cadoni, G.; Fetoni, A.R.; Agostino, S.; Santis, A.D.; Manna, R.; Ottaviani, F.; Paludetti, G. Autoimmunity in sudden sensorineural hearing loss: Possible role of anti-endothelial cell autoantibodies. Acta Otolaryngol. Suppl. 2002, 122, 30–33. [Google Scholar] [CrossRef]
- Merchant, S.N.; Durand, M.L.; Adams, J.C. Sudden deafness: Is it viral? ORL J. Otorhinolaryngol. Relat. Spec. 2008, 70, 52–60. [Google Scholar] [CrossRef]
- Stokroos, R.J.; Albers, F.W. The etiology of idiopathic sudden sensorineural hearing loss. A review of the literature. Acta Otorhinolaryngol. Belg. 1996, 50, 69–76. [Google Scholar]
- Ballesteros, F.; Tassiesm, D.; Reverter, J.C.; Alobid, I.; Bernal-Sprekelsen, M. Idiopathic sudden sensorineural hearing loss: Classic cardiovascular and new genetic risk factors. Audiol. Neurootol. 2012, 17, 400–408. [Google Scholar] [CrossRef]
- Rybak, L.P.; Mukherjea, D.; Jajoo, S.; Ramkumar, V. Cisplatin ototoxicity and protection: Clinical and experimental studies. Tohoku J. Exp. Med. 2009, 219, 177–186. [Google Scholar] [CrossRef]
- Wei, B.P.C.; Stathopoulos, D.; O’Leary, S. Steroids for idiopathic sudden sensorineural hearing loss. Cochrane Database Syst. Rev. 2013, 7, CD003998. [Google Scholar] [CrossRef]
- Freyer, D.R.; Chen, L.; Krailo, M.D.; Knight, K.; Villaluna, D.; Bliss, B.; Pollock, B.H.; Ramdas, J.; Lange, B.; Van Hoff, D.; et al. Effects of sodium thiosulfate versus observation on development of cisplatin-induced hearing loss in children with cancer (ACCL0431): A multicentre, randomised, controlled, open-label, phase 3 trial. Lancet Oncol. 2017, 18, 63–74. [Google Scholar] [CrossRef]
- Minasian, L.M.; Frazier, A.L.; Sung, L.; O’Mara, A.; Kelaghan, J.; Chang, K.W.; Krailo, M.; Pollock, B.H.; Reaman, G.; Freyer, D.R. Prevention of cisplatin-induced hearing loss in children: Informing the design of future clinical trials. Cancer Med. 2018, 7, 2951–2959. [Google Scholar] [CrossRef]
- Grevelman, E.G.; Breed, W.P.M. Prevention of chemotherapy-induced hair loss by scalp cooling. Ann. Oncol. 2005, 16, 352–358. [Google Scholar] [CrossRef]
- Monzack, E.L.; May, L.A.; Roy, S.; Gale, J.E.; Cunningham, L.L. Live imaging the phagocytic activity of inner ear supporting cells in response to hair cell death. Cell Death Differ. 2015, 22, 1995–2005. [Google Scholar] [CrossRef]
- Royl, G.; Füchtemeier, M.; Leithner, C.; Megow, D.; Offenhauser, N.; Steinbrink, J.; Kohl-Bareis, M.; Dirnagl, U.; Lindauer, U. Hypothermia effects on neurovascular coupling and cerebral metabolic rate of oxygen. Neuroimage 2008, 40, 1523–1532. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Brown, M.C.; Smith, D.I.; Nuttall, A.L. The temperature dependency of neural and hair cell responses evoked by high frequencies. J. Acoust. Soc. Am. 1983, 73, 1662–1670. [Google Scholar] [CrossRef]
- Fernandez, C.; Singh, H.; Perlmann, H. Effect of short-term hypothermia on cochlear responses. Acta Otolaryngol. 1958, 49, 189–205. [Google Scholar] [CrossRef]
- Harrison, J.B. Temperature Effects on Responses in the Auditory System of the Little Brown Bat Myotis l. lucifugus. Physiol. Zool. 1965, 38, 34–48. [Google Scholar] [CrossRef]
- Ohlemiller, K.K.; Siegel, J.H. The effects of moderate cooling on gross cochlear potentials in the gerbil: Basal and apical differences. Hear Res. 1992, 63, 79–89. [Google Scholar] [CrossRef]
- Shore, S.E.; Nuttall, A.L. The effects of cochlear hypothermia on compound action potential tuning. J. Acoust. Soc. Am. 1985, 77, 590–598. [Google Scholar] [CrossRef]
- Konishi, T.; Salt, A.N.; Hamrick, P.E. Effects of hypothermia on ionic movement in the guinea pig cochlea. Hear Res. 1981, 4, 265–278. [Google Scholar] [CrossRef]
- Gummer, A.W.; Klinke, R. Influence of temperature on tuning of primary-like units in the guinea pig cochlear nucleus. Hear Res. 1983, 12, 367–380. [Google Scholar] [CrossRef]
- Ohlemiller, K.K.; Siegel, J.H. Cochlear basal and apical differences reflected in the effects of cooling on responses of single auditory nerve fibers. Hear Res. 1994, 80, 174–190. [Google Scholar] [CrossRef]
- Khvoles, R.; Freeman, S.; Sohmer, H. Effect of temperature on the transient evoked and distortion product otoacoustic emissions in rats. Audiol. Neurootol. 1998, 3, 349–360. [Google Scholar] [CrossRef] [PubMed]
- Meenderink, S.W.; van Dijk, P. Temperature Dependence of Anuran Distortion Product Otoacoustic Emissions. J. Assoc. Res. Otolaryngol. 2006, 7, 246–252. [Google Scholar] [CrossRef]
- Noyes, W.; McCaffrey, T.; Fabry, D.; Robinette, M.; Suman, V. Effect of temperature elevation on rabbit cochlear function as measured by distortion-product otoacoustic emissions. Otolaryngol. Head Neck Surg. 1996, 115, 548–552. [Google Scholar] [CrossRef]
- Miller, J.M.; Goodwin, P.C.; Marks, N.J. Inner ear blood flow measured with a laser Doppler system. Arch. Otolaryngol. 1984, 110, 305–308. [Google Scholar] [CrossRef]
- Miller, J.M.; Marks, N.J.; Goodwin, P.C. Laser Doppler measurements of cochlear blood flow. Hear Res. 1983, 11, 385–394. [Google Scholar] [CrossRef]
- Smith, L.P.; Eshraghi, A.A.; Whitley, D.E.; van de Water, T.R.; Balkany, T.J. Induction of localized cochlear hypothermia. Acta Otolaryngol. 2007, 127, 228–233. [Google Scholar] [CrossRef]
- Stanford, J.K.; Morgan, D.S.; Bosworth, N.A.; Proctor, G.; Chen, T.; Palmer, T.T.; Thapa, P.; Walters, B.J.; Vetter, D.E.; Black, R.D.; et al. Cool OtOprotective Ear Lumen (COOL) Therapy for Cisplatin-induced Hearing Loss. Otol. Neurotol. 2021, 42, 466–474. [Google Scholar] [CrossRef]
- Borin, A.; Cruz, O.L.M. Study of distortion-product otoacoustic emissions during hypothermia in humans. Braz. J. Otorhinolaryngol. 2008, 74, 401–409. [Google Scholar] [CrossRef]
- El Ganzoury, M.M.; Kamel, T.B.; Khalil, L.H.; Seliem, A.M. Cochlear Dysfunction in Children following Cardiac Bypass Surgery. ISRN Pediatr. 2012, 2012, 1–6. [Google Scholar] [CrossRef]
- Seifert, E.; Lamprecht-Dinnesen, A.; Asfour, B.; Rotering, H.; Bone, H.G.; Scheld, H.H. The influence of body temperature on transient evoked otoacoustic emissions. Br. J. Audiol. 1998, 32, 387–398. [Google Scholar] [CrossRef] [PubMed]
- Seifert, E.; Brand, K.; van de Flierdt, K.; Hahn, M.; Riebandt, M.; Lamprecht-Dinnesen, A. The influence of hypothermia on outer hair cells of the cochlea and its efferents. Br. J. Audiol. 2001, 35, 87–98. [Google Scholar] [CrossRef] [PubMed]
- Veuillet, E.; Gartner, M.; Champsaur, G.; Neidecker, J.; Collet, L. Effects of hypothermia on cochlear micromechanical properties in humans. J. Neurol. Sci. 1997, 145, 69–76. [Google Scholar] [CrossRef]
- Kleinfeldt, D.; Dahl, D. Temperaturmessungen am Menschlichen Bogengang Nach Thermischer Reizung. Acta Otolaryngol. 1969, 68, 411–419. [Google Scholar] [CrossRef]
- Schmaltz, G. The physical phenomena occurring in the semicircular canals during rotatory and thermic stimulation. Proc. R. Soc. Med. 1931, 25, 359–381. [Google Scholar]
- Spankovich, C.; Lobarinas, E.; Ding, D.; Salvi, R.; Le Prell, C.G. Assessment of thermal treatment via irrigation of external ear to reduce cisplatin-induced hearing loss. Hear Res. 2016, 332, 55–60. [Google Scholar] [CrossRef]
- Hato, N.; Hyodo, J.; Takeda, S.; Takagi, D.; Okada, M.; Hakuba, N.; Gyo, K. Local hypothermia in the treatment of idiopathic sudden sensorineural hearing loss. Auris Nasus Larynx 2010, 37, 626–630. [Google Scholar] [CrossRef]
- Watanabe, F.; Koga, K.; Hakuba, N.; Gyo, K. Hypothermia prevents hearing loss and progressive hair cell loss after transient cochlear ischemia in gerbils. Neuroscience 2001, 102, 639–645. [Google Scholar] [CrossRef]
- Hyodo, J.; Hakuba, N.; Koga, K.; Watanabe, F.; Shudou, M.; Taniguchi, M.; Gyo, K. Hypothermia reduces glutamate efflux in perilymph following transient cochlear ischemia. Neuroreport 2001, 12, 1983–1987. [Google Scholar] [CrossRef]
- Takeda, S.; Hakuba, N.; Yoshida, T.; Fujita, K.; Hato, N.; Hata, R.; Hyodo, J.; Gyo, K. Postischemic mild hypothermia alleviates hearing loss because of transient ischemia. Neuroreport 2008, 19, 1325–1328. [Google Scholar] [CrossRef] [PubMed]
- Takeda, S.; Hata, R.; Cao, F.; Yoshida, T.; Hakuba, N.; Hato, N.; Gyo, K. Ischemic tolerance in the cochlea. Neurosci. Lett. 2009, 462, 263–266. [Google Scholar] [CrossRef] [PubMed]
- Henry, K.R.; Chole, R.A. Hypothermia protects the cochlea from noise damage. Hear Res. 1984, 16, 225–230. [Google Scholar] [CrossRef]
- Balkany, T.J.; Eshraghi, A.A.; Jiao, H.; Polak, M.; Mou, C.; Dietrich, D.W.; Van De Water, T.R. Mild hypothermia protects auditory function during cochlear implant surgery. Laryngoscope 2005, 115, 1543–1547. [Google Scholar] [CrossRef]
- Tamames, I.; King, C.; Bas, E.; Dietrich, W.D.; Telischi, F.; Rajguru, S.M. A cool approach to reducing electrode-induced trauma: Localized therapeutic hypothermia conserves residual hearing in cochlear implantation. Hear Res. 2016, 339, 32–39. [Google Scholar] [CrossRef]
- Miller, J.M.; Ren, T.Y.; Nuttall, A.L. Studies of inner ear blood flow in animals and human beings. Otolaryngol. Head Neck Surg. 1995, 112, 101–113. [Google Scholar] [CrossRef]
- Spankovich, C.; Walters, B.J. Mild Therapeutic Hypothermia and Putative Mechanisms of Hair Cell Survival in the Cochlea. Antioxid Redox Signal 2021, 36, 1203–1214. [Google Scholar] [CrossRef]
- Koehn, J.; Kollmar, R.; Cimpianu, C.L.; Kallmünzer, B.; Moeller, S.; Schwab, S.; Hilz, M.J. Head and neck cooling decreases tympanic and skin temperature, but significantly increases blood pressure. Stroke 2012, 43, 2142–2148. [Google Scholar] [CrossRef]
- Koehn, J.; Wang, R.; de Rojas Leal, C.; Kallmünzer, B.; Winder, K.; Köhrmann, M.; Kollmar, R.; Schwab, S.; Hilz, M.J. Neck cooling induces blood pressure increase and peripheral vasoconstriction in healthy persons. Neurol. Sci. 2020, 41, 2521–2529. [Google Scholar] [CrossRef]
- Poli, S.; Purrucker, J.; Priglinger, M.; Diedler, J.; Sykora, M.; Popp, E.; Steiner, T.; Veltkamp, R.; Bösel, J.; Rupp, A.; et al. Induction of cooling with a passive head and neck cooling device: Effects on brain temperature after stroke. Stroke 2013, 44, 708–713. [Google Scholar] [CrossRef]
- Furman, J.M.; Wall, C.; Kamerer, D.B. Alternate and simultaneous binaural bithermal caloric testing: A comparison. Ann. Otol. Rhinol. Laryngol. 1988, 97, 359–364. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, R.A.; Brookler, K.H.; Baker, A.H. The accuracy of the simultaneous binaural bithermal test in the diagnosis of acoustic neuroma. Laryngoscope 1979, 89, 1046–1052. [Google Scholar] [CrossRef] [PubMed]
- Sataloff, R.T.; Pavlick, M.L.; McCaffrey, J.D.; Davis, J.M.; Stewart, S.M. Simultaneous binaural bithermal caloric testing: Clinical value. Ear Nose Throat J. 2017, 96, 29–31. [Google Scholar] [PubMed]


{kind=link}
| Results | Whole-Body | Ectopic, Cervical | Invasive, Promontory | Ear Canal |
|---|---|---|---|---|
| Increase of the cochlear ischaemic tolerance | Takeda et al. 2008 (gerbils) | |||
| Watanabe et al. 2001 (gerbils) | ||||
| Hyodo et al. 2001 (gerbils) | ||||
| Decrease of noise damage | Henry et Chole 1984 (mice, gerbils) | |||
| Henry 2003 (mice) | ||||
| Increasing the residual hearing after CI | Balkany et al. 2005 (rats) | Tamames et al. 2016 (rats) | ||
| Increased rate of cured patients after sudden idopathic hearing loss | Hato et al. 2010 (human) | |||
| Decrease of cisplatin ototoxicity | Spankovich et al. 2016 | |||
| Stanford et al. 2020 | ||||
| (guinea pigs) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Péus, D.; Sellathurai, S.; Newcomb, N.; Tschopp, K.; Radeloff, A. The Otoprotective Effect of Ear Cryotherapy: Systematic Review and Future Perspectives. Audiol. Res. 2022, 12, 377-387. https://doi.org/10.3390/audiolres12040038
Péus D, Sellathurai S, Newcomb N, Tschopp K, Radeloff A. The Otoprotective Effect of Ear Cryotherapy: Systematic Review and Future Perspectives. Audiology Research. 2022; 12(4):377-387. https://doi.org/10.3390/audiolres12040038
Chicago/Turabian StylePéus, Dominik, Shaumiya Sellathurai, Nicolas Newcomb, Kurt Tschopp, and Andreas Radeloff. 2022. "The Otoprotective Effect of Ear Cryotherapy: Systematic Review and Future Perspectives" Audiology Research 12, no. 4: 377-387. https://doi.org/10.3390/audiolres12040038
APA StylePéus, D., Sellathurai, S., Newcomb, N., Tschopp, K., & Radeloff, A. (2022). The Otoprotective Effect of Ear Cryotherapy: Systematic Review and Future Perspectives. Audiology Research, 12(4), 377-387. https://doi.org/10.3390/audiolres12040038