
Prevalence and Pattern of Birth Defects in Saudi Arabia: A Systematic Review of Observational Studies

 ,
, 
Abstract
1. Introduction
2. Methods
2.1. Study Design and Registration
2.2. Search Strategy
2.3. Study Selection and Eligibility Criteria
2.4. Data Extraction and Management
2.5. Synthesis of the Evidence
3. Results
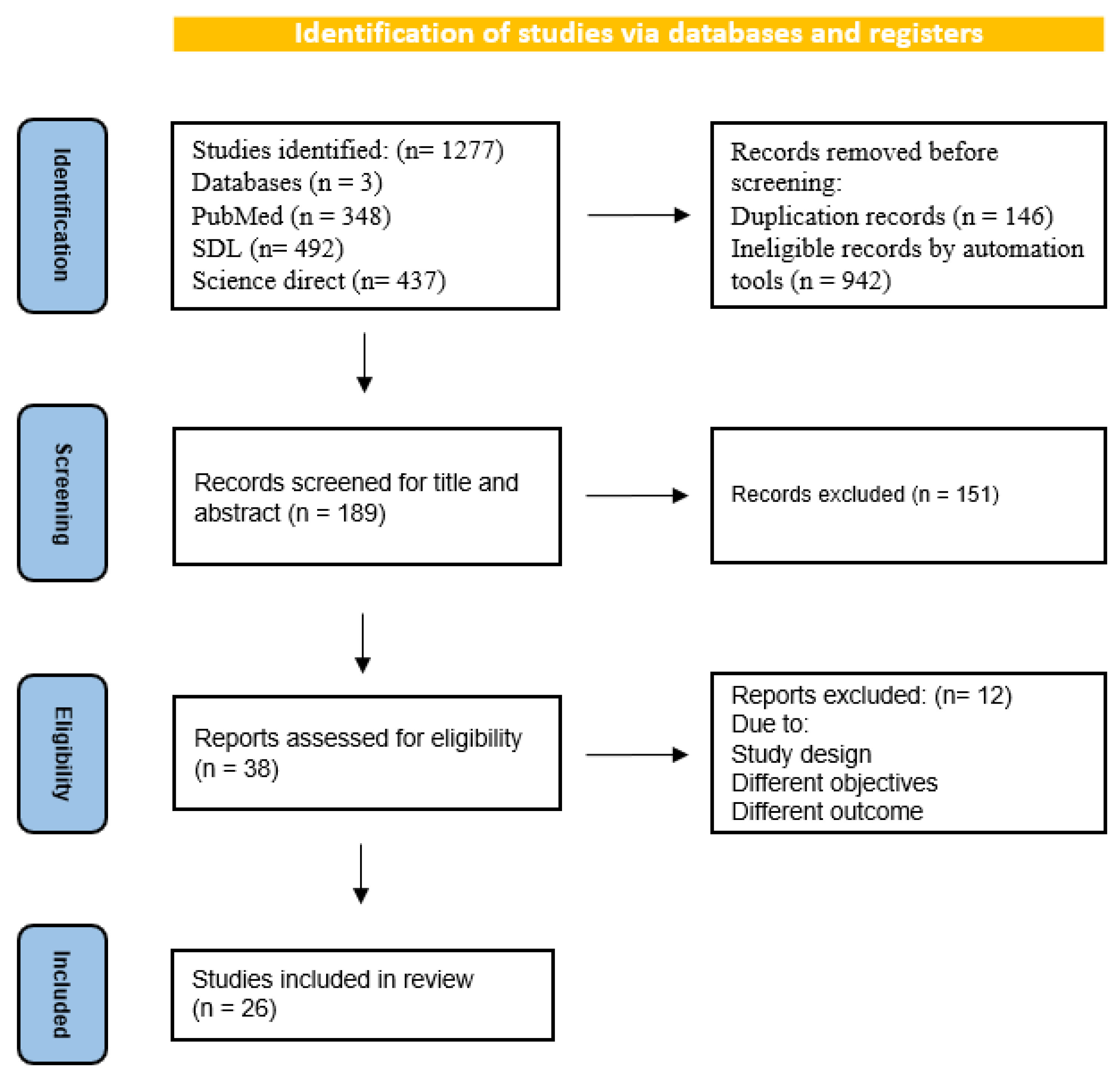
3.1. Search Results
3.2. Characteristics of Included Studies
3.3. Prevalence of Birth Defects
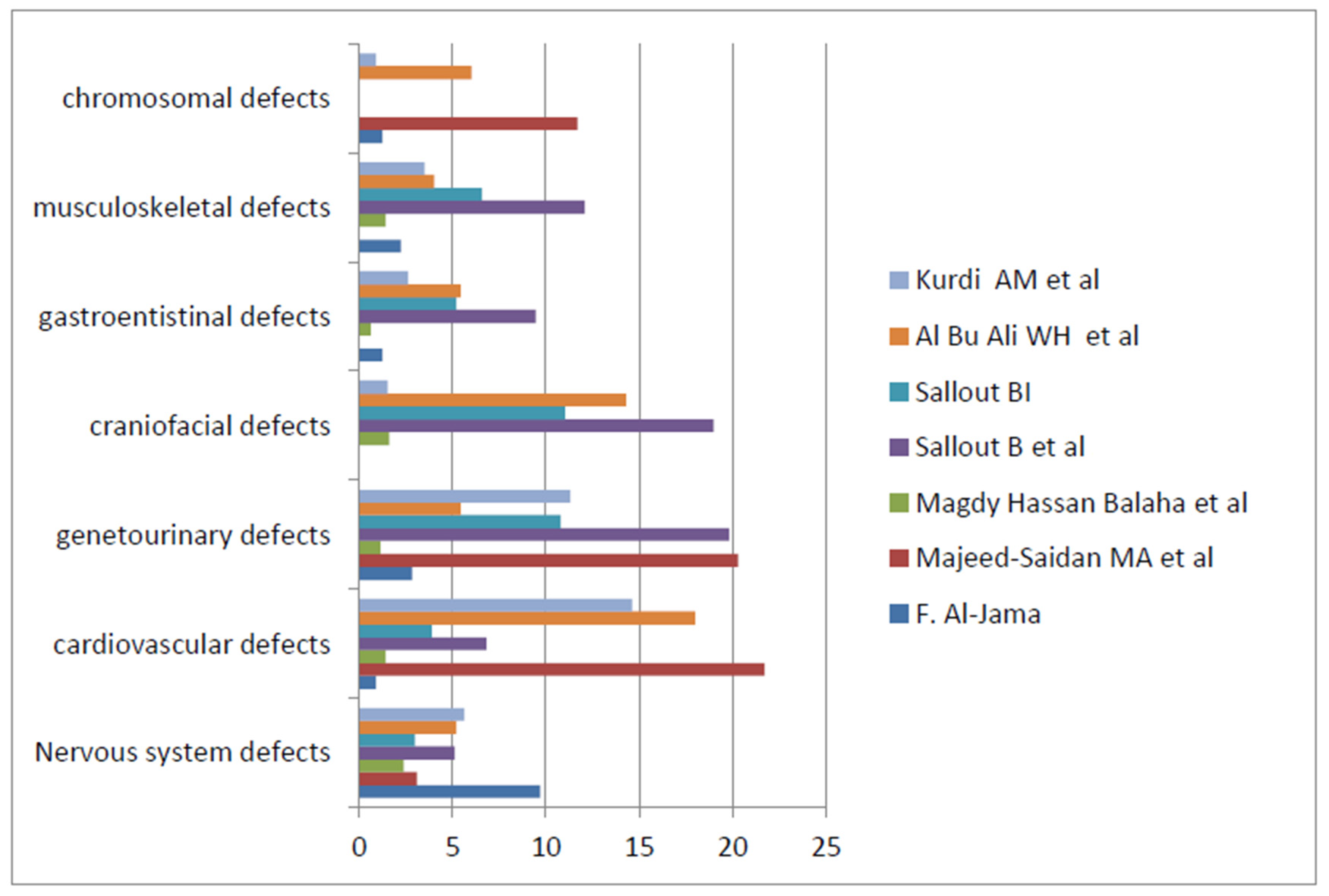
3.4. Pattern of Birth Defects
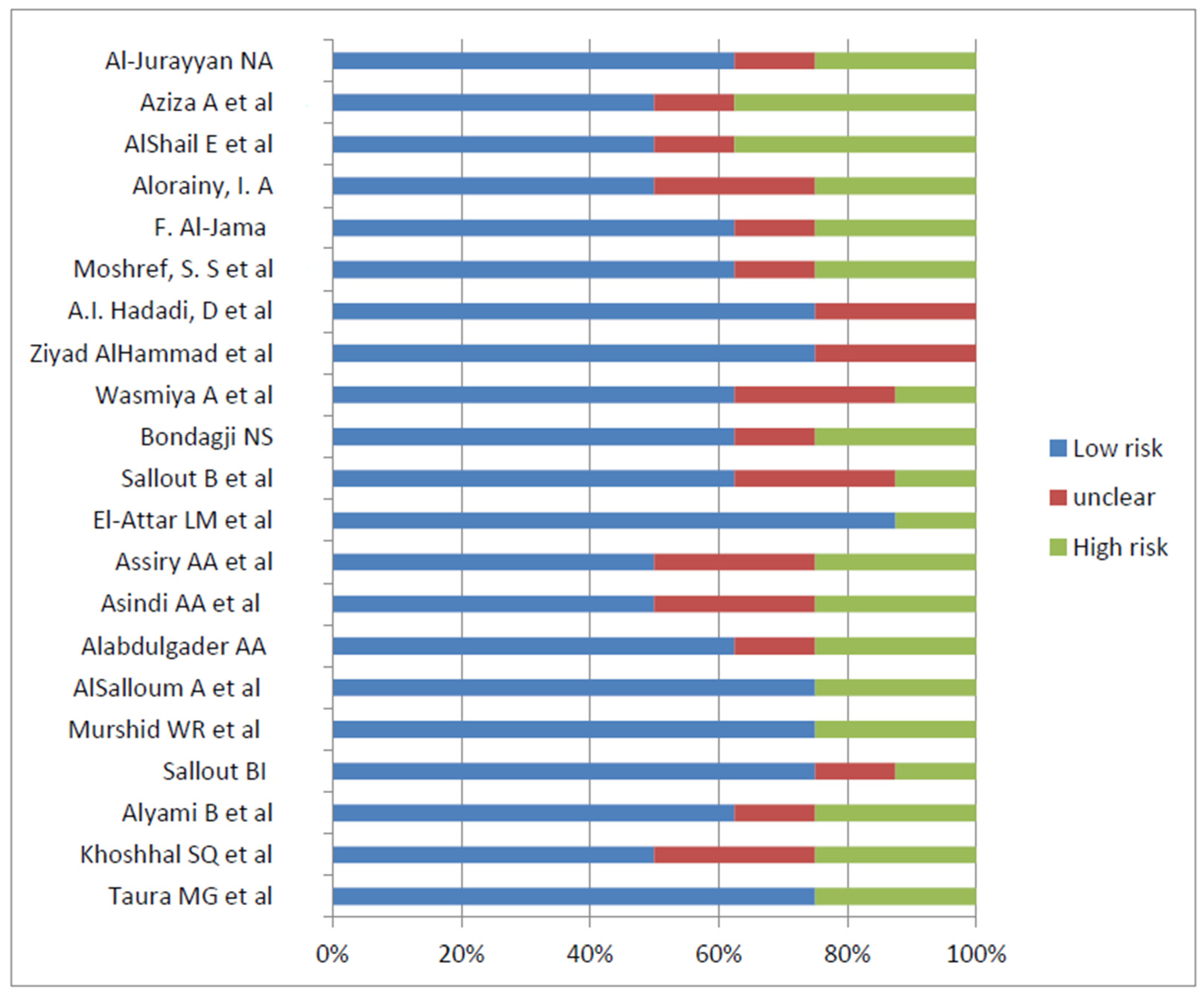
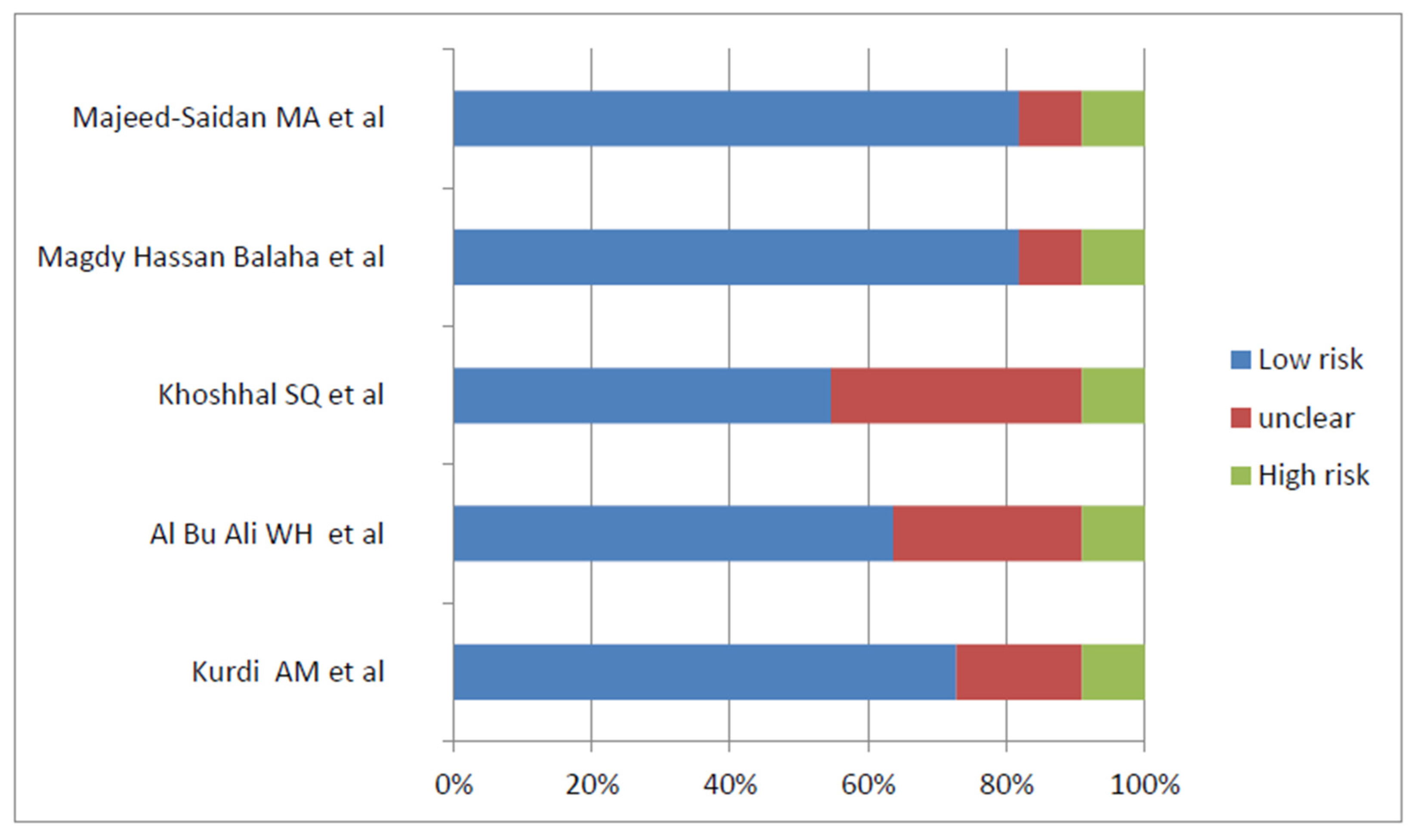
3.5. Risk Factors Associated with Birth Defects
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mannan, M.; Afroze, S.; Dey, S.K.; Moni, S.C.; Shabuj, M.K.H.; Jahan, I.; Sultana, S.N.; Shahidullah, M. Birth Defect and Its Impact in Neonatal Health: A Review. Bangladesh J. Child Health 2019, 43, 49–58. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Committee on Improving Birth Outcomes. Improving Birth Outcomes: Meeting the Challenge in the Developing World; Bale, J.R., Stoll, B.J., Lucas, A.O., Eds.; P237 Reducing Mortality and Morbidity from Birth Defects; National Academies Press: Washington, DC, USA, 2003. Available online: https://www.ncbi.nlm.nih.gov/books/NBK222106/ (accessed on 20 April 2023).
- World Health Organization. Congenital Disorders. 2023. Available online: https://www.who.int/news-room/fact-sheets/detail/birth-defects (accessed on 20 April 2023).
- Martínez-Frías, M.L. Developmental field defects and associations: Epidemiological evidence of their relationship. Am. J. Med. Genet. 1994, 49, 45–51. [Google Scholar] [CrossRef]
- Ameen, S.K.; Alalaf, S.K.; Shabila, N.P. Pattern of congenital anomalies at birth and their correlations with maternal characteristics in the maternity teaching hospital, Erbil city, Iraq. BMC Pregnancy Childbirth 2018, 18, 501. [Google Scholar] [CrossRef] [PubMed]
- Zarocostas, J. Serious birth defects kill at least three million children a year. BMJ 2006, 332, 256. [Google Scholar] [CrossRef] [PubMed]
- Egbe, A.C. Birth Defects in the Newborn Population: Race and Ethnicity. Pediatr. Neonatol. 2015, 56, 183–188. [Google Scholar] [CrossRef]
- Dolk, H.; Loane, M.; Garne, E. The prevalence of congenital anomalies in Europe. Adv. Exp. Med. Biol. 2010, 686, 349–364. [Google Scholar] [CrossRef]
- Adane, F.; Afework, M.; Seyoum, G.; Gebrie, A. Prevalence and associated factors of birth defects among newborns in sub-Saharan African countries: A systematic review and meta-analysis. Pan Afr. Med. J. 2020, 36, 19. [Google Scholar] [CrossRef]
- Harris, B.S.; Bishop, K.C.; Kemeny, H.R.; Walker, J.S.; Rhee, E.; Kuller, J.A. Risk Factors for Birth Defects. Obs. Gynecol. Surv. 2017, 72, 123–135. [Google Scholar] [CrossRef]
- Savitz, D.A.; Schwingl, P.J.; Keels, M.A. Influence of paternal age, smoking, and alcohol consumption on congenital anomalies. Teratology 1991, 44, 429–440. [Google Scholar] [CrossRef]
- Wilson, R.D.; Davies, G.; Désilets, V.; Wilson, R.D.; Davies, G.; Désilets, V.; Reid, G.J.; Summers, A.; Wyatt, P.; Young, D. The use of folic acid for the prevention of neural tube defects and other congenital anomalies. J. Obs. Gynaecol. Can. 2003, 25, 959–973. [Google Scholar] [CrossRef]
- Gill, S.K.; Broussard, C.; Devine, O.; Green, R.F.; Rasmussen, S.A.; Reefhuis, J.; National Birth Defects Prevention Study. Association between maternal age and birth defects of unknown etiology: United States, 1997–2007. Birth Defects Res. Part A 2012, 94, 1010–1018. [Google Scholar] [CrossRef] [PubMed]
- Romitti, P.A. Utility of family history reports of major birth defects as a public health strategy. Pediatrics 2007, 120 (Suppl. 2), S71–S77. [Google Scholar] [CrossRef] [PubMed]
- Almuneef, M.; Saleheen, H.; Albuhairan, F.; Al-Eissa, M.; Al Muntaser, M.; Al Alem, H.; Baylon, B. A Child mortality in Saudi Arabia: Time for action at all levels. Int. J. Pediatr. Adolesc. Med. 2021, 8, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Al Husain, M.; Al Bunyan, M. Consanguineous marriages in a Saudi population and the effect of inbreeding on prenatal and postnatal mortality. Ann. Trop. Paediatr. 1997, 17, 155–160. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Moher, D. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. J. Clin. Epidemiol. 2021, 134, 178–189. [Google Scholar] [CrossRef]
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems, 10th ed.; World Health Organization: Geneva, Switzerland, 2004; Volume 3, Available online: https://icd.who.int/browse10/2010/en#/XVII (accessed on 1 May 2023).
- Checklist for Systematic Reviews and Research Syntheses—Jbi. Available online: https://jbi.global/sites/default/files/202008/Checklist_for_Systematic_Reviews_and_Research_Syntheses.pdf (accessed on 25 February 2023).
- Taura, M.G.; Alshahrani, A.M.; Alqahtani, D.O. Prevalence of congenital heart disease among patients with Down syndrome in Southwestern Saudi Arabia. Ann. Afr. Med. 2021, 20, 265–269. [Google Scholar]
- Khoshhal, S.Q.; Albasri, A.M.; Morsy, M.M.F.; Alnajjar, A.A. The trends and patterns of congenital heart diseases at Madinah Cardiac Center, Madinah, Saudi Arabia. Saudi Med. J. 2020, 41, 977–983. [Google Scholar] [CrossRef]
- Alyami, B.; Ali-Hassan, M.; Braimah, R.; Al-Mahri, M.; Alyami, F.; Alharieth, S. Prevalence and Clinical Case Series of Syndromic and Nonsyndromic Cleft Lip and Palate in a Saudi Arabian Neonatal Population. Cleft Palate-Craniofacial J. 2020, 57, 1259–1265. [Google Scholar] [CrossRef]
- Sallout, B.I.; Al-Hoshan, M.S.; Attyyaa, R.A.; Al Suleimat, A.A. Antenatal diagnosis, prevalence and outcome of major congenital anomalies in Saudi Arabia: A hospital-based study. Ann. Saudi Med. 2008, 28, 272–276. [Google Scholar] [CrossRef]
- Murshid, W.R.; Jarallah, J.S.; Dad, M.I. Epidemiology of infantile hydrocephalus in Saudi Arabia: Birth prevalence and associated factors. Pediatr. Neurosurg. 2000, 32, 119–123. [Google Scholar] [CrossRef]
- AlSalloum, A.; El Mouzan, M.I.; AlHerbish, A.; AlOmer, A.; Qurashi, M. Prevalence of selected congenital anomalies in Saudi children: A community-based study. Ann. Saudi Med. 2015, 35, 107–110. [Google Scholar] [CrossRef] [PubMed]
- Alabdulgader, A.A. Congenital heart disease in 740 subjects: Epidemiological aspects. Ann. Trop. Paediatr. 2001, 21, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Asindi, A.A.; Al-Daama, S.A.; Zayed, M.S.; Fatinni, Y.A. Congenital malformation of the gastrointestinal tract in Aseer region, Saudi Arabia. Saudi Med. J. 2002, 23, 1078–1082. [Google Scholar]
- Assiry, A.A.; Khan, S.D.; Al-Shubrmi, H.R.; Al-Shammary, D.H.; Al-Fahhad, H.M.; Al-Shammary, A.F.; Al-Shammari, A.F. Head and Neck Congenital Anomalies in Neonate Hospitals in Hail, Saudi Arabia. Int. J. Clin. Pediatr. Dent. 2020, 13, 160–162. [Google Scholar] [CrossRef] [PubMed]
- El-Attar, L.M.; Bahashwan, A.A.; Bakhsh, A.D.; Moshrif, Y.M. The prevalence and patterns of chromosome abnormalities in newborns with major congenital anomalies: A retrospective study from Saudi Arabia. Intractable Rare Dis. Res. 2021, 10, 81–87. [Google Scholar] [CrossRef]
- Sallout, B.; Obedat, N.; Shakeel, F.; Mansoor, A.; Walker, M.; Al-Badr, A. Prevalence of major congenital anomalies at King Fahad Medical City in Saudi Arabia: A tertiary care centre-based study. Ann. Saudi Med. 2015, 35, 343–351. [Google Scholar] [CrossRef]
- Bondagji, N.S. Antenatal diagnosis, prevalence and outcome of congenital anomalies of the kidney and urinary tract in Saudi Arabia. Urol. Ann. 2014, 6, 36–40. [Google Scholar] [CrossRef]
- AlHayyan, W.A.; Al Hayek, S.; AlOtabi, S.S.; AlGhanim, S.A. Birth prevalence of orofacial cleft in a tertiary hospital in Riyadh, Saudi Arabia: A retrospective audit. Saudi Dent. J. 2021, 33, 954–957. [Google Scholar] [CrossRef]
- AlHammad, Z.; Suliman, I.; Alotaibi, S.; Alnofaie, H.; Alsaadi, W.; Alhusseini, S.; Aldakheel, G.; Alsubaie, N. The prevalence of non-syndromic orofacial clefts and associated congenital heart diseases of a tertiary hospital in Riyadh, Saudi Arabia. Saudi Dent. J. 2021, 33, 137–142. [Google Scholar] [CrossRef]
- Hadadi, A.I.; Al Wohaibi, D.; Almtrok, N.; Aljahdali, N.; AlMeshal, O.; Badri, M. Congenital anomalies associated with syndromic and non-syndromic cleft lip and palate. JPRAS Open 2017, 14, 5–15. [Google Scholar] [CrossRef]
- Moshref, S.S.; Jamal, Y.S.; Fakiha, M.; Awan, B.A.; Alsiny, F.; Alzhrani, F.; Ammar, H.; Bamashmos, A.; Baamer, A. Non-Syndromic Orofacial Cleft Malformations in Jeddah, Saudi Arabia. J. King Abdulaziz Univ. Med. Sci. 2017, 24, 1–11. [Google Scholar] [CrossRef]
- Al-Jama, F. Congenital malformations in newborns in a teaching hospital in eastern Saudi Arabia. J. Obstet. Gynaecol. 2001, 21, 595–598. [Google Scholar] [CrossRef] [PubMed]
- Alorainy, I.A. Pattern of congenital brain malformations at a referral hospital in saudi arabia: An MRI study. Ann. Saudi Med. 2006, 26, 28–37. Available online: https://www.proquest.com/scholarly-journals/pattern-congenital-brain-malformations-at/docview/1441872821/se-2 (accessed on 25 February 2023). [CrossRef]
- AlShail, E.; De Vol, E.; Yassen, A.; Elgamal, E.A. Epidemiology of neural tube defects in Saudi Arabia. Saudi Med. J. 2014, 35 (Suppl. 1), S68–S71. [Google Scholar] [PubMed]
- Aziza, A.; Kandasamy, R.; Shazia, S. Pattern of craniofacial anomalies seen in a tertiary care hospital in Saudi Arabia. Ann. Saudi Med. 2011, 31, 488–493. [Google Scholar] [CrossRef] [PubMed]
- Al-Jurayyan, N.A. Ambiguous genitalia: Two decades of experience. Ann. Saudi Med. 2011, 31, 284–288. [Google Scholar] [CrossRef]
- Kurdi, A.M.; Majeed-Saidan, M.A.; Al Rakaf, M.S.; AlHashem, A.M.; Botto, L.D.; Baaqeel, H.S.; Ammari, A.N. Congenital anomalies and associated risk factors in a Saudi population: A cohort study from pregnancy to age 2 years. BMJ Open 2019, 9, e026351. [Google Scholar] [CrossRef]
- Ali, W.A.B.; Balaha, M.H.; Al Moghannum, M.S.; Hashim, I. Risk factors and birth prevalence of birth defects and inborn errors of metabolism in Al Ahsa, Saudi Arabia. Pan Afr. Med. J. 2011, 8, 14. [Google Scholar] [CrossRef]
- Balaha, M.H.; Al Bu Ali, W.H.; Al Aswad, L.H.; Al Moghannum, M.S. Maternal obesity predict isolated birth defects in live births in Eastern Province of Saudi Arabia. J. Matern. Fetal Neonatal Med. 2012, 25, 924–929. [Google Scholar] [CrossRef]
- Majeed-Saidan, M.A.; Ammari, A.N.; AlHashem, A.M.; Al Rakaf, M.S.; Shoukri, M.M.; Garne, E.; Kurdi, A.M. Effect of consanguinity on birth defects in Saudi women: Results from a nested case-control study. Birth Defects Res. Part A 2015, 103, 100–104. [Google Scholar] [CrossRef]
- Kamal, N.M.; Alzeky, A.M.; Omair, M.R.; Attar, R.A.; Alotaibi, A.M.; Safar, A.; Abosabie, S.A. First report of SYNE1 arthrogryposis multiplex congenita from Saudi Arabia with a novel mutation: A case report. Ital. J. Pediatr. 2022, 48, 107. [Google Scholar] [CrossRef] [PubMed]
- Stoll, C.; Alembik, Y.; Roth, M.P.; Dott, B. Parental consanguinity as a cause for increased incidence of births defects in a study of 238,942 consecutive births. Ann. Genet. 1999, 42, 133–139. [Google Scholar] [PubMed]
- El Koumi, M.A.; Al Banna, E.A.; Lebda, I. Pattern of congenital anomalies in newborn: A hospital-based study. Pediatr. Rep. 2013, 5, e5. [Google Scholar] [CrossRef]
- Sarmah, S.; Muralidharan, P.; Marrs, J.A. Common congenital anomalies: Environmental causes and prevention with folic acid-containing multivitamins. Birth Defects Res. C Embryo Today 2016, 108, 274–286. [Google Scholar] [CrossRef] [PubMed]
- Kumar, J.; Saini, S.S.; Sundaram, V.; Mukhopadhyay, K.; Dutta, S.; Kakkar, N.; Kumar, P. Prevalence & spectrum of congenital anomalies at a tertiary care centre in north India over 20 years (1998–2017). Indian J. Med. Res. 2021, 154, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Mai, C.T.; Isenburg, J.L.; Canfield, M.A.; Meyer, R.E.; Correa, A.; Alverson, C.J.; National Birth Defects Prevention Network. National population-based estimates for major birth defects, 2010–2014. Birth Defects Res. 2019, 111, 1420–1435. [Google Scholar] [CrossRef] [PubMed]
- Mikwar, M.; MacFarlane, A.J.; Marchetti, F. Mechanisms of oocyte aneuploidy associated with advanced maternal age. Mutat. Res./Rev. Mutat. Res. 2020, 785, 108320. [Google Scholar] [CrossRef]
- Zhu, Y.; Chen, Y.; Feng, Y.; Yu, D.; Mo, X. Association between maternal body mass index and congenital heart defects in infants: A meta-analysis. Congenit. Heart Dis. 2018, 13, 271–281. [Google Scholar] [CrossRef]
- Honein, M.A.; Moore, C.A.; Watkins, M.L. Subfertility and prepregnancy overweight/obesity: Possible interaction between these risk factors in the etiology of congenital renal anomalies. Birth Defects Res. A 2003, 67, 572–577. [Google Scholar] [CrossRef]
- Stothard, K.J.; Tennant, P.W.; Bell, R.; Rankin, J. Maternal overweight and obesity and the risk of congenital anomalies: A systematic review and meta-analysis. JAMA 2009, 301, 636–650. [Google Scholar] [CrossRef]
- Gajagowni, S.; Nair, P.; Bapat, A.C.; Vachharajani, A.J. Diabetic Embryopathies. Neoreviews 2022, 23, 677–688. [Google Scholar] [CrossRef] [PubMed]
- Brent, R.L. Utilization of developmental basic science principles in the evaluation of reproductive risks from pre- and postconception environmental radiation exposures. Teratology 1999, 59, 182–204. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eltyeb, E.E.; Halawi, M.H.A.; Tashari, T.B.M.; Alharbi, K.; Alsayari, O.S.; Albarrak, D.A.; Eltayeb, R.A.; Al-Makramani, A.A.A.; Medani, I.E.M. Prevalence and Pattern of Birth Defects in Saudi Arabia: A Systematic Review of Observational Studies. Pediatr. Rep. 2023, 15, 431-441. https://doi.org/10.3390/pediatric15030040
Eltyeb EE, Halawi MHA, Tashari TBM, Alharbi K, Alsayari OS, Albarrak DA, Eltayeb RA, Al-Makramani AAA, Medani IEM. Prevalence and Pattern of Birth Defects in Saudi Arabia: A Systematic Review of Observational Studies. Pediatric Reports. 2023; 15(3):431-441. https://doi.org/10.3390/pediatric15030040
Chicago/Turabian StyleEltyeb, Ebtihal Elameen, Majidah Hussain Asiri Halawi, Thekra Badr Mohammed Tashari, Khaled Alharbi, Ohoud Saad Alsayari, Danah Abdullah Albarrak, Raga Abdelkhalig Eltayeb, Ali Ali Ahmed Al-Makramani, and Isameldin Elamin M. Medani. 2023. "Prevalence and Pattern of Birth Defects in Saudi Arabia: A Systematic Review of Observational Studies" Pediatric Reports 15, no. 3: 431-441. https://doi.org/10.3390/pediatric15030040
APA StyleEltyeb, E. E., Halawi, M. H. A., Tashari, T. B. M., Alharbi, K., Alsayari, O. S., Albarrak, D. A., Eltayeb, R. A., Al-Makramani, A. A. A., & Medani, I. E. M. (2023). Prevalence and Pattern of Birth Defects in Saudi Arabia: A Systematic Review of Observational Studies. Pediatric Reports, 15(3), 431-441. https://doi.org/10.3390/pediatric15030040