
Detection of Red Blood Cell Membrane Proteins in Myelodysplastic Syndromes Using Eosin-5-Maleimide (EMA) Staining by Flow Cytometry

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
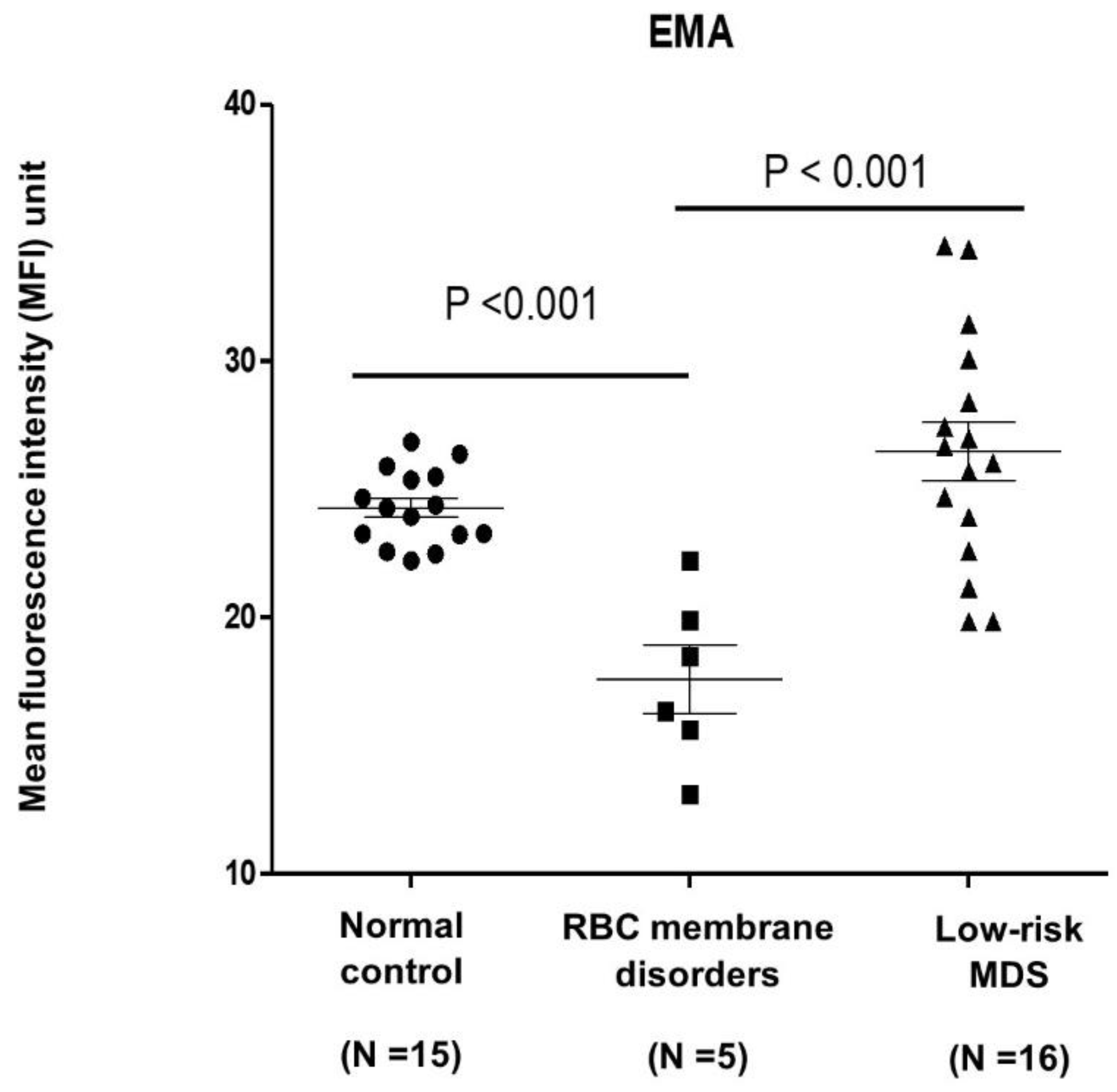
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Castelli, R.; Schiavon, R.; Rossi, V.; Deliliers, G.L. Management of anemia in low-risk myelodysplastic syndromes treated with erythropoiesis-stimulating agents newer and older agents. Med Oncol. 2018, 35, 76. [Google Scholar] [CrossRef] [PubMed]
- Cazzola, M.; Barosi, G.; Berzuini, C.; Dacco, M.; Orlandi, E.; Stefanelli, M.; Ascari, E. Quantitative evaluation of erythropoietic activity in dysmyelopoietic syndromes. Br. J. Haematol. 1982, 50, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Liu, J.; Xue, F.; Halverson, G.; Reid, M.; Guo, A.; Chen, L.; Raza, A.; Galili, N.; Jaffray, J.; et al. Isolation and functional characterization of human erythroblasts at distinct stages: Implications for understanding of normal and disordered erythropoiesis in vivo. Blood 2013, 121, 3246–3253. [Google Scholar] [CrossRef] [PubMed]
- Komrokji, R.S.; Al Ali, M.N.; Hussaini, M.O.; Sallman, D.A.; Rollison, D.E.; Padron, E. U2AF1 and EZH2 Mutations Are Associated with Non-Immune Hemolytic Anemia in Myelodysplastic Syndromes. Blood 2020, 136, 35–36. [Google Scholar] [CrossRef]
- Glenthøj, A.; Sharfo, A.; Brieghel, C.; Nardo-Marino, A.; Birgens, H.; Petersen, J.B. Improving the EMA Binding Test by Using Commercially Available Fluorescent Beads. Front. Physiol. 2020, 11, 569289. [Google Scholar] [CrossRef]
- Picard, V.; Proust, A.; Eveillard, M.; Flatt, J.F.; Couec, M.-L.; Caillaux, G.; Feneant-Thibault, M.; Finkelstein, A.; Raphael, M.; Delaunay, J.; et al. Homozygous Southeast Asian ovalocytosis is a severe dyserythropoietic anemia associated with distal renal tubular acidosis. Blood 2014, 123, 1963–1965. [Google Scholar] [CrossRef] [PubMed]
- King, M.-J.; Smythe, J.S.; Mushens, R. Eosin-5-maleimide binding to band 3 and Rh-related proteins forms the basis of a screening test for hereditary spherocytosis. Br. J. Haematol. 2004, 124, 106–113. [Google Scholar] [CrossRef]
- Adan, A.; Alizada, G.; Kiraz, Y.; Baran, Y.; Nalbant, A. Flow cytometry: Basic principles and applications. Crit. Rev. Biotechnol. 2016, 37, 163–176. [Google Scholar] [CrossRef] [PubMed]
- Arber, D.A.; Orazi, A.; Hasserjian, R.; Thiele, J.; Borowitz, M.J.; Le Beau, M.M.; Bloomfield, C.D.; Cazzola, M.; Vardiman, J.W. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood 2016, 127, 2391–2405. [Google Scholar] [CrossRef] [PubMed]
- Park, S.H.; Park, C.-J.; Lee, B.-R.; Cho, Y.-U.; Jang, S.; Kim, N.; Koh, K.-N.; Im, H.-J.; Seo, J.-J.; Park, E.S.; et al. Comparison Study of the Eosin-5′-Maleimide Binding Test, Flow Cytometric Osmotic Fragility Test, and Cryohemolysis Test in the Diagnosis of Hereditary Spherocytosis. Am. J. Clin. Pathol. 2014, 142, 474–484. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.M.; Huang, Y.; Pinheiro, R.F.; Xue, F.; Hu, J.; Iverson, N.; Hoehn, D.; Coutinho, D.; Kayani, J.; Chernak, B.; et al. Severely impaired terminal erythroid differentiation as an independent prognostic marker in myelodysplastic syndromes. Blood Adv. 2018, 2, 1393–1402. [Google Scholar] [CrossRef]
- Ciepiela, O.; Adamowicz-Salach, A.; Bystrzycka, W.; Łukasik, J.; Kotuła, I. Mean corpuscular volume of control red blood cells determines the interpretation of eosin-5′-maleimide (EMA) test result in infants aged less than 6 months. Ann. Hematol. 2015, 94, 1277–1283. [Google Scholar] [CrossRef]
- Falay, M.; Ulusan, G.E.; Şenes, M.; Acar, İ.O. Are the Reference Ranges and Cutoff Values of Eosin-5′-Maleimide (EMA) Binding Test for Hereditary Spherocytosis Specific for Each Age Group? Clin. Lab. 2018, 64, 1101–1103. [Google Scholar] [CrossRef]


{kind=link}
| Control (N = 16) | MDS (N = 15) | RBC Membrane Disorders (N = 6) | p-Value | |
|---|---|---|---|---|
| Median (IQR) age (years) | 28 (27–30) | 76 (67–82) | 36 (27–45) | <0.001 |
| Gender, N (%) | 0.07 | |||
| Female | 11 (73.3) | 5 (31.3) | 4(66.7) | |
| Male | 4 (26.7) | 11 (68.7) | 2 (33.3) | |
| Hemoglobin (g/dL) | 13 (1.0) | 8.6 (1.8) | 10.3 (3.2) | <0.001 |
| MCV (fL) | 86.2 (5.7) | 92.5 (17.1) | 85.2 (6.8) | 0.62 |
| MCH (pg) | 28.7 (2.3) | 29.5 (5.6) | 29.6 (2.6) | 0.77 |
| MCHC (g/dl) | 33.2 (0.7) | 31.9 (1.3) | 34.2 (1.4) | <0.001 |
| RDW (%) | 12.8 (0.7) | 18.5 (3.9) | 18.6 (4.3) | <0.001 |
| Unadjusted | Adjusted * | |||
|---|---|---|---|---|
| Mean Difference (95%CI) | p-Value | Mean Difference (95%CI) | p-Value | |
| Group | ||||
| Normal | Ref. | Ref. | Ref. | Ref. |
| MDS | 2.2 (−0.18 to 4.58) | 0.08 | 1.5 (−6.07 to 9.17) | 0.68 |
| HS | −6.7 (−10.03 to −3.34) | <0.001 | −6.87 (−10.48 to −3.26) | 0.001 |
| ณNo. | 1 | 2 | 3 | 4 | 5 | Mean (SD) | 6 |
|---|---|---|---|---|---|---|---|
| Group | HS | HS | HS | HS | HS | - | SAO |
| Age | 26 | 47 | 27 | 32 | 40 | 34.4 (8.9) | 45 |
| Gender | Female | Female | Female | Male | Male | - | Female |
| Hb (g/dL) | 9.2 | 10.4 | 10.2 | 8.8 | 16.4 | 11 (3.1) | 7 |
| MCV (fL) | 81 | 87.6 | 73.3 | 90.4 | 89 | 84.3 (7.1) | 90 |
| MCH (pg) | 27.8 | 29.7 | 25.7 | 29.9 | 32.7 | 29.2 (2.6) | 32 |
| MCHC (g/dl) | 33.1 | 33.9 | 35.1 | 33 | 36.8 | 34.4 (1.6) | 33 |
| RDW (%) | 21.1 | 19.6 | 23.4 | 20.7 | 12.5 | 19.5 (4.1) | 14 |
| PLT | 250 | 237 | 211 | 286 | 328 | 262 (45.5) | 160.2 |
| (×103 cell/mm3) | |||||||
| WBC (cell/mm3) | 11,300 | 8320 | 9820 | 7010 | 6590 | 8608 (1.9) | 9600 |
| EMA | 22.23 | 16.35 | 18.48 | 19.88 | 13.09 | 18.01 (3.5) | 15.62 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uman, N.; Kobbuaklee, S.; Kansuwan, P.; Watanaboonyongcharoen, P.; Polprasert, C. Detection of Red Blood Cell Membrane Proteins in Myelodysplastic Syndromes Using Eosin-5-Maleimide (EMA) Staining by Flow Cytometry. Hematol. Rep. 2022, 14, 13-18. https://doi.org/10.3390/hematolrep14010003
Uman N, Kobbuaklee S, Kansuwan P, Watanaboonyongcharoen P, Polprasert C. Detection of Red Blood Cell Membrane Proteins in Myelodysplastic Syndromes Using Eosin-5-Maleimide (EMA) Staining by Flow Cytometry. Hematology Reports. 2022; 14(1):13-18. https://doi.org/10.3390/hematolrep14010003
Chicago/Turabian StyleUman, Navavee, Sirorat Kobbuaklee, Patsita Kansuwan, Phandee Watanaboonyongcharoen, and Chantana Polprasert. 2022. "Detection of Red Blood Cell Membrane Proteins in Myelodysplastic Syndromes Using Eosin-5-Maleimide (EMA) Staining by Flow Cytometry" Hematology Reports 14, no. 1: 13-18. https://doi.org/10.3390/hematolrep14010003
APA StyleUman, N., Kobbuaklee, S., Kansuwan, P., Watanaboonyongcharoen, P., & Polprasert, C. (2022). Detection of Red Blood Cell Membrane Proteins in Myelodysplastic Syndromes Using Eosin-5-Maleimide (EMA) Staining by Flow Cytometry. Hematology Reports, 14(1), 13-18. https://doi.org/10.3390/hematolrep14010003