
Genetic and Non Genetic Hearing Loss and Associated Disabilities: An Epidemiological Survey in Emilia-Romagna Region



 and
and
Abstract
:1. Introduction
2. Materials and Methods
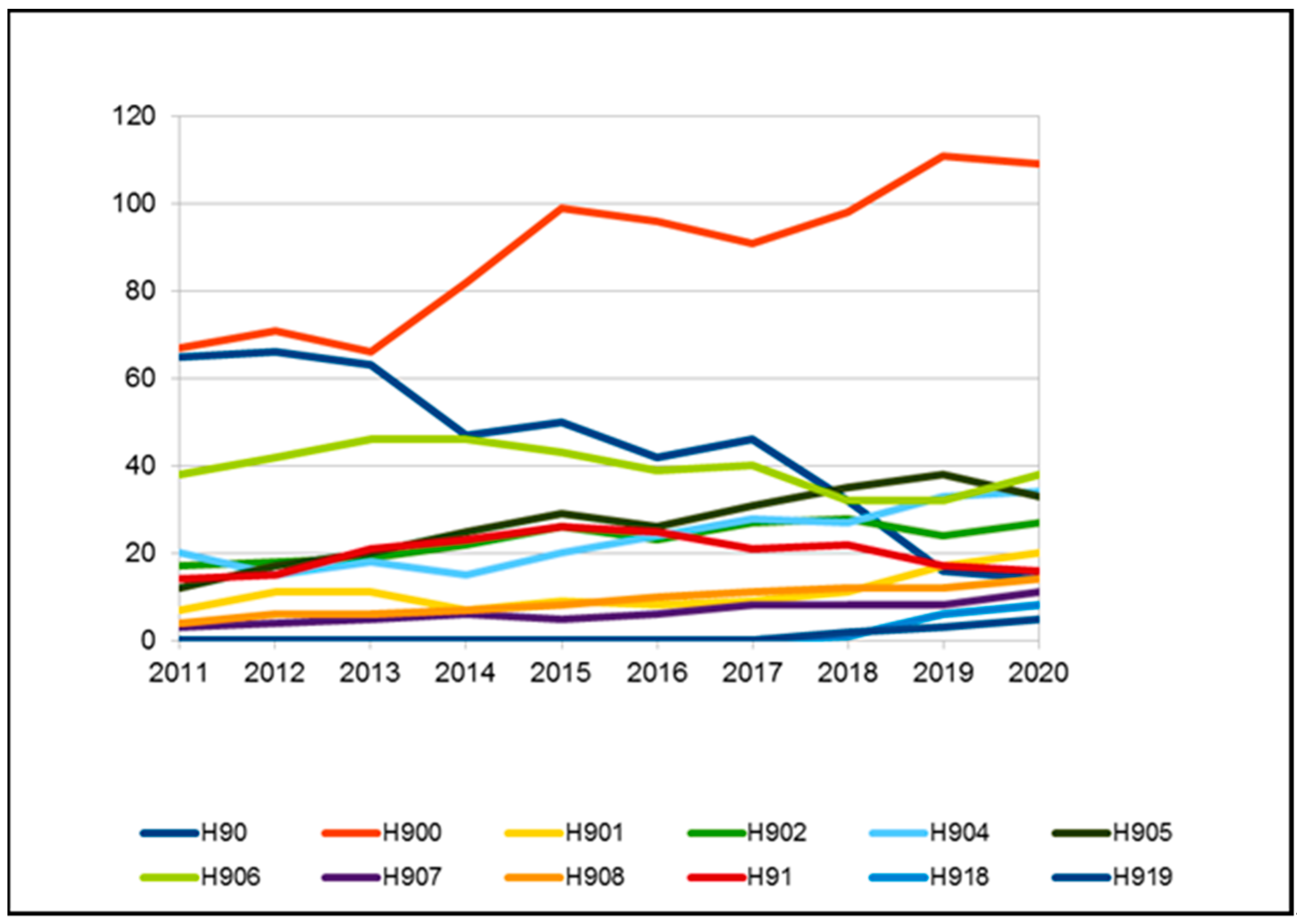
- H90 Conductive and sensorineural hearing loss:
- H90.0 Conductive hearing loss, bilateral;
- H90.1 Conductive hearing loss, unilateral with unrestricted hearing on the contralateral side;
- H90.2 Conductive hearing loss, unspecified;
- H90.3 Sensorineural hearing loss, bilateral;
- H90.4 Sensorineural hearing loss, unilateral with unrestricted hearing on the contralateral side;
- H90.5 Sensorineural hearing loss, unspecified;
- H90.6 Mixed conductive and sensorineural hearing loss, bilateral;
- H90.7 Mixed conductive and sensorineural hearing loss, unilateral with unrestricted hearing on the contralateral side;
- H90.8 Mixed conductive and sensorineural hearing loss, unspecified.
- H91 Other hearing loss:
- H91.8 Other specified hearing loss;
- H91.9 Hearing loss, unspecified.
- -
- Prevalence and incidence of H90–H91 users among the general population and among CAMHS users;
- -
- Gender and citizenship of H90–H91;
- -
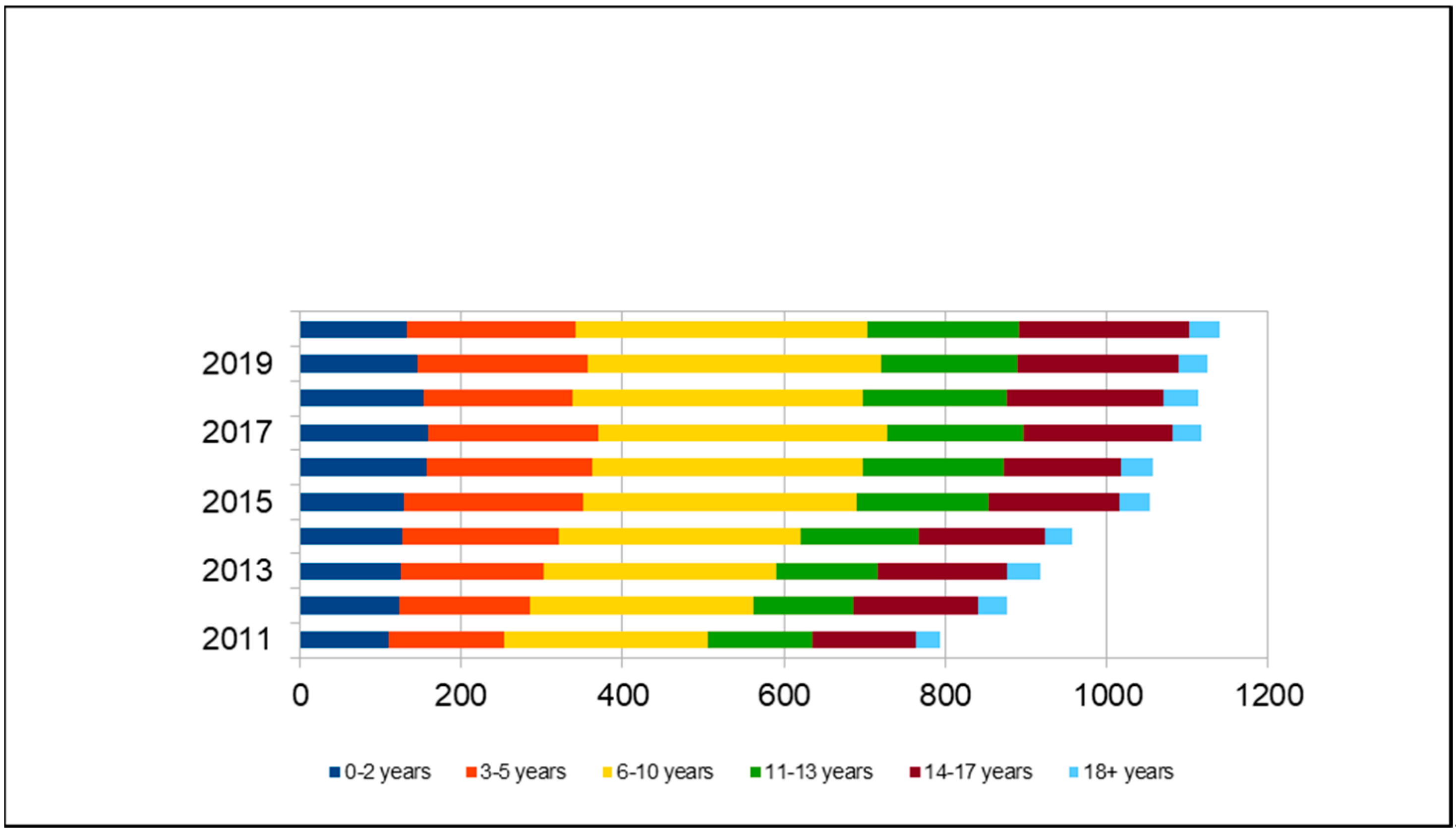
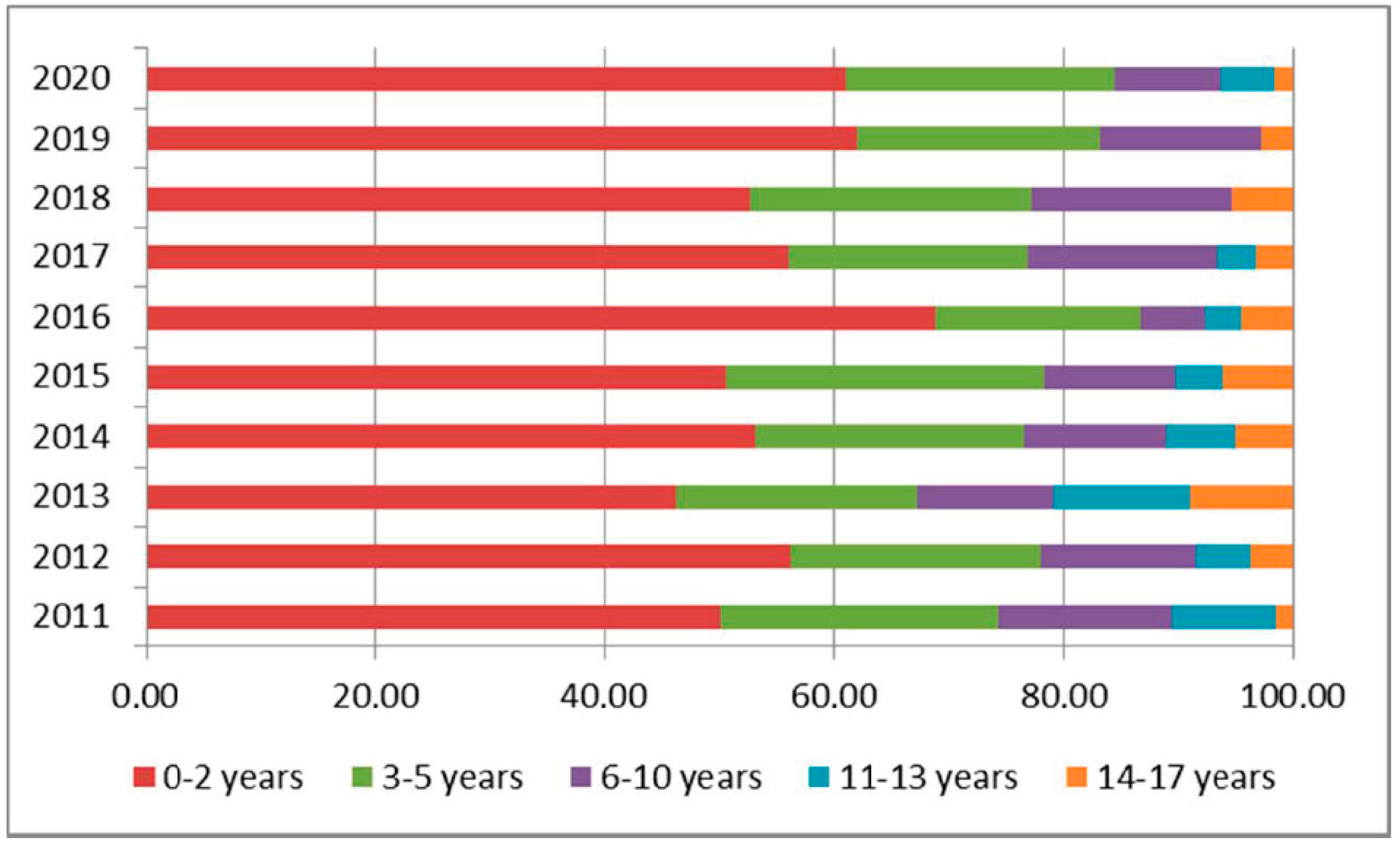
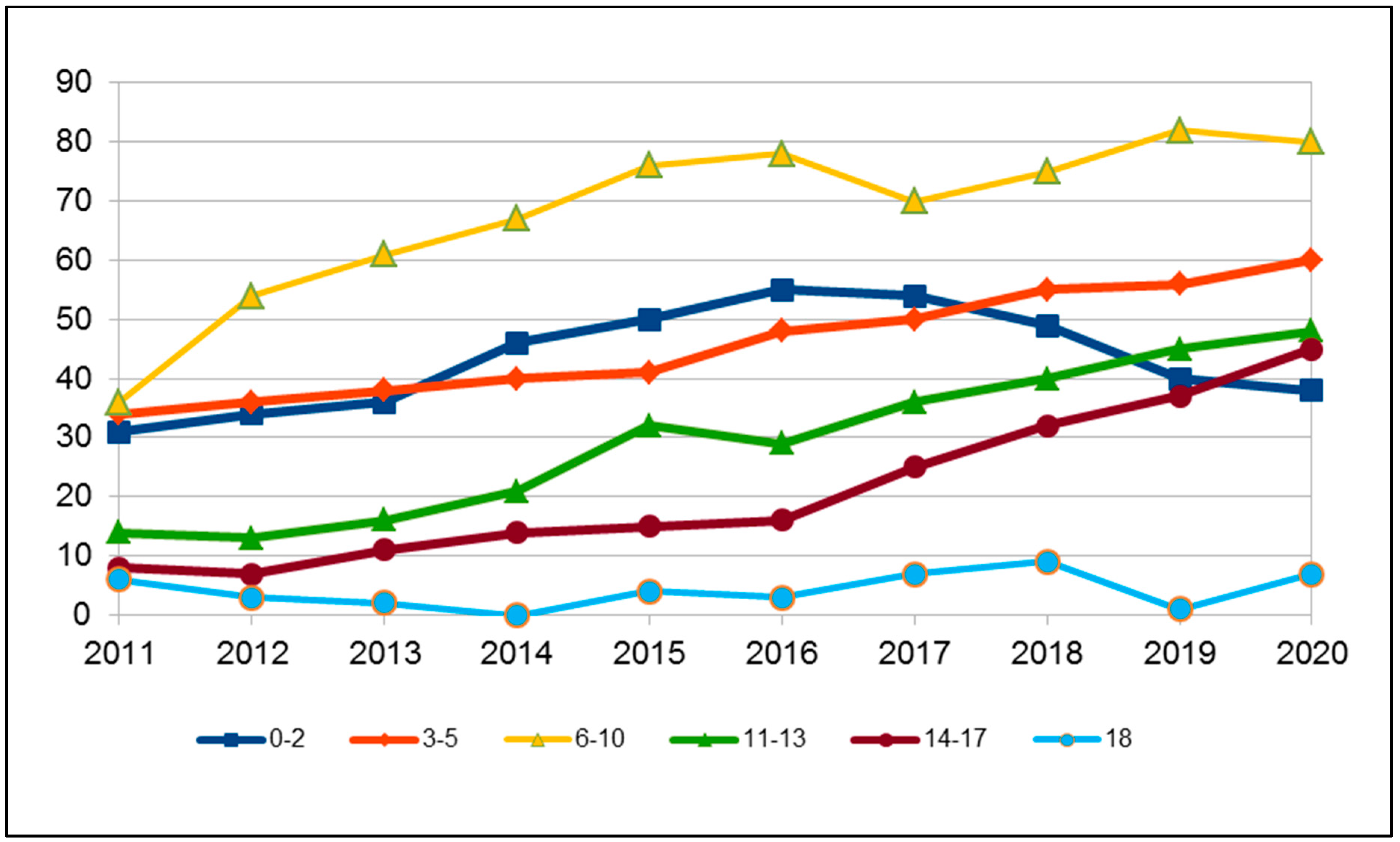
- Distribution by age range: 0–2 years, 3–5 years, 6–10 years, 11–13 years,14–17 years, and 18 years. Age range groups are related to school-aged children: maternal school, primary school, secondary school;
- -
- Number and percentage of users with isolated diagnostic codes (DC) H90-H91;
- -
- Number of DC H90-H91 with the following other associated codes:Q00–Q99 Congenital malformations, deformations and chromosomal abnormalities;Q10–Q18 Congenital malformations of eye, ear, face, and neck;Q35–Q37 Cleft lip and cleft palate;Q67 Congenitalmusculoskeletal deformities of head, face, spine, and chest;Q75 Other congenital malformations of skull and face bones;Q80–Q89 Other congenital malformations;Q90–Q99 Chromosomal abnormalities not elsewhere classified;F70–F79 Mental retardation;F84 Pervasive developmental disorders (autism spectrum disorders listed here);G80–G83 Cerebral palsy and other paralytic syndromes;H3–H59 Visual impairment;P00–P96 Certain conditions originating in the perinatal period.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Morton, C.C.; Nance, W.E. Newborn hearing screening—A silent revolution. N. Engl. J. Med. 2006, 354, 2151–2164. [Google Scholar] [CrossRef]
- van Beeck Calkoen, E.A.; Engel, M.S.D.; van de Kamp, J.M.; Yntema, H.G.; Goverts, S.T.; Mulder, M.F.; Merkus, P.; Hensen, E.F. The etiological evaluation of sensorineural hearing loss in children. Eur. J. Pediatrics 2019, 178, 1195–1205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joint Committee on Infant Hearing. Year 2019 Position statement: Principles and guidelines for early hearing detection and intervention programs. J. Early Hear. Detect. Interv. 2019, 4, 1–44. [Google Scholar]
- GPG/2011/498 Screening uditivo neonatale e percorso clinico ed organizzativo per i bambini affetti da ipoacusia in Emilia-Romagna. In Approvazione Linee Guida per le Aziende Sanitarie. 23 Maggio 2011, N. 694; Bollettino Ufficiale della Regione Emilia-Romagna: Bologna, Italy, 2011; pp. 18–49.
- Van Naarden Braun, K.; Christensen, D.; Doernberg, N.; Schieve, L.; Rice, C.; Wiggins, L.; Schendel, D.; Marshalyn Yeargin-Allsopp, M. Trends in the Prevalence of Autism Spectrum Disorder, Cerebral Palsy, Hearing Loss, Intellectual Disability, and Vision Impairment, Metropolitan Atlanta, 1991–2010. PLoS ONE 2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeargin-Allsopp, M.; Murphy, C.C.; Oakley, G.P.; Sikes, R.K. A multiple-source method for studying the prevalence of developmental disabilities in children: The Metropolitan Atlanta Developmental Disabilities Study. Pediatrics 1992, 89, 624–630. [Google Scholar] [PubMed]
- Erickson, K.; Quick, N. The Profiles of Students with Significant Cognitive Disabilities and Known Hearing Loss. J. Deaf. Stud. Deaf. Educ. 2017, 35–48, Empirical Manuscript. [Google Scholar] [CrossRef]
- Johnson, K.; Wiley, S. Cochlear implantation in children with multiple disabilities. In Clinical Management of Children with Cochlear Implants; Eisenberg, L.S., Ed.; Plural Publishing Inc.: San Diego, CA, USA, 2009. [Google Scholar]
- Birman, C.S.; Elliott, E.J.; Gibson, W.P. Pediatric cochlear implants: Additional disabilities prevalence, risk factors, and effect on language outcomes. Otol Neurotol. 2012, 33, 1347–1452. [Google Scholar] [CrossRef] [PubMed]
- Berrettini, S.; Forli, F.; Genovese, E.; Santarelli, R.; Arslan, E.; Chilosi, A.M.; Cipriani, P. Cochlear implantation in deaf children with associated disabilities: Challenges and outcomes. Int. J. Audiol. 2008, 47, 199–208. [Google Scholar] [CrossRef]
- Olusanya, B.O.; Wright, S.M.; Nair, M.K.C.; Boo, N.Y.; Halpern, R.; Kuper, H.; Abubakar, A.A.; Almasri, N.A.; Arabloo, J.; Arora, N.K.; et al. Global Burden of Childhood Epilepsy, Intellectual Disability, and Sensory Impairments. Pediatrics 2020, 146, e20192623. [Google Scholar] [CrossRef]
- Manual of International Statistical Classification of Diseases and Related Health Problems; ICD 10th Revision; World Health Organization: Geneva, Switzerland, 2010.
- Alford, R.L.; Arnos, K.S.; Fox, M.; Lin, J.W.; Palmer, C.G.; Pandya, A.; Rehm, H.L.; Robin, N.H.; Scott, D.A.; Yoshinaga-Itano, C. American college of medical genetics and genomics guideline for the clinical evaluation and etiologic diagnosis of hearing loss. Genet. Med. 2014, 16, 347–355. [Google Scholar]
- Morgan, A.; Gasparini, P.; Girotto, G. Molecular testing for the study of non-syndromic hearing loss. Hear. Balance Commun. 2020, 18, 270–277. [Google Scholar] [CrossRef]
- Bussè, A.M.L.; Hoeve, H.L.J.; Nasserinejadb, K.; Mackey, R.A.; Simonsz, H.J.; Goedegebure, A. Prevalence of permanent neonatal hearing impairment: Systematic review and Bayesian meta-analysis. Int. J. Audiol. 2020, 59, 475–485. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Sung, V.; Carew, P.; Burt, R.A.; Liu, M.; Wang, Y.; Afandi, A.; Wake, M. Prevalence of childhood hearing loss and secular trends: A systematic review and meta-analysis. Acad. Pediatr. 2019, 19, 504–514. [Google Scholar] [CrossRef]
- World Health Organization. The Global Burden of Disease: 2004 Update; World Health Organization: Geneva, Switzerland, 2008; Available online: www.who.int/iris/handle/10665/43942 (accessed on 15 July 2021).
- Awad, R.; Oropeza, J.; Uhlera, K.M. Meeting the Joint Committee on Infant Hearing Standards in a Large Metropolitan Children’s Hospital: Barriers and Next Steps. Am. J. Audiol. 2019, 28, 251–259. [Google Scholar] [CrossRef]
- McGuire, D.O.; Tiana, L.H.; Yeargin-Allsopp, M.; Dowling, N.F.; Christensen, D.L. Prevalence of cerebral palsy, intellectual disability, hearing loss, and blindness, National Health Interview Survey, 2009–2016. Disabil. Health J. 2019, 12, 443–451. [Google Scholar] [CrossRef]
- Smith, A.; Taggart, R.T. Chapt. Genetic Hearing Loss with No Associated Abnormalities. In Hereditary Hearing Loss and Its Syndromes; Toriello, H.V., Reardon, W., Gorlin, R.J., Eds.; Oxford University Press: New York, NY, USA, 2004. [Google Scholar]
- Morgan, A.; Pelliccione, G.; Ambrosetti, U.; Dell’Orco, D.; Girotto, G. SLC12A2: A new gene associated with autosomal dominant Non-Syndromic hearing loss in humans. Hear. Balance Commun. 2020, 18, 149–151. [Google Scholar] [CrossRef]
- Brotto, D.; Uberti, A.; Manara, R. From Mondini to the latest inner ear malformations’ classifications: An historical and critical review. Hear. Balance Commun. 2019, 17, 241–248. [Google Scholar] [CrossRef]
- Lieu, J.E.C.; Kenna, M.; Anne, S.; Davidson, L. Hearing Loss in Children A Review. JAMA 2020, 324, 2195. [Google Scholar] [CrossRef] [PubMed]
- Zablotsky, B.; Black, I.L.; Maenner, M.J.; Schieve, L.A.; Danielson, M.L.; Bitsko, R.H.; Blumberg, S.J.; Kogan, M.D.; Boyle, C.A. Prevalence and Trends of Developmental Disabilities among Children in the US: 2009–2017. Pediatrics 2019, 144. [Google Scholar] [CrossRef]
- Petrini, J.R.; Dias, T.; McCormick, M.C.; Massolo, M.L.; Green, N.S.; Escobar, G.J. Increased risk of adverse neurological development for late preterm infants. J. Pediatr. 2009, 154, 169–176. [Google Scholar] [CrossRef]
- Ideura, M.; Nishio, S.; Moteki, H.; Takumi, Y.; Miyagawa, M.; Sato, T.; Kobayashi, Y.; Ohyama, K.; Oda, K.; Matsui, T.; et al. Comprehensive analysis of syndromic hearing loss patients in Japan. Sci. Rep. 2019, 9, 11976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pakula, A.T.; Van Naarden Braun, K.; Yeargin-Allsopp, M. Cerebral palsy: Classification and epidemiology. Phys. Med. Rehabil. Clin. 2009, 20, 425–452. [Google Scholar] [CrossRef] [PubMed]
- Dufresne, D.; Dagenais, L.; Shevell, M.I. Epidemiology of severe hearing impairment in a population-based cerebral palsy cohort. Pediatr. Neurol. 2014, 51, 641–644. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
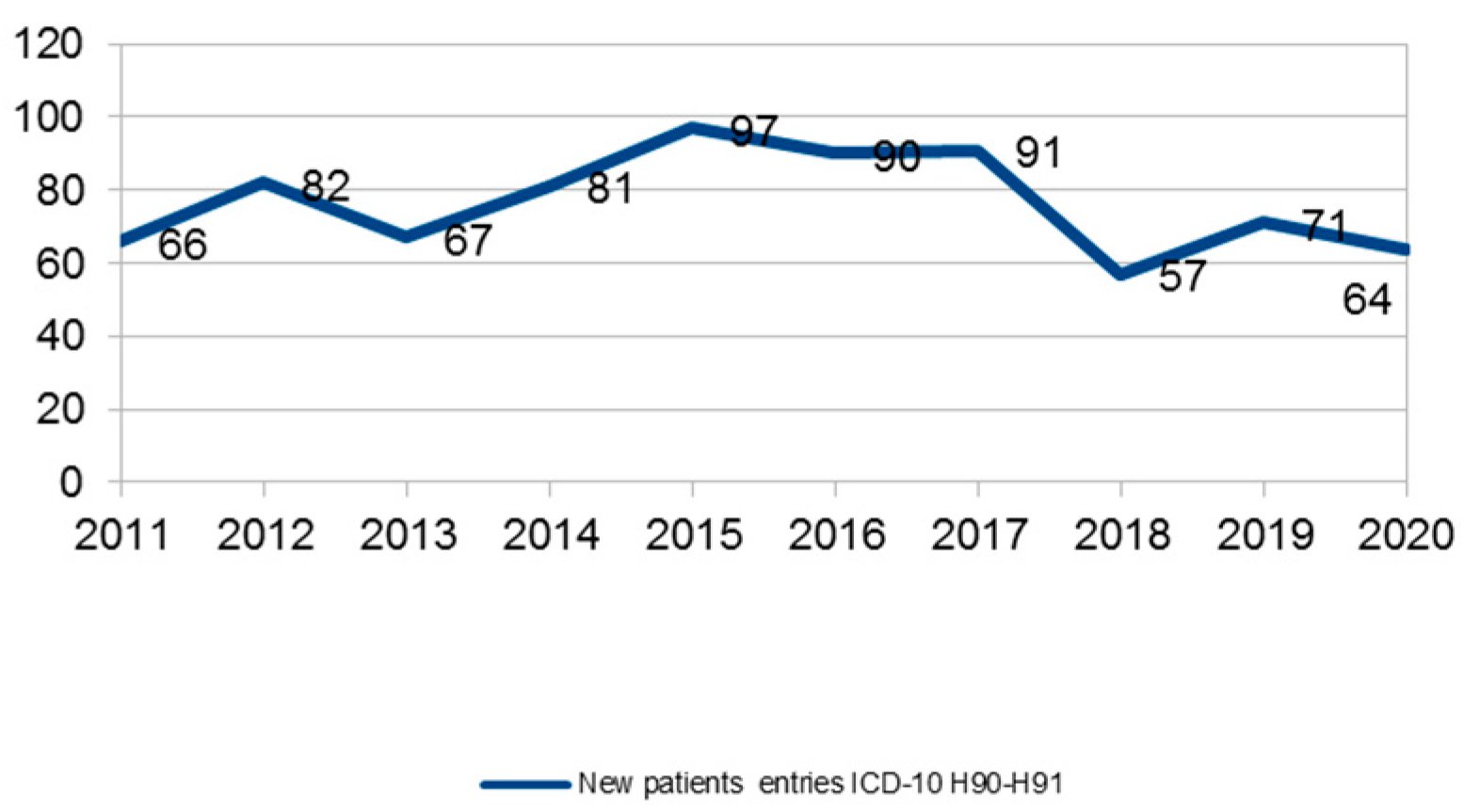
| Years | Pop. Age 0–17 | Patients under UONPIA-ER Care | Patients H.90–91 Diagnosis under UONPIA-ER Care | Prevalence:1000 | Incidence:10.000 |
|---|---|---|---|---|---|
| 2011 | 695.043 | 41.012 | 794 (1.9%) | 1.1 | 0.95 |
| 2012 | 704.716 | 45.079 | 876 (1.9%) | 1.2 | 1.16 |
| 2013 | 711.268 | 48.486 | 917 (1.9%) | 1.3 | 0.94 |
| 2014 | 712.298 | 50.660 | 957 (1.9%) | 1.3 | 1.14 |
| 2015 | 714.051 | 52.132 | 1053 (2%) | 1.5 | 1.36 |
| 2016 | 713.391 | 54.007 | 1058 (2%) | 1.5 | 1.26 |
| 2017 | 711.765 | 57.996 | 1118 (1.9%) | 1.6 | 1.28 |
| 2018 | 708.622 | 59.897 | 1114 (1.9%) | 1.6 | 0.80 |
| 2019 | 704.439 | 62.353 | 1125 (1.8%) | 1.6 | 1.01 |
| 2020 | 698.003 | 56.405 | 1140 (2%) | 1.6 | 0.92 |
| Age Group | ||||||
|---|---|---|---|---|---|---|
| Year | 0–2 Years | 3–5 Years | 6–10 Years | 11–13 Years | 14–17 Years | Total |
| 2011 | 50.00 | 24.24 | 15.15 | 9.09 | 1.52 | 100 |
| 2012 | 56.10 | 21.95 | 13.41 | 4.88 | 3.66 | 100 |
| 2013 | 46.27 | 20.90 | 11.94 | 11.94 | 8.96 | 100 |
| 2014 | 53.09 | 23.46 | 12.35 | 6.17 | 4.94 | 100 |
| 2015 | 50.52 | 27.84 | 11.34 | 4.12 | 6.19 | 100 |
| 2016 | 68.89 | 17.78 | 5.56 | 3.33 | 4.44 | 100 |
| 2017 | 56.04 | 20.88 | 16.48 | 3.30 | 3.30 | 100 |
| 2018 | 52.63 | 24.56 | 17.54 | 0.00 | 5.26 | 100 |
| 2019 | 61.97 | 21.13 | 14.08 | 0.00 | 2.82 | 100 |
| 2020 | 60.94 | 23.44 | 9.38 | 4.69 | 1.56 | 100 |
| ICD-10 Diagnosis | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 |
|---|---|---|---|---|---|---|---|---|---|---|
| H90 | 8.19 | 7.53 | 6.87 | 4.91 | 4.75 | 3.97 | 4.11 | 2.87 | 1.42 | 1.23 |
| H900 | 8.44 | 8.11 | 7.20 | 8.57 | 9.40 | 9.07 | 8.14 | 8.80 | 9.87 | 9.56 |
| H901 | 0.88 | 1.26 | 1.20 | 0.73 | 0.85 | 0.76 | 0.81 | 0.99 | 1.51 | 1.75 |
| H902 | 2.14 | 2.05 | 2.07 | 2.30 | 2.47 | 2.17 | 2.42 | 2.51 | 2.13 | 2.37 |
| H903 | 68.89 | 69.75 | 70.01 | 70.74 | 70.09 | 71.74 | 72.09 | 72.35 | 71.82 | 71.14 |
| H904 | 2.52 | 1.71 | 1.96 | 1.57 | 1.90 | 2.27 | 2.50 | 2.42 | 2.93 | 2.98 |
| H905 | 1.51 | 1.94 | 2.18 | 2.61 | 2.75 | 2.46 | 2.77 | 3.14 | 3.38 | 2.89 |
| H906 | 4.79 | 4.79 | 5.02 | 4.81 | 4.08 | 3.69 | 3.58 | 2.87 | 2.84 | 3.33 |
| H907 | 0.38 | 0.46 | 0.55 | 0.63 | 0.47 | 0.57 | 0.72 | 0.72 | 0.71 | 0.96 |
| H908 | 0.50 | 0.68 | 0.65 | 0.73 | 0.76 | 0.95 | 0.98 | 1.08 | 1.07 | 1.23 |
| H91 | 1.76 | 1.71 | 2.29 | 2.40 | 2.47 | 2.36 | 1.88 | 1.97 | 1.51 | 1.40 |
| H918 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.09 | 0.53 | 0.70 |
| H919 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.18 | 0.27 | 0.44 |
| tot | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 |
| Years | Patients with H.90–91 Diagnosis under UONPIA-ER Care | Patients with Only Hearing-Loss H.90–91 | Patients with Hearing-Loss H.90–91 and Associated Diseases |
|---|---|---|---|
| 2011 | 794 | 466 (58.7%) | 328 (41.3%) |
| 2012 | 876 | 521 (59.5%) | 355 (40.5%) |
| 2013 | 917 | 529 (57.6%) | 388 (42.4%) |
| 2014 | 957 | 524 (54.7%) | 433 (45.3%) |
| 2015 | 1053 | 561 (53.3%) | 492 (46.7%) |
| 2016 | 1058 | 558 (52.7%) | 500 (47.3%) |
| 2017 | 1118 | 565 (50.5%) | 553 (49.5%) |
| 2018 | 1114 | 550 (49.4%) | 564 (50.6%) |
| 2019 | 1125 | 474 (42.1%) | 651 (57.9%) |
| 2020 | 1140 | 467 (40.9%) | 673 (59.1%) |
| ICD-10 Diagnosis | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 |
|---|---|---|---|---|---|---|---|---|---|---|
| Q Q00–Q99 = Congenital Malformations. Deformations and Chromosomal Abnormalities | 13.9 | 15.02 | 15.46 | 15.89 | 16.87 | 17.05 | 16.97 | 17.97 | 16.16 | 17.18 |
| F70-F79 = Mental Retardation | 14.66 | 13.38 | 14.23 | 14.62 | 13.16 | 13.48 | 12.83 | 13.34 | 14.92 | 15.33 |
| P00-P96 = Certain Conditions Originating in the Perinatal Period | 8.08 | 7.97 | 7.63 | 7.61 | 7.82 | 7.82 | 7.43 | 7.05 | 5.88 | 5.44 |
| G G80-G83 Cerebral Palsy and other Paralytic Syndromes | 4.74 | 5.1 | 4.43 | 3.72 | 3.64 | 3.72 | 3.51 | 3.32 | 2.85 | 2.6 |
| F84 Pervasive Developmental Disorders | 1.51 | 1.33 | 0.94 | 0.85 | 1.63 | 1.71 | 1.96 | 2.14 | 1.92 | 2.41 |
| H3-H5 Visual Impairment | 5.28 | 5.52 | 5.56 | 5.83 | 5.5 | 5.29 | 5.75 | 5.81 | 5.08 | 5.13 |
| Years | Q Q00–Q99 = Congenital Malformations. Deformations and Chromosomal Abnormalities | Prevalence Pop 0–17 Years:10000 |
|---|---|---|
| 2011 | 129 | 1.9 |
| 2012 | 147 | 2.1 |
| 2013 | 164 | 2.3 |
| 2014 | 188 | 2.6 |
| 2015 | 218 | 3.1 |
| 2016 | 229 | 3.2 |
| 2017 | 242 | 3.4 |
| 2018 | 260 | 3.7 |
| 2019 | 261 | 3.7 |
| 2020 | 278 | 4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Genovese, E.; Palma, S.; Polizzi, V.; Bianchin, G.; Cappai, M.; Kaleci, S.; Martini, A.; Ciorba, A.; Stagi, P. Genetic and Non Genetic Hearing Loss and Associated Disabilities: An Epidemiological Survey in Emilia-Romagna Region. Audiol. Res. 2021, 11, 463-473. https://doi.org/10.3390/audiolres11030043
Genovese E, Palma S, Polizzi V, Bianchin G, Cappai M, Kaleci S, Martini A, Ciorba A, Stagi P. Genetic and Non Genetic Hearing Loss and Associated Disabilities: An Epidemiological Survey in Emilia-Romagna Region. Audiology Research. 2021; 11(3):463-473. https://doi.org/10.3390/audiolres11030043
Chicago/Turabian StyleGenovese, Elisabetta, Silvia Palma, Valeria Polizzi, Giovanni Bianchin, Michela Cappai, Shaniko Kaleci, Alessandro Martini, Andrea Ciorba, and Paolo Stagi. 2021. "Genetic and Non Genetic Hearing Loss and Associated Disabilities: An Epidemiological Survey in Emilia-Romagna Region" Audiology Research 11, no. 3: 463-473. https://doi.org/10.3390/audiolres11030043
APA StyleGenovese, E., Palma, S., Polizzi, V., Bianchin, G., Cappai, M., Kaleci, S., Martini, A., Ciorba, A., & Stagi, P. (2021). Genetic and Non Genetic Hearing Loss and Associated Disabilities: An Epidemiological Survey in Emilia-Romagna Region. Audiology Research, 11(3), 463-473. https://doi.org/10.3390/audiolres11030043