
Skull Vibration Induced Nystagmus Test: Correlations with Semicircular Canal and Otolith Asymmetries

 , ,
, ,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Terminology
2.2. Participants
2.3. Vestibular Testing Methods
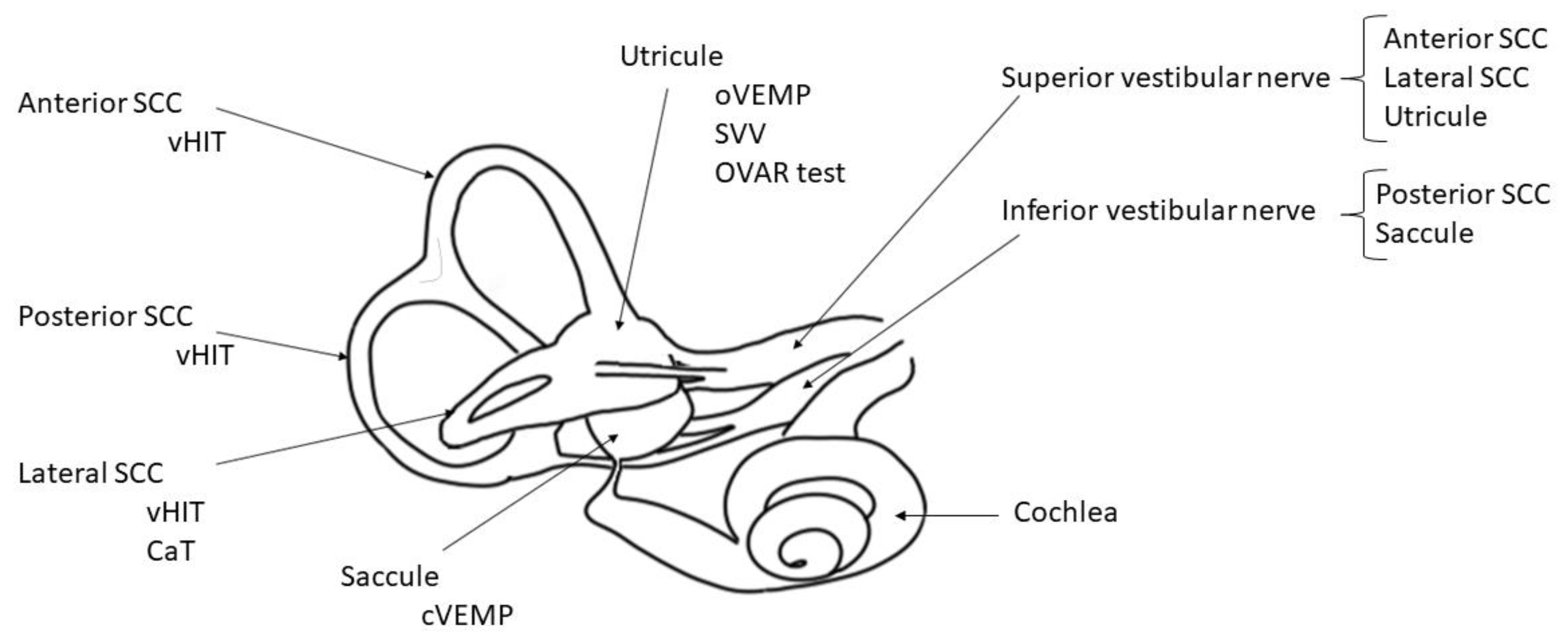
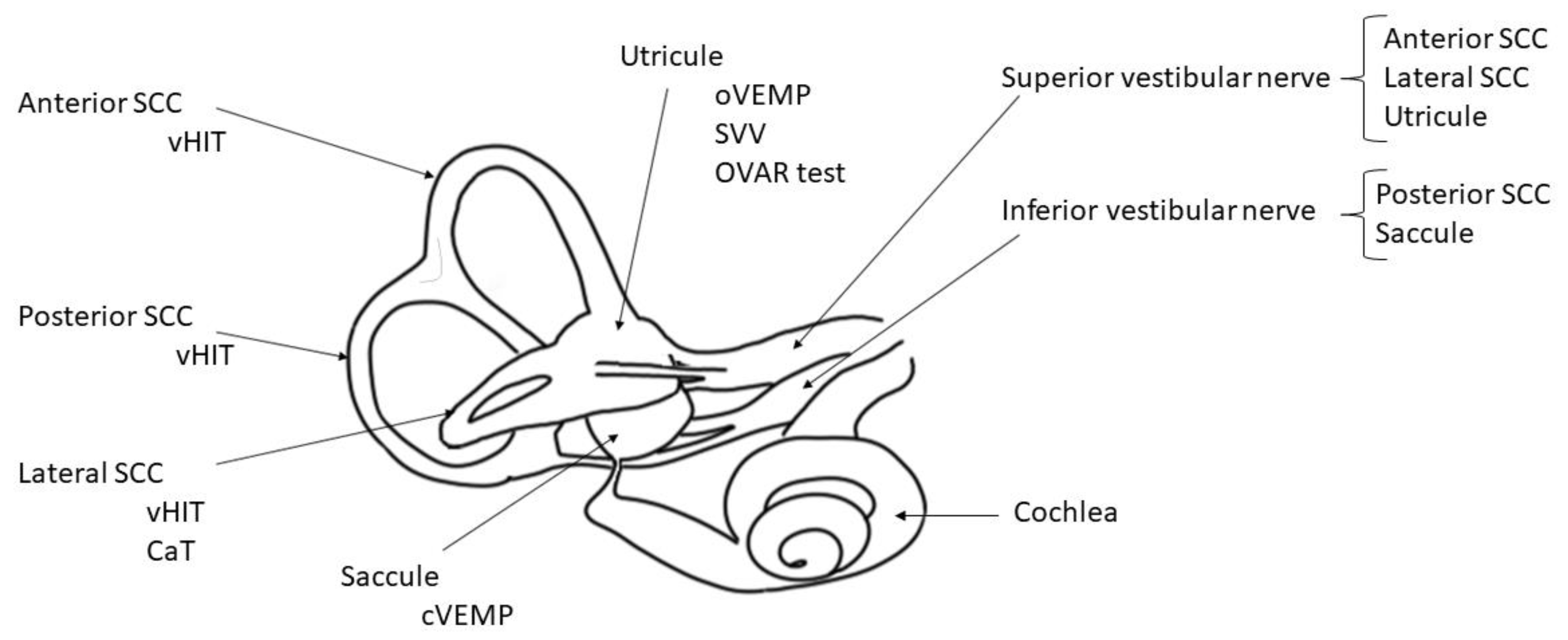
- SVINT: The vibratory stimulation was applied in all participants during 10 s successively to the right and left mastoid processes using the hand-held V.VIB 3F stimulator (Synapsys, Marseille, France) at a stimulus frequency of 100 Hz. A 3D videonystagmographic (VNG) device (Synapsys, Marseille, France) was used to detect the SVIN occurrence and to measure its slow-phase eye velocity for horizontal (H-SPV, °/s), vertical (V-SPV, °/s) and torsional components (T-SPV, °/s). A positive SVINT is defined by consistent responses on both mastoids and with a H-SPV > 2°/s [1]. The 3D VNG device from synapsis has proven its efficiency and accuracy by measuring and an objective torsional vertical component in posterior canal benign paroxysmal positional vertigo (BPPV) and only horizontal component in horizontal SCC BPPV [26].
- VHIT: The participants were installed in front of a camera device VHIT Ulmer II 0 14 (Synapsys, Marseille, France). Semicircular canals (SCC) were tested in pairs according to the planes of stimulation (horizontal plane, right–anterior–left–posterior plane, left–anterior–right–posterior plane). Ten valid head-impulses were needed for each canal. The gains were given for: L-VHIT (lateral SCCs), A-VHIT (anterior SCCs) and P-VHIT (posterior SCCs). A gain < 0.8 for L-VHIT and <0.7 for A-VHIT and P-VHIT and asymmetry between canals >20% were considered abnormal.
- VEMP test: Recordings were performed with Neuro-Audio System (Russia). The VEMPs were performed with the Neuro-Audio device (Neuro Audio Collin Medical France). The stimuli delivered with headphones (TDH 39) were short-tone bursts at a frequency of 500 Hz and intensities ranged from 110 to 70 dB. The stimulus was a 500 Hz air-conducted tone-burst (rise/fall time 1 ms, plateau 2 ms; ear headphones TDH39). For oVEMP, the active electrode was positioned approximately 1 cm below the lower eyelids, the ground electrode on the high forehead (Fz) and reference electrode was placed on the chin. The subjects were instructed to direct their gaze at a visual target with a vertical elevation of about 30 degrees. For cVEMP, the ground electrode was placed on the medium part of the forehead (Fz), the active electrodes at the junction of the superior one third and inferior two-third of both sternocleidomastoid muscles, the reference electrode was located over the upper sternum. The subjects were informed to turn the head in the opposite direction to the stimulated side. A difference in amplitude between both sides higher than 25% was considered to be significant to show an asymmetry (positive test).
- CaT: The bithermal caloric test protocol (30 °C, 44 °C) was performed on each ear with VNG device (Synapsys, Marseille, France) following the Fitzgerald-Hallpike technique. A unilateral vestibular weakness was considered significant when the difference between both ears was greater than 20% [27]. The percentage of hypofunction (CaT) and relative preponderance (% RP) were used for the quantitative study and correlations with SVIN-SPV.
2.4. Procedure
2.5. Statistical Analysis
3. Results
3.1. Identified Groups of Patients
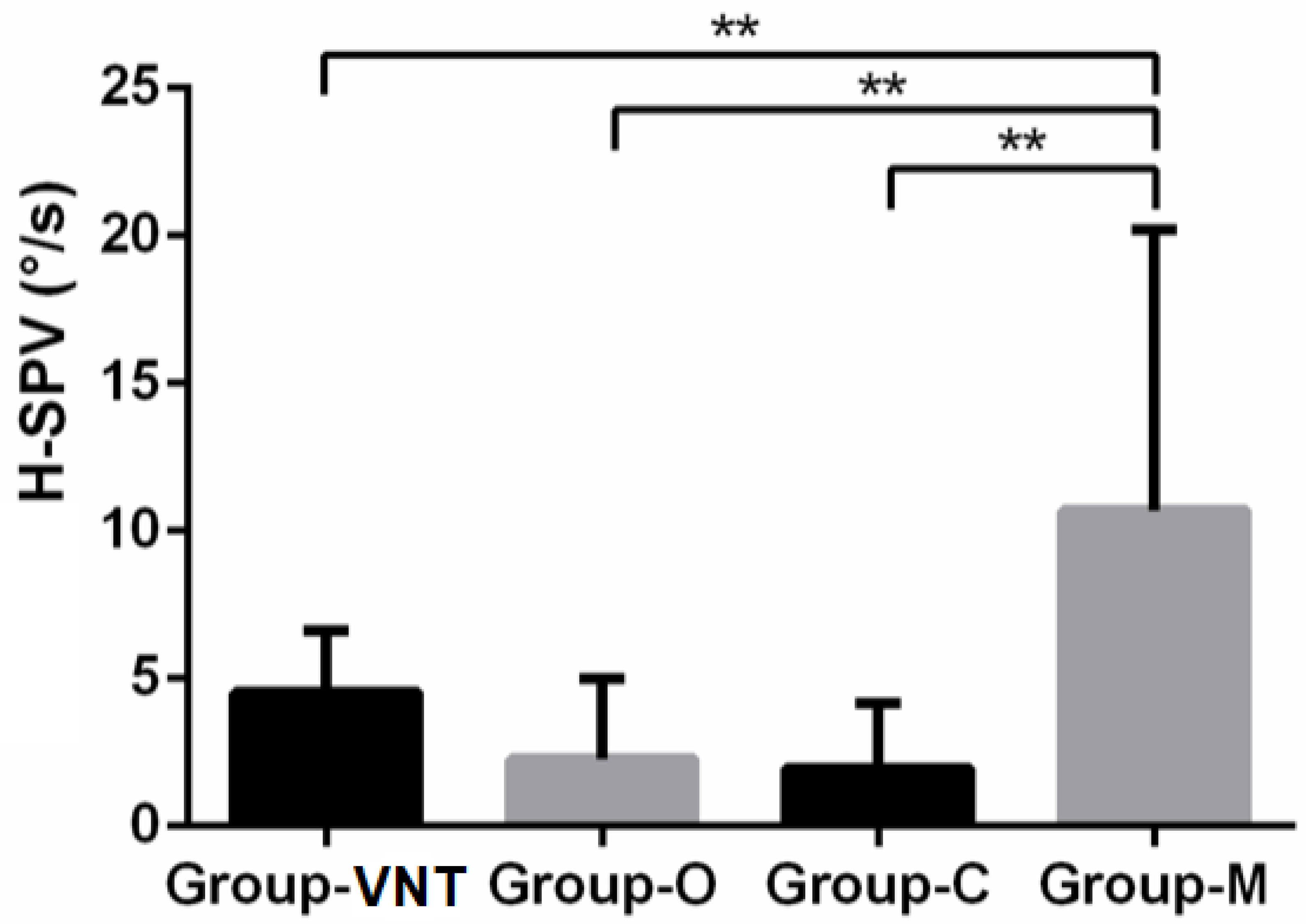
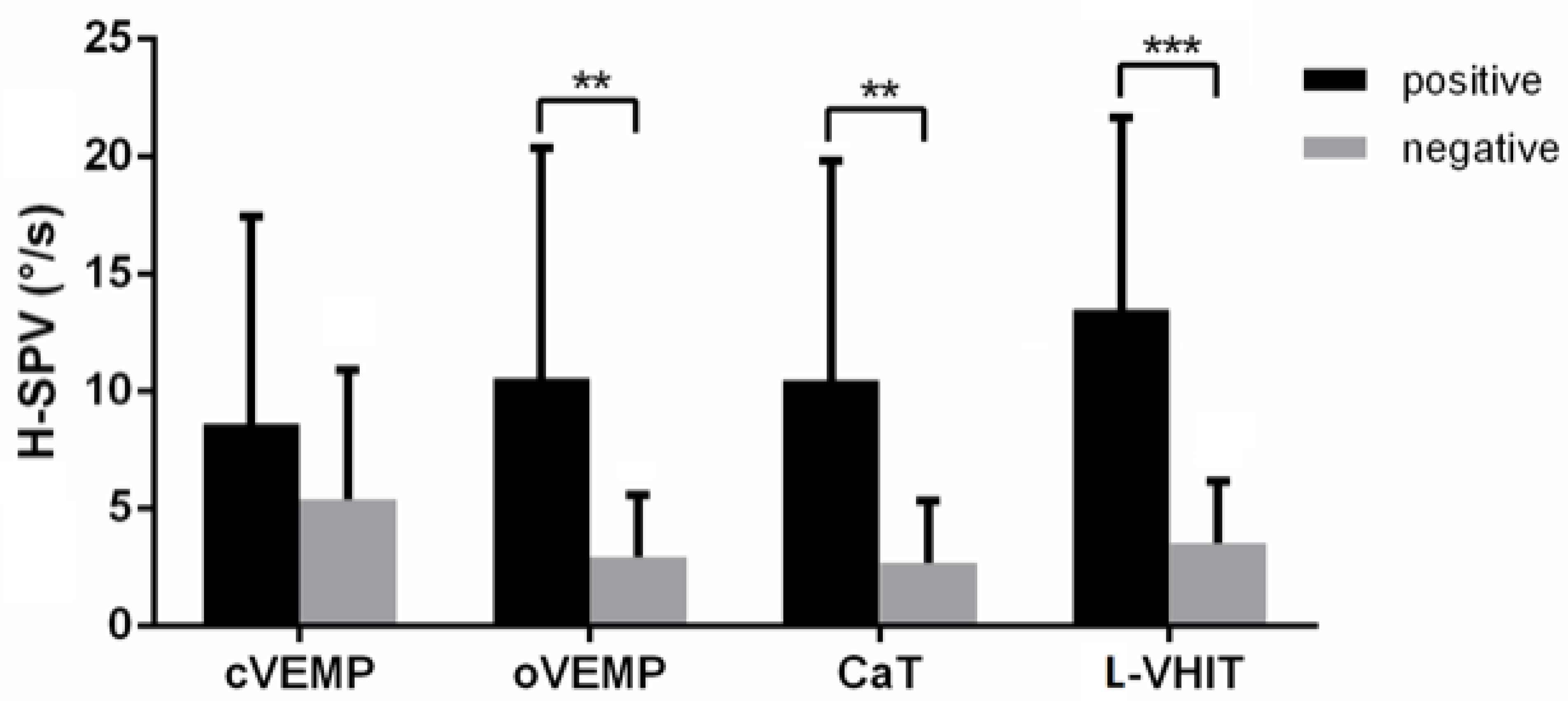
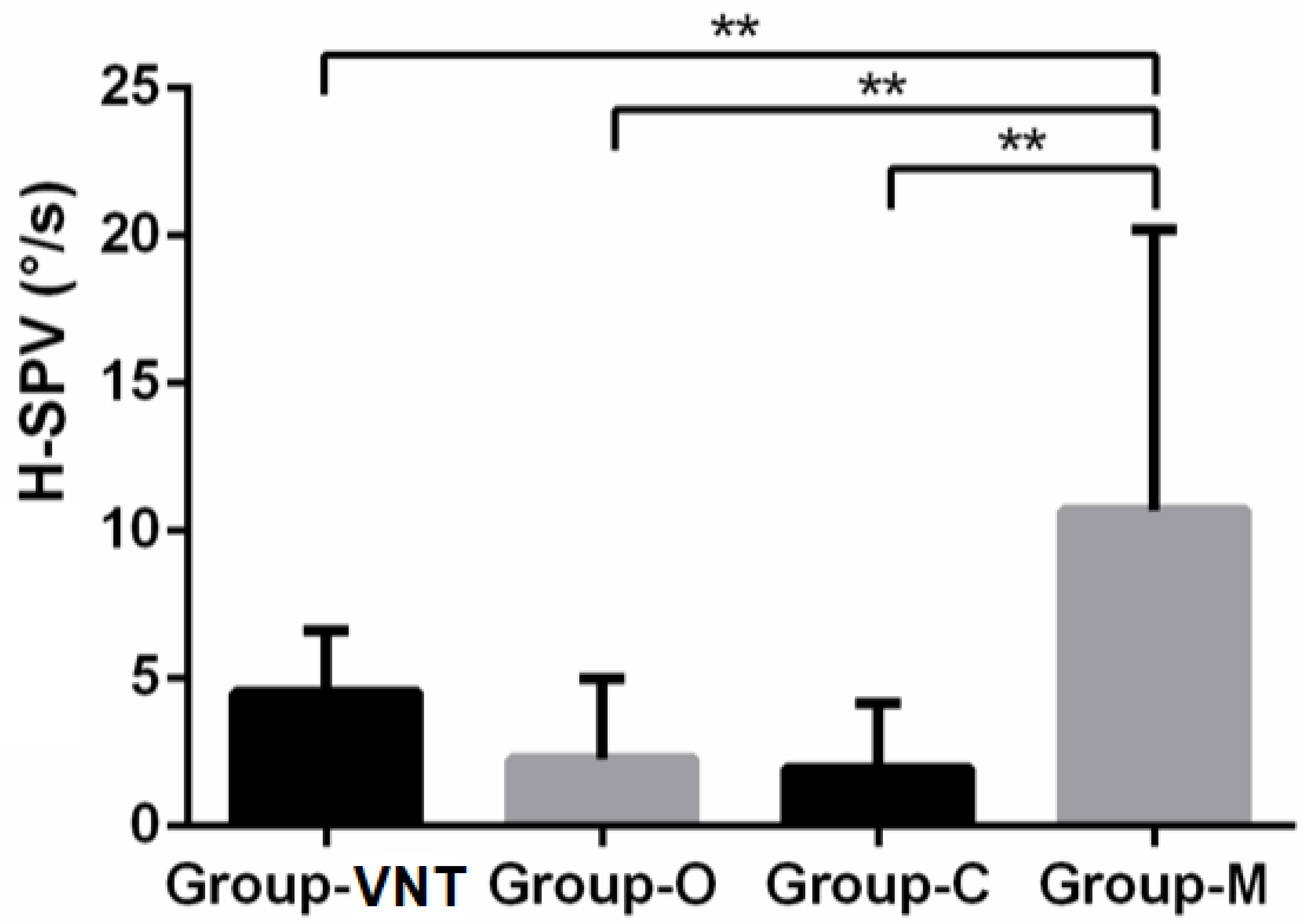
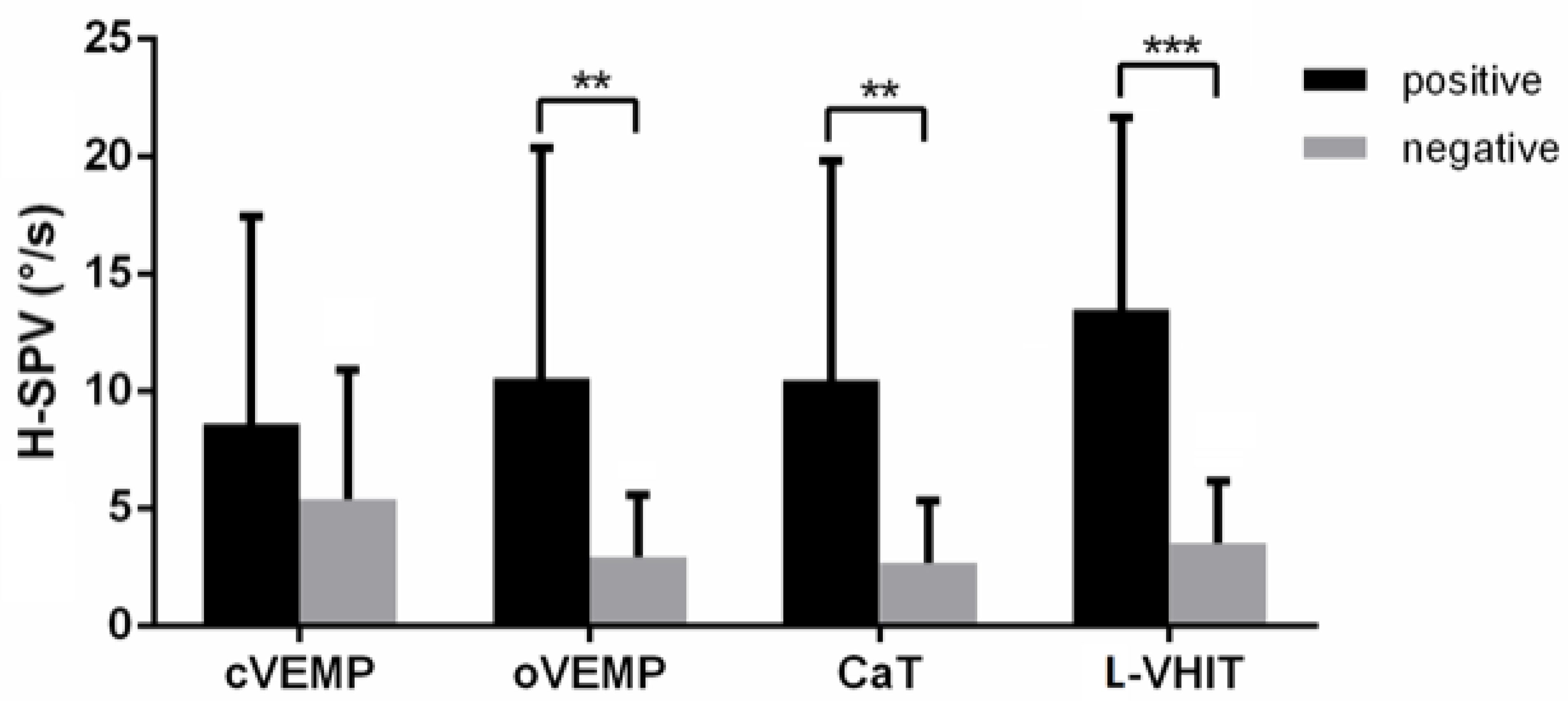
3.2. SVIN Horizontal Component
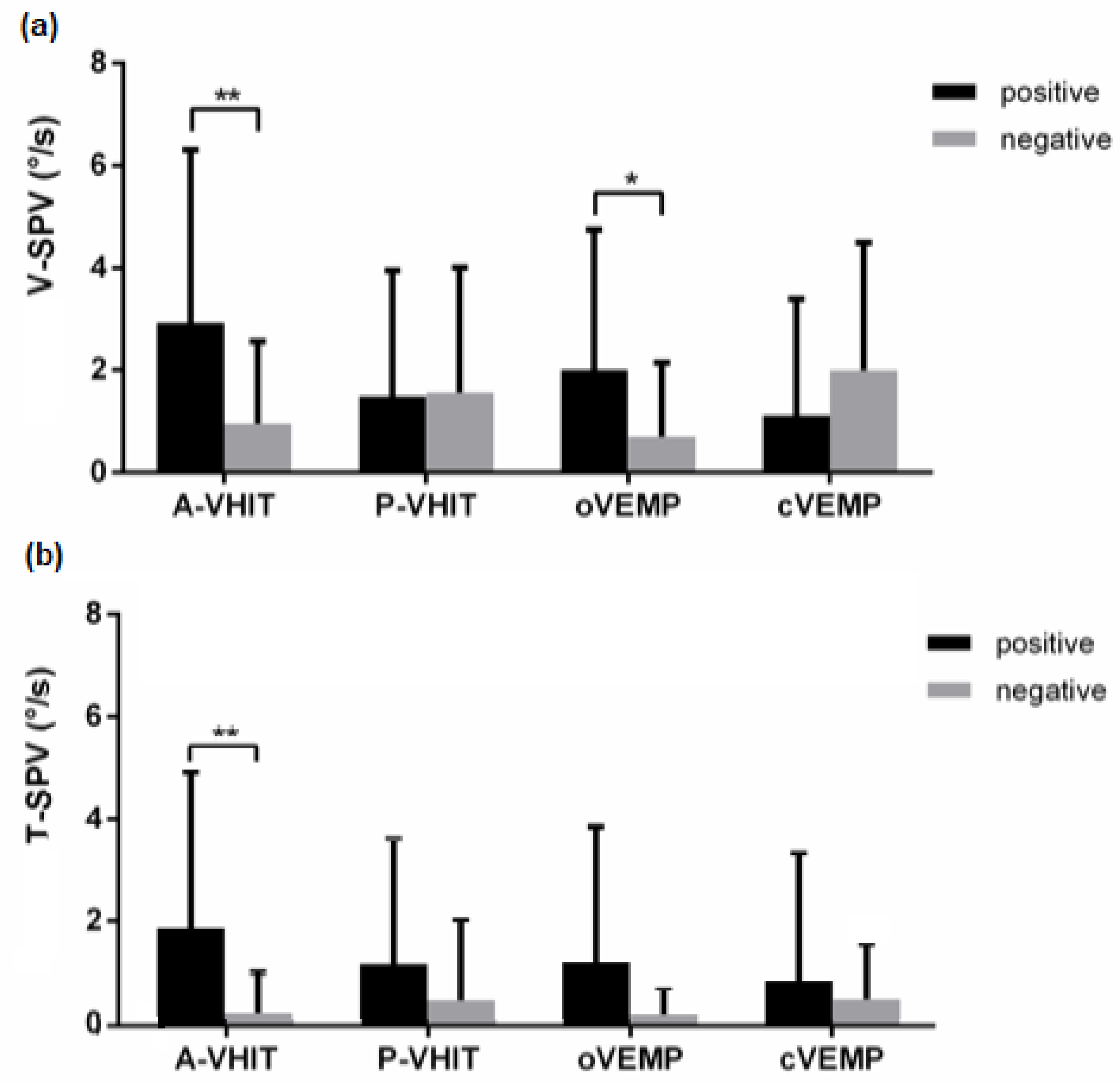
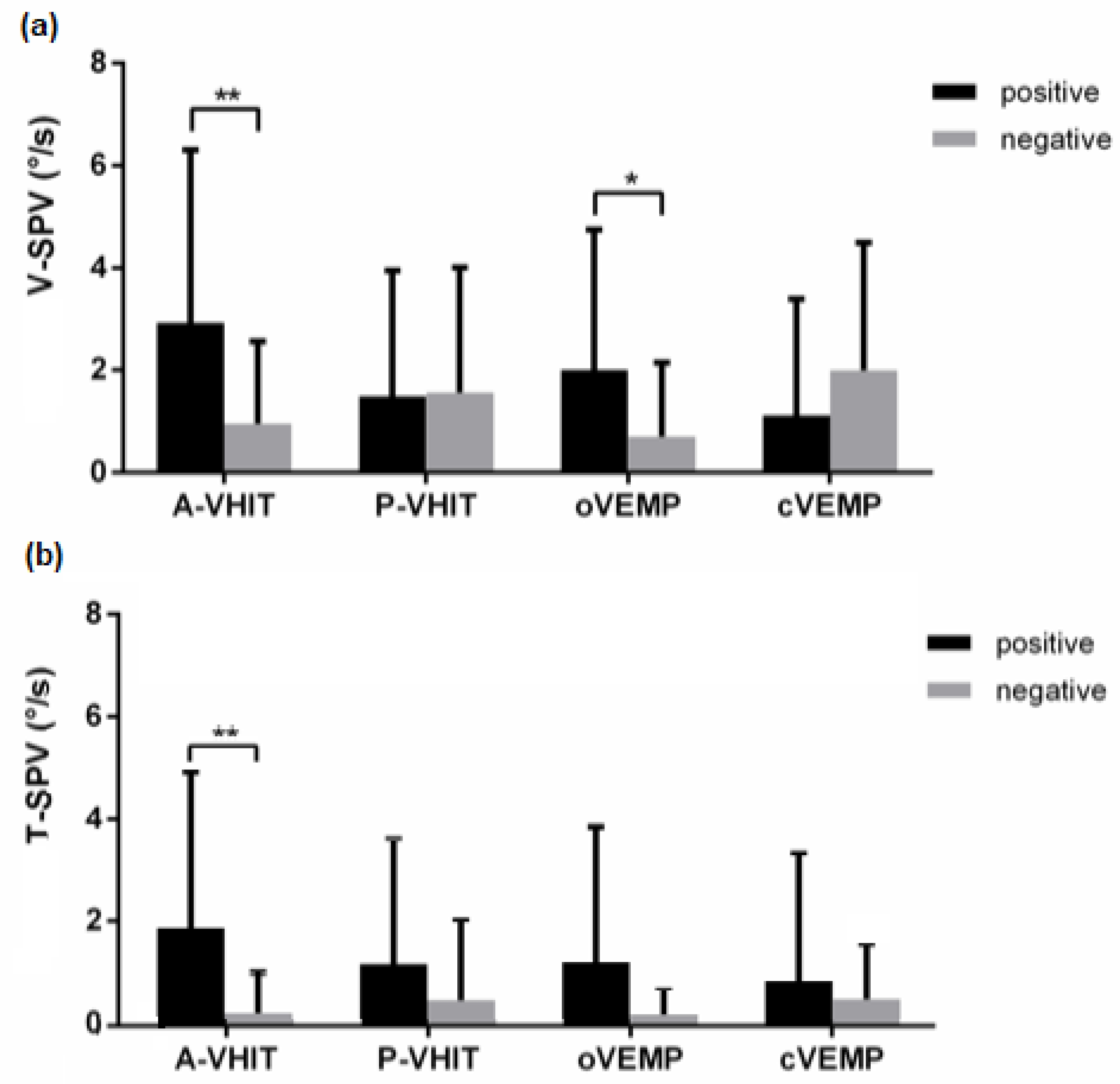
3.3. SVIN Vertical and Torsional Components
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Dumas, G.; Curthoys, I.S.; Lion, A.; Perrin, P.; Schmerber, S. The Skull Vibration-Induced Nystagmus Test of Vestibular Function-A Review. Front. Neurol. 2017, 8, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dumas, G.; Perrin, P.; Schmerber, S. Nystagmus Induced by High Frequency Vibrations of the Skull in Total Unilateral Peripheral Vestibular Lesions. Acta Otolaryngol. 2008, 128, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Dumas, G.; Perrin, P.; Ouedraogo, E.; Schmerber, S. How to Perform the Skull Vibration-Induced Nystagmus Test (SVINT). Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2016, 133, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Dumas, G.; Lion, A.; Karkas, A.; Perrin, P.; Perottino, F.; Schmerber, S. Skull Vibration-Induced Nystagmus Test in Unilateral Superior Canal Dehiscence and Otosclerosis: A Vestibular Weber Test. Acta Otolaryngol. 2014, 134, 588–600. [Google Scholar] [CrossRef]
- Park, H.; Hong, S.-C.; Shin, J. Clinical Significance of Vibration-Induced Nystagmus and Head-Shaking Nystagmus through Follow-up Examinations in Patients with Vestibular Neuritis. Otol. Neurotol. 2008, 29, 375–379. [Google Scholar] [CrossRef]
- Park, H.; Lee, Y.; Park, M.; Kim, J.; Shin, J. Test-Retest Reliability of Vibration-Induced Nystagmus in Peripheral Dizzy Patients. J. Vestib. Res. 2010, 20, 427–431. [Google Scholar] [CrossRef]
- Lee, J.M.; Kim, M.J.; Kim, J.W.; Shim, D.B.; Kim, J.; Kim, S.H. Vibration-Induced Nystagmus in Patients with Vestibular Schwannoma: Characteristics and Clinical Implications. Clin. Neurophysiol. 2017, 128, 1372–1379. [Google Scholar] [CrossRef]
- Nuti, D.; Mandalà, M. Sensitivity and Specificity of Mastoid Vibration Test in Detection of Effects of Vestibular Neuritis. Acta Otorhinolaryngol. Ital. 2005, 25, 271–276. [Google Scholar]
- Curthoys, I.S.; Kim, J.; McPhedran, S.K.; Camp, A.J. Bone Conducted Vibration Selectively Activates Irregular Primary Otolithic Vestibular Neurons in the Guinea Pig. Exp. Brain Res. 2006, 175, 256–267. [Google Scholar] [CrossRef]
- Curthoys, I.S.; Vulovic, V.; Burgess, A.M.; Sokolic, L.; Goonetilleke, S.C. The Response of Guinea Pig Primary Utricular and Saccular Irregular Neurons to Bone-Conducted Vibration (BCV) and Air-Conducted Sound (ACS). Hear. Res. 2016, 331, 131–143. [Google Scholar] [CrossRef]
- Hamann, K.F.; Schuster, E.M. Vibration-Induced Nystagmus—A Sign of Unilateral Vestibular Deficit. ORL J. Otorhinolaryngol. Relat. Spec. 1999, 61, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Dumas, G.; Tan, H.; Dumas, L.; Perrin, P.; Lion, A.; Schmerber, S. Skull Vibration Induced Nystagmus in Patients with Superior Semicircular Canal Dehiscence. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2019, 136, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Dlugaiczyk, J.; Burgess, A.M.; Goonetilleke, S.C.; Sokolic, L.; Curthoys, I.S. Superior Canal Dehiscence Syndrome: Relating Clinical Findings with Vestibular Neural Responses From a Guinea Pig Model. Otol. Neurotol. 2019, 40, e406–e414. [Google Scholar] [CrossRef] [PubMed]
- Curthoys, I.S. Concepts and Physiological Aspects of the Otolith Organ in Relation to Electrical Stimulation. AUD 2020, 25, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Dumas, G.; Michel, J.; Lavieille, J.P.; Charachon, R.; Ouedraogo, E. Clinical Value of the Cranial Vibratory Test. A 3D Analysis of the Nystagmus. J. Fr. ORL 1999, 48, 13–21. [Google Scholar]
- Yagi, T.; Ohyama, Y. Three-Dimensional Analysis of Nystagmus Induced by Neck Vibration. Acta Otolaryngol. 1996, 116, 167–169. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Soper, J.; Lohse, C.M.; Eggers, S.D.Z.; Kaufman, K.R.; McCaslin, D.L. Agreement between the Skull Vibration-Induced Nystagmus Test and Semicircular Canal and Otolith Asymmetry. J Am. Acad. Audiol. 2021, 32, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Fujimoto, C.; Kawahara, T.; Yagi, M.; Murofushi, T. Association between Vestibular Dysfunction and Findings of Horizontal Head-Shaking and Vibration-Induced Nystagmus. J. Vestib. Res. 2020, 30, 319–327. [Google Scholar] [CrossRef]
- Lopez-Escamez, J.A.; Carey, J.; Chung, W.-H.; Goebel, J.A.; Magnusson, M.; Mandalà, M.; Newman-Toker, D.E.; Strupp, M.; Suzuki, M.; Trabalzini, F.; et al. Diagnostic criteria for Menière’s disease. Consensus document of the Bárány Society, the Japan Society for Equilibrium Research, the European Academy of Otology and Neurotology (EAONO), the American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS) and the Korean Balance Society. Acta Otorrinolaringol. Esp. 2016, 67, 1–7. [Google Scholar] [CrossRef]
- Strupp, M.; Magnusson, M. Acute Unilateral Vestibulopathy. Neurol. Clin. 2015, 33, 669–685. [Google Scholar] [CrossRef]
- Slater, R. Benign Recurrent Vertigo. J. Neurol. Neurosurg. Psychiatry 1979, 42, 363–367. [Google Scholar] [CrossRef] [Green Version]
- van Esch, B.F.; van Wensen, E.; van der Zaag-Loonen, H.J.; Benthem, P.P.G.v.; van Leeuwen, R.B. Clinical Characteristics of Benign Recurrent Vestibulopathy: Clearly Distinctive From Vestibular Migraine and Menière’s Disease? Otol. Neurotol. 2017, 38, e357–e363. [Google Scholar] [CrossRef]
- Ducroz, C.; Dumas, G.; Quatre, R.; Attyé, A.; Fabre, C.; Schmerber, S. Benign Recurrent Vestibulopathy: MRI and Vestibular Tests Results in a Series of 128 Cases. Eur. Arch. Otorhinolaryngol. 2021, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Dlugaiczyk, J.; Lempert, T.; Lopez-Escamez, J.A.; Teggi, R.; von Brevern, M.; Bisdorff, A. Recurrent Vestibular Symptoms Not Otherwise Specified: Clinical Characteristics Compared with Vestibular Migraine and Menière’s Disease. Front. Neurol. 2021, 12, 674092. [Google Scholar] [CrossRef] [PubMed]
- Maheu, M.; Houde, M.-S.; Landry, S.P.; Champoux, F. The Effects of Aging on Clinical Vestibular Evaluations. Front. Neurol. 2015, 6, 205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dumas, G.; Charachon, R.; Lavieille, J.P. Benign Positioning Vertigo (BPV) and Three-Dimensional (3-D) Eye Movement Analysis. Acta. Otorhinolaryngol. Belg. 1998, 52, 291–307. [Google Scholar] [PubMed]
- Starkov, D.; Strupp, M.; Pleshkov, M.; Kingma, H.; van de Berg, R. Diagnosing Vestibular Hypofunction: An Update. J. Neurol. 2021, 268, 377–385. [Google Scholar] [CrossRef]
- Angelaki, D.E. Eyes on Target: What Neurons Must Do for the Vestibuloocular Reflex during Linear Motion. J. Neurophysiol. 2004, 92, 20–35. [Google Scholar] [CrossRef]
- Dumas, G.; Fabre, C.; Charpiot, A.; Fath, L.; Chaney-Vuong, H.; Perrin, P.; Schmerber, S. Skull Vibration-Induced Nystagmus Test in a Human Model of Horizontal Canal Plugging. Audiol. Res. 2021, 11, 301–312. [Google Scholar] [CrossRef]
- Suzuki, J.I.; Tokumasu, K.; Goto, K. Eye Movements from Single Utricular Nerve Stimulation In The Cat. Acta Oto-Laryngol. 1969, 68, 350–362. [Google Scholar] [CrossRef]
- Isu, N.; Graf, W.; Sato, H.; Kushiro, K.; Zakir, M.; Imagawa, M.; Uchino, Y. Sacculo-Ocular Reflex Connectivity in Cats. Exp. Brain Res. 2000, 131, 262–268. [Google Scholar] [CrossRef]
- Goto, F.; Meng, H.; Bai, R.; Sato, H.; Imagawa, M.; Sasaki, M.; Uchino, Y. Eye Movements Evoked by Selective Saccular Nerve Stimulation in Cats. Auris Nasus Larynx 2004, 31, 220–225. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pathology | Group-VNT | Group-O | Group-C | Group-M |
|---|---|---|---|---|
| VN | 1 | 0 | 2 | 15 |
| MD | 1 | 2 | 3 | 2 |
| BRV | 4 | 2 | 1 | 4 |
| ITG | 0 | 2 | 1 | 12 |
| Group-VNT | Group-O | Group-C | Group-M | p-value | |
|---|---|---|---|---|---|
| Cases (n) | 6 | 6 | 6 | 34 | |
| SVIN (n) | 5 | 5 | 5 | 30 | p = 1 |
| SVIN (%) | 83 | 83 | 83 | 88 | |
| H-SPV (°/s) | 4.52 ± 2.12 | 2.29 ± 2.72 | 1.96 ± 2.21 | 10.7 ± 9.50 | p < 0.01 |
| 95% CI | 1.73 | 2.22 | 1.80 | 3.26 |
| CaT | L-VHIT | oVEMP | cVEMP | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| + | − | p-Value | + | − | p-Value | + | − | p-Value | + | − | p-Value | |
| Cases (n) | 27 | 25 | 17 | 35 | 38 | 14 | 33 | 19 | ||||
| SVINT (n) | 25 | 17 | 0.036 | 16 | 26 | 0.13 | 34 | 8 | 0.016 | 25 | 17 | 0.29 |
| SVINT+ (%) | 93% | 68% | 94% | 74% | 89% | 57% | 76% | 89% | ||||
| SVIN-SPV (°/s) | 10.5 ± 8.9 | 2.7 ± 2.8 | <0.01 | 14.1 ± 7.3 | 2.6 ± 3.5 | <0.001 | 10.6 ± 10.6 | 3.0 ± 2.3 | <0.01 | 8.6 ± 8.6 | 5.4 ± 5.9 | 0.58 |
| 95% CI | 3.46 | 1.13 | 3.56 | 1.20 | 3.45 | 1.24 | 3.02 | 2.76 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fabre, C.; Tan, H.; Dumas, G.; Giraud, L.; Perrin, P.; Schmerber, S. Skull Vibration Induced Nystagmus Test: Correlations with Semicircular Canal and Otolith Asymmetries. Audiol. Res. 2021, 11, 618-628. https://doi.org/10.3390/audiolres11040056
Fabre C, Tan H, Dumas G, Giraud L, Perrin P, Schmerber S. Skull Vibration Induced Nystagmus Test: Correlations with Semicircular Canal and Otolith Asymmetries. Audiology Research. 2021; 11(4):618-628. https://doi.org/10.3390/audiolres11040056
Chicago/Turabian StyleFabre, Christol, Haoyue Tan, Georges Dumas, Ludovic Giraud, Philippe Perrin, and Sébastien Schmerber. 2021. "Skull Vibration Induced Nystagmus Test: Correlations with Semicircular Canal and Otolith Asymmetries" Audiology Research 11, no. 4: 618-628. https://doi.org/10.3390/audiolres11040056
APA StyleFabre, C., Tan, H., Dumas, G., Giraud, L., Perrin, P., & Schmerber, S. (2021). Skull Vibration Induced Nystagmus Test: Correlations with Semicircular Canal and Otolith Asymmetries. Audiology Research, 11(4), 618-628. https://doi.org/10.3390/audiolres11040056