
Ingrowing Liver as Atypical Recurrent Diaphragmatic Hernia Presentation—Diagnostic and Treatment Difficulties: A Case Report

 , ,
, ,
Abstract
:1. Introduction
2. Case Presentation
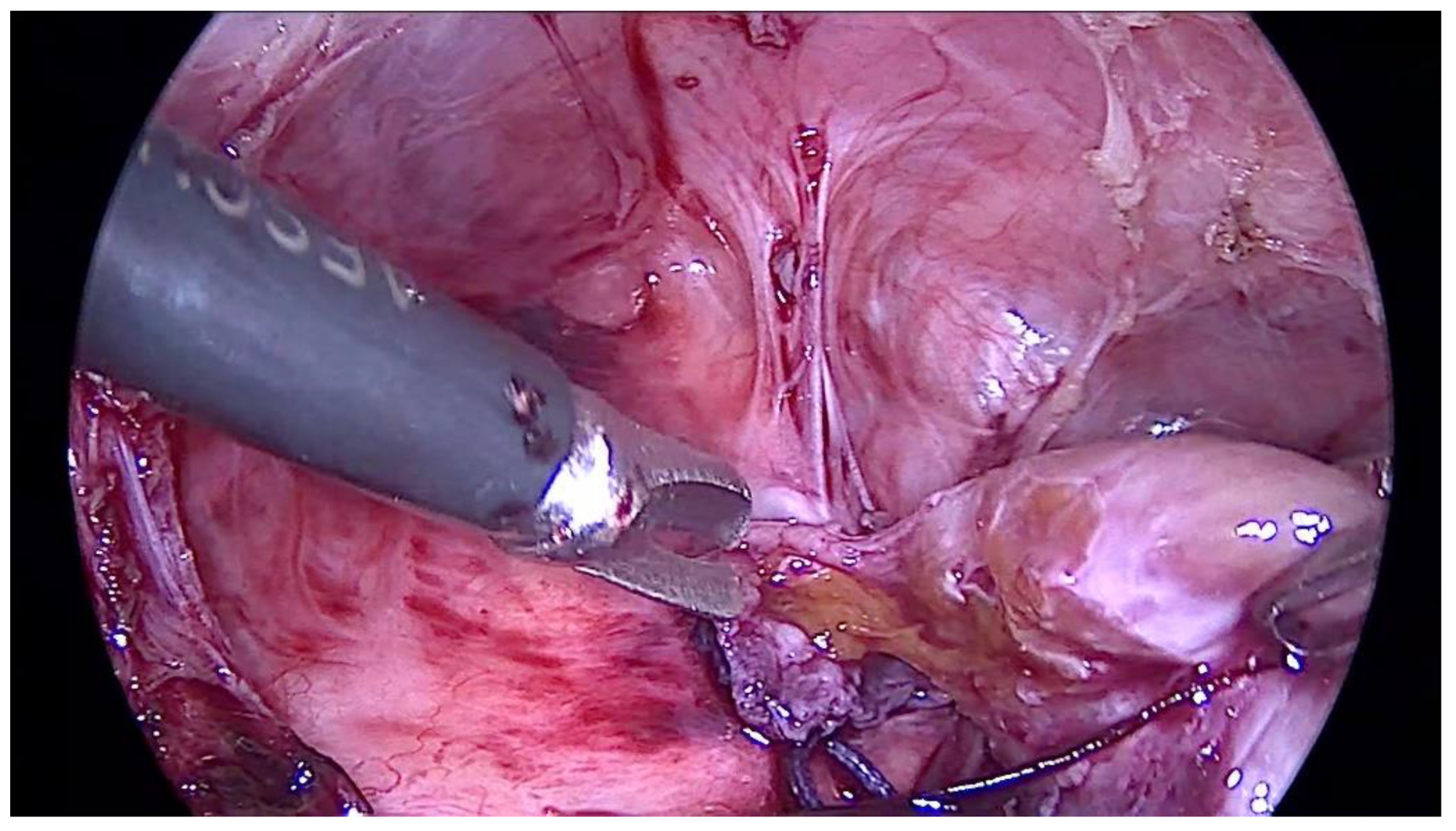
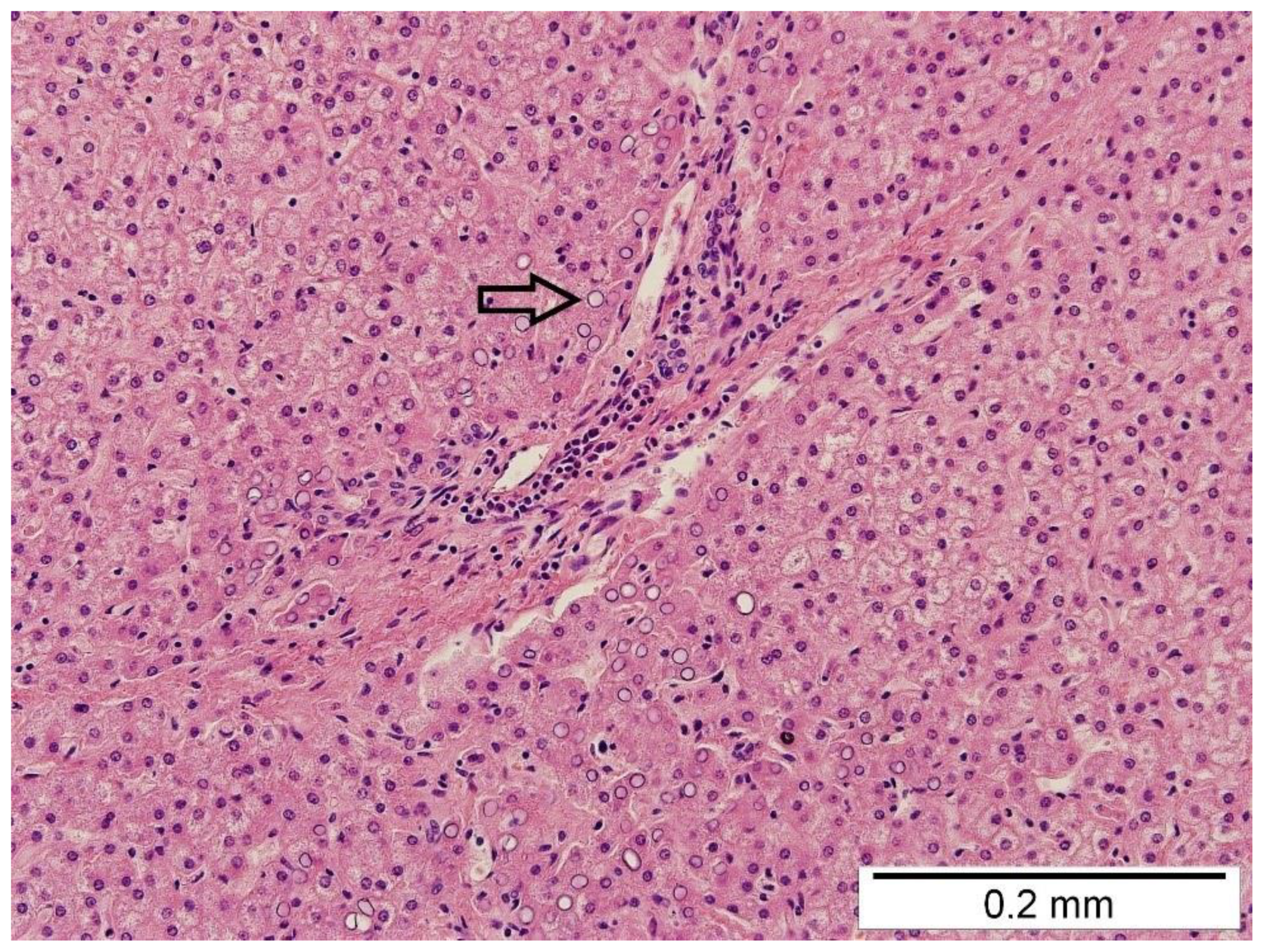
3. Diagnostics and Therapeutic Intervention
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fisher, J.C.; Haley, M.J.; Ruiz-Elizalde, A.; Stolar, C.J.H.; Arkovitz, M.S. Multivariate model for predicting recurrence in congenital diaphragmatic hernia. J. Pediatric Surg. 2009, 44, 1173–1180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamran, A.; Zendejas, B.; Demehri, F.R.; Nath, B.; Zurakowski, D.; Smithers, C.J. Risk factors for recurrence after thoracoscopic repair of congenital diaphragmatic hernia. J. Pediatric Surg. 2018, 53, 2087–2091. [Google Scholar] [CrossRef] [PubMed]
- Tsao, K.; Lally, P.A.; Lally, K.P. Minimally Invasive Repair of Congenital Diaphragmatic Hernia. J. Pediatric Surg. 2011, 46, 1158–1164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Federle, M.P.; Jeffrey, R.B.; Woodward, P.J.; Borhani, A. The Digestive Tract and the Abdominal Cavity. In Diagnostic Imaging: Abdomen, 2nd ed.; Federle, M.P., Jeffrey, R.B., Woodward, P.J., Borhani, A.A., Eds.; Amirsys Inc.: Salt Lake City, UT, USA, 2010; pp. 1–105. [Google Scholar]
- Schwaartz, C.; Duggan, E.; Lee, D.S.; Divino, C.M.; Chin, E.H. Diaphragmatic eventration presenting as a recurrent diaphragmatic hernia. Ann. R. Coll. Surg. Engl. 2017, 99, e196–e199. [Google Scholar] [CrossRef] [PubMed]
- Blinman, T.; Ponsky, T. Pediatric Minimally Invasive Surgery: Laparoscopy and Thoracoscopy in Infants and Children. Pediatrics 2012, 130, 539–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AlFraih, Y. Congenital diaphragmatic hernia with hepatic heterotopia. J. Pediatric Surg. Case Rep. 2021, 64, 101738. [Google Scholar] [CrossRef]
- Mito, K.; Amano, Y.; Oshiro, H.; Matsubara, D.; Fukushima, N.; Ono, S. Liver heterotopia associated with congenital diaphragmatic hernia. Medicine 2019, 98, 4. [Google Scholar] [CrossRef] [PubMed]
- Arakawa, M.; Kimura, Y.; Sakata, K.; Kubo, Y.; Fukushima, T.; Okuda, K. Propensity of ectopic liver to hepatocarcinogenesis: Case report and a review of the literature. Hepatology 1999, 29, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Peetsold, M.G.; Heij, H.A.; Kneepkens, C.M.F.; Nagelkerke, A.F.; Huisman, J.; Gemke, R.J.B.J. The long-term follow-up of patients with a congenital diaphragmatic hernia: A broad spectrum of morbidity. Pediatric Surg. Int. 2009, 25, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Age | Patient’s Data |
|---|---|
| First day of life | The first thoracoscopy—primary closure of diaphragm defect |
| Between 0–4 years | Recurrent upper and lower respiratory tract infections |
| The first at four months, the second at two years old | Bronchoscopy |
| Almost four years old | Lobar pneumonia, X-ray |
| Four years and one month old | The ultrasonography of thoracic cavities during a control visit |
| Four years and two months old | The CT scan of thorax |
| Four years and six months old | The second thoracoscopy—removing the part of ‘ingrowing liver’ and suturing a diaphragmatic defect |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borselle, D.; Międzybrodzki, K.; Gerus, S.; Zaleska-Dorobisz, U.; Hałoń, A.; Szenborn, L.; Patkowski, D. Ingrowing Liver as Atypical Recurrent Diaphragmatic Hernia Presentation—Diagnostic and Treatment Difficulties: A Case Report. Pediatr. Rep. 2022, 14, 140-146. https://doi.org/10.3390/pediatric14010020
Borselle D, Międzybrodzki K, Gerus S, Zaleska-Dorobisz U, Hałoń A, Szenborn L, Patkowski D. Ingrowing Liver as Atypical Recurrent Diaphragmatic Hernia Presentation—Diagnostic and Treatment Difficulties: A Case Report. Pediatric Reports. 2022; 14(1):140-146. https://doi.org/10.3390/pediatric14010020
Chicago/Turabian StyleBorselle, Dominika, Krzysztof Międzybrodzki, Sylwester Gerus, Urszula Zaleska-Dorobisz, Agnieszka Hałoń, Leszek Szenborn, and Dariusz Patkowski. 2022. "Ingrowing Liver as Atypical Recurrent Diaphragmatic Hernia Presentation—Diagnostic and Treatment Difficulties: A Case Report" Pediatric Reports 14, no. 1: 140-146. https://doi.org/10.3390/pediatric14010020
APA StyleBorselle, D., Międzybrodzki, K., Gerus, S., Zaleska-Dorobisz, U., Hałoń, A., Szenborn, L., & Patkowski, D. (2022). Ingrowing Liver as Atypical Recurrent Diaphragmatic Hernia Presentation—Diagnostic and Treatment Difficulties: A Case Report. Pediatric Reports, 14(1), 140-146. https://doi.org/10.3390/pediatric14010020