
Cannabinoid Hyperemesis Syndrome in Adolescents: A Narrative Review


 ,
,  , , ,
, , ,  ,
, 
{kind=link}
{kind=link}
Abstract
1. Introduction
1.1. Definition and Brief History of Cannabinoid Hyperemesis Syndrome (CHS)
1.2. Cannabinoid Use Among Adolescents and Young Adults
1.3. Purposes of the Review
2. Materials and Methods
3. Results
3.1. Epidemiology
3.2. Pathophysiology
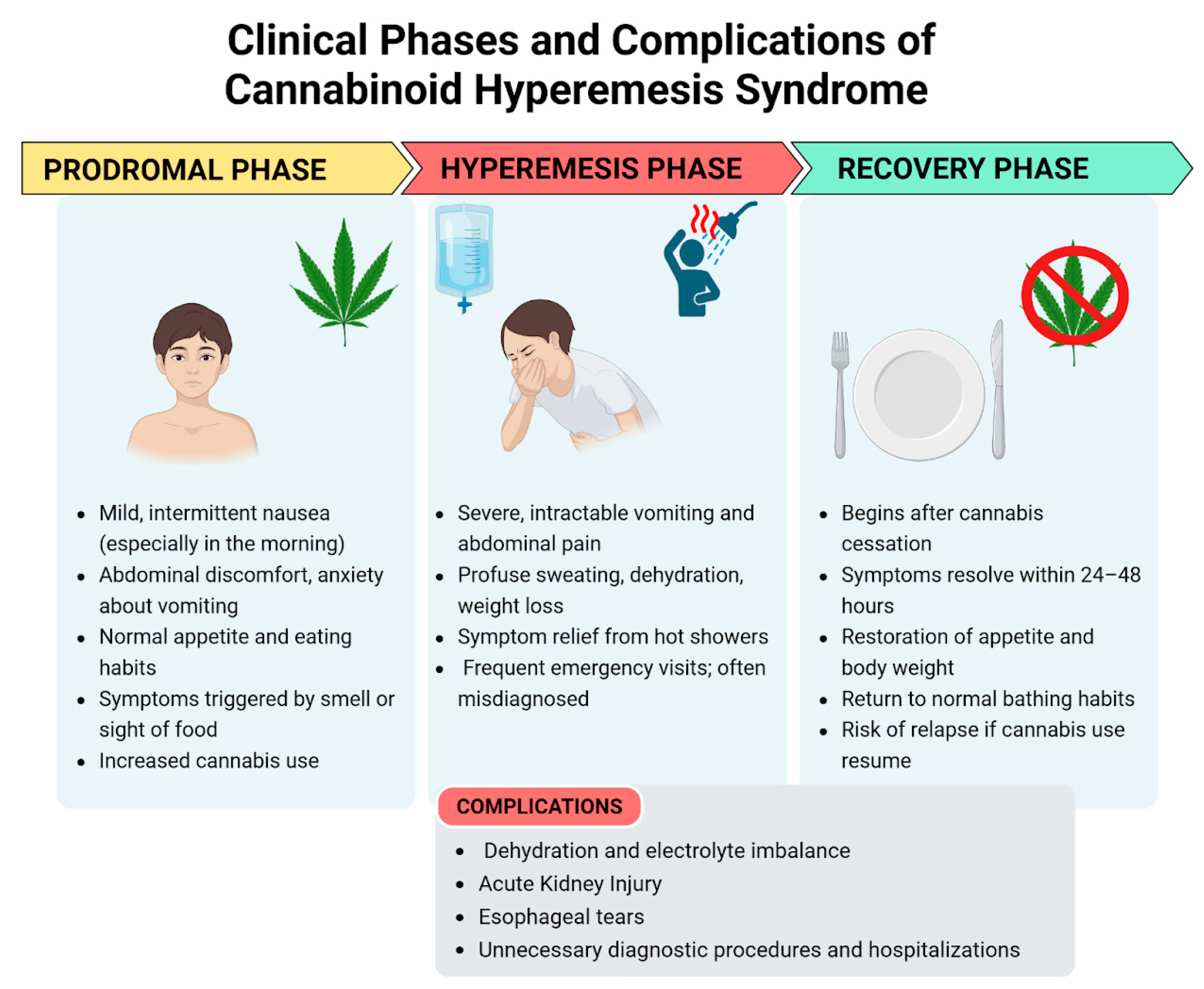
3.3. Clinical Presentation
3.3.1. Prodromal Phase
3.3.2. Hyperemesis Phase
3.3.3. Recovery Phase
3.4. Diagnosis
- Regular cannabis use for at least 3 months;
- Onset or worsening of episodic nausea and vomiting resembling CVS after the initiation of regular cannabis use;
- Absence of other underlying medical conditions that could explain the symptoms, confirmed through appropriate negative investigations.
- Symptom relief with hot baths or showers;
- Weight loss;
- Abdominal pain;
- Altered bowel habits.
- Gastrointestinal conditions such as abdominal migraine, celiac disease, eosinophilic esophagitis, food sensitivities, gastroesophageal reflux disease, liver disease, pancreatitis, appendicitis, and anatomical obstruction such as malrotation or volvulus;
- Metabolic conditions such as mitochondrial dysfunctions;
- Neurological and psychiatric conditions such as migraines, intracranial masses, autonomic dysfunction, epilepsy, drug toxicity, anxiety, bulimia, and psychogenic vomiting;
- Endocrinological conditions [15].
3.5. Management and Treatment
3.6. Prognosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhu, J.W.; Gonsalves, C.L.; Issenman, R.M.; Kam, A.J. Diagnosis and Acute Management of Adolescent Cannabinoid Hyperemesis Syndrome: A Systematic Review. J. Adolesc. Health 2021, 68, 246–254. [Google Scholar] [CrossRef]
- Allen, J.H. Cannabinoid hyperemesis: Cyclical hyperemesis in association with chronic cannabis abuse. Gut 2004, 53, 1566–1570. [Google Scholar] [CrossRef] [PubMed]
- Venkatesan, T.; Levinthal, D.J.; Li, B.U.K.; Tarbell, S.E.; Adams, K.A.; Issenman, R.M.; Sarosiek, I.; Jaradeh, S.S.; Sharaf, R.N.; Sultan, S.; et al. Role of chronic cannabis use: Cyclic vomiting syndrome vs cannabinoid hyperemesis syndrome. Neurogastroenterol. Motil. 2019, 31, e13606. [Google Scholar] [CrossRef] [PubMed]
- Sontineni, S.P. Cannabinoid hyperemesis syndrome: Clinical diagnosis of an underrecognised manifestation of chronic cannabis abuse. World J. Gastroenterol. 2009, 15, 1264. [Google Scholar] [CrossRef]
- Simonetto, D.A.; Oxentenko, A.S.; Herman, M.L.; Szostek, J.H. Cannabinoid Hyperemesis: A Case Series of 98 Patients. Mayo Clin. Proc. 2012, 87, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Lonsdale, H.; Peck, J. Pediatric Cannabinoid Hyperemesis: A Single Institution 10-Year Case Series. J. Adolesc. Health 2021, 68, 255–261. [Google Scholar] [CrossRef]
- Cannabis. Available online: https://www.who.int/teams/mental-health-and-substance-use/alcohol-drugs-and-addictive-behaviours/drugs-psychoactive/cannabis (accessed on 20 March 2025).
- Blohm, E.; Sell, P.; Neavyn, M. Cannabinoid toxicity in pediatrics. Curr. Opin. Pediatr. 2019, 31, 256–261. [Google Scholar] [CrossRef]
- European Monitoring Centre for Drugs and Drug Addiction (EMCDDA). European Drug Report 2024: Trends and Developments. Luxembourg: Publications Office of the European Union. 2024. Available online: https://www.emcdda.europa.eu/publications/european-drug-report/2024_en (accessed on 20 March 2025).
- Yang, J.; Mejia, M.C.; Sacca, L.; Hennekens, C.H.; Kitsantas, P. Trends in Marijuana Use among Adolescents in the United States. Pediatr. Rep. 2024, 16, 872–879. [Google Scholar] [CrossRef]
- World Drug Report 2024—Key Findings and Conclusions. United Nations: Office on Drugs and Crime. Available online: https://www.unodc.org/unodc/en/data-and-analysis/wdr2024-key-findings-conclusions.html (accessed on 20 March 2025).
- Benedetti, E.; Resce, G.; Brunori, P.; Molinaro, S. Cannabis Policy Changes and Adolescent Cannabis Use: Evidence from Europe. Int. J. Environ. Res. Public Health 2021, 18, 5174. [Google Scholar] [CrossRef]
- Chhabra, M.; Ben-Eltriki, M.; Mansell, H.; Lê, M.L.; Huntsman, R.J.; Finkelstein, Y.; Kelly, L.E. Cannabinoids Used for Medical Purposes in Children and Adolescents: A Systematic Review and Meta-Analysis. JAMA Pediatr. 2024, 178, 1124. [Google Scholar] [CrossRef]
- Mandelbaum, D.E.; de la Monte, S.M. Adverse Structural and Functional Effects of Marijuana on the Brain: Evidence Reviewed. Pediatr. Neurol. 2017, 66, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Dosani, K.; Koletic, C.; Alhosh, R. Cannabinoid Hyperemesis Syndrome in Pediatrics: An Emerging Problem. Pediatr. Rev. 2021, 42, 500–506. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.; Jergel, A.; George, R.P.; Jenkins, E.; Bashaw, H. Distinguishing Clinical Features of Cannabinoid Hyperemesis Syndrome and Cyclic Vomiting Syndrome: A Retrospective Cohort Study. J. Pediatr. 2024, 271, 114054. [Google Scholar] [CrossRef] [PubMed]
- ElSohly, M.A.; Mehmedic, Z.; Foster, S.; Gon, C.; Chandra, S.; Church, J.C. Changes in Cannabis Potency over the Last Two Decades (1995-2014)—Analysis of Current Data in the United States. Biol. Psychiatry 2016, 79, 613–619. [Google Scholar] [CrossRef]
- Sawni, A.; Vaniawala, V.P.; Good, M.; Lim, W.Y.; Golec, A.S. Recurrent Cyclic Vomiting in Adolescents: Can It Be Cannabinoid Hyperemesis Syndrome? Clin. Pediatr. 2016, 55, 560–563. [Google Scholar] [CrossRef]
- Hernandez, J.M.; Paty, J.; Price, I.M. Cannabinoid hyperemesis syndrome presentation to the emergency department: A two-year multicentre retrospective chart review in a major urban area. CJEM 2018, 20, 550–555. [Google Scholar] [CrossRef]
- Lonsdale, H.; Wilsey, M.J. Paediatric cannabinoid hyperemesis. Curr. Opin. Pediatr. 2022, 34, 510–515. [Google Scholar] [CrossRef]
- Wagner, S.; Hoppe, J.; Zuckerman, M.; Schwarz, K.; McLaughlin, J. Efficacy and safety of topical capsaicin for cannabinoid hyperemesis syndrome in the emergency department. Clin. Toxicol. 2020, 58, 471–475. [Google Scholar] [CrossRef]
- Perisetti, A.; Goyal, H. Endocannabinoid system and cannabis hyperemesis syndrome: A narrative update. Eur. J. Gastroenterol. Hepatol. 2022, 34, 1–8. [Google Scholar] [CrossRef]
- Reinert, J.P.; Niyamugabo, O.; Harmon, K.S.; Fenn, N.E. Management of Pediatric Cannabinoid Hyperemesis Syndrome: A Review. J. Pediatr. Pharmacol. Ther. 2021, 26, 339–345. [Google Scholar] [CrossRef]
- Ruberto, A.J.; Sivilotti, M.L.A.; Forrester, S.; Hall, A.K.; Crawford, F.M.; Day, A.G. Intravenous Haloperidol Versus Ondansetron for Cannabis Hyperemesis Syndrome (HaVOC): A Randomized, Controlled Trial. Ann. Emerg. Med. 2021, 77, 613–619. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pietrantoni, C.; Margiotta, G.; Marano, G.; Mazza, M.; Proli, F.; Stella, G.; Cherubino, A.; Viozzi, F.; Guida, F.R.; Rendeli, C.; et al. Cannabinoid Hyperemesis Syndrome in Adolescents: A Narrative Review. Pediatr. Rep. 2025, 17, 75. https://doi.org/10.3390/pediatric17040075
Pietrantoni C, Margiotta G, Marano G, Mazza M, Proli F, Stella G, Cherubino A, Viozzi F, Guida FR, Rendeli C, et al. Cannabinoid Hyperemesis Syndrome in Adolescents: A Narrative Review. Pediatric Reports. 2025; 17(4):75. https://doi.org/10.3390/pediatric17040075
Chicago/Turabian StylePietrantoni, Camilla, Gaia Margiotta, Giuseppe Marano, Marianna Mazza, Francesco Proli, Giuseppe Stella, Alessia Cherubino, Francesca Viozzi, Fabiana Rita Guida, Claudia Rendeli, and et al. 2025. "Cannabinoid Hyperemesis Syndrome in Adolescents: A Narrative Review" Pediatric Reports 17, no. 4: 75. https://doi.org/10.3390/pediatric17040075
APA StylePietrantoni, C., Margiotta, G., Marano, G., Mazza, M., Proli, F., Stella, G., Cherubino, A., Viozzi, F., Guida, F. R., Rendeli, C., Pola, R., Gaetani, E., & Giorgio, V. (2025). Cannabinoid Hyperemesis Syndrome in Adolescents: A Narrative Review. Pediatric Reports, 17(4), 75. https://doi.org/10.3390/pediatric17040075