1. Introduction
Sacral fractures are often associated with high-energy mechanisms of injury [
1]. The incidence of non-osteoporotic sacral fractures in 2011 has been shown to be triple what it was in 2002, reaching a rate of 2.1 per 100,000 people [
2]. This increase in the incidence of sacral fractures can be explained by the increased use of computed tomography (CT) imaging in trauma patients in recent years, which has allowed for greater identification of this underdiagnosed fracture type [
3]. The increase in diagnosis with CT imaging may be explained by plain radiographs often missing these fractures due to poor patient positioning, large body habitus obscuring images, the irregularly contoured nature of the sacrum, or small nondisplaced fractures. As trauma protocols in hospitals are more widely using CT to assess abdominal and pelvic anatomy, the increase in fracture identification is expected with enhanced imaging.
Treatment options for sacral fractures vary depending on the morphology and stability of the fracture. Nonoperative management can be used in cases of stable, nondisplaced sacral fractures, while displaced fractures that are irreducible by closed maneuvers require open reduction and internal fixation (ORIF) [
1]. Surgical techniques for sacral fractures include percutaneous iliosacral screws, sacral plate fixation, and techniques such as triangular osteosynthesis which uses a combination of lumbopelvic distraction and transverse fracture fixation, thus allowing for multiplane stability [
4].
Sacral fractures, and their subsequent treatments, can cause a myriad of complications. Most notably, due to the sacrum’s anatomical relationship to the lumbosacral plexus, neurological injuries are common, presenting in over 50% of cases [
5]. Consequences of neurologic injuries can present in a variety of patterns depending on specific nerve involvement but can all lead to deficiencies in lower extremity motor and sensation. Individual nerve involvement can lead to long-term problems with hip and thigh extension, knee flexion and extension, foot drop, and more. Perioperative complications have also been reported, including implant malpositioning, neurologic insult, blood loss, superior gluteal artery injury, and rarely, ureteral or bowel damage [
2]. Bydon et al. found that complications of sacral fracture surgery occurred in 26% of patients, and included infection, wound issues, and implant irritation or failure [
2]. The independent factors most closely associated with in-hospital complications of sacral fracture surgery are congestive heart failure, coagulopathy, and electrolyte abnormalities [
6]. These in-hospital complications can lead to increased morbidity and mortality, especially in the elderly population. Although operative stabilization can improve pain related to these fractures, post-operative surgical pain may limit patient ambulation in the perioperative period, leading to atelectasis and pneumonia development. This is a case presentation of a patient with a postoperative complication that led to the use of a novel technique in order to achieve fixation of a displaced vertical sheer sacral fracture.
2. Case Report
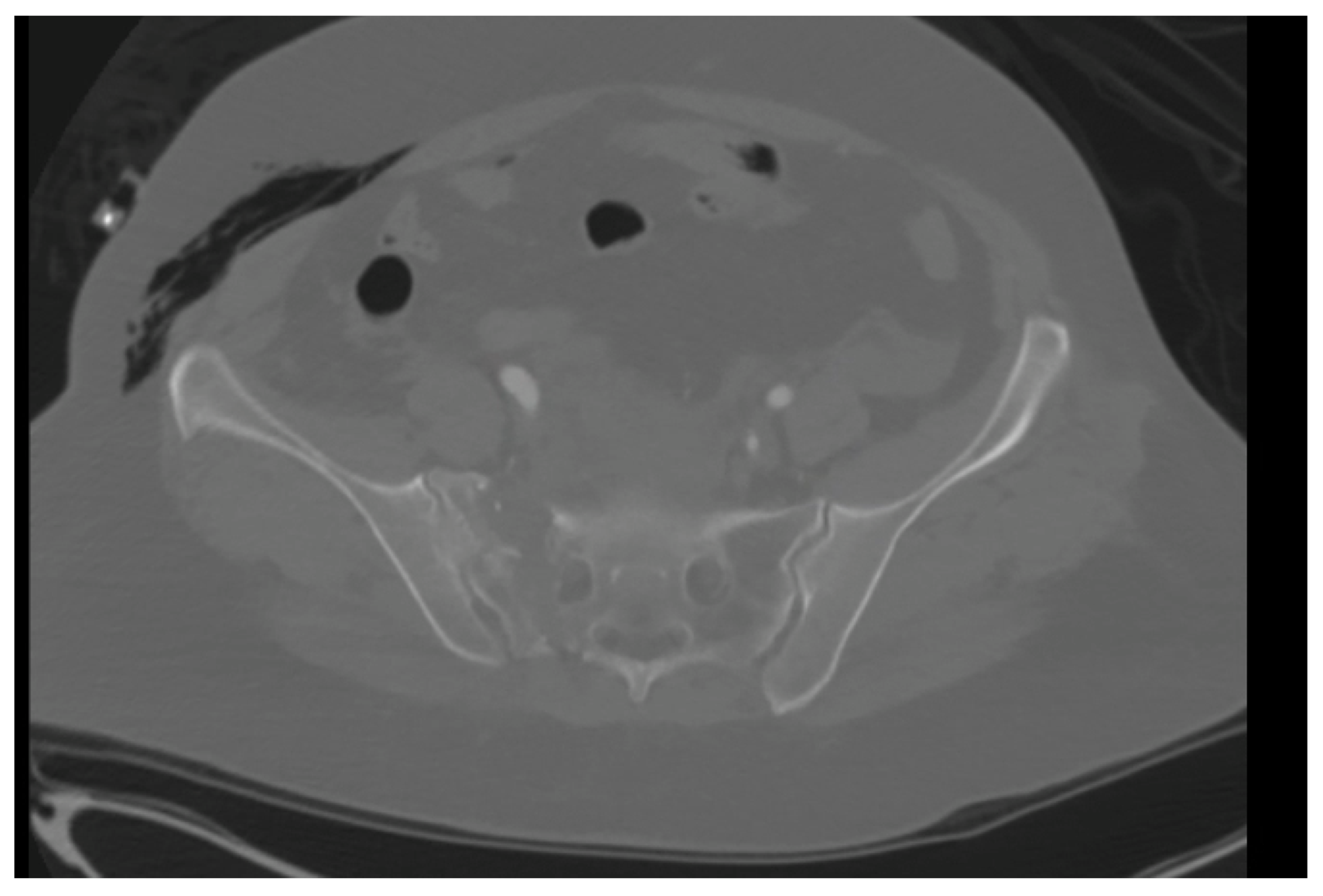
A 59-year-old female with no known past medical history presented to our level 1 trauma center, having been involved in a rollover motor vehicle collision. Plain radiographs and CT imaging demonstrated various orthopedic injuries including a Dennis type 1 vertical shear sacral fracture, bilateral superior and inferior pubic rami fractures (
Figure 1 and
Figure 2), right T5–T6, L1–L5, and left L2–L3 transverse process fractures, spinous process fractures of T7 and T9, and right posterior rib 4–7 fractures. Additional, non-orthopedic injuries included pneumothorax, retroperitoneal hematoma, grade 4 hepatic injury, grade 3 splenic injury, and grade 2 kidney injury. On day 3 of presentation, the patient was stable enough for operative fixation from the orthopedic surgery team.
2.1. Initial Surgery
Prior to surgery, the injury was placed under traction via tension bow. Operative management of the patient’s pelvic ring injuries occurred 4 days after the initial injury. After debridement of necrotic tissue and dissection to the sacral fracture site, it was determined that the posterior sacral nerve roots had been traumatically transected. The fracture site was debrided, and direct visualization confirmed the Dennis I classification with significant anterior comminution. The fracture was reduced and compressed with a DePuy Synthes (Raynham, MA, USA) partially threaded 7.3 mm cannulated screw placed in S1 in a trans-iliac trans-sacral fashion. A fully threaded 7.3 mm cannulated screw was then placed in S2 in a similar fashion. Finally, an identical screw was placed across S1, and the original partially threaded screw was removed.
The patient was then repositioned to a supine position to address the bilateral superior and inferior pubic rami fractures. The anterior pelvis had been partially reduced due to the posterior stabilization in the sacrum. Interim packing from multiple prior abdominal surgeries had rendered external fixation as the most appropriate treatment. Five mm Schanz pins were placed along the LC-2 corridor in typical fashion to create a Hannover frame (
Figure 3). After appropriate positioning was confirmed via fluoroscopy, pins were connected via external fixator bars and clamps. There were no obvious perioperative complications, and the patient was transferred to the post-anesthesia care unit (PACU).
2.2. Post-Op Course 1
The patient was instructed to be non-weight bearing on the right lower extremity and remained in the hospital for the next 34 days until the next surgical procedure. During this time, the patient underwent an esophagogastroduodenoscopy and percutaneous tracheostomy placement. The patient developed E. Coli bacteremia and pneumonia during her hospital course. On POD 15, the posterior surgical incision was noted to have some minor serosanguineous drainage. The right anterior pin site started draining thin yellow fluid on POD 18. The surgical wounds continued to drain over her postoperative course. Finally, a CT scan was obtained, which displayed osseous healing of the pelvis with posterior hardware failure, along with a fluid collection beneath the sacral incision site (
Figure 4). These factors, along with the noted infection, necessitated a revision of the sacral hardware, debridement of the sacral wound, and removal of the external fixator as appropriate.
2.3. Revision Surgery
On POD 34, the patient returned to the operating room for external fixator removal, irrigation and debridement of the sacral wound, and revision of the sacral screws. During removal of the anterior pelvic external fixation device, the left Schanz pin was noted to be quite loose, indicating the external fixator was most likely providing little to no support. There was a 2 mm wound dehiscence at the inferior margin of the prior sacral incision, which had active serous drainage. The wound was opened and meticulously debrided and it was noted that there was no excess warmth or erythema around the wound, suggesting seroma over abscess. Thereafter, potentially contaminated instruments were discarded, and gloves and drapes changed.
Prior lateral hip incisions were reopened and enlarged to gain access to the posterior sacral hardware. Both existing screws were recannulated with wires, and the S2 screw was removed and replaced with a new Synthes 130 mm fully threaded 7.3 mm cannulated screw, which achieved moderate purchase. The S1 screw was removed; however, the standard washer was determined to be too small, risking propagation of the fracture. Instead, a mesh plate from the Synthes Variable Angle Midfoot set was chosen to act as the washer and cut to 3 × 3 holes. The larger surface area of the mesh plate allowed for increased bony interface of the construct, thus distributing the forces and decreasing the risk of fracture propagation while also increasing stability. The middle hole of the plate was placed over the S1 wire, followed by a standard washer, and the Synthes 165 mm fully threaded 7.3 mm cannulated screw (
Figure 5). This combination of hardware achieved excellent purchase and re-established stability of the right posterior pelvis. Alignment was confirmed with intraoperative fluoroscopy. There were no obvious perioperative complications, and the patient was transferred to the PACU.
2.4. Post-Op Course 2
The patient was instructed to be non-weight bearing on the right lower extremity and move through tolerated range of motion. The patient stayed in the hospital until being discharged on POD 6. The second postoperative course was benign.
The patient followed up in the outpatient clinic at three weeks, wherein pain was minimal, range of motion was good, and right lower extremity sensation was recovering faster than expected. Her incisions were healing well with no signs of infection and radiographs displayed stable alignment and healing progression. On her 6 week postoperative visit, there was further improvement. At her last office visit, the patient was 3 months post-surgery and had minimal pain, good range of motion, and full sensation through her right foot. Radiographs displayed fully healed fractures and stable alignment. At this point, the patient had not recovered any motor function of her right foot, likely related to the lumbosacral nerve injuries sustained in the car crash and was using a walker to ambulate. The patient was instructed to follow up again in 3 months but failed to schedule another appointment.
3. Discussion
Revision surgeries in the case of failed fixation for sacral fractures present a unique challenge. Getting an appropriately stable fixation while also being attentive to patient safety and avoiding neural injury is of the utmost importance. We present a case of a patient who sustained a highly displaced and translated sacral fracture treated with surgical fixation via a novel technique: a Synthes cannulated screw and washer combination wherein a tailored midfoot mesh plate was used as an additional washer for superior fixation. Upon hardware removal and revision, internal fixation was accomplished via Synthes cannulated screws and midfoot mesh plate as a washer. At 3 months of follow-up, fracture union was achieved, and the patient was able to return to weight-bearing with the assistance of an ambulatory device. It should be noted that the delay in recovery was primarily due to the lack of motor function of the right foot.
Sacral fractures, while generally rare, have increased in incidence in recent years due to the increased use of CT imaging and an aging population [
2]. Moreover, they are commonly concurrent with pelvic ring injuries, with a 30–40% occurrence in the case of the latter. They are often underdiagnosed and are associated with neurologic deficits in 25–50% of cases [
2]. This was observed in our patient who had a lasting foot drop, delaying ambulation. Vertical sacral fractures still pose a challenge for orthopedic surgeons to treat. Therefore, surgeons must choose the best treatment among various methods including percutaneous iliosacral screws, sacral plate fixation, and triangular osteosynthesis [
4]. The goal of surgical intervention in the case of this fracture is to achieve stability of sacral fracture as well as the SI joint, specifically in the vertical plane, to allow for stable weight bearing. That is why the use of trans-iliac trans-sacral screw was deployed in this setting to improve the load to failure [
4]. The use of the larger washer aided the construct by improving the compression that was achieved across the joint while also increasing the interface with the bone, thus allowing for more friction and more stable fixation.
While the concept of using a piece of equipment for an unintended use is far from novel, the innovative adaptation of using a midfoot mesh plate as a washer for sacral fracture fixation and for compressing a sacral fracture appears to be sparsely represented in the literature. Perhaps most analogously, Weale et al. performed an ORIF of a Leddy and Packer Type II flexor digitorum profundus (FDP) avulsion, using a single-hole cut of a plate to act as a washer for a 1.3 mm cortical screw. On a 6 week follow up, the fracture had healed, and the FDP was intact and possessed full flexion; although, the patient did develop a flexion contracture which required therapy [
7]. Of course, this case report diverges from that previous vignette as the vertical sacral fracture in question shares little in common with the avulsion fracture described. This is to say that, while the principle and technique of each treatment were comparable, the specific contexts of each injury were not, thereby making this case study all the more unique. The specific case by Weale et al., while clinically quite different, demonstrates similar principles and demonstrates that orthopedic equipment can be used in a variety of ways to achieve stable fracture fixation.
Principally, our technique does share elements with a procedure described by Qi-Fang et al.: in order to address inferior pole fractures, 2.4 mm straight locking compression plates were contoured intraoperatively to fixate proximal patellar fragments via the patellar tendon, yielding universally excellent outcomes [
8]. This novel approach mirrors our own in that both display instances in which the intraoperative modification of plates in particular was used to achieve proper fixation of a fracture at a joint. Although, once more, our approach becomes more unique upon comparison as Qi-Fang et al.’s plate contouring was a relatively minor adjustment meant to achieve the same goal as when using standard plating technique. This was not the case in our context as the functional role of the plate was completely divergent from providing corrective support for proper bone union.
Adjusting surgical technique invariably impacts the biomechanics of the joint in question. This was the case when Kong et Al. utilized a novel arrangement of plates to fixate distal humerus fractures. In doing so, they found that their adjustment of the standard two plate arrangement was superior to standard methods, boasting reduced stress, displacement, and greater stiffness [
9]. Similar results were found by Vojdani et al., who used a spiked washer-intramedullary screw combination to repair proximal fibular avulsions resulting from posterolateral corner (PLC) injury. Compared to the typical suture-bone tunnel method, the novel spiked washer approach granted greater biomechanical integrity in a cadaveric study [
10].
Although, in our context, the new technique of employing a midfoot plate as a primary washer to achieve superior fixation seemingly did not improve the biomechanics of the sacroiliac joint; rather, it was comparable to standard techniques. The focus of our technique was not to improve the biomechanical outcomes afforded by surgical intervention, but to achieve robust fixation of a sacral fracture where standard methods failed. Therefore, its lack of negative impact on SI joint biomechanics should be seen as meritorious. Potential drawbacks of the implementation of this method include the need for a larger surgical incision in order for the plate to fit into the tissue. This could lead to increased risk of wound complications that are not seen in the small percutaneous incision that is typically used. Additionally, the presence of more hardware leads to the inherent risk of peri-implant infection. Our study did not demonstrate any issue with these downsides; however, they should be considered when implementing this technique.



 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}