
Optimization of the Speech Test Material in a Group of Hearing Impaired Subjects: A Feasibility Study for Multilingual Digit Triplet Test Development


Abstract
1. Introduction
2. Materials and Methods
2.1. Speech Material
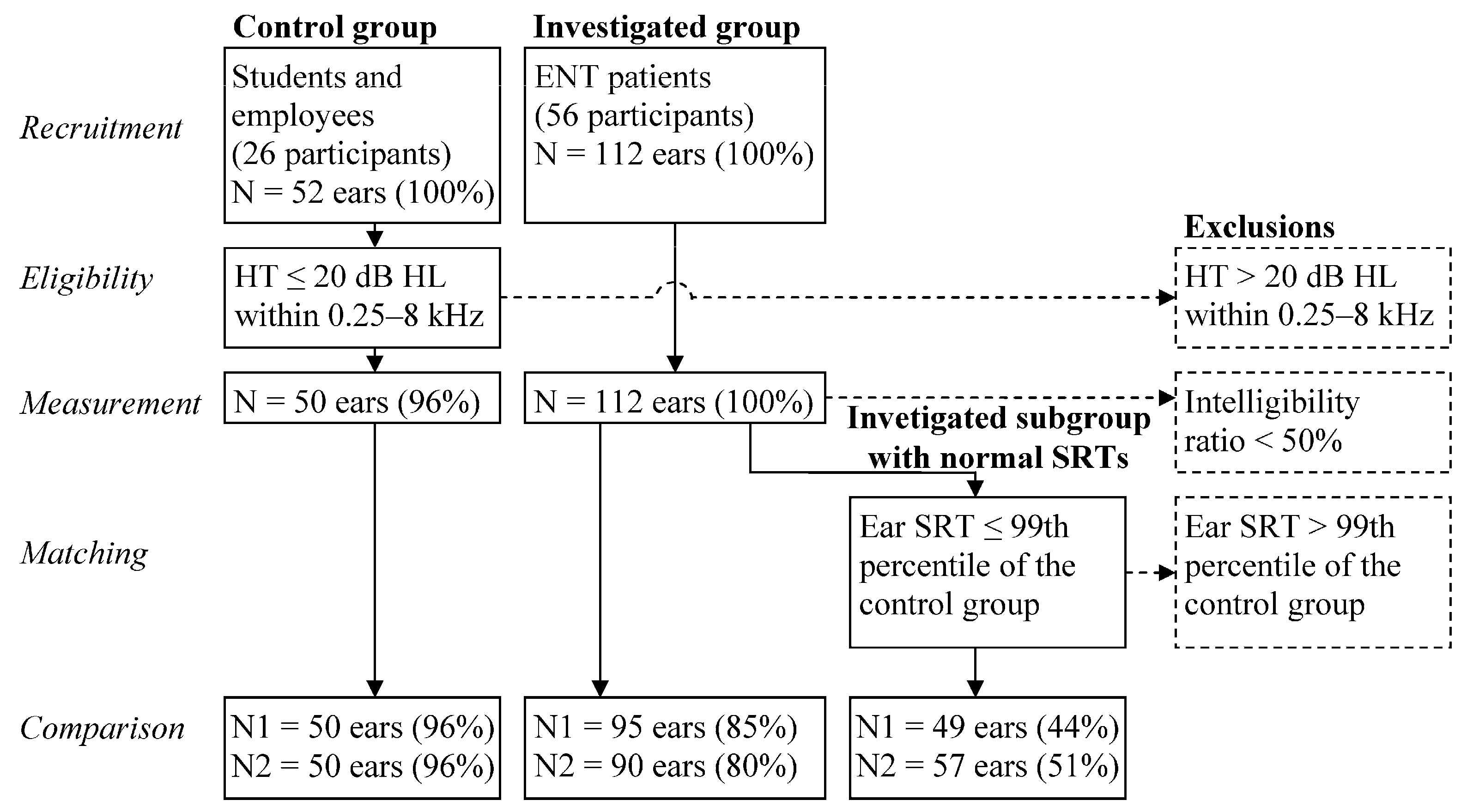
2.2. Measurement
2.3. Statistical Analysis
2.4. Adjusted and Additional Analysis
3. Results
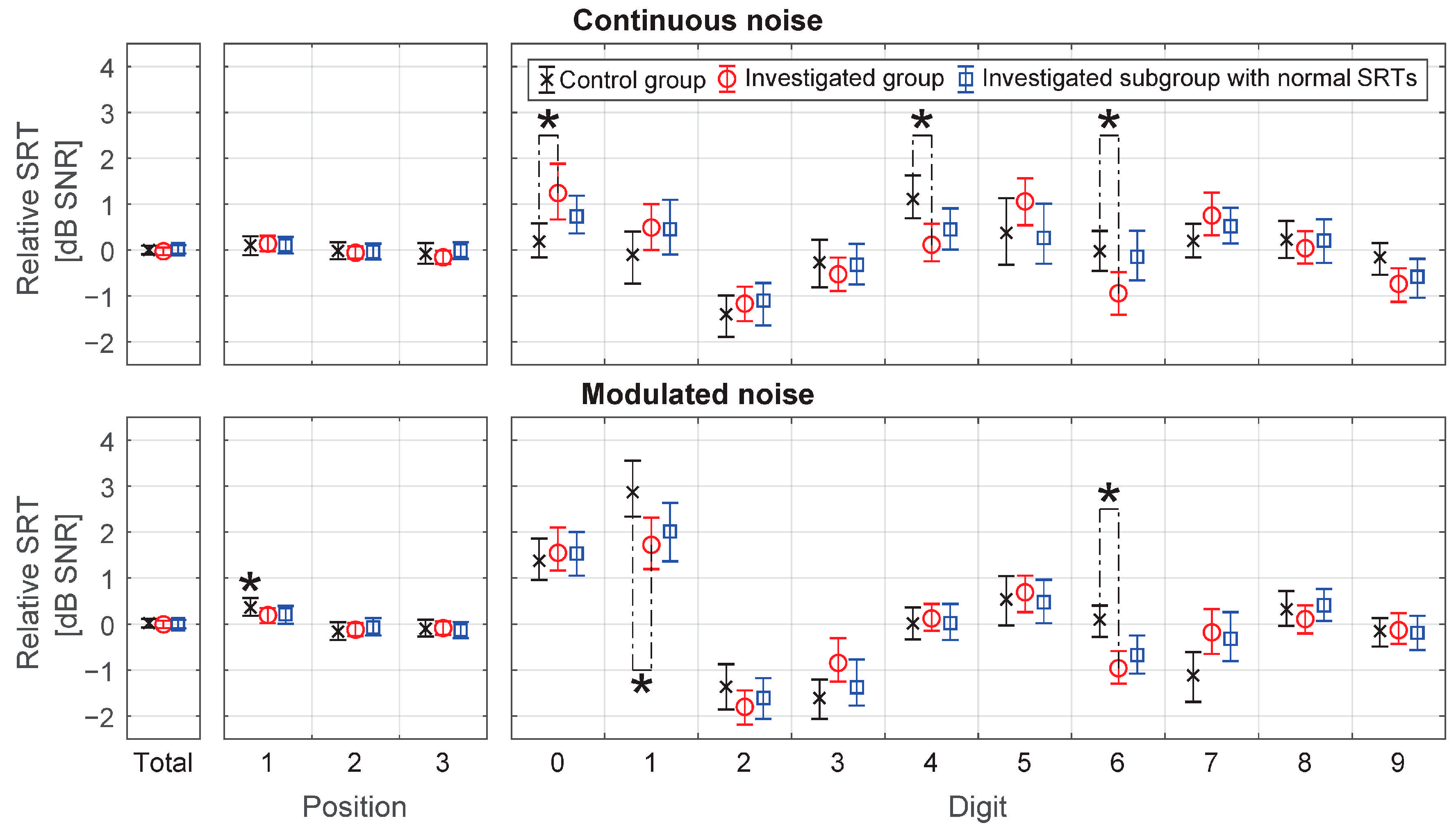
3.1. Speech Reception Threshold
3.2. Adjusted Analysis
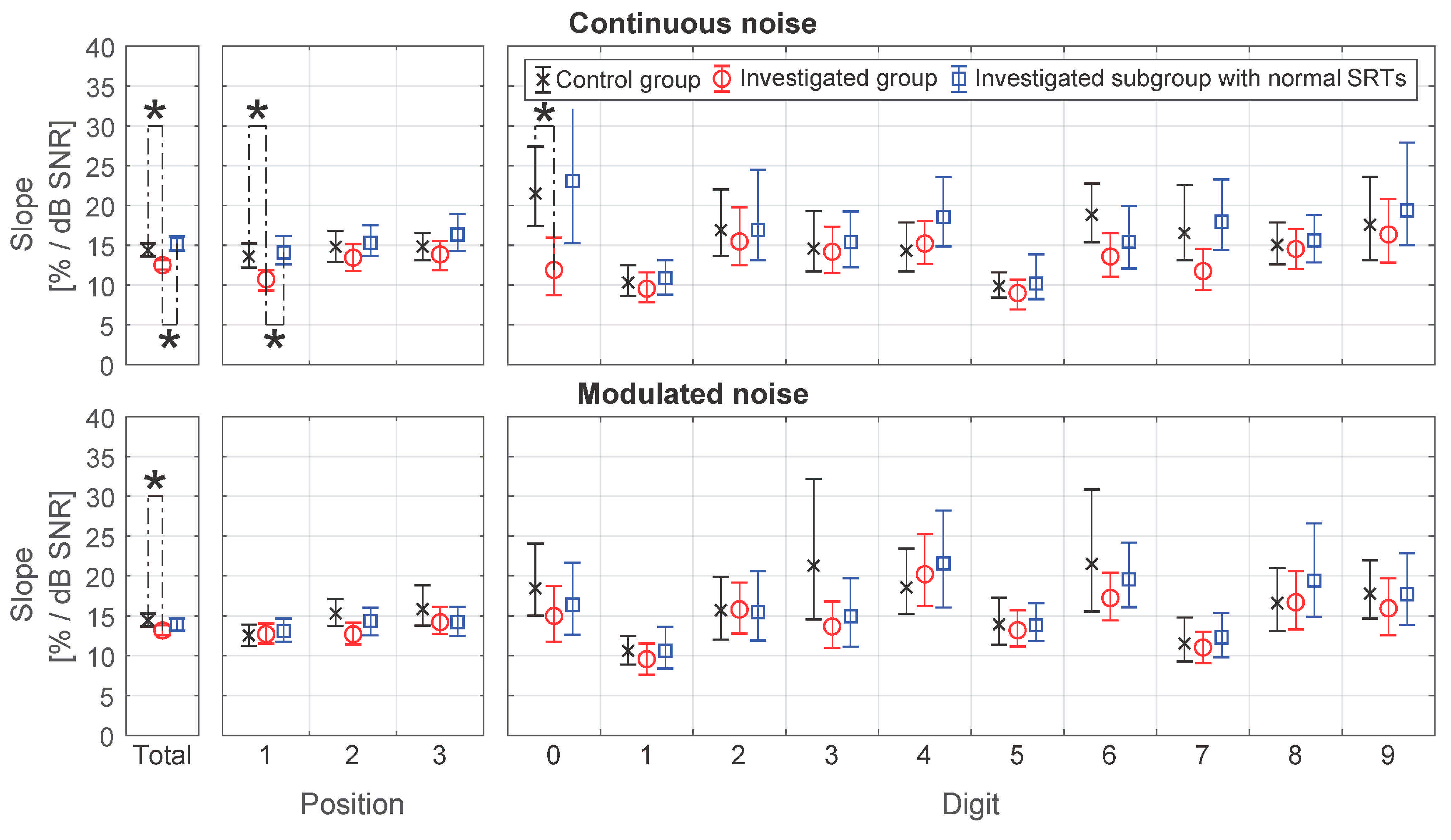
3.3. Additional Analysis. The Slope
4. Discussion
4.1. Principal Results
4.2. Comparison with Prior Work
4.3. Limitations
4.4. Generalization
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Control Group | Investigated Group | Investigated Subgroup with Normal Srts |
|---|---|---|---|
| Continuous noise | |||
| N (ears) | 50 | 95 | 49 |
| SRT (dB SNR), CI (95%), p-value 1 | |||
| Position 1 | 0.10 (−0.11, 0.30) | 0.14 (−0.03, 0.31), 0.83 | 0.11 (−0.07, 0.28), 0.99 |
| Position 2 | −0.02 (−0.20, 0.17) | −0.06 (−0.19, 0.08), 0.78 | −0.04 (−0.21, 0.14), 0.90 |
| Position 3 | −0.08 (−0.30, 0.15) | −0.16 (−0.30,−0.01), 0.63 | −0.01 (−0.19, 0.17), 0.71 |
| Digit 0 | 0.19 (−0.16, 0.58) | 1.24 (0.67, 1.88), 0.04 * | 0.74 (0.36, 1.19), 0.17 |
| Digit 1 | −0.10 (−0.73, 0.40) | 0.49 (−0.00, 1.00), 0.25 | 0.46 (−0.10, 1.09), 0.31 |
| Digit 2 | −1.40 (−1.80,−0.99) | −1.17 (−1.55,−0.80), 0.57 | −1.10 (−1.64, −0.72), 0.55 |
| Digit 3 | −0.27 (−0.81, 0.23) | −0.53 (−0.89,−0.17), 0.59 | −0.32 (−0.75, 0.14), 0.92 |
| Digit 4 | 1.11 (0.69, 1.63) | 0.11 (−0.24, 0.57), 0.03 * | 0.45 (0.01, 0.91), 0.15 |
| Digit 5 | 0.37 (−0.32, 1.13) | 1.06 (0.54, 1.56), 0.31 | 0.26 (−0.30, 1.01), 0.88 |
| Digit 6 | −0.03 (−0.45, 0.41) | −0.94 (−1.41, −0.48), 0.05 * | −0.15 (−0.66, 0.42), 0.82 |
| Digit 7 | 0.20 (−0.16, 0.57) | 0.75 (0.32, 1.25), 0.18 | 0.52 (0.14, 0.92), 0.41 |
| Digit 8 | 0.23 (−0.18, 0.64) | 0.04 (−0.30, 0.41), 0.64 | 0.21 (−0.28, 0.67), 0.96 |
| Digit 9 | −0.16 (−0.54, 0.15) | −0.74 (−1.13, −0.40), 0.12 | −0.58 (−1.04, −0.19), 0.29 |
| Total 2 | 0.00 (−0.09, 0.09) | −0.03 (−0.11, 0.06), 0.65 | 0.02 (−0.07, 0.11), 0.79 |
| Modulated noise | |||
| N (ears) | 50 | 90 | 57 |
| SRT (dB SNR), CI (95%), p-value 1 | |||
| Position 1 | 0.36 (0.18, 0.56) | 0.20 (0.02, 0.35), 0.26 | 0.21 (0.01, 0.40), 0.36 |
| Position 2 | −0.16 (−0.35, 0.04) | −0.12 (−0.26, 0.03), 0.80 | −0.07 (−0.25, 0.13), 0.60 |
| Position 3 | −0.10 (−0.27, 0.10) | −0.09 (−0.23, 0.06), 0.94 | −0.13 (−0.30, 0.05), 0.83 |
| Digit 0 | 1.37 (0.95, 1.86) | 1.55 (1.16, 2.10), 0.70 | 1.53 (1.05, 2.00), 0.75 |
| Digit 1 | 2.87 (2.34, 3.56) | 1.72 (1.19, 2.31), 0.05 * | 2.01 (1.36, 2.64), 0.15 |
| Digit 2 | −1.36 (−1.86, −0.87) | −1.80 (−2.19, −1.44), 0.33 | −1.61 (−2.06, −1.18), 0.61 |
| Digit 3 | −1.61 (−2.07, −1.21) | −0.84 (−1.25, −0.31), 0.07 | −1.37 (−1.78, −0.77), 0.57 |
| Digit 4 | 0.02 (−0.33, 0.37) | 0.13 (−0.15, 0.44), 0.74 | 0.02 (−0.34, 0.44), 0.99 |
| Digit 5 | 0.54 (−0.03, 1.04) | 0.69 (0.26, 1.05), 0.75 | 0.48 ( 0.02, 0.96), 0.91 |
| Digit 6 | 0.10 (−0.28, 0.40) | −0.96 (−1.30, −0.58), 0.01 * | −0.67 (−1.08, −0.25), 0.06 |
| Digit 7 | −1.12 (−1.69, −0.60) | −0.18 (−0.65, 0.33), 0.06 | −0.32 (−0.81, 0.26), 0.12 |
| Digit 8 | 0.32 (−0.04, 0.72) | 0.11 (−0.20, 0.41), 0.53 | 0.41 ( 0.07, 0.76), 0.82 |
| Digit 9 | −0.15 (−0.48, 0.13) | −0.13 (−0.43, 0.24), 0.95 | −0.19 (−0.56, 0.18), 0.82 |
| Total 2 | 0.02 (−0.07, 0.11) | −0.00 (−0.08, 0.07), 0.68 | 0.00 (−0.09, 0.09), 0.75 |
Appendix B
| Characteristic | Control Group | Investigated Group | Investigated Subgroup with Normal Srts |
|---|---|---|---|
| Continuous noise | |||
| N (ears) | 50 | 95 | 49 |
| Slope (%/dB), CI (95%), p-value 1 | |||
| Position 1 | 13.61 (12.19, 15.24) | 10.73 (9.32, 11.88), 0.01 * | 14.09 (12.61, 16.17), 0.73 |
| Position 2 | 14.82 (12.89, 16.83) | 13.44 (11.75, 15.17), 0.39 | 15.30 (13.63, 17.53), 0.77 |
| Position 3 | 14.83 (13.14, 16.56) | 13.85 (11.89, 15.54), 0.51 | 16.34 (14.28, 18.94), 0.37 |
| Digit 0 | 21.50 (17.40, 27.40) | 11.90 (8.73, 15.69), 0.02 * | 23.08 (15.27, 32.17), 0.83 |
| Digit 1 | 10.33 (8.64, 12.48) | 9.55 (7.84, 11.59), 0.69 | 10.87 (8.78, 13.13), 0.81 |
| Digit 2 | 16.90 (13.67, 22.01) | 15.48 (12.49, 19.78), 0.72 | 16.92 (13.13, 24.49), 0.99 |
| Digit 3 | 14.60 (11.74, 19.28) | 14.19 (11.47, 17.35), 0.89 | 15.40 (12.24, 19.24), 0.85 |
| Digit 4 | 14.33 (11.74, 17.87) | 15.22 (12.66, 18.04), 0.78 | 18.56 (14.85, 23.56), 0.26 |
| Digit 5 | 9.87 (8.41, 11.60) | 9.00 (6.92, 10.69), 0.59 | 10.19 (8.24, 13.86), 0.87 |
| Digit 6 | 18.84 (15.39, 22.76) | 13.59 (11.04, 16.53), 0.11 | 15.45 (12.08, 19.95), 0.41 |
| Digit 7 | 16.54 (13.12, 22.60) | 11.76 (9.40, 14.58), 0.14 | 17.96 (14.41, 23.27), 0.78 |
| Digit 8 | 15.04 (12.59, 17.87) | 14.54 (12.01, 17.04), 0.84 | 15.62 (12.84, 18.82), 0.84 |
| Digit 9 | 17.57 (13.15, 23.63) | 16.37 (12.80, 20.81), 0.79 | 19.38 (15.03, 27.9), 0.74 |
| Total | 14.36 (13.59, 15.23) | 12.50 (11.96, 13.09), <0.001 * | 15.17 2 (14.33, 16.11), 0.19 |
| Modulated noise | |||
| N (ears) | 50 | 90 | 57 |
| Slope (%/dB), CI (95%), p-value 1 | |||
| Position 1 | 12.55 (11.27, 13.91) | 12.73 (11.53, 14.06), 0.88 | 13.11 (11.78, 14.66), 0.64 |
| Position 2 | 15.33 (13.75, 17.10) | 12.71 (11.41, 14.16), 0.05 | 14.37 (12.56, 16.03), 0.50 |
| Position 3 | 15.85 (13.78, 18.82) | 14.22 (12.77, 15.15), 0.36 | 14.21 (12.47, 16.12), 0.35 |
| Digit 0 | 18.44 (15.05, 24.06) | 14.99 (11.76, 18.76), 0.35 | 16.36 (12.62, 21.62), 0.65 |
| Digit 1 | 10.61 (8.90, 12.47) | 9.58 (7.62, 11.54), 0.59 | 10.62 (8.41, 13.64), 0.99 |
| Digit 2 | 15.72 (12.02, 19.89) | 15.80 (12.81, 19.15), 0.98 | 15.48 (11.93, 20.62), 0.96 |
| Digit 3 | 21.27 (14.57, 32.20) | 13.68 (10.99, 16.76), 0.16 | 14.97 (11.13, 19.72), 0.29 |
| Digit 4 | 18.54 (15.28, 23.40) | 20.21 (16.22, 25.25), 0.72 | 21.56 (16.07, 28.19), 0.57 |
| Digit 5 | 13.93 (11.37, 17.26) | 13.20 (11.16, 15.72), 0.78 | 13.81 (11.82, 16.57), 0.97 |
| Digit 6 | 21.50 (15.57, 30.85) | 17.24 (14.45, 20.38), 0.38 | 19.55 (16.12, 24.19), 0.72 |
| Digit 7 | 11.55 (9.31, 14.79) | 11.03 (9.04, 13.00), 0.81 | 12.31 (9.81, 15.36), 0.80 |
| Digit 8 | 16.60 (13.09, 21.01) | 16.70 (13.31, 20.59), 0.98 | 19.41 (14.86, 26.60), 0.54 |
| Digit 9 | 17.76 (14.69, 21.95) | 15.95 (12.58, 19.68), 0.61 | 17.70 (13.87, 22.84), 0.99 |
| Total | 14.44 (13.66, 15.31) | 13.18(12.61, 13.81), 0.01 * | 13.87 (13.16, 14.66), 0.31 |
References
- Mathers, C.D.; Smith, A.; Concha, M. Global Burden of Hearing Loss in the Year 2000; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Arlinger, S. Negative consequences of uncorrected hearing loss—A review. Int. J. Audiol. 2003, 42, 2S17–2S20. [Google Scholar] [CrossRef]
- Heine, C.; Browning, C.J. Communication and psychosocial consequences of sensory loss in older adults: Overview and rehabilitation directions. Disabil. Rehabil. 2002, 24, 763–773. [Google Scholar] [CrossRef]
- World Health Organization. Addressing the Rising Prevalence of Hearing Loss; World Health Organization: Geneva, Switzerland, 2018; ISBN 9789241550260. [Google Scholar]
- Wilson, B.S.; Tucci, D.L.; Merson, M.H.; O’Donoghue, G.M. Global hearing health care: New findings and perspectives. Lancet 2017, 390, 2503–2515. [Google Scholar] [CrossRef]
- Stevens, G.; Flaxman, S.; Brunskill, E.; Mascarenhas, M.; Mathers, C.D.; Finucane, M. Global and regional hearing impairment prevalence: An analysis of 42 studies in 29 countries. Eur. J. Public Health 2011, 23, 146–152. [Google Scholar] [CrossRef]
- Vos, T.; Allen, C.; Arora, M.; Barber, R.M.; Bhutta, Z.A.; Brown, A.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: A systematic analysis for the Global Burden of Disease Study. Lancet 2016, 388, 1545–1602. [Google Scholar] [CrossRef]
- Masalski, M.; Morawski, K. Worldwide Prevalence of Hearing Loss Among Smartphone Users: Cross-Sectional Study Using a Mobile-Based App. J. Med. Internet Res. 2020, 22, e17238. [Google Scholar] [CrossRef] [PubMed]
- Olusanya, B.O.; Neumann, K.J.; Saunders, J.E. The global burden of disabling hearing impairment: A call to action. Bull. World Health Organ. 2014, 92, 367–373. [Google Scholar] [CrossRef] [PubMed]
- Szudek, J.; Ostevik, A.; Dziegielewski, P.; Robinson-Anagor, J.; Gomaa, N.; Hodgetts, B.; Ho, A. Can Uhear me now? Validation of an iPod-based hearing loss screening test. J. Otolaryngol. Head Neck Surg. 2012, 41, S78–S84. [Google Scholar] [PubMed]
- Kam, A.C.S.; Sung, J.K.K.; Lee, T.; Wong, T.K.C.; Van Hasselt, A. Clinical evaluation of a computerized self-administered hearing test. Int. J. Audiol. 2012, 51, 606–610. [Google Scholar] [CrossRef]
- Foulad, A.; Bui, P.; Djalilian, H. Automated audiometry using apple iOS-based application technology. Otolaryngol. Head Neck Surg. 2013, 149, 700–706. [Google Scholar] [CrossRef]
- De Swanepoel, W.; Myburgh, H.C.; Howe, D.M.; Mahomed, F.; Eikelboom, R.H. Smartphone hearing screening with integrated quality control and data management. Int. J. Audiol. 2014, 53, 841–849. [Google Scholar] [CrossRef] [PubMed]
- Yeung, J.C.; Heley, S.; Beauregard, Y.; Champagne, S.; Bromwich, M.A. Self-administered hearing loss screening using an interactive, tablet play audiometer with ear bud headphones. Int. J. Pediatr. Otorhinolaryngol. 2015, 79, 1248–1252. [Google Scholar] [CrossRef] [PubMed]
- Larrosa, F.; Rama-Lopez, J.; Benitez, J.; Morales, J.M.; Martinez, A.; Alañon, M.A.; Arancibia-Tagle, D.; Batuecas-Caletrío, Á.; Martinez-Lopez, M.; Pérez-Fernández, N.; et al. Development and evaluation of an audiology app for iPhone/iPad mobile devices. Acta Oto-Laryngol. 2015, 135, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Renda, L.; Selcuk, O.T.; Eyigor, H.; Osma, U.; Yilmaz, M.D. Smartphone Based Audiometric Test for Confirming the Level of Hearing; Is It Useable in Underserved Areas? J. Int. Adv. Otol. 2016, 12, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Sandström, J.; Swanepoel, D.W.; Myburgh, H.C.; Laurent, C. Smartphone threshold audiometry in underserved primary health-care contexts. Int. J. Audiol. 2016, 55, 232–238. [Google Scholar] [CrossRef]
- Masalski, M.; Grysiński, T.; Kręcicki, T. Hearing Tests Based on Biologically Calibrated Mobile Devices: Comparison with Pure-Tone Audiometry. JMIR mHealth uHealth 2018, 6, e10. [Google Scholar] [CrossRef]
- Masalski, M.; Kręcicki, T.; Eriksson, M. Self-Test Web-Based Pure-Tone Audiometry: Validity Evaluation and Measurement Error Analysis. J. Med. Internet Res. 2013, 15, e71. [Google Scholar] [CrossRef]
- Yousuf, H.S.; Wet, S.D.; Biagio, J.L.; Myburgh, H.C.; Eikelboom, R.H.; Hugo, J. Smartphone hearing screening in mHealth assisted community-based primary care. J. Telemed. Telecare 2016, 22, 405–412. [Google Scholar] [CrossRef]
- Chu, Y.-C.; Cheng, Y.-F.; Lai, Y.-H.; Tsao, Y.; Tu, T.-Y.; Young, S.T.; Chen, T.-S.; Chung, Y.-F.; Lai, F.; Liao, W.-H. A Mobile Phone–Based Approach for Hearing Screening of School-Age Children: Cross-Sectional Validation Study. JMIR mHealth uHealth 2019, 7, e12033. [Google Scholar] [CrossRef] [PubMed]
- Sandström, J.; Swanepoel, D.; Laurent, C.; Umefjord, G.; Lundberg, T. Accuracy and Reliability of Smartphone Self-Test Audiometry in Community Clinics in Low Income Settings: A Comparative Study. Ann. Otol. Rhinol. Laryngol. 2020, 129, 578–584. [Google Scholar] [CrossRef]
- Zokoll, M.A.; Wagener, K.C.; Brand, T.; Buschermöhle, M.; Kollmeier, B. Internationally comparable screening tests for listening in noise in several European languages: The German digit triplet test as an optimization prototype. Int. J. Audiol. 2012, 51, 697–707. [Google Scholar] [CrossRef] [PubMed]
- Potgieter, J.M.; Swanepoel, D.W.; Myburgh, H.C.; Hopper, T.C.; Smits, C. Development and validation of a smartphone-based dig-its-in-noise hearing test in South African English. Int. J. Audiol. 2016, 55, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Song, T.; Song, M.; Wu, X.; Chen, J. An iOS-based speech audiometry for self-assessment of hearing status. In Proceedings of the 1st International Conference on Challenges in Hearing Assistive Technology (CHAT-17), Stockholm, Sweden, 19 August 2017; ISBN 978-1-5272-1357-9. [Google Scholar]
- Yimtae, K.; Israsena, P.; Thanawirattananit, P.; Seesutas, S.; Saibua, S.; Kasemsiri, P.; Noymai, A.; Soonrach, T. A Tablet-Based Mobile Hearing Screening System for Preschoolers: Design and Validation Study. JMIR mHealth uHealth 2018, 6, e186. [Google Scholar] [CrossRef] [PubMed]
- Vlaming, M.S.M.G.; Kollmeier, B.; Dreschler, W.A.; Martin, R.; Wouters, J.; Grover, B.; Mohammadh, Y.; Houtgast, T. HearCom: Hearing in the Communication Society. Acta Acust. United Acust. 2011, 97, 175–192. [Google Scholar] [CrossRef]
- Akeroyd, M.A.; Arlinger, S.; Bentler, R.A.; Boothroyd, A.; Dillier, N.; Dreschler, W.A.; Gagné, J.-P.; Lutman, M.; Wouters, J.; Wong, L.; et al. International Collegium of Rehabilitative Audiology (ICRA) recommendations for the construction of multilingual speech tests. Int. J. Audiol. 2015, 54, 1–6. [Google Scholar] [CrossRef]
- Smits, C. Comment on ‘International collegium of rehabilitative audiology (ICRA) recommendations for the construction of multilingual speech tests’, by Akeroyd et al. Int. J. Audiol. 2016, 55, 268–269. [Google Scholar] [CrossRef]
- Smits, C.; Kapteyn, T.S.; Houtgast, T. Development and validation of an automatic speech-in-noise screening test by telephone. Int. J. Audiol. 2004, 43, 15–28. [Google Scholar] [CrossRef] [PubMed]
- Smits, C.; Merkus, P.; Houtgast, T. How we do it: The Dutch functional hearing-screening tests by telephone and internet. Clin. Otolaryngol. 2006, 31, 436–440. [Google Scholar] [CrossRef]
- Ozimek, E.; Kutzner, D.; Sęk, A.; Wicher, A. Development and evaluation of Polish digit triplet test for auditory screening. Speech Commun. 2009, 51, 307–316. [Google Scholar] [CrossRef]
- Wagener, K.; Eeenboom, F.; Brand, T.; Kollmeier, B. Ziffern-Tripel-Test: Sprachverständlichkeitstest über das Telefon; DGA 8. Jahrestag: Göttingen, Germany, 2005; ISBN 3-9809869-4-2. [Google Scholar]
- Rudmin, F.; Rudmin, F. Speech reception thresholds for digits. J. Audit. Res. 1987, 27, 15–21. [Google Scholar]
- Giguère, C.; Lagacé, J.; Ellaham, N.N.; Pichora-Fuller, M.K.; Goy, H.; Bégin, C.; Alary, É.; Bowman, R. Development of the Canadian Digit Triplet Test in English and French. J. Acoust. Soc. Am. 2020, 147, EL252–EL258. [Google Scholar] [CrossRef]
- Elberling, C.; Ludvigsen, C.; Lyregaard, P.E. Dantale: A New Danish Speech Material. Scand. Audiol. 1989, 18, 169–175. [Google Scholar] [CrossRef]
- Ramkissoon, I.; Proctor, A.; Lansing, C.R.; Bilger, R.C. Digit Speech Recognition Thresholds (SRT) for Non-Native Speakers of English. Am. J. Audiol. 2002, 11, 23–28. [Google Scholar] [CrossRef]
- Wilson, R.H.; Weakley, D.G. The Use of Digit Triplets to Evaluate Word-Recognition Abilities in Multitalker Babble. Semin. Hear. 2004, 25, 93–111. [Google Scholar] [CrossRef]
- Eenboom, F. Der Ziffern-Tripel-Test. Entwicklung und Optimierung eines Sprachverständlichkeitstests über das Telefon. Bachelor’s Thesis, Universität Oldenburg, Oldenburg, Germany, 2004. [Google Scholar]
- Bräcker, T. Evaluation des Deutschen Ziffern-Tripel-Tests. Diploma Thesis, Universität Oldenburg, Oldenburg, Germany, 2005. [Google Scholar]
- Wagener, K.; Bräcker, T.; Brand, T.; Kollmeier, B. Evaluation des Ziffern-Tripel-Test über Kopfhörer und Telefon; DGA 9. Jahrestag: Köln, Germany, 2006; ISBN 3-9809869-5-0. [Google Scholar]
- Hall, S. The Development of a New English Sentence in Noise Test and an English Number Recognition Test. MSc Thesis, University of Southampton, Southampton, UK, 2006. [Google Scholar]
- Phipps, H.L. Assessment of Telephone Bandwidth on the English Number Recognition in Noise Test. MSc Thesis, University of Southampton, Southampton, UK, 2007. [Google Scholar]
- Jansen, S.; Luts, H.; Wagener, K.C.; Frachet, B.; Wouters, J. The French digit triplet test: A hearing screening tool for speech intelligibility in noise. Int. J. Audiol. 2010, 49, 378–387. [Google Scholar] [CrossRef]
- King, S.M. Development and Evaluation of a New Zealand Digit Triplet Test for Auditory Screening. Master’s Thesis, University of Canterbury, Christchurch, New Zeeland, 2010. [Google Scholar]
- Willberg, T.; Buschermöhle, M.; Sivonen, V.; Aarnisalo, A.A.; Löppönen, H.; Kollmeier, B.; Dietz, A. The development and evaluation of the Finnish digit triplet test. Acta Oto-Laryngol. 2016, 136, 1035–1040. [Google Scholar] [CrossRef]
- Warzybok, A.; Zokoll, M.A.; Kollmeier, B. Development and Evaluation of the Russian Digit Triplet Test. Acta Acust. United Acust. 2016, 102, 714–724. [Google Scholar] [CrossRef]
- Jamaluddin, S.A. Development and Evaluation of the Digit Triplet and Auditory-Visual Matrix Sentence Tests in Malay. Ph.D. Thesis, University of Canterbury, Christchurch, New Zeeland, 2016. [Google Scholar]
- Ebrahimi, A.; Mahdavi, M.E.; Jalilvand, H. Auditory recognition of Persian digits in presence of speech-spectrum noise and multi-talker babble: A validation study. Audit. Vestib. Res. 2020. [Google Scholar] [CrossRef]
- Han, J.-H.; Yi, D.-W.; Lee, J.; Chang, W.-D.; Lee, H.-J. Development of a Smartphone-Based Digits-in-Noise Test in Korean: A Hearing Screening Tool for Speech Perception in Noise. J. Korean Med. Sci. 2020, 35, e163. [Google Scholar] [CrossRef]
- Hagerman, B. Efficiency of speech audiometry and other tests. Br. J. Audiol. 1993, 27, 423–425. [Google Scholar] [CrossRef]
- Smits, C.; Houtgast, T. Recognition of digits in different types of noise by normal-hearing and hearing-impaired listeners. Int. J. Audiol. 2007, 46, 134–144. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.H.; Burks, C.A.; Weakley, D.G. Word Recognition of Digit Triplets and Monosyllabic Words in Multitalker Babble by Listeners with Sensorineural Hearing Loss. J. Am. Acad. Audiol. 2006, 17, 385–397. [Google Scholar] [CrossRef]
- Smits, C.; Houtgast, T. Measurements and calculations on the simple up-down adaptive procedure for speech-in-noise tests. J. Acoust. Soc. Am. 2006, 120, 1608–1621. [Google Scholar] [CrossRef]
- Kollmeier, B. Messmethodik, Modellierung und Verbesserung der Verständlichkeit von Sprache; Habilitation, Universität Göttingen: Göttingen, Germany, 1990. [Google Scholar]
- Versfeld, N.J.; Daalder, L.; Festen, J.M.; Houtgast, T. Method for the selection of sentence materials for efficient measurement of the speech reception threshold. J. Acoust. Soc. Am. 2000, 107, 1671–1684. [Google Scholar] [CrossRef]
- British Society of Audiology. Recommended Procedure. Pure-Tone Air-Conduction and Bone-Conduction Threshold Audiometry with and Without Masking; British Society of Audiology: Berkshire, UK, 2011. [Google Scholar]
- Doyle, J.; Wong, L.L. Mismatch between aspects of hearing impairment and hearing disability/handicap in adult/elderly Cantonese speakers: Some hypotheses concerning cultural and linguistic influences. J. Am. Acad. Audiol. 1996, 7, 442–446. [Google Scholar]
- Chen, F.; Wong, L.L.N.; Hu, Y. Effects of Lexical Tone Contour on Mandarin Sentence Intelligibility. J. Speech Lang. Hear. Res. 2014, 57, 338–345. [Google Scholar] [CrossRef]
- Hu, H.; Xi, X.; Wong, L.L.N.; Hochmuth, S.; Warzybok, A.; Kollmeier, B. Construction and evaluation of the Mandarin Chinese matrix (CMNmatrix) sentence test for the assessment of speech recognition in noise. Int. J. Audiol. 2018, 57, 838–850. [Google Scholar] [CrossRef] [PubMed]
- Lyzenga, J.; Smits, C. Effects of Coarticulation, Prosody, and Noise Freshness on the Intelligibility of Digit Triplets in Noise. J. Am. Acad. Audiol. 2011, 22, 215–221. [Google Scholar] [CrossRef] [PubMed]







| Characteristic | Control Group | Investigated Group |
|---|---|---|
| Number of participants | 26 | 56 |
| Age (years), range (median) | 18–36 (26.5) | 21–71(40) |
| Gender (male), n (%) | 12 (48%) | 13 (52%) |
| Number of ears | 50 | 112 |
| Hearing threshold 1 (dB HL), mean (SD) | 6.3 (6.0) | 30.0 (24.7) |
| Study Group | N | Hearing Loss Type 1 | |||
|---|---|---|---|---|---|
| Normal Hearing | Sensorineural | Conductive | Mixed | ||
| Control group | 50 | 50 (100%) | 0 | 0 | 0 |
| Investigated group | 95 | 34 (36%) | 29 (31%) | 4 (4%) | 28 (29%) |
| Investigated group with normal SRTs | |||||
| Continuous noise | 49 | 30 (61%) | 12 (31%) | 1 (2%) | 7 (12%) |
| Modulated noise | 57 | 33 (58%) | 13 (58%) | 2 (4%) | 8 (14%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Masalski, M.; Adamczyk, M.; Morawski, K. Optimization of the Speech Test Material in a Group of Hearing Impaired Subjects: A Feasibility Study for Multilingual Digit Triplet Test Development. Audiol. Res. 2021, 11, 342-356. https://doi.org/10.3390/audiolres11030032
Masalski M, Adamczyk M, Morawski K. Optimization of the Speech Test Material in a Group of Hearing Impaired Subjects: A Feasibility Study for Multilingual Digit Triplet Test Development. Audiology Research. 2021; 11(3):342-356. https://doi.org/10.3390/audiolres11030032
Chicago/Turabian StyleMasalski, Marcin, Martyna Adamczyk, and Krzysztof Morawski. 2021. "Optimization of the Speech Test Material in a Group of Hearing Impaired Subjects: A Feasibility Study for Multilingual Digit Triplet Test Development" Audiology Research 11, no. 3: 342-356. https://doi.org/10.3390/audiolres11030032
APA StyleMasalski, M., Adamczyk, M., & Morawski, K. (2021). Optimization of the Speech Test Material in a Group of Hearing Impaired Subjects: A Feasibility Study for Multilingual Digit Triplet Test Development. Audiology Research, 11(3), 342-356. https://doi.org/10.3390/audiolres11030032