
Monitoring Humoral Response Following BNT162b2 mRNA Vaccination against SARS-CoV-2 in Hematopoietic Stem-Cell Transplantation Patients: A Single-Center Prospective Study along with a Brief Review of Current Literature

 , , , ,
, , , ,  ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Treatment
3.2. Hypogammaglobulinemia
3.3. Time between HSCT and Vaccination
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yigenoglu, T.N.; Ata, N.; Altuntas, F.; Bascı, S.; Dal, M.S.; Korkmaz, S.; Namdaroglu, S.; Basturk, A.; Hacıbekiroglu, T.; Dogu, M.H.; et al. The Outcome of COVID-19 in Patients with Hematological Malignancy. J. Med. Virol. 2021, 93, 1099–1104. [Google Scholar] [CrossRef] [PubMed]
- Vijenthira, A.; Gong, I.Y.; Fox, T.A.; Booth, S.; Cook, G.; Fattizzo, B.; Martín-Moro, F.; Razanamahery, J.; Riches, J.C.; Zwicker, J.; et al. Outcomes of Patients with Hematologic Malignancies and COVID-19: A Systematic Review and Meta-Analysis of 3377 Patients. Blood 2020, 136, 2881. [Google Scholar] [CrossRef]
- Sharma, A.; Bhatt, N.S.; St Martin, A.; Abid, M.B.; Bloomquist, J.; Chemaly, R.F.; Dandoy, C.; Gauthier, J.; Gowda, L.; Perales, M.A.; et al. Clinical Characteristics and Outcomes of COVID-19 in Haematopoietic Stem-Cell Transplantation Recipients: An Observational Cohort Study. Lancet Haematol. 2021, 8, e185–e193. [Google Scholar] [CrossRef]
- Ljungman, P.; de la Camara, R.; Mikulska, M.; Tridello, G.; Aguado, B.; Zahrani, M.A.; Apperley, J.; Berceanu, A.; Bofarull, R.M.; Calbacho, M.; et al. COVID-19 and Stem Cell Transplantation; Results from an EBMT and GETH Multicenter Prospective Survey. Leukemia 2021, 35, 2885–2894. [Google Scholar] [CrossRef] [PubMed]
- Boyarsky, B.J.; Werbel, W.A.; Avery, R.K.; Tobian, A.A.R.; Massie, A.B.; Segev, D.L.; Garonzik-Wang, J.M. Antibody Response to 2-Dose SARS-CoV-2 MRNA Vaccine Series in Solid Organ Transplant Recipients. JAMA 2021, 325, 2204–2206. [Google Scholar] [CrossRef]
- Herishanu, Y.; Avivi, I.; Aharon, A.; Shefer, G.; Levi, S.; Bronstein, Y.; Morales, M.; Ziv, T.; Shorer Arbel, Y.; Scarfò, L.; et al. Efficacy of the BNT162b2 MRNA COVID-19 Vaccine in Patients with Chronic Lymphocytic Leukemia. Blood 2021, 137, 3165–3173. [Google Scholar] [CrossRef] [PubMed]
- Terpos, E.; Gavriatopoulou, M.; Fotiou, D.; Giatra, C.; Asimakopoulos, I.; Dimou, M.; Sklirou, A.D.; Ntanasis-Stathopoulos, I.; Darmani, I.; Briasoulis, A.; et al. Poor Neutralizing Antibody Responses in 132 Patients with CLL, NHL and HL after Vaccination against SARS-CoV-2: A Prospective Study. Cancers 2021, 13, 4480. [Google Scholar] [CrossRef]
- Werbel, W.A.; Boyarsky, B.J.; Ou, M.T.; Massie, A.B.; Tobian, A.A.R.; Garonzik-Wang, J.M.; Segev, D.L. Safety and Immunogenicity of a Third Dose of SARS-CoV-2 Vaccine in Solid Organ Transplant Recipients: A Case Series. Ann. Intern. Med. 2021, 174, 1330–1332. [Google Scholar] [CrossRef]
- Attolico, I.; Tarantini, F.; Carluccio, P.; Schifone, C.P.; Delia, M.; Gagliardi, V.P.; Perrone, T.; Gaudio, F.; Longo, C.; Giordano, A.; et al. Serological Response Following BNT162b2 Anti-SARS-CoV-2 MRNA Vaccination in Haematopoietic Stem Cell Transplantation Patients. Br. J. Haematol. 2022, 196, 928–931. [Google Scholar] [CrossRef]
- Autore, F.; Stirparo, L.; Innocenti, I.; Papa, E.; Marchesi, F.; Togni, C.; Mariani, S.; Torrieri, L.; Salvatori, M.; Fazio, F.; et al. Immunogenicity of SARS-CoV-2 Vaccination in Patients Undergoing Autologous Stem Cell Transplantation. A Multicentric Experience. Front. Oncol. 2022, 12, 897937. [Google Scholar] [CrossRef]
- Canti, L.; Humblet-Baron, S.; Desombere, I.; Neumann, J.; Pannus, P.; Heyndrickx, L.; Henry, A.; Servais, S.; Willems, E.; Ehx, G.; et al. Predictors of Neutralizing Antibody Response to BNT162b2 Vaccination in Allogeneic Hematopoietic Stem Cell Transplant Recipients. J. Hematol. Oncol. 2021, 14, 174. [Google Scholar] [CrossRef] [PubMed]
- Chevallier, P.; Coste-Burel, M.; Le Bourgeois, A.; Peterlin, P.; Garnier, A.; Béné, M.C.; Imbert, B.; Drumel, T.; Le Gouill, S.; Moreau, P.; et al. Safety and Immunogenicity of a First Dose of SARS-CoV-2 MRNA Vaccine in Allogeneic Hematopoietic Stem-Cells Recipients. EJHaem 2021, 2, 520–524. [Google Scholar] [CrossRef] [PubMed]
- Chiarucci, M.; Paolasini, S.; Isidori, A.; Guiducci, B.; Loscocco, F.; Capalbo, M.; Visani, G. Immunological Response Against SARS-COV-2 After BNT162b2 Vaccine Administration Is Impaired in Allogeneic but Not in Autologous Stem Cell Transplant Recipients. Front. Oncol. 2021, 11, 737300. [Google Scholar] [CrossRef]
- Dhakal, B.; Abedin, S.; Fenske, T.; Chhabra, S.; Ledeboer, N.; Hari, P.; Hamadani, M. Response to SARS-CoV-2 Vaccination in Patients after Hematopoietic Cell Transplantation and CAR T-Cell Therapy. Blood 2021, 138, 1278–1281. [Google Scholar] [CrossRef] [PubMed]
- Mamez, A.C.; Pradier, A.; Giannotti, F.; Petitpas, A.; Urdiola, M.F.; Vu, D.L.; Masouridi-Levrat, S.; Morin, S.; Dantin, C.; Clerc-Renaud, D.; et al. Antibody Responses to SARS-CoV2 Vaccination in Allogeneic Hematopoietic Stem Cell Transplant Recipients. Bone Marrow Transplant. 2021, 56, 3094–3096. [Google Scholar] [CrossRef]
- Matkowska-Kocjan, A.; Owoc-Lempach, J.; Chruszcz, J.; Kuźnik, E.; Szenborn, F.; Jurczenko, L.; Wójcik, M.; Banyś, D.; Szenborn, L.; Ussowicz, M. The COVID-19 MRNA BNT163b2 Vaccine Was Well Tolerated and Highly Immunogenic in Young Adults in Long Follow-Up after Haematopoietic Stem Cell Transplantation. Vaccines 2021, 9, 1209. [Google Scholar] [CrossRef] [PubMed]
- Kimura, M.; Ferreira, V.H.; Kothari, S.; Pasic, I.; Mattsson, J.I.; Kulasingam, V.; Humar, A.; Mah, A.; Delisle, J.S.; Ierullo, M.; et al. Safety and Immunogenicity After a Three-Dose SARS-CoV-2 Vaccine Schedule in Allogeneic Stem Cell Transplant Recipients. Transplant. Cell Ther. 2022, 28, 706.e1–706.e10. [Google Scholar] [CrossRef]
- Le Bourgeois, A.; Coste-Burel, M.; Guillaume, T.; Peterlin, P.; Garnier, A.; Béné, M.C.; Chevallier, P. Safety and Antibody Response After 1 and 2 Doses of BNT162b2 MRNA Vaccine in Recipients of Allogeneic Hematopoietic Stem Cell Transplant. JAMA Netw. Open 2021, 4, e2126344. [Google Scholar] [CrossRef]
- Leclerc, M.; Redjoul, R.; Le Bouter, A.; Beckerich, F.; Robin, C.; Parinet, V.; Pautas, C.; Menouche, D.; Bouledroua, S.; Roy, L.; et al. Determinants of SARS-CoV-2 Waning Immunity in Allogeneic Hematopoietic Stem Cell Transplant Recipients. J. Hematol. Oncol. 2022, 15, 27. [Google Scholar] [CrossRef]
- Piñana, J.L.; López-Corral, L.; Martino, R.; Montoro, J.; Vazquez, L.; Pérez, A.; Martin-Martin, G.; Facal-Malvar, A.; Ferrer, E.; Pascual, M.J.; et al. SARS-CoV-2-Reactive Antibody Detection after SARS-CoV-2 Vaccination in Hematopoietic Stem Cell Transplant Recipients: Prospective Survey from the Spanish Hematopoietic Stem Cell Transplantation and Cell Therapy Group. Am. J. Hematol. 2022, 97, 30–42. [Google Scholar] [CrossRef]
- Ram, R.; Hagin, D.; Kikozashvilli, N.; Freund, T.; Amit, O.; Bar-On, Y.; Beyar-Katz, O.; Shefer, G.; Moshiashvili, M.M.; Karni, C.; et al. Safety and Immunogenicity of the BNT162b2 MRNA COVID-19 Vaccine in Patients after Allogeneic HCT or CD19-Based CART Therapy-A Single-Center Prospective Cohort Study. Transplant. Cell Ther. 2021, 27, 788–794. [Google Scholar] [CrossRef] [PubMed]
- Redjoul, R.; Le Bouter, A.; Beckerich, F.; Fourati, S.; Maury, S. Antibody Response after Second BNT162b2 Dose in Allogeneic HSCT Recipients. Lancet 2021, 398, 298–299. [Google Scholar] [CrossRef] [PubMed]
- Salvini, M.; Maggi, F.; Damonte, C.; Mortara, L.; Bruno, A.; Mora, B.; Brociner, M.; Mattarucchi, R.; Ingrassia, A.; Sirocchi, D.; et al. Immunogenicity of Anti-SARS-CoV-2 Comirnaty Vaccine in Patients with Lymphomas and Myeloma Who Underwent Autologous Stem Cell Transplantation. Bone Marrow Transplant. 2022, 57, 137–139. [Google Scholar] [CrossRef] [PubMed]
- Shem-Tov, N.; Yerushalmi, R.; Danylesko, I.; Litachevsky, V.; Levy, I.; Olmer, L.; Lusitg, Y.; Avigdor, A.; Nagler, A.; Shimoni, A.; et al. Immunogenicity and Safety of the BNT162b2 MRNA COVID-19 Vaccine in Haematopoietic Stem Cell Transplantation Recipients. Br. J. Haematol. 2022, 196, 884–891. [Google Scholar] [CrossRef] [PubMed]
- Tamari, R.; Politikos, I.; Knorr, D.A.; Vardhana, S.A.; Young, J.C.; Marcello, L.A.T.; Doddi, S.; Devlin, S.M.; Ramanathan, L.V.; Pessin, M.S.; et al. Predictors of Humoral Response to SARS-CoV-2 Vaccination after Hematopoietic Cell Transplantation and CAR T-Cell Therapy. Blood Cancer Discov. 2021, 2, 577–585. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, M.; Yakushijin, K.; Funakoshi, Y.; Ohji, G.; Hojo, W.; Sakai, H.; Saeki, M.; Hirakawa, Y.; Matsumoto, S.; Sakai, R.; et al. The Safety and Immunogenicity of the BNT162b2 MRNA COVID-19 Vaccine in Japanese Patients after Allogeneic Stem Cell Transplantation. Vaccines 2022, 10, 158. [Google Scholar] [CrossRef] [PubMed]
- Gagelmann, N.; Passamonti, F.; Wolschke, C.; Massoud, R.; Niederwieser, C.; Adjallé, R.; Mora, B.; Ayuk, F.; Kröger, N. Antibody Response after Vaccination against SARS-CoV-2 in Adults with Hematological Malignancies: A Systematic Review and Meta-Analysis. Haematologica 2022, 107, 1840–1849. [Google Scholar] [CrossRef] [PubMed]
- Cordonnier, C.; Einarsdottir, S.; Cesaro, S.; Di Blasi, R.; Mikulska, M.; Rieger, C.; de Lavallade, H.; Gallo, G.; Lehrnbecher, T.; Engelhard, D.; et al. Vaccination of Haemopoietic Stem Cell Transplant Recipients: Guidelines of the 2017 European Conference on Infections in Leukaemia (ECIL 7). Lancet Infect Dis 2019, 19, e200–e212. [Google Scholar] [CrossRef] [PubMed]
- Montague, B.T.; Wipperman, M.F.; Chio, E.; Crow, R.; Hooper, A.T.; O’Brien, M.P.; Simões, E.A.F. Elevated Serum IgA Following Vaccination against SARS-CoV-2 in a Cohort of High-Risk First Responders. Sci. Rep. 2022, 12, 14932. [Google Scholar] [CrossRef]
- Luis Piñana, J.; Vazquez, L.; Calabuig, M.; López-Corral, L.; Martin-Martin, G.; Villalon, L.; Sanz-Linares, G.; Conesa-Garcia, V.; Sanchez-Salinas, A.; Gago, B.; et al. One-Year Breakthrough SARS-CoV-2 Infection and Correlates of Protection in Fully Vaccinated Hematological Patients. Blood Cancer J. 2023, 13, 8. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | N [%] |
|---|---|
| Median age in years (range) | 56 (19–71) |
| Median time from HSCT in months (range) | 32.9 (6.4–60) |
| Male | 30 [55.6] |
| Underlying hematologic malignancy | |
| Lymphoma | 31 [57.4] |
| Hodgkin | 12 [22.2] |
| non-Hodgkin | 19 [35.2] |
| Multiple myeloma | 19 [35.2] |
| Acute leukemia | 4 [7.4] |
| Type of HSCT | |
| Autologous | 50 [92.6] |
| Treatment at the time of vaccination | 24/51 [47.1] |
| Anti-CD20 antibody | 5 [10.0] |
| Lenalidomide | 11 [22.0] |
| Other α | 8 [14.0] |
| Prior lines of treatment, median (range) | 3 (2–8) |
| Patients with hypogammaglobulinemia | |
| IgG levels <700 mg/dL | 11/43 [25.6] |
| IgG levels <500 mg/dL | 5/43 [11.6] |
| IgA levels <70 mg/dL | 10/40 [25.0] |
| IgM levels <40 mg/dL | 21/43 [48.8] |
| Any class hypogammaglobulinemia β | 26/43 [60.5] |
| Measurement of AT post-vaccination | |
| Both at 1 month and at 3 months | 47 [87.0] |
| At 1 month only | 5 [9.0] |
| At 3 months only | 2 [4.0] |
| Pt | Gender/ Age (y) | Disease | Hypo-γ | Time from HSCT to Vaccination (mo) | Tx at Vaccination | No. of Tx Lines Before Vaccination |
|---|---|---|---|---|---|---|
| 1 | M/68 | DLBCL | No | 23.90 | No | 3 |
| 2 | F/49 | HL | No | 50.39 | No | 7 |
| 3 | M/37 | FL | Yes | 21.41 | Rituximab | 4 |
| 4 | F/62 | AITL | Yes | 21.87 | BV/Benda | 3 |
| 5 α | F/66 | FL | Yes | 59.05 | Azacitidine | 6 |
| 6 | M/47 | MCL | Yes | 9.64 | Rituximab | 3 |
| 7 | M/67 | MCL | Yes | 39.15 | Rituximab | 3 |
| 8 | F/65 | MM | Yes | 13.64 | Pom/Dex | 8 |
| 9 | F/69 | MM | Yes | 45.64 | Carlf/Dex | 8 |
| Antibody Titers Post-Vaccination (U/mL) | 1 Month After, % | 3 Months After, % |
|---|---|---|
| <0.8 | 19.2 | 14.3 |
| 0.8–19.9 | 5.8 | 6.1 |
| 20–249.9 | 13.5 | 26.5 |
| 250–999.9 | 23.1 | 22.4 |
| 1000–1999.9 | 13.5 | 18.4 |
| 2000–4999.9 | 15.4 | 10.2 |
| ≥5000.0 | 9.6 | 2.0 |
| Factor | N | AR at m1 | AT at m1 (U/mL) | p | N | AR at m3 | AT at m3 (U/mL) | p | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pos [%] | p | Median | Range | Pos [%] | p | Median | Range | |||||
| IgA hypogamma | 0.019 | 0.02 | 0.046 | 0.04 | ||||||||
| IgA < 70 mg/dL | 10 | 5 [50.0] | 5.3 | 0.4–112 | 10 | 6 [60.0] | 25.38 | 0.4–1504 | ||||
| IgA ≥ 70 mg/dl | 29 | 25 [86.2] | 388 | 0.4–25,000 | 27 | 24 [88.8] | 269 | 0.4–7869 | ||||
| Any class hypogamma | 0.02 | 0.018 | 0.017 | |||||||||
| Yes | 25 | 16 [64.0] | 110 | 0.4–3419 | 22 | 16 [72.7] | 0.08 | 86.7 | 0.4–2486 | |||
| No | 17 | 16 [94.1] | 1065 | 0.4–25,000 | 17 | 16 [94.1] | 850 | 0.4–7869 | ||||
| Combined IgA hypogamma and levels of other Ig classes | 0.04 | 0.049 | 0.1 | 0.06 | ||||||||
| Group A | 15 | 14 [93.3] | 538 | 0.4–25,000 | 15 | 14 [93.3] | 703 | 0.4–7869 | ||||
| Group B | 14 | 11 [78.5] | 277 | 0.4–3419 | 12 | 10 [83.3] | 203 | 0.4–2486 | ||||
| Group C | 10 | 5 [50.0] | 5.3 | 0.4–1112 | 10 | 6 [60.0] | 25.3 | 0.4–1704 | ||||
| Time from HSCT to vaccine | 0.6 | 0.037 | 1 | 0.29 | ||||||||
| <18 months | 44 | 36 [81.8] | 64.25 | 0.4–828 | 42 | 36 [85.7] | 118 | 0.4–1704 | ||||
| ≥18 months | 8 | 6 [75.0] | 767 | 0.4–25,000 | 7 | 6 [85.7] | 339 | 0.4–7869 | ||||
| Treatment | <0.001 | <0.0001 | 0.006 | <0.0001 | ||||||||
| No treatment | 26 | 24 [92.3] | 1488 | 0.4–25,000 | 26 | 24 [92.3] | 1193 | 0.4–7869 | ||||
| Anti-CD20 antibody | 5 | 1 [20.0] | 0.4 | 0.4–423 | 5 | 2 [40.0] | 0.4 | 0.4–97.9 | ||||
| Other | 8 | 4 [50.0] | 9755 | 0.4–1844 | 6 | 4 [66.6] | 95.85 | 0.4–850 | ||||
| Lenalidomide | 10 | 10 [100.0] | 210 | 10.2–1100 | 10 | 6 [60.0] | 118.75 | 4.06–418 | ||||
| Previous lines of Tx | 0.137 | 0.016 | 0.237 | 0.026 | ||||||||
| <3 | 7 | 7 [100.0] | 2174 | 282–3591 | 7 | 7 [100.0] | 1647 | 118–2486 | ||||
| ≥3 | 36 | 27 [75.0] | 330 | 0.4–25,000 | 35 | 29 [83.0] | 145 | 0.4–7869 | ||||
| Study, First Author | Ref. | N | AGE, y (δ), [Range] | HSCT Type | TΙTV, m (δ), [Range] | TMV, d (δ), [Range] | RR [%], (PCO) | AT (δ), [Range] |
|---|---|---|---|---|---|---|---|---|
| ATTOLICO | [9] | 114 | 56 [20–71] | BOTH α | NA β | 28 [NA] γ | 84 (≥50 AU/mL) | 4481 [0–104,689] |
| AUTORE | [10] | 58 | 59 [27–71] | AUTO | 8 [0.6–17] | 65 [24–214] | 67 (>0.8 BAU/mL) | 139.533 [0.02–11,097] |
| CANTI | [11] | 37 | 60 [26–76] | ALLO | 31 [5–51] | 28 δ | 86 (>5 IU/mL) | NA |
| CHEVALLIER | [12] | 112 | 57 [20–75] | ALLO | 22 [3–206] | 21.5 [16–35] ε | 55 | NA |
| CHIARUCCI | [13] | 50 | 60 [21–72] | BOTH στ | 13 [0.2–26] | 30 | 76 | 282 AU/mL [68–>400] |
| DHAKAL ζ | [14] | 130 | 65 [25–77] | BOTH η | NA | NA | 60 | NA |
| MAMEZ θ | [15] | 63 | 54 [18–78] | ALLO | 14 [3–150] | 38 [13–98] | 76 | 815 IU/mL [NA] |
| MATKOWSKA | [16] | 65 | 21 [18–31] | ALLO | 126 [36–324] | NA [14–21] | 96 | NA ι |
| KIMURA (3-dose vacc) | [17] | 122 | 57 [45–64] | ALLO | d2; 8.3[5.3–22.7] d3; 15.3[9.8–29.4] | NA | 89.1 (after 3rd dose) | 2nd dose; 125.6 U/mL [2.8–1251] κ 3rd dose; 10,358 U/mL [673.9–31.753] κ |
| LE BOURGEOIS | [18] | 117 | 57 [20–75] | ALLO | 22 [3–207] | 35 [18–77] | 83 (>0.8 U/mL) | NA |
| LECLERC λ | [19] | 133 μ | NA | ALLO | NA | NA ν | 72 ξ | NA |
| PINANA ο | [20] | 397 | 59 [18–80] | BOTH | 93 [3–763] | 21 [15–59] | 78 | NA |
| RAM | [21] | 66 | 65 [23–83] | ALLO | 32 [3–263] | NA [7–14] | 75 | 178 [0.4–250] |
| REDJOUL | [22] | 88 | 28 [26–31] | ALLO | 23 [3–213] | 28 [26–31] κ | 78 | NA |
| SALVINI | [23] | 64 | 62 [29–75] | AUTO | 25.6 [1.2–58.1] | 28 [25–48] | 87 | 747 BAU/mL [101–2018] |
| SHEM-TOV | [24] | 152 | 58 π [22–82]κ | ALLO | 41 [24–77] | 28 [8–69] κ | 78 | NA |
| TAMARI ρ | [25] | 217 | 66 [25–84] | BOTH σ | 36 [17–63] κ | 28 and 90 | 1-m; 61 τ 3-m; 87 | 1-m; 479.75 AU/mL [170.4–3658.8] κ 3-m; 5379 AU/mL [451–15,750] ξκ |
| WATANABE | [26] | 25 | 55 [23–71] | ALLO | 57 [6–147] | NA υ | 76 | NA |
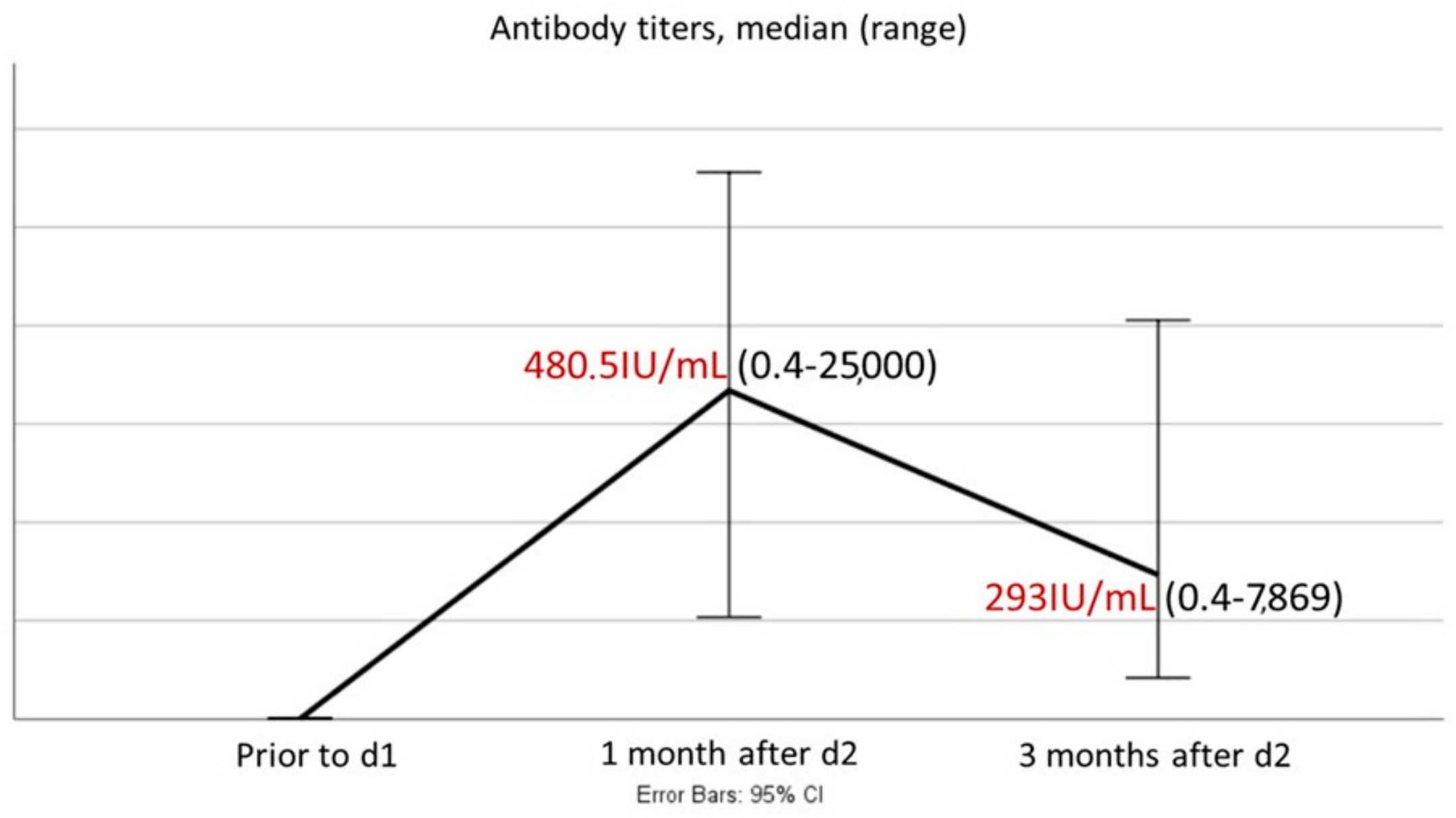
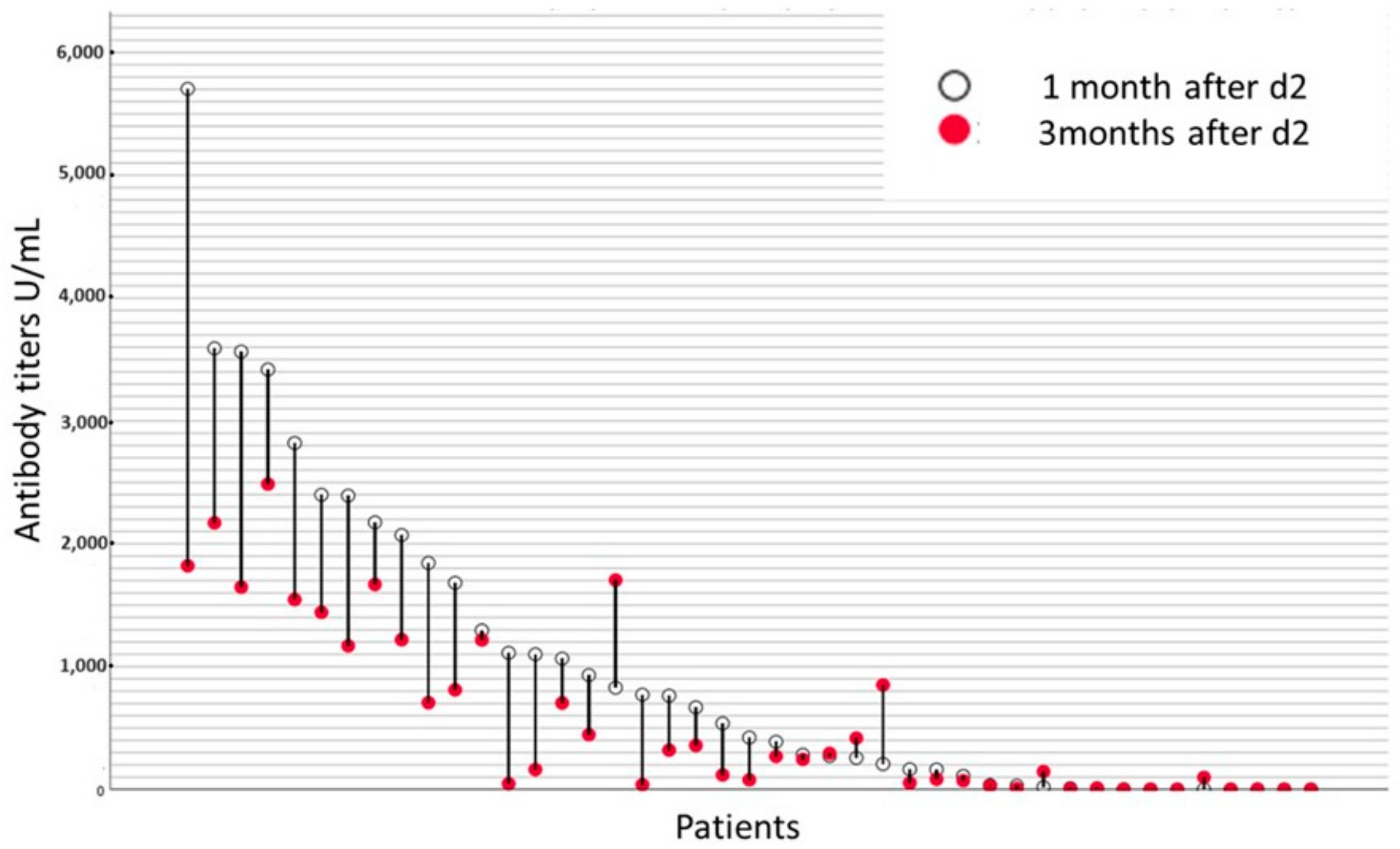
| PRESENT STUDY | 54 | 56 [19–71] | BOTH | 33 [6–60] | 28 and 90 | 1-m; 80.8 3-m; 85.7 | 1-m; 480.5 U/mL [0.4–25,000] 3-m; 293 U/mL [0.4–7869] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asimakopoulos, J.V.; Lalou, E.; Seferlis, G.; Malliarou, M.; Konstantinou, E.; Drandakis, I.; Vasilopoulos, I.; Georgopoulou, A.N.; Kopsaftopoulou, A.; Machairas, A.; et al. Monitoring Humoral Response Following BNT162b2 mRNA Vaccination against SARS-CoV-2 in Hematopoietic Stem-Cell Transplantation Patients: A Single-Center Prospective Study along with a Brief Review of Current Literature. Hematol. Rep. 2024, 16, 220-233. https://doi.org/10.3390/hematolrep16020022
Asimakopoulos JV, Lalou E, Seferlis G, Malliarou M, Konstantinou E, Drandakis I, Vasilopoulos I, Georgopoulou AN, Kopsaftopoulou A, Machairas A, et al. Monitoring Humoral Response Following BNT162b2 mRNA Vaccination against SARS-CoV-2 in Hematopoietic Stem-Cell Transplantation Patients: A Single-Center Prospective Study along with a Brief Review of Current Literature. Hematology Reports. 2024; 16(2):220-233. https://doi.org/10.3390/hematolrep16020022
Chicago/Turabian StyleAsimakopoulos, John V., Eleni Lalou, George Seferlis, Maria Malliarou, Eliana Konstantinou, Ioannis Drandakis, Ioannis Vasilopoulos, Angeliki N. Georgopoulou, Anastasia Kopsaftopoulou, Alexandros Machairas, and et al. 2024. "Monitoring Humoral Response Following BNT162b2 mRNA Vaccination against SARS-CoV-2 in Hematopoietic Stem-Cell Transplantation Patients: A Single-Center Prospective Study along with a Brief Review of Current Literature" Hematology Reports 16, no. 2: 220-233. https://doi.org/10.3390/hematolrep16020022
APA StyleAsimakopoulos, J. V., Lalou, E., Seferlis, G., Malliarou, M., Konstantinou, E., Drandakis, I., Vasilopoulos, I., Georgopoulou, A. N., Kopsaftopoulou, A., Machairas, A., Piperidou, A., Karapaschalidis, A., Lefaki, M.-E., Galopoulos, D., Arapaki, M.-P., Petsa, P., Benekou, E., Siakantaris, M. P., Papavassiliou, A. G., ... Angelopoulou, M. K. (2024). Monitoring Humoral Response Following BNT162b2 mRNA Vaccination against SARS-CoV-2 in Hematopoietic Stem-Cell Transplantation Patients: A Single-Center Prospective Study along with a Brief Review of Current Literature. Hematology Reports, 16(2), 220-233. https://doi.org/10.3390/hematolrep16020022