COVID-19 in Patients with Transfusion Dependent Thalassemia (TDT) in Indonesia: Characteristics of the Disease and Patients, and Comparison between Epidemiological Data for COVID-19 and Thalassemia in Indonesia and Southeast Asia


Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Coronavirus. 2021. Available online: https://www.who.int/health-topics/coronavirus#tab=tab_1 (accessed on 18 February 2021).
- Indonesian Thalassemia Foundation (POPTI). Report on The Number of People Living with Thalassemia in Indonesia; Indonesian Thalassemia Foundation: Jakarta, Indonesia, 2020; unpublished report. [Google Scholar]
- Atmakusuma, D.; Eleftheriou, A.; Skafi, A.; Loriz Brunetta, A. Meet the Experts: COVID-19 Vaccines for Thalassemia Survivor: Do’s and Dont’s; Hematology Reports: 13:9379; PAGE Press: Pavia, Italy, 2021. [Google Scholar]
- Eleftheriou, A.; Angastiniotis, M. Global Thalassemia Review; Thalassaemia International Federation: Nicosia, Cyprus, 2021. [Google Scholar]
- Lansiaux, E.; Pebay, P.P.; Picard, J.L.; Son-Forget, J. COVID-19: Beta-thalassemia subjects immunised? Med. Hypotheses 2020, 142, 109827. [Google Scholar] [CrossRef] [PubMed]
- CSIS. Southeast Asia COVID-19 Tracker. Available online: https://www.csis.org/programs/southeast-asia-program/projects/southeast-asia-covid-19-tracker (accessed on 18 February 2021).
- De Sanctis, V.; Canatan, D.; Corrons, J.L.V.; Karimi, M.; Daar, S.; Kattamis, C.; Kilinc, Y. A comprehensive update of ICET-A Network on COVID-19 in thalassemias: What we know and where we stand. Acta Bio Med. 2020, 91, e2020026. [Google Scholar]
- Papadopoulos, K.I.; Sutheesophon, W.; Manipalviratn, S.; Aw, T.C. A Southeast Asian Perspective on the COVID-19 Pandemic: Hemoglobin E (HbE)-Trait Confers Resistance Against COVID-19. Med. Sci. Monit. Basic Res. 2021, 27, e929207. [Google Scholar] [CrossRef] [PubMed]
- Weatherall, D.J.; Clegg, J.B. The Thalassaemia Syndromes; Blackwell Science Ltd.: Hoboken, NJ, USA, 2001. [Google Scholar]
- Marhaeni, W.; Wijaya, A.B.; Kusumaningtyas, P.; Mapianto, R.S. Thalassemic Child Presenting with Anosmia due to COVID-19. Indian J. Pediatr. 2020, 87, 750. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.L.H. COVID-19: Attacks the 1-Beta Chain of Hemoglobin and Captures the Porphyrin to Inhibit Human Heme Metabolism. ChemRxiv 2020. [Google Scholar] [CrossRef]
- Torti, L.; Maffei, L.; Sorrentino, F.; De Fabritiis, P.; Miceli, R.; Abruzzese, E. Impact of SARS CoV-2 in Hemoglobinopathies with Immune Disfunction and Epidemiology. A Protective Mechanism from Beta Chain Hemoglobin Defects? Mediterr. J. Hematol. Infect. Dis. 2020, 12, e2020052. [Google Scholar] [CrossRef] [PubMed]
- Farmakis, D.; Giakoumis, A.; Polymeropoulo, E.; Aessopos, A. Pathogenetic aspects of immune deficiency associated with beta-thalassemia. Med. Sci. Monit. 2003, 9, 19–22. [Google Scholar]
- Ye, Q.; Wang, B.; Mao, J. The pathogenesis and treatment of the ‘Cytokine Storm’ in COVID-19. J. Infect. 2020, 80, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Okar, L.; Ali, M.; Parengal, J.; Yassin, M.A. COVID-19 and thalassemia beta major in splenectomized patient: Clinical case progression and literature review. Clin. Case Rep. 2020, 8, 2918–2922. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, S.F.; Anwar, S. Management of Hemoglobin Disorders During the COVID-19 Pandemic. Front. Med. 2020, 7, 306. [Google Scholar] [CrossRef] [PubMed]
- Karimi, M.; De Sanctis, V. Implications of SARSr-CoV 2 infection in thalassemias: Do patients fall into the “high clinical risk” category? Acta Bio Med. 2020, 91, 50–56. [Google Scholar]
- Zietz, M.; Zucker, J.; Tatonetti, N.P. Testing the association between blood type and COVID-19 infection, intubation, and death. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| General Characteristic | N = 66 |
|---|---|
| Gender, n (%) | |
| Male | 29 (43.3) |
| Female | 37 (56.7) |
| Age, n (%) | |
| 3.0–18.0 | 30 (44.8) |
| 19.0–40.0 | 26 (38.8) |
| 41.0–60.0 | 10 (16.4) |
| Blood Type, n (%) | |
| A (+) | 20 (29.9) |
| AB (+) | 10 (14.9) |
| B (+) | 14 (20.9) |
| O (+) | 23 (34.3) |
| Ethnicity, n (%) | |
| Bataknese | 1 (1.4) |
| Bengkulu | 1 (1.4) |
| Betawi | 14 (20.8) |
| Buginese | 1 (1.4) |
| Chinese | 2 (2.9) |
| Javanese | 24 (35.8) |
| Lampung | 1 (1.4) |
| Medan | 2 (2.9) |
| Malay | 2 (2.9) |
| Minang | 1 (1.4) |
| Sundanese | 18 (26.8) |
| Thalassemia Type, n (%) | |
| Alfa 3 deletion | 2 (3.0) |
| Beta Intermedia | 1 (1.5) |
| Beta HbE TDT | 19 (28.4) |
| Beta Mayor | 44 (65.7) |
| Beta minor | 1 (1.5) |
| COVID-19 clinical severity, n (%) | |
| Asymptomatic | 31 (46.3) |
| Mild | 32 (47.8) |
| Moderate | 4 (6.0) |
| Severe | 0 (0.0) |
| Outcome, n (%) | |
| Deceased | 2 (2.9) |
| Recovered | 65 (97.1) |
| Vaccination Status Prior to COVID-19 infection, n (%) | |
| Already | 3 (4.2) |
| Not Done | 66 (91.7) |
| Patient’s Characteristics | COVID-19 Status | p-Value | |
|---|---|---|---|
| Survive | Deceased | ||
| Gender, n | |||
| Male | 29 | 0 | 0.318 |
| Female | 36 | 2 | |
| Age Group, n | |||
| 3–18 | 30 | 0 | 0.300 |
| 19–40 | 25 | 1 | |
| 41–60 | 10 | 1 | |
| Blood Type, n | |||
| A (+) | 19 | 1 | 0.374 |
| AB (+) | 14 | 0 | |
| B (+) | 9 | 1 | |
| O (+) | 23 | 0 | |
| Thalassemia Type, n | |||
| Alfa 3 deletion | 2 | 0 | 0.898 |
| Beta Intermedia | 1 | 0 | |
| Beta HbE TDT | 19 | 0 | |
| Beta Mayor | 42 | 2 | |
| Beta minor | 1 | 0 | |
| COVID-19 Clinical Severity | |||
| Asymptomatic | 30 | 1 | 0.021 |
| Mild | 32 | 0 | |
| Moderate | 3 | 1 | |
| Severe | 0 | 0 | |
| Vaccination Status Prior to COVID-19 Infection | |||
| Already | 3 | 0 | 0.912 |
| Not Done | 62 | 2 | |
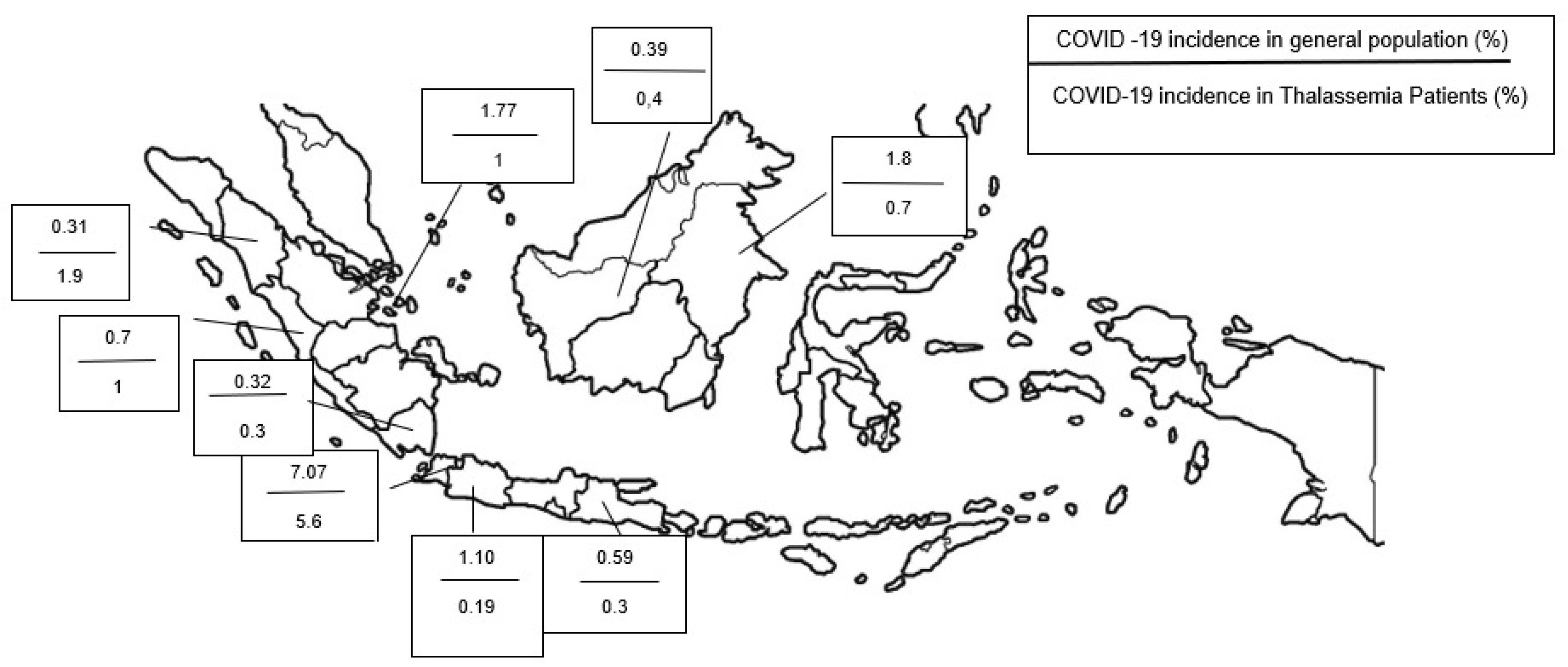
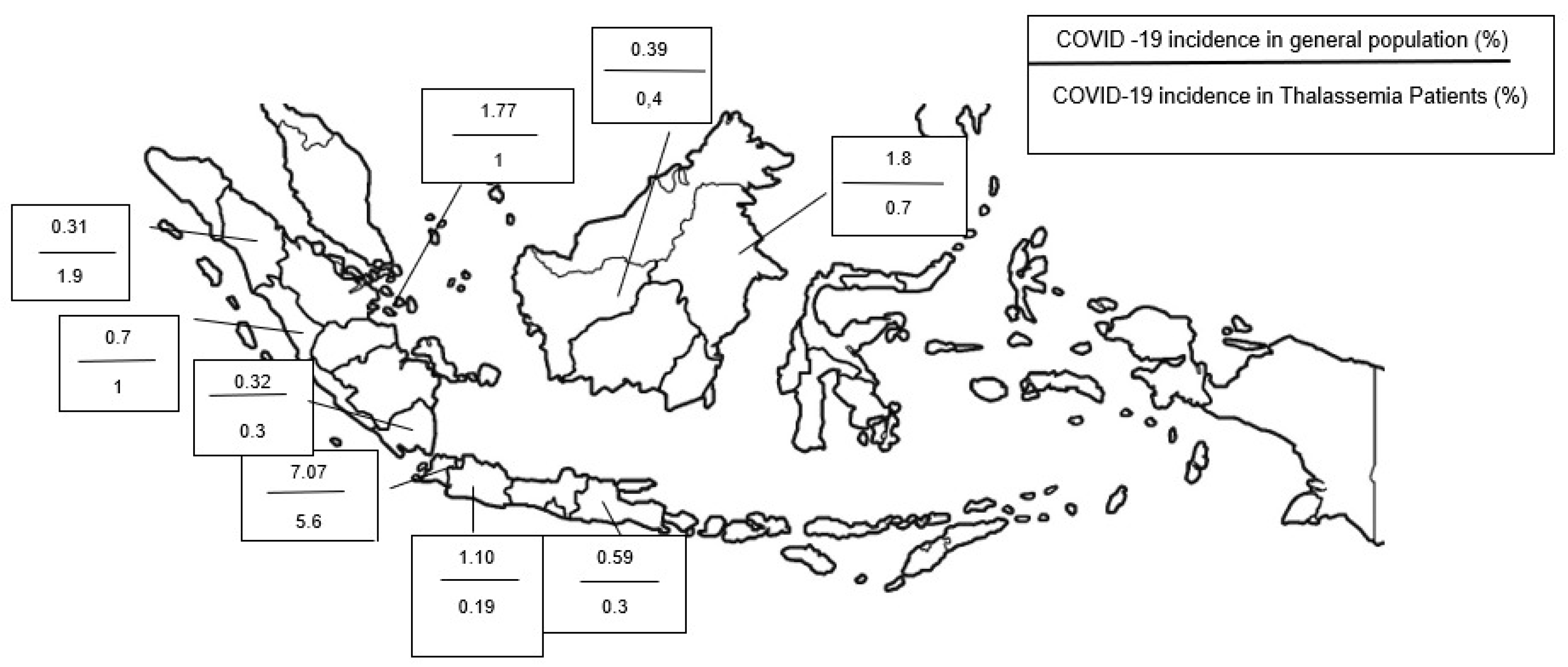
| No | Province | Total Population | Total TDT Patient | Prevalence of TDT/Population | Total COVID Cases in General Population | TDT Patients with COVID-19 | TDT Patients with COVID-19 (%) | Mortality in TDT Patients with COVID-19 |
|---|---|---|---|---|---|---|---|---|
| 1 | ACEH | 5,274,871 | 631 | 0.0120% | 20,949 | 0 | 0% | 0 |
| 2 | NORTH SUMATRA | 14,799,361 | 162 | 0.0011% | 46,053 | 3 | 1.9% | 1 |
| 3 | WEST SUMATRA | 5,534,472 | 22 | 0.0004% | 61,350 | 0 | 0% | 0 |
| 4 | RIAU | 6,394,087 | 97 | 0.0015% | 83,628 | 0 | 0% | 0 |
| 5 | JAMBI | 3,548,228 | 54 | 0.0015% | 16,443 | 0 | 0% | 0 |
| 6 | SOUTH SUMATRA | 8,467,432 | 332 | 0.0039% | 37,917 | 0 | 0% | 0 |
| 7 | BENGKULU | 2,010,670 | 100 | 0.0050% | 14,003 | 1 | 1.0% | 0 |
| 8 | LAMPUNG | 9,007,848 | 316 | 0.0035% | 29,078 | 1 | 0.3% | 0 |
| 9 | BANGKA BELITUNG ISLANDS | 1,455,678 | 117 | 0.0080% | 26,778 | 0 | 0% | 0 |
| 10 | RIAU ISLANDS | 2,064,564 | 97 | 0.0047% | 36,581 | 1 | 1.0% | 0 |
| 11 | DKI JAKARTA | 10,562,088 | 864 | 0.0082% | 746,306 | 49 | 5.6% | 1 |
| 12 | WEST JAVA | 48,274,162 | 4164 | 0.0086% | 530,806 | 8 | 0.19% | 0 |
| 13 | CENTRAL JAVA | 36,516,035 | 1449 | 0.0040% | 329,216 | 0 | 0% | 0 |
| 14 | DI YOGYAKARTA | 3,668,719 | 165 | 0.0045% | 92,085 | 0 | 0% | 0 |
| 15 | EAST JAVA | 40,665,696 | 695 | 0.0017% | 239,168 | 2 | 0.3% | 0 |
| 16 | BANTEN | 11,904,562 | 654 | 0.0055% | 92,746 | 0 | 0% | 0 |
| 17 | BALI | 4,317,404 | 23 | 0.0005% | 61,175 | 0 | 0% | 0 |
| 18 | WEST NUSA TENGGARA | 5,320,092 | 26 | 0.0005% | 16,331 | 0 | 0% | 0 |
| 19 | EAST NUSA TENGGARA | 5,325,566 | 0 | 0% | 26,363 | 0 | 0% | 0 |
| 20 | WEST KALIMANTAN | 5,414,390 | 234 | 0.0043% | 21,149 | 1 | 0.4% | 0 |
| 21 | CENTRAL BORNEO | 2,669,969 | 38 | 0.0014% | 30,347 | 0 | 0% | 0 |
| 22 | SOUTH BORNEO | 4,073,584 | 157 | 0.0039% | 40,029 | 0 | 0% | 0 |
| 23 | EAST KALIMANTAN | 3,766,039 | 137 | 0.0036% | 96,564 | 1 | 0.72% | 0 |
| 24 | NORTH KALIMANTAN | 701,814 | 0 | 0% | 16,286 | 0 | 0% | 0 |
| 25 | NORTH SULAWESI | 2,621,923 | 0 | 0% | 19,718 | 0 | 0% | 0 |
| 26 | CENTRAL SULAWESI | 2,985,734 | 0 | 0% | 16,792 | 0 | 0% | 0 |
| 27 | SOUTH SULAWESI | 9,073,509 | 61 | 0.0007% | 72,240 | 0 | 0% | 0 |
| 28 | SOUTHEAST SULAWESI | 2,624,875 | 0 | 0% | 13,817 | 0 | 0% | 0 |
| 29 | GORONTALO | 1,171,681 | 0 | 0% | 6948 | 0 | 0% | 0 |
| 30 | WEST SULAWESI | 1,419,229 | 0 | 0% | 7113 | 0 | 0% | 0 |
| 31 | MALUKU | 1,848,923 | 0 | 0% | 12,127 | 0 | 0% | 0 |
| 32 | NORTH MALUKU | 1,282,937 | 0 | 0% | 8204 | 0 | 0% | 0 |
| 33 | WEST PAPUA | 1,134,068 | 0 | 0% | 15,904 | 0 | 0% | 0 |
| 34 | PAPUA | 4,303,707 | 0 | 0% | 23,826 | 0 | 0% | 0 |
| Total | 270,203,917 | 10,397 | 0.089% | 2,908,040 | 67 | 11.21% | 2 |
| No | Country | Total Population | Number of COVID-19 Cases | COVID-19 Cases/1 Million Population (n) | Alpha Thalassemia (%) | Beta Thalassemia (%) | HbE Thalassemia (%) | TDT Patient Mortality due to COVID-19 |
|---|---|---|---|---|---|---|---|---|
| 1 | Indonesia | 270,203,917 | 2,908,040 | 10,762 | 0.5% | 3% | 1–25% | 7 |
| 2 | Philippines | 104,900,000 | 1,605,762 | 15,308 | 5.4% | 1.2% | 1% | N/A |
| 3 | Vietnamese | 95,540,000 | 165,339 | 1731 | 0.05% | 1.6–25% | 1–73% | N/A |
| 4 | Thailand | 69,400,000 | 652,185 | 9397 | 5.5–30% | 1–9% | 5–50% | N/A |
| 5 | Myanmar | 53,370,000 | 306,354 | 5740 | 10.5% | 4% | 1–26% | N/A |
| 6 | Malaysia | 31,200,000 | 1,163,291 | 37,285 | 1.8–7.5% | 3–5% | 5–46% | N/A |
| 7 | Cambodia | 16,010,000 | 79,051 | 4938 | 10% | 3% | 31–63% | N/A |
| 8 | Laos | 7,364,903 | 7015 | 952 | 42% | 9% | 24–48% | N/A |
| 9 | Singapore | 5,612,000 | 65,213 | 11,620 | 2.91% | 0.93% | 0.64% | N/A |
| 10 | Timor Leste | 1,339,862 | 10,982 | 8196 | N/A | N/A | N/A | N/A |
| 11 | Brunei | 428,607 | 338 | 789 | 4.3% | 0.02% | 0.01% | N/A |
| Total | 655,369,289 | 6,963,570 | 106,718 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Atmakusuma, T.D. COVID-19 in Patients with Transfusion Dependent Thalassemia (TDT) in Indonesia: Characteristics of the Disease and Patients, and Comparison between Epidemiological Data for COVID-19 and Thalassemia in Indonesia and Southeast Asia. Hematol. Rep. 2022, 14, 2-12. https://doi.org/10.3390/hematolrep14010002
Atmakusuma TD. COVID-19 in Patients with Transfusion Dependent Thalassemia (TDT) in Indonesia: Characteristics of the Disease and Patients, and Comparison between Epidemiological Data for COVID-19 and Thalassemia in Indonesia and Southeast Asia. Hematology Reports. 2022; 14(1):2-12. https://doi.org/10.3390/hematolrep14010002
Chicago/Turabian StyleAtmakusuma, Tubagus Djumhana. 2022. "COVID-19 in Patients with Transfusion Dependent Thalassemia (TDT) in Indonesia: Characteristics of the Disease and Patients, and Comparison between Epidemiological Data for COVID-19 and Thalassemia in Indonesia and Southeast Asia" Hematology Reports 14, no. 1: 2-12. https://doi.org/10.3390/hematolrep14010002
APA StyleAtmakusuma, T. D. (2022). COVID-19 in Patients with Transfusion Dependent Thalassemia (TDT) in Indonesia: Characteristics of the Disease and Patients, and Comparison between Epidemiological Data for COVID-19 and Thalassemia in Indonesia and Southeast Asia. Hematology Reports, 14(1), 2-12. https://doi.org/10.3390/hematolrep14010002