Abstract
Background: There is sparse literature on the technique of single-stage anterior discectomy fusion and posterior decompression and flavectomy using the biportal endoscopic technique. Methods: Single-stage anterior discectomy fusion and posterior biportal endoscopic decompression and flavectomy apply to cervical myelopathy at a single level with an anterior disc and posterior ossified ligamentum flavum complex. Anterior discectomy and fusion were performed in the usual fashion in the supine position, and subsequently, posterior biportal endoscopic decompression was carried out after turning the patient prone. Conclusion: Single-stage anterior discectomy fusion and posterior biportal endoscopic decompression and flavectomy are good alternatives for circumferential decompression with myelopathy
1. Relevant Surgical Anatomy
Ossification of the ligamentum flavum (OLF) is a relatively rare clinical entity secondary to a combination of intrinsic and extrinsic factors occurring in all parts of the spine, particularly in the thoracic spine, but rarely in the cervical region [1]. Advanced imaging modalities, especially computed tomography (CT) and magnetic resonance imaging (MRI), increased the detectable rate of asymptomatic OLF [2].
Cervical OLF is refractory to conservative management, and surgical decompression is recommended [3]. Cervical OLF can manifest as a single-segment or multi-segment distribution on sagittal Magnetic Resonance Imaging. Depending on the location of ossification lesions in the lamina, Cervical OLF could be grouped into right-sided, central, left-sided or bilateral. OLF is analyzed into two parts: as a capsular portion and an inter-laminar portion. Ossification begins from the capsular portion and progresses to the interlaminar portion of the LF. In the transverse plane, ossification begins from the posterior side and progresses to the Dura. Sato classified this disorder according to the progression into Lateral, Extended, Enlarged, Fused and Tuberous types. The more advanced the ossification, the more stenotic the spinal canal [4].
In addition, the distribution of Cervical OLF, just like the ossified posterior longitudinal ligament, has a distinct predisposition in Japan [5]. The common symptoms of Cervical OLF patients are similar to those of cervical myelopathy, including motor, sensory and gait disturbances. Cervical OLF patients usually present first with sensory deficits, followed by limb weakness and, later, gait disturbance [6].
Here, we describe a case of cervical myelopathy with degenerative disc disease and ossified ligamentum flavum at the c3 level (Figure 1A–D).
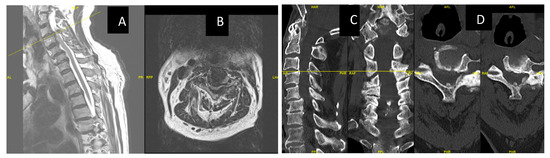
Figure 1.
(A,B): MRI showing severe central canal and severe bilateral neural foraminal stenosis at C3-4 with compression on the spinal cord and focal gliosis/myelomalacia/ Figure 2 (C,D) show CT images of C34 OLF, C34 and C56 listhesis.
2. Technique Description
2.1. Clinical Examination and Radiological Investigation for Identifying the Cause of Cervical Myelopathy
Clinical symptoms and signs for cervical myelopathy with radiological imaging are key in patient selection. X-ray Antero-Posterior and lateral views help to identify the alignment of the neck, recognize any kyphotic deformity, and identify any gross instability. MRI identifies the level of compression of the spinal cord to determine any spinal cord signal changes. CT scans help to delineate the type of ossification of the flavum and help in surgical planning.
2.2. Anesthesia and Positioning
The patient is positioned supine first for the first part of the surgery for Anterior Cervical Discectomy and Fusion. Surgery is performed under General Anesthesia, and the patient is placed onto a radiolucent table. The authors prefer to approach from the right for the anterior approach to the cervical spine. Once Anterior Cervical Discectomy and Fusion are carried out, the patient is then turned prone after the application of the Mayfield clamp (Figure 2A).
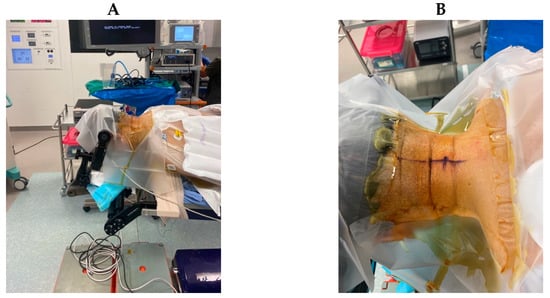
Figure 2.
(A): Patient positioned prone after the application of Mayfield clamps after the ACDF procedure, (B): Skin markings 2 cm apart over the pedicle line at the target level C3 lamina.
2.3. Skin Marking
The surgeon stands on the same side as the pathology (the left side, in this case). Two portals are made with two skin incisions (Figure 2B) of 7 mm in length that are made horizontally on the pedicle under the guidance of C-arm fluoroscopy (Figure 3A–D). Each skin incision for the portal is made at the upper and lower pedicle (C3 and C4), related to the target level. The distance between these two portals is about 2 cm.
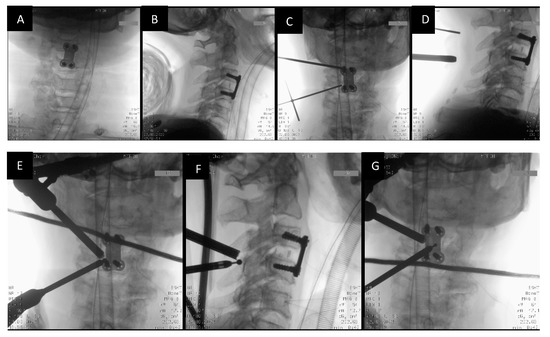
Figure 3.
Radiological identification of the portal placement levels with the Image Intensifier. (A,B) show the AP and Lateral views prior to skin marking. (C,D) show skin marking with metal markers in AP and Lateral views. (E,F) show ipsilateral burring using a 3.5 mm spherical diamond burr. (G) shows sublaminar burring of the contralateral side.
2.4. Docking and Working Channel Placement
After making two portals, fascia is incised in a T-shape manner. A muscle elevator is used to elevate and clear the muscle over the lamina. Serial dilators are used to dissect the neck muscle and generate operative space. A 0° endoscope is inserted through the viewing portal. The saline irrigation pressure is kept at 30 mmHg. Surgical instruments of the biportal endoscopic spine surgery set (BESS™ set) are inserted through the working portal.
2.5. Identification of the V Point
Triangulation with the endoscope and instrument is carried out on the margin of the superior lamina. Then, the inferior lamina and medial point of the facet joint (V-point) are identified. Remnant soft tissue around the V-point is removed, and the minor bleeding is controlled with a radiofrequency (RF) probe (Bonss Medical™) to clear the surgical field.
2.6. Drilling of the Ipsilateral Lamina and Laminectomy
The upper lamina (C3) is drilled starting at the inferolateral region, then proceeding in the craniolateral direction with the 3.0 mm spherical diamond burr. This is done until the ligament flavum is just detached from the upper lamina. The superolateral part of the lower lamina (C4) is then burred in the caudal direction until it is paper thin. The ligament flavum should be preserved until the bone work is finished for the protection of the thecal sac (Figure 4A–C).
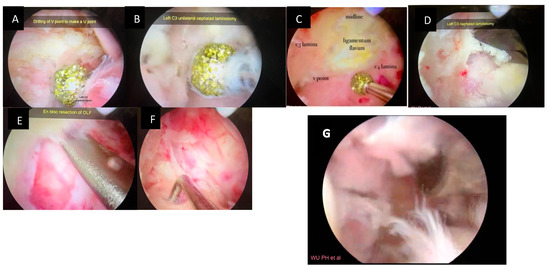
Figure 4.
Intraoperative pictures showing various stages of posterior decompression and flavectomy. (A): Drilling at the V point, (B): drilling of cephalad lamina until the margin of OLF, (C): drilling until the caudal margin of OLF, (D): cephalad laminotomy with a 1 mm Kerrison punch (E): lifting and en bloc removal of OLF by a fine dissector, (F): dura after resection of ligamentum flavum, (G): video of the UBE_technique (Video S1).
2.7. Sublaminar Drilling of the Contralateral Lamina
The sublaminar area of the contralateral side is drilled until the medial part of the contralateral facet is exposed. This is carried out while retaining the spinous process and the contralateral outer cortical bone (Figure 3E–G). Further, the thinned area of the lamina is removed using the fine dissector or 1 mm Kerrison punch (Figure 4D)
2.8. Detaching the Ligamentum Flavum en Bloc
Subsequently, the LF is separated from the edges of attachment to the lamina and the facet joints using a fine dissector and nerve hook (Figure 4E). Then, the LF is removed en bloc (Figure 5B) using fine pituitary forceps, and the dura is fully exposed. (Figure 4F).
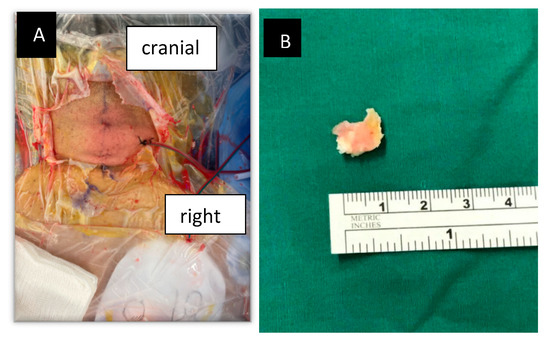
Figure 5.
(A) Wound closure after drain insertion. (B) Ligamentum flavum after en bloc excision.
2.9. Confirmation of Decompression Using Intraoperative Computer Tomographic (O Arm) SCAN
After the completion of decompression, we perform an intraoperative 3-D CT imaging using an O- Arm to radiologically confirm the adequacy of decompression (Figure 6A–D).
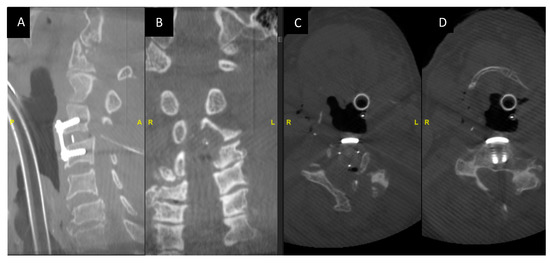
Figure 6.
Intraoperative O-arm CT images showing the adequacy of decompression and the implant position. (A,B) Intraoperative O arm imaging sagittal and coronal images post-decompression. (C,D) Axial cuts at the C3 level post-decompression.
2.10. Wound Closure with Drain
The wound is closed after the insertion of the surgical drain (Figure 5A). Vicryl 3/0 is used to oppose skin edges. The drain is maintained active to avoid any hematoma collection.
3. Indications
Treating cervical stenosis associated with myelopathy contributed by ossification of the ligamentum flavum. Facet cyst and residual foraminal stenosis after anterior cervical discectomy fusion.
4. Limitations
Cervical stenosis extending more than three levels with an extensively ossified ligamentum flavum may be a limitation for the procedure.
5. How to Avoid Complications
- Preoperative radiological imaging such as MRI for evaluating the level and extent of stenosis and myelopathy.
- Identification of the calcified ligamentum flavum on the CT scan and knowing the extent and location of the calcification.
- Using a high-speed drill to gradually thin the ossified ligamentum flavum until there is a translucent thin layer left. Before the resection of the ossified ligamentum flavum, the normal boundary of the ligamentum flavum should be clearly revealed [7].
- A technique performed through the stepwise approach can help in the identification of key anatomical structure checkpoints and in highlighting the targets for decompression required to achieve good radiological and clinical outcomes [8].
- The ligament flavum can be preserved until the bone work is finished.
- An intraoperative 3D CT scan confirming the adequacy of decompression.
6. Specific Perioperative Considerations
The patient can mobilize the next morning; the drain can be removed when the drainage is below 80 mL per 24 h.
7. Patient Education about Surgery and the Potential Risks Involved
There is potential risk of injury to the dura and spinal cord. Conversion to open surgery is possible in cases of significant bleeding obstructing endoscopic vision. Alternative treatments including posterior open decompression and stabilization can be discussed.
8. Summary of 10 Key Points
- The advantages of biportal endoscopic approaches over conventional open surgery include the preservation of the normal structures, less intraoperative bleeding and fast postoperative recovery [9].
- Biportal endoscopy allows for a direct, magnified and closeup view of the pathology.
- Systematic evaluation of the MRI and CT scans to plan the surgery.
- Usage of intraoperative fluoroscopy to localize the drilling and the extent of decompression.
- Use of a 3.5 mm high-speed diamond drill to thin out the lamina, and use of dissectors and a 1 mm Kerrison for the final flavectomy.
- Before the resection of the ossified ligamentum flavum, the normal boundary of the ligamentum flavum is to be clearly revealed.
- The flavum is to be preserved until the bone work is finished.
- Hemostasis with radiofrequency is preferred rather than increasing the pump pressure. Keeping the pump pressure at 30–40 mmHg in most parts of the operation is preferred.
- Intraoperative 3D CT scan to confirm adequate decompression.
- Usage of the drain is preferred to avoid hematoma at the spinal cord level.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/std12020007/s1, Video S1: Cervical UBE one-block resection of calcified ligamentum flavum.
Author Contributions
R.G. and P.H.W. contributed equally in study conception and methodology, data curation, analysis, interpretation of results and original draft preparation. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This is an IRB-exempt technical case report; informed consent was obtained from the patient for publication.
Informed Consent Statement
Informed consent was obtained from the patient for publishing this article.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy protection.
Conflicts of Interest
Pang Hung Wu, as the first co-author, declares that his spouse is the director of the Singapore-based company Endocare PTE LTD, which distributes orthopedic and spine products including BESS, NSK drills and Bonss Energy systems. Rajeesh George, as the co-author, declares no conflict of interest.
References
- Kim, S.I.; Ha, K.Y.; Lee, J.W.; Kim, Y.H. Prevalence and related clinical factors of thoracic ossification of the ligamentum flavum-a computed tomography-based cross-sectional study. Spine J. 2018, 18, 551–557. [Google Scholar] [CrossRef] [PubMed]
- Kubota, M.; Baba, I.; Sumida, T. Myelopathy due to ossification of the ligamentum flavum of the cervical spine. A report of two cases. Spine 1981, 6, 553–559. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.J.; Luk, K.D.; Karppinen, J.; Yang, H.; Cheung, K.M. Prevalence, distribution, and morphology of ossification of the ligamentum flavum: A population study of one thousand seven hundred thirty-six magnetic resonance imaging scans. Spine 2010, 35, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Ahn, D.K.; Lee, S.; Moon, S.H.; Boo, K.H.; Chang, B.K.; Lee, J.I. Ossification of the ligamentum flavum. Asian Spine J. 2014, 8, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Nouri, A.; Tetreault, L.; Singh, A.; Karadimas, S.K.; Fehlings, M.G. Degenerative Cervical Myelopathy: Epidemiology, Genetics, and Pathogenesis. Spine 2015, 40, E675–E693. [Google Scholar] [CrossRef] [PubMed]
- Baron, E.M.; Young, W.F. Cervical spondylotic myelopathy: A brief review of its pathophysiology, clinical course, and diagnosis. Neurosurgery 2007, 60, S35–S41. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Rao, S.; Li, Y.; Zhao, S.; Chen, B. Posterior percutaneous full-endoscopic cervical laminectomy and decompression for cervical stenosis with myelopathy: A technical note. World Neurosurg. 2019, 124, 350357. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.H.; Kim, H.S.; Lee, Y.J.; Kim, D.H.; Lee, J.H.; Yang, K.-H.; Raorane, H.D.; Jang, I.-T. Posterior endoscopic cervical foramiotomy and discectomy: Clinical and radiological computer tomography evaluation on the bony effect of decompression with 2 years follow-up. Eur. Spine J. 2021, 30, 534–546. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Heo, D.H.; Lee, D.C.; Chung, H.T. Biportal endoscopic unilateral laminotomy with bilateral decompression for the treatment of cervical spondylotic myelopathy. Acta Neurochir. 2021, 163, 2537–2543. [Google Scholar] [CrossRef] [PubMed]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).