
Biomechanical Gait Analysis of an Adult with Severe Hemophilia: A Case Report

 and
and
Abstract
:1. Introduction
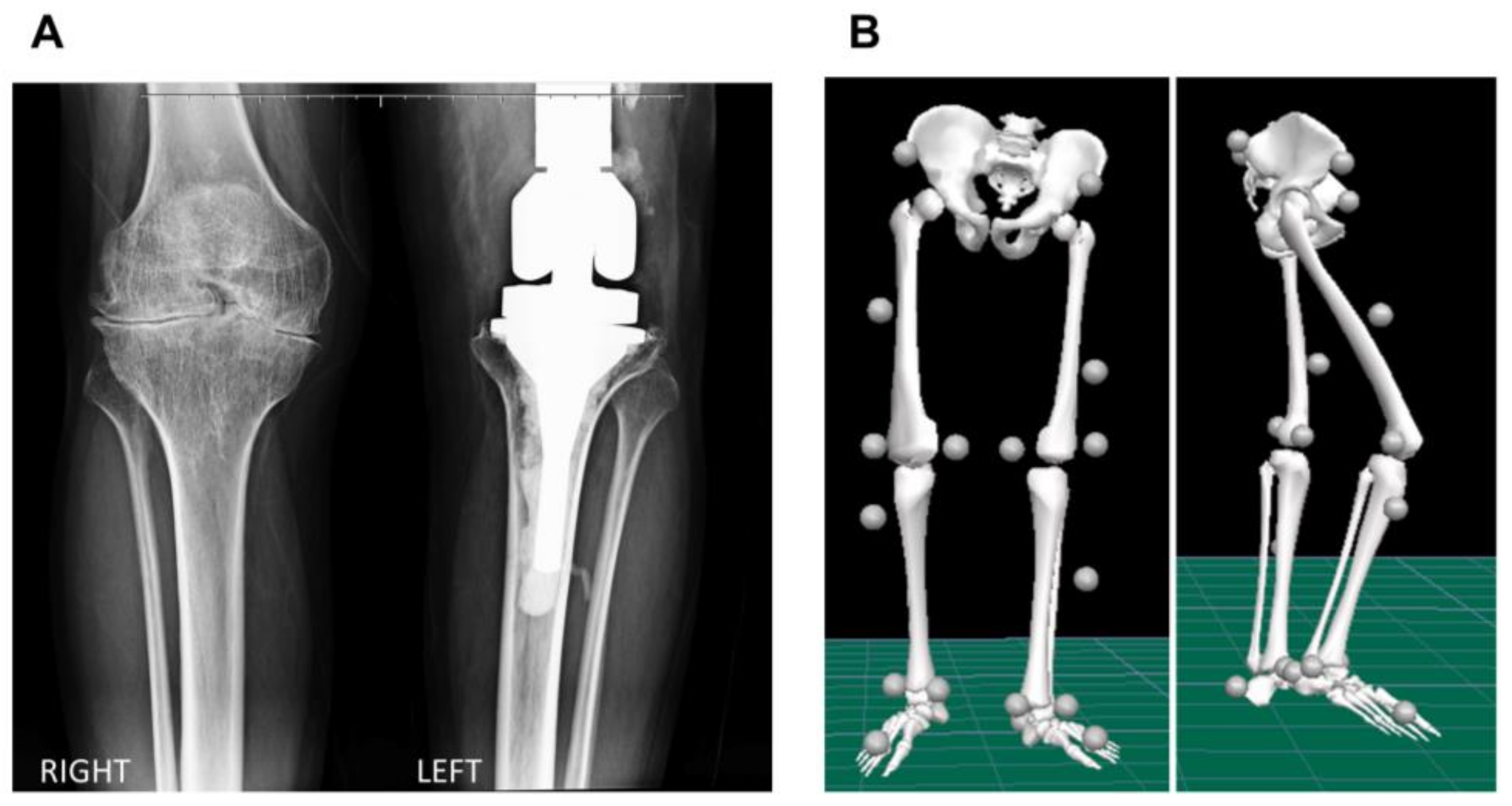
2. Case Report
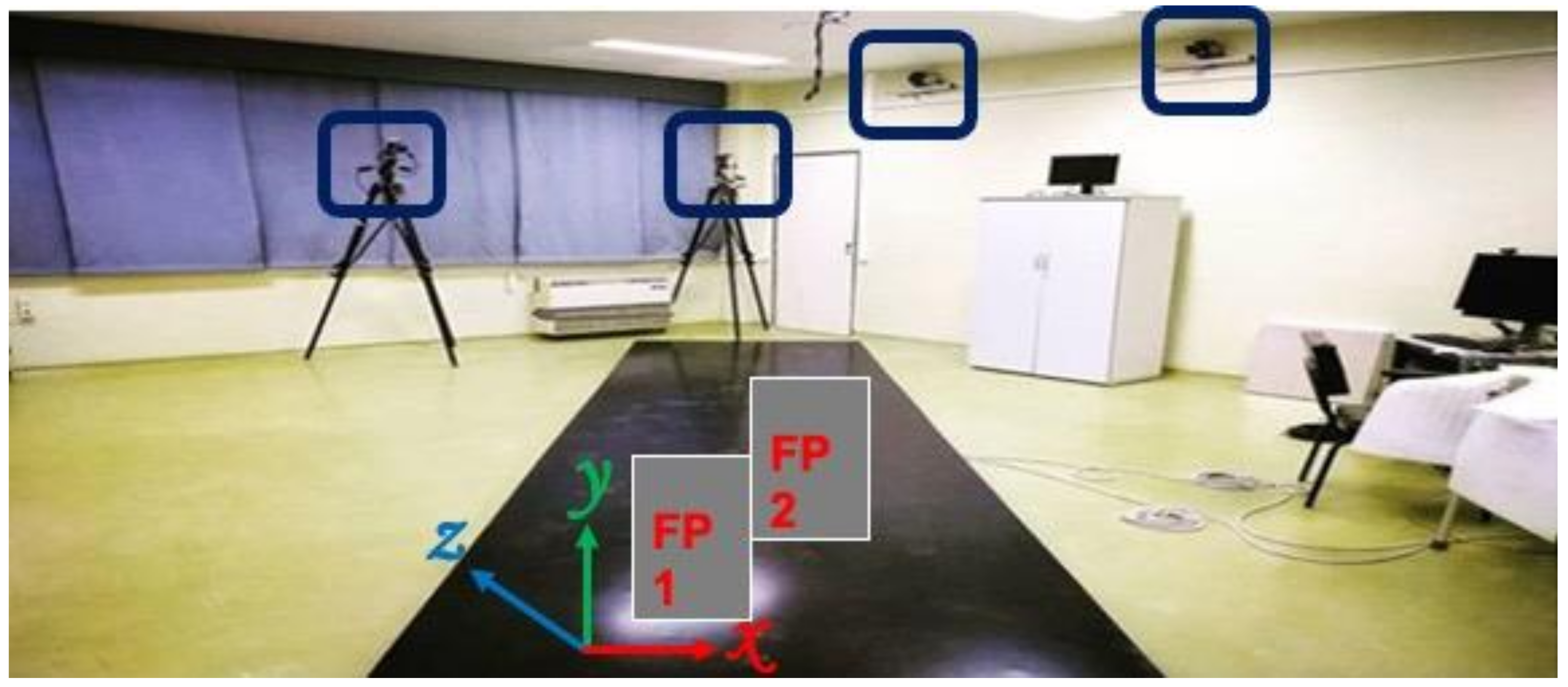
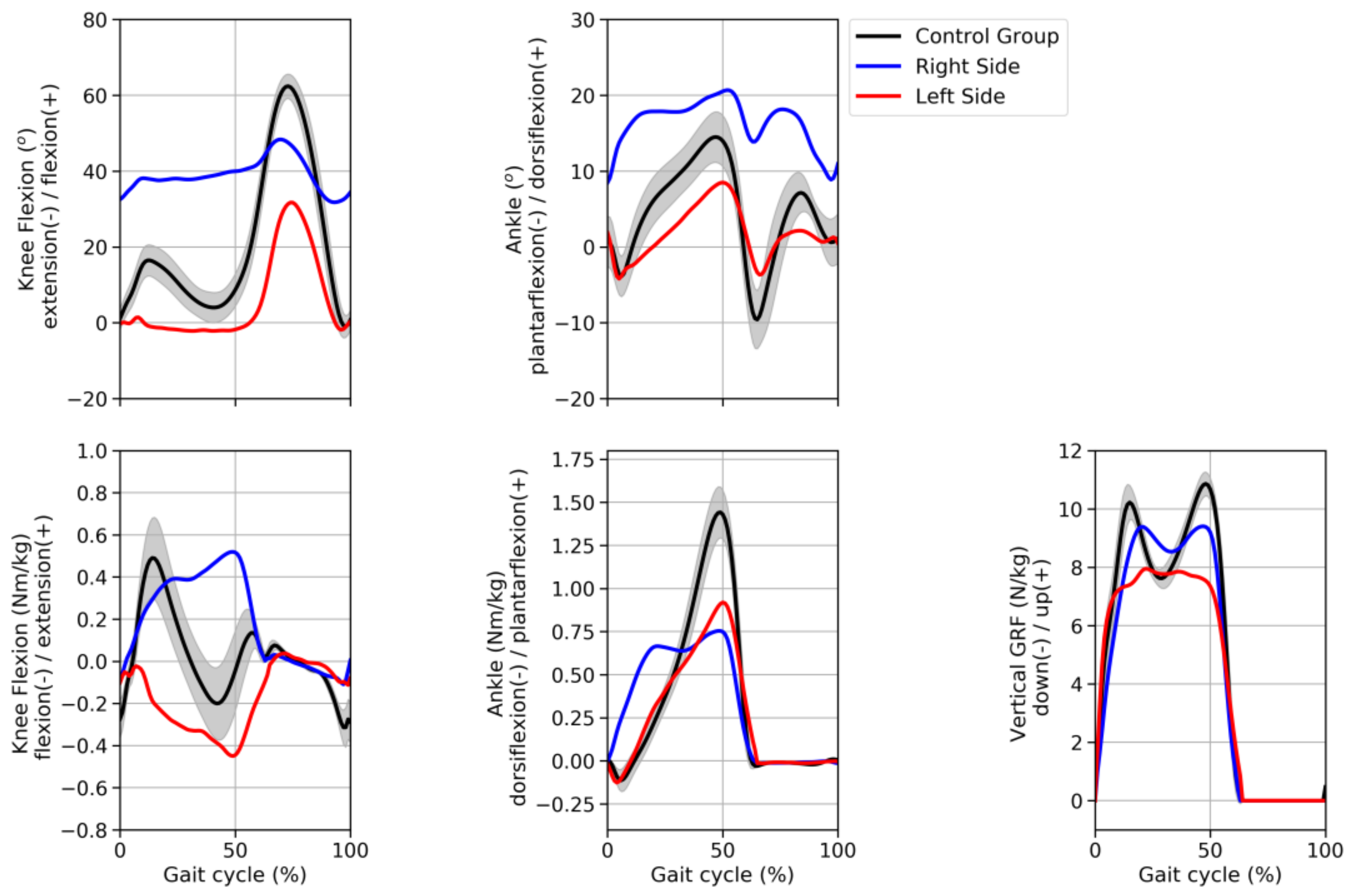
2.1. Biomechanical Assessment
2.2. Clinical Assessment
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tirunagari, S.; Shaik, D. Hemophilia and Acquired Hemophilia A. Webmed. Cent. Clin. Trials. 2013, 4, 1–12. [Google Scholar]
- Jansen, N.W.D.; Roosendaal, G.; Bijlsma, J.W.J.; De Groot, J.; Lafeber, F.P.J.G. Exposure of human cartilage tissue to low concentrations of blood for a short period of time leads to prolonged cartilage damage: An in vitro study. Arthritis Rheum. 2007, 56, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Feldman, B.M.; Rivard, G.E.; Babyn, P.; Wu, J.K.M.; Steele, M.; Poon, M.C.; Card, R.T.; Israels, S.J.; Laferriere, N.; Gill, K.; et al. Tailored frequency-escalated primary prophylaxis for severe haemophilia A: Results of the 16-year Canadian Hemophilia Prophylaxis Study longitudinal cohort. Lancet Haematol. 2018, 5, e252–e260. [Google Scholar] [CrossRef]
- Lafeber, F.; Miossec, P.; Valentino, L.A. Physiopathology of haemophilic arthropathy. Haemophilia 2008, 14, 3–9. [Google Scholar] [CrossRef]
- Wallny, T.; Lahaye, L.; Bracjmann, H.H.; Beß, L.; Seuser, A.; Kraft, C.N. Clinical and radiographic scores in haemophlic arthropathies: How well do these correlate to subjective pain status and daily activities? Haemophilia 2002, 8, 802–808. [Google Scholar] [CrossRef]
- Wallny, T.; Saker, A.; Hofmann, P.; Brackmann, H.H.; Nicolay, C.; Kraft, C.N. Long-term follow-up after osteotomy for haemophilic arthropathy of the knee. Haemophilia 2003, 9, 69–75. [Google Scholar] [CrossRef]
- Tusell, J.M.; Aznar, J.A.; Querol, F.; Quintana, M.; Moreno, M.; Gorina, E.; The Orthopaedic Study Group. Results of an orthopaedic survey in young patients with severe haemophilia in Spain. Haemophilia 2002, 8, 38–42. [Google Scholar] [CrossRef]
- Wren, T.A.L.; Gorton, G.E.; Ounpuu, S.; Tucker, C.A. Efficacy of clinical gait analysis: A systematic review. Gait Posture 2011, 34, 149–153. [Google Scholar] [CrossRef]
- Wren, T.A.L.; Otsuka, N.Y.; Bowen, R.E.; Scaduto, A.A.; Chan, L.S.; Sheng, M.; Hara, R.; Kay, R.M. Influence of gait analysis on decision-making for lower extremity orthopaedic surgery: Baseline data from a randomized controlled trial. Gait Posture 2011, 34, 364–369. [Google Scholar] [CrossRef]
- Fouasson-Chailloux, A.; Maugars, Y.; Vinatier, C.; Trossaert, M.; Menu, P.; Rannou, F.; Guicheux, J.; Dauty, M. Clinical relevance of 3D gait analysis in patients with haemophilia. Haemophilia 2018, 24, 703–710. [Google Scholar] [CrossRef]
- Bladen, M.; Alderson, L.; Khair, K.; Liesner, R.; Green, J.; Main, E. Can early subclinical gait changes in children with haemophilia be identified using the GAITRite® walkway. Haemophilia 2007, 13, 542–547. [Google Scholar] [CrossRef] [PubMed]
- Filho, D.J.; Battistella, L.R.; Lourenço, C. Computerized pedobarography in the characterization of ankle-foot instabilities of haemophilic patients. Haemophilia 2006, 12, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Putz, P.; Durstberger, S.; Kaufmann, C.; Klinger, M.; Plessl, K.; Rejtö, J.; Widhalm, K.; Male, C.; Pabinger, I. 3D gait analysis, haemophilia joint health score, leg muscle laterality and biomarkers of joint damage: A cross-sectional comparative assessment of haemophilic arthropathy. Haemophilia 2020, 26, e323–e333. [Google Scholar] [CrossRef]
- Lobet, S.; Detrembleur, C.; Francq, B.; Hermans, C. Natural progression of blood-induced joint damage in patients with haemophilia: Clinical relevance and reproducibility of three-dimensional gait analysis. Haemophilia 2010, 16, 813–821. [Google Scholar] [CrossRef] [PubMed]
- Lobet, S.; Hermans, C.; Bastien, G.J.; Massaad, F.; Detrembleur, C. Impact of ankle osteoarthritis on the energetics and mechanics of gait: The case of hemophilic arthropathy. Clin. Biomech. 2012, 27, 625–631. [Google Scholar] [CrossRef]
- Lobet, S.; Detrembleur, C.; Hermans, C. Impact of multiple joint impairments on the energetics and mechanics of walking in patients with haemophilia. Haemophilia 2013, 19, 66–72. [Google Scholar] [CrossRef]
- Lobet, S.; Detrembleur, C.; Massaad, F.; Hermans, C. Three-dimensional gait analysis can shed new light on walking in patients with haemophilia. Sci. World J. 2013, 2013, 284358. [Google Scholar] [CrossRef] [Green Version]
- Alton, F.; Baldey, L.; Caplan, S.; Morrissey, M.C. A kinematic comparison of overground and treadmill walking. Clin. Biomech. 1998, 13, 434–440. [Google Scholar] [CrossRef]
- Fukuchi, C.A.; Fukuchi, R.K.; Duarte, M. A public dataset of overground and treadmill walking kinematics and kinetics in healthy individuals. PeerJ 2018, 6, e4640. [Google Scholar] [CrossRef] [Green Version]
- Row Lazzarini, B.S.; Kataras, T.J. Treadmill walking is not equivalent to overground walking for the study of walking smoothness and rhythmicity in older adults. Gait Posture 2016, 46, 42–46. [Google Scholar] [CrossRef]
- Simons, M.R.; Tawy, G.; Rowe, P.; Gleeson, N.; Biant, L.C. Correlation of muscle strength and gait stability in patients with end stage osteoarthritis. Knee 2017, 24, VII. [Google Scholar] [CrossRef]
- Zhao, D.; Banks, S.A.; Mitchell, K.H.; D’Lima, D.D.; Colwell, C.W., Jr.; Fregly, B.J. Correlation between the Knee Adduction Torque and Medial Contact Force for a Variety of Gait Patterns Dong. J. Orthop. Res. Sept. 2007, 25, 789–797. [Google Scholar] [CrossRef] [PubMed]
- Stephensen, D.; Drechsler, W.I.; Scott, O.M. Influence of ankle plantar flexor muscle architecture and strength on gait in boys with haemophilia in comparison to typically developing children. Haemophilia 2014, 20, 413–420. [Google Scholar] [CrossRef]
- Stephensen, D.; Drechsler, W.; Winter, M.; Scott, O. Comparison of biomechanical gait parameters of young children with haemophilia and those of age-matched peers. Haemophilia 2009, 15, 509–518. [Google Scholar] [CrossRef] [PubMed]
- Stephensen, D.; Taylor, S.; Bladen, M.; Drechsler, W.I. Relationship between physical function and biomechanical gait patterns in boys with haemophilia. Haemophilia 2016, 22, e512–e518. [Google Scholar] [CrossRef] [PubMed]
- Davari, M.; Gharibnaseri, Z.; Ravanbod, R.; Sadeghi, A. Health status and quality of life in patients with severe hemophilia A: A cross-sectional survey. Hematol. Rep. 2019, 11, 39–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukuchi, C.A.; Fukuchi, R.K.; Duarte, M. Effects of walking speed on gait biomechanics in healthy participants: A systematic review and meta-analysis. Syst Rev. 2019, 8, 153. [Google Scholar] [CrossRef] [Green Version]
- Simon, S.R. Quantification of human motion: Gait analysis—benefits and limitations to its application to clinical problems. J. Biomech. 2004, 37, 1869–1880. [Google Scholar] [CrossRef]
- Baker, R.; McGinley, J.; Schwartz, M.; Beynon, S.; Rozumalski, A.; Graham, H.; Tirosh, O. The gait profile score and movement analysis profile. Gait Posture 2009, 30, 265–269. [Google Scholar] [CrossRef]
- Schwartz, M.H.; Rozumalski, A. The Gait Deviation Index: A New Comprehensive Index of Gait Pathology. Gait Posture 2008, 28, 351–357. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Elbow | Knee | Ankle | ||||
|---|---|---|---|---|---|---|
| Left | Right | Left | Right | Left | Right | |
| Flexion (°) | 134 | 112 | 78 | 60 | 36 | 46 |
| Extension (°) | −32 | −45 | 0 | −36 | 13 | −2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fukuchi, C.A.; Zorzi, A.R.; Fukuchi, R.K.; Ricciardi, J.B.S.; Feldberg, G.; Cliquet, A., Jr. Biomechanical Gait Analysis of an Adult with Severe Hemophilia: A Case Report. Hematol. Rep. 2022, 14, 112-118. https://doi.org/10.3390/hematolrep14020017
Fukuchi CA, Zorzi AR, Fukuchi RK, Ricciardi JBS, Feldberg G, Cliquet A Jr. Biomechanical Gait Analysis of an Adult with Severe Hemophilia: A Case Report. Hematology Reports. 2022; 14(2):112-118. https://doi.org/10.3390/hematolrep14020017
Chicago/Turabian StyleFukuchi, Claudiane A., Alessandro R. Zorzi, Reginaldo K. Fukuchi, Janaina B. S. Ricciardi, Glenda Feldberg, and Alberto Cliquet, Jr. 2022. "Biomechanical Gait Analysis of an Adult with Severe Hemophilia: A Case Report" Hematology Reports 14, no. 2: 112-118. https://doi.org/10.3390/hematolrep14020017
APA StyleFukuchi, C. A., Zorzi, A. R., Fukuchi, R. K., Ricciardi, J. B. S., Feldberg, G., & Cliquet, A., Jr. (2022). Biomechanical Gait Analysis of an Adult with Severe Hemophilia: A Case Report. Hematology Reports, 14(2), 112-118. https://doi.org/10.3390/hematolrep14020017