1. Introduction
In a SARS-CoV-2 virus infection, there are certain parameters, presented in the specialized literature, which can be used as markers of severity in infected patients [
1]. Since the beginning of the COVID-19 pandemic, advanced age has been established among the risk factors, as well as the association of certain comorbidities, including type 2 diabetes [
2,
3,
4,
5,
6,
7]. Other severity parameters in the infection with the new coronavirus included the following: increased levels of pro-inflammatory cytokines such as IL-6, high ferritin levels, increased D-dimers, increased CRP (C reactive protein), and decreased numbers of lymphocytes [
8,
9,
10,
11,
12,
13,
14,
15,
16,
17]. In COVID-19, IL-6 is an important member of the cytokine network and it is one of the primary inflammatory agents that causes an inflammatory storm. Biomarkers which are related to inflammation and infection such as CRP and procalcitonin are induced by IL-6; in this way, IL-6 can be used as a biomarker of disease severity and prognosis [
12]. In addition to increased ferritin, regarding iron metabolism in COVID-19, decreased serum iron was associated with the severity of infection [
18,
19,
20]. The link between decreased transferrin, high ferritin levels, and increased CRP was associated with a proinflammatory status and progression to severe forms of the disease [
21,
22,
23]. The study of ceruloplasmin in SARS-CoV-2 virus infections is a topic of interest because there are studies that describe the fact that ceruloplasmin can act in healthy people both as antioxidant and as pro-oxidant [
24,
25,
26]. Ceruloplasmin is a glycoprotein synthesized in the liver and has six copper atoms in its composition, with a particularly important role in iron metabolism, oxidizing ferrous iron to ferric iron, the ferric iron form being the only one that can be bound to transferrin [
27,
28]. It is known that ceruloplasmin can also act as an acute phase reactant, and ceruloplasmin levels are increased in inflammation, being an independent risk factor for complications associated with diabetes mellitus [
29,
30]. Most of the copper in the body, 90%, is bound to ceruloplasmin and 10% is bound to albumin [
31]. Type 2 diabetes is a metabolic condition characterized by a chronic inflammatory state in which serum ceruloplasmin is elevated, but ceruloplasmin is not correlated with diabetes severity [
32,
33,
34,
35]. In type 2 diabetes, insulin resistance occurs due to endothelial dysfunction, which is associated with increased ROS (reactive oxygen species) production [
36,
37,
38]. The imbalance between ROS and antioxidants is represented by oxidative stress, one of the most important factors in the pathogenesis of type 2 diabetes [
39,
40]. Oxidative stress affects pancreatic beta-cell function and induces apoptosis [
41,
42,
43]. Iron excess is toxic and acts as pro-oxidant, and its accumulation causes inflammation of pancreatic beta cells and is a risk factor for diabetes development and evolution, and a risk of mortality [
44,
45,
46]. Iron homeostasis is regulated by hepcidin and ferroportin, which modulates the flux of iron into the systemic circulation [
47,
48,
49]. Iron deposits are mainly represented by ferritin, which can also plays a role as an acute phase reactant, and high ferritin levels are significantly associated with the severity and unfavorable prognosis in a COVID-19 infection [
50,
51]. Decreased transferrin levels were strongly associated with severe forms of a SARS-CoV-2 infection, with transferrin representing the transport of circulating iron [
52].
The aim of this study was to identify other possible biomarkers of severity in SARS-CoV-2 virus infections at hospital admission in patients with type 2 diabetes as an associated comorbidity.
2. Material and Methods
2.1. Study Design
The study included 90 subjects who were divided into groups of 45 patients that were hospitalized at the clinical hospital “Gavril Curteanu” Oradea between 21 October 2021 and 31 December 2021, and were randomly selected, having as the main inclusion criteria a positive RT-PCR (reverse transcription polymerase chain reaction) rapid antigen test for viral infection and the diagnosis of type 2 diabetes. The control group of 45 healthy persons was randomly chosen, with a negative RT-PCR/rapid antigen test as the inclusion criterion and who were not known to have diabetes or other associated pathologies. The present study was conducted in accordance with the Declaration of Helsinki. Before taking part in this study, each participant gave written informed consent for inclusion. The study protocol was approved by the Ethics Committee of the Clinical Hospital “Gavril Curteanu” Oradea (No. 32652/16.11.2020) and by the Ethics Committee of the University of Oradea (No. 5/A, 21.09.2020).
The inclusion criteria in the group of patients were the diagnosis of type 2 diabetes and SARS-CoV-2 virus infection confirmed by positive RT-PCR/rapid antigen test. Exclusion criteria from the group of patients included absence of type 2 diabetes and absence of infection with the SARS-CoV-2 virus by negative RT-PCR/rapid antigen test. Inclusion criteria in the control group were healthy individuals, absence of any diseases or medication, including absence of type 2 diabetes and negative RT-PCR/rapid antigen test.
2.2. Data Collection
The data were collected in an EXCEL file including the following biomedical parameters at hospital admission: iron biomarkers (ceruloplasmin, serum iron, and transferrin), anthropometric parameters—age (years), angiotensin-converting enzyme (ACE), interleukin 6 (IL-6), and COVID-19 severity on computer tomography at hospital admission (mild, moderate, or severe forms of SARS-CoV-2 viral infection). In the group of patients with type 2 diabetes mellitus and a SARS-CoV-2 virus infection, we also evaluated the relationship between certain parameters of iron metabolism (including serum iron, transferrin, ceruloplasmin, hemoglobin, number of erythrocytes, and ferritin), coagulation parameters (INR—international normalized ratio, platelets number), inflammation parameters (CRP, fibrinogen, LDH—lactate dehydrogenase, and lymphocytes number) and HBA1C level at admission was increased more than 6.6% in all patients with diabetes. We analyzed the regression models that reflected the connection and influence of independent parameters such as coagulation and inflammation on serum iron levels at hospital admission. We also evaluated if the gender of the subjects influenced the level of the biomedical parameters considered in our study.
2.3. Methods
Ceruloplasmin determination was performed by using the nephelometric method (reagent N Antiserum to Human Ceruloplasmin, ref. 10446451, BN ProSpec analyzer, Siemens Healthineers, Erlangen, Germany). Spectrophotometric method was employed for serum iron measurement (Iron_2 reagent, ref. 10377510, Advia 1800 analyzer, Siemens Healthineers). Transferrin was determined by using the nephelometric method (reagent N Antiserum to Human Transferrin, ref. 10446309, BN ProSpec analyzer, Siemens Healthineers). The ACE biomarker was determined by the spectrophotometric method (angiotensin-converting enzyme (ACE) reagent, ref. 12796, analyzer A15, BioSystems SA, Barcelona, Spain). Interleukin 6 was quantified by the electrochemiluminescence method (ECLIA—electrochemiluminescence immunoassay) (IL-6 reagent, ref. 05109442190, Cobas E4111 analyzer, Roche Diagnostics GmbH, Mannheim, Germany). All these biomarkers were analyzed from blood samples collected at the time of hospital admission.
2.4. Statistical Analysis
In the statistical processing of the data, both descriptive statistics procedures were used to calculate averages, standard deviations (for quantitative data), frequencies (for qualitative data), correlation coefficients, graphic representations of the data, as well as statistical analysis procedures. To process the data statistically, we used nonparametric chi-square and descriptive methods and the figures. The threshold of statistical significance of the tests used in the statistical analyses was the one usually applied in medical research p = 0.05 (=5%). The significance threshold p = 0.01 was also used for the case when the result of the analysis was strongly significant (p < 0.01). To perform the statistical calculations, the EXCEL data file which contained the study data, was converted into an SPSS file, the statistical processing was performed with the statistical software SPSS version 20.
3. Results
In the comparative analysis between infected patients and healthy persons, we denoted group 1 as the group of patients with type 2 diabetes mellitus and a SARS-CoV-2 virus infection, and group 2 as the control group of healthy subjects. In group 1, there were 5 mild, 13 moderate, and 27 severe forms of SARS-CoV-2 viral infection on CT (computer tomography) at hospital admission.
We identified a significant statistical difference between the means of the quantitative parameters in the group of infected patients compared to the group of healthy subjects. The means of IL-6 and ceruloplasmin parameters in patients infected with the SARS-CoV-2 virus were statistically significantly higher than in the control group. Regarding the parameters, such as serum iron, ACE, and transferrin, the means for patients infected with the novel coronavirus were statistically significantly lower than in healthy subjects (
Table 1).
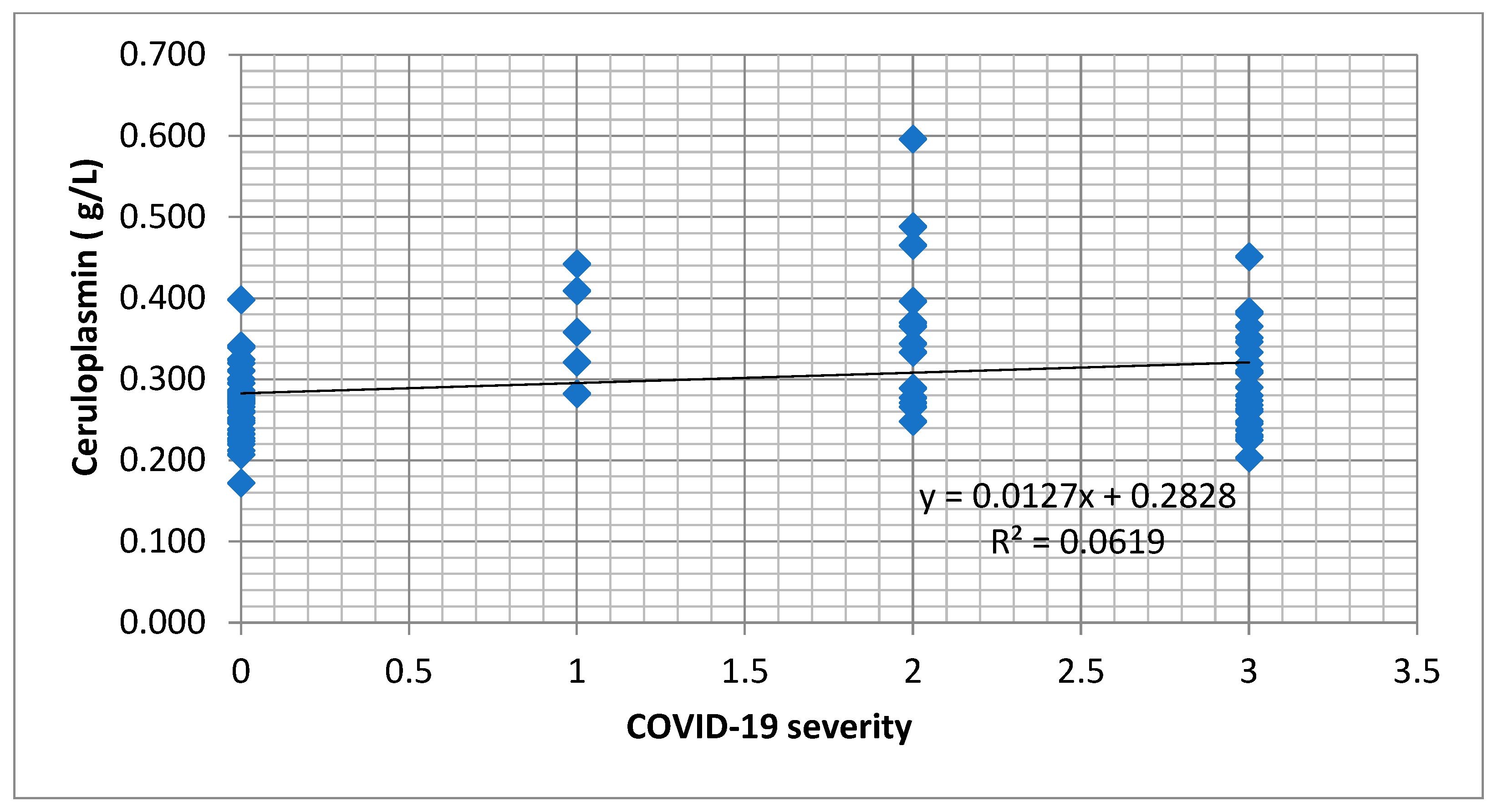
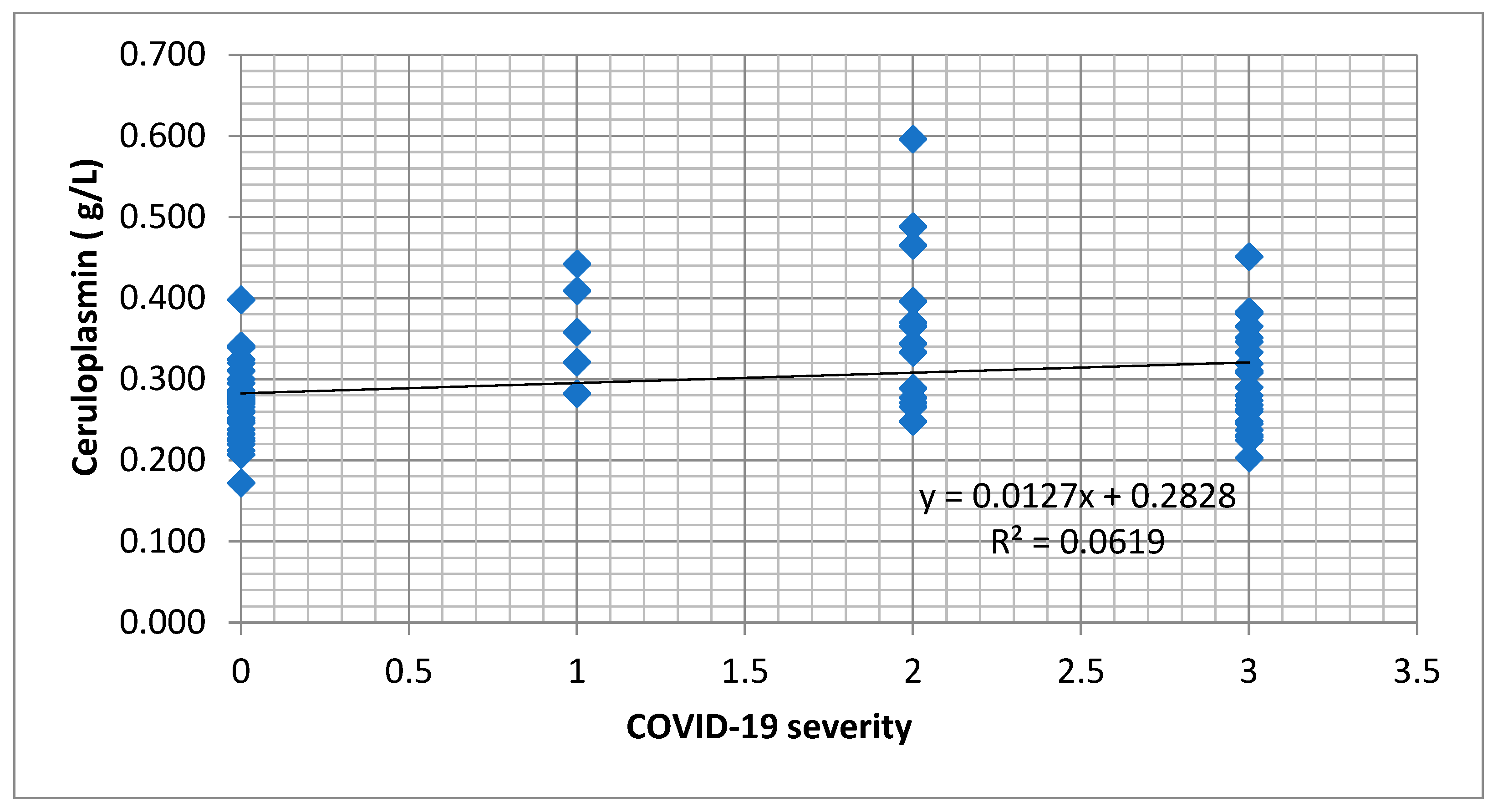
The serum ceruloplasmin was statistically significant and directly correlated with the severity of the SARS-CoV-2 infection, and also with IL-6, but inversely correlated with serum iron levels. However, ceruloplasmin did not statistically significantly correlate with transferrin, ACE, or age (
Table 2). We identified an increasing tendency of the ceruloplasmin concentration depending on the level of infection with COVID-19 (
Figure 1).
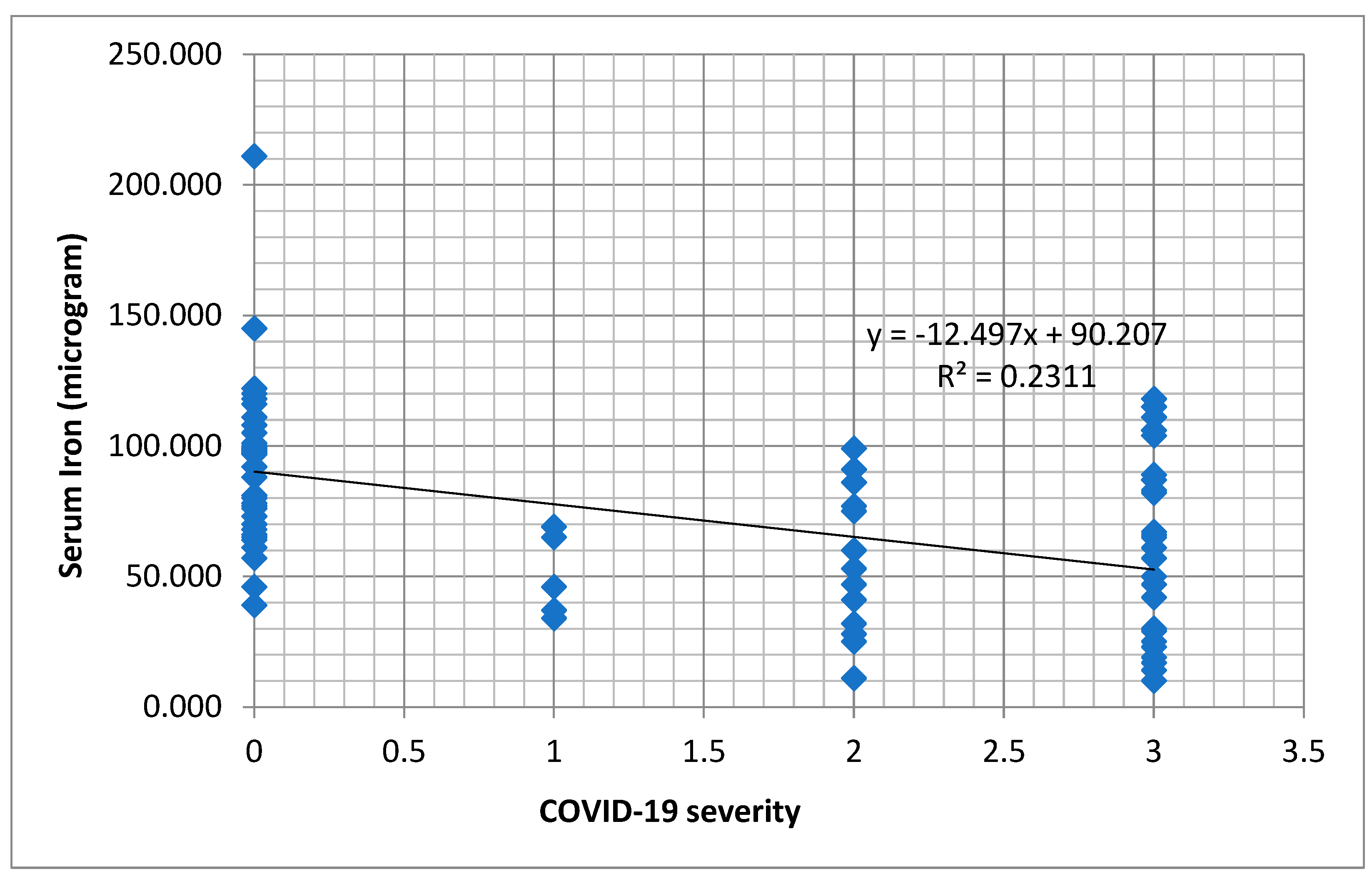
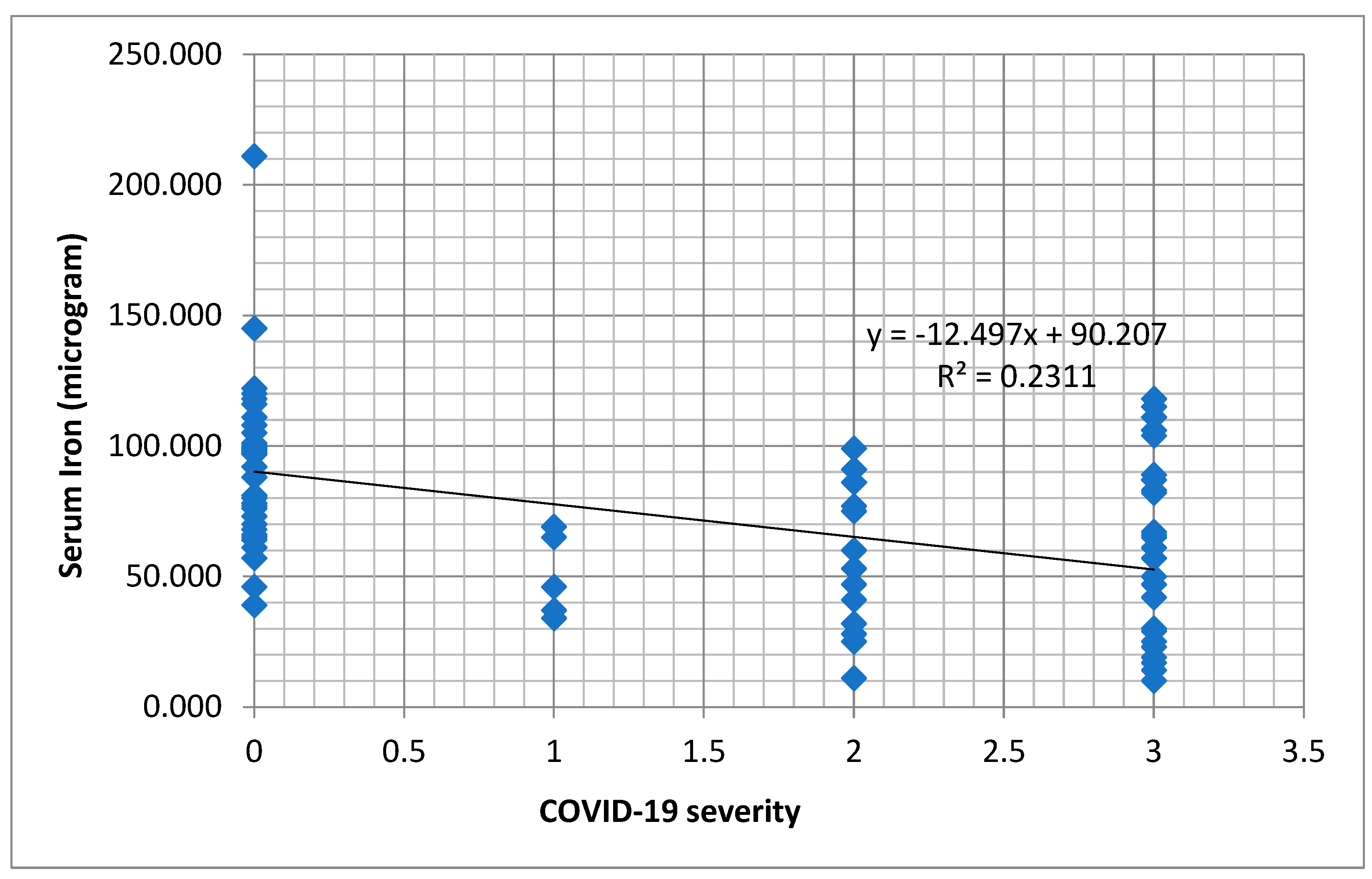
In the case of serum iron level, this parameter correlated strongly and significantly (
p < 0.001) and inversely with the severity of COVID-19, ceruloplasmin, age, and IL-6 (
Table 3). A decreasing tendency of serum iron values was observed in dependence with the severity of the COVID-19 infection (
Figure 2).
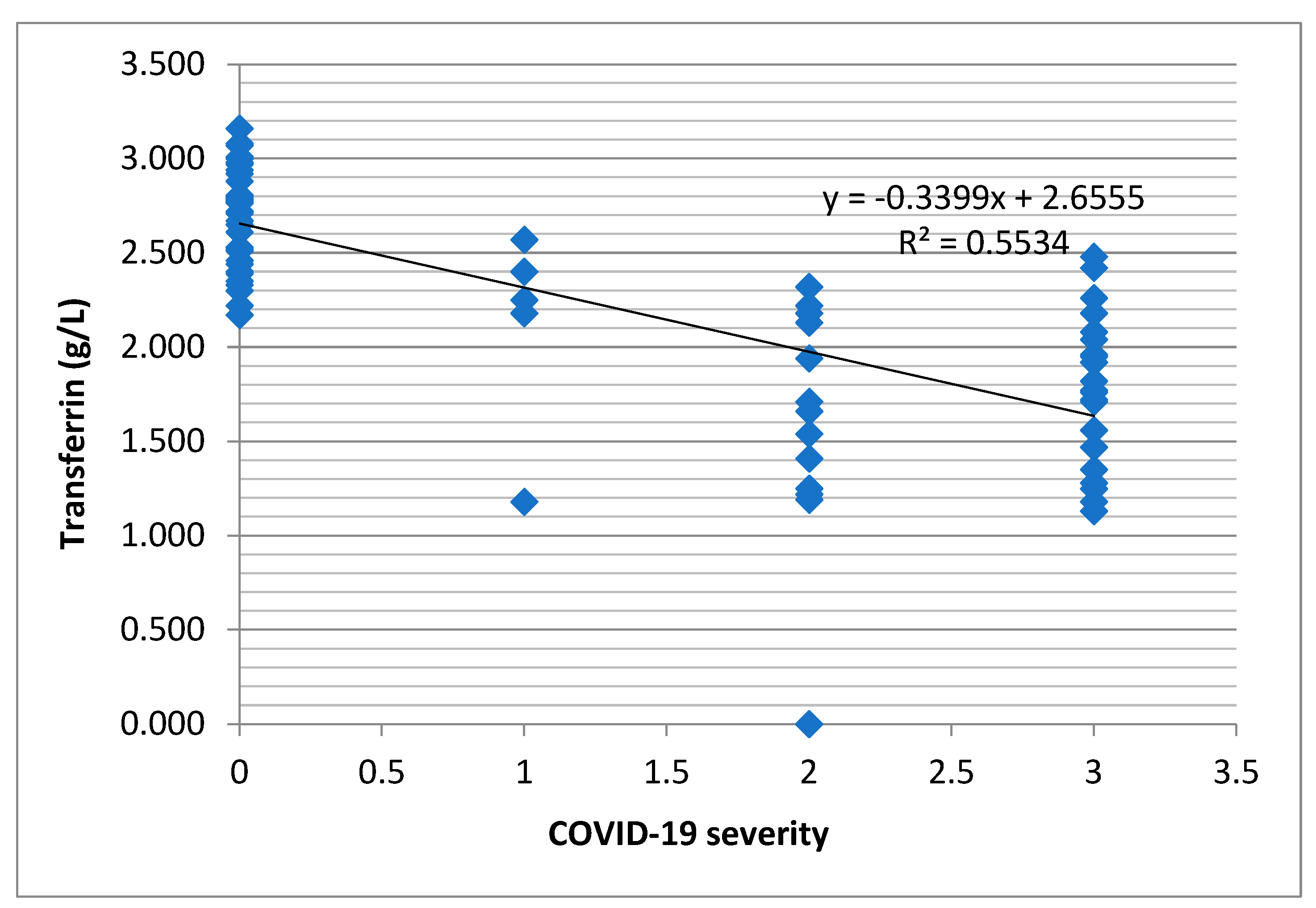
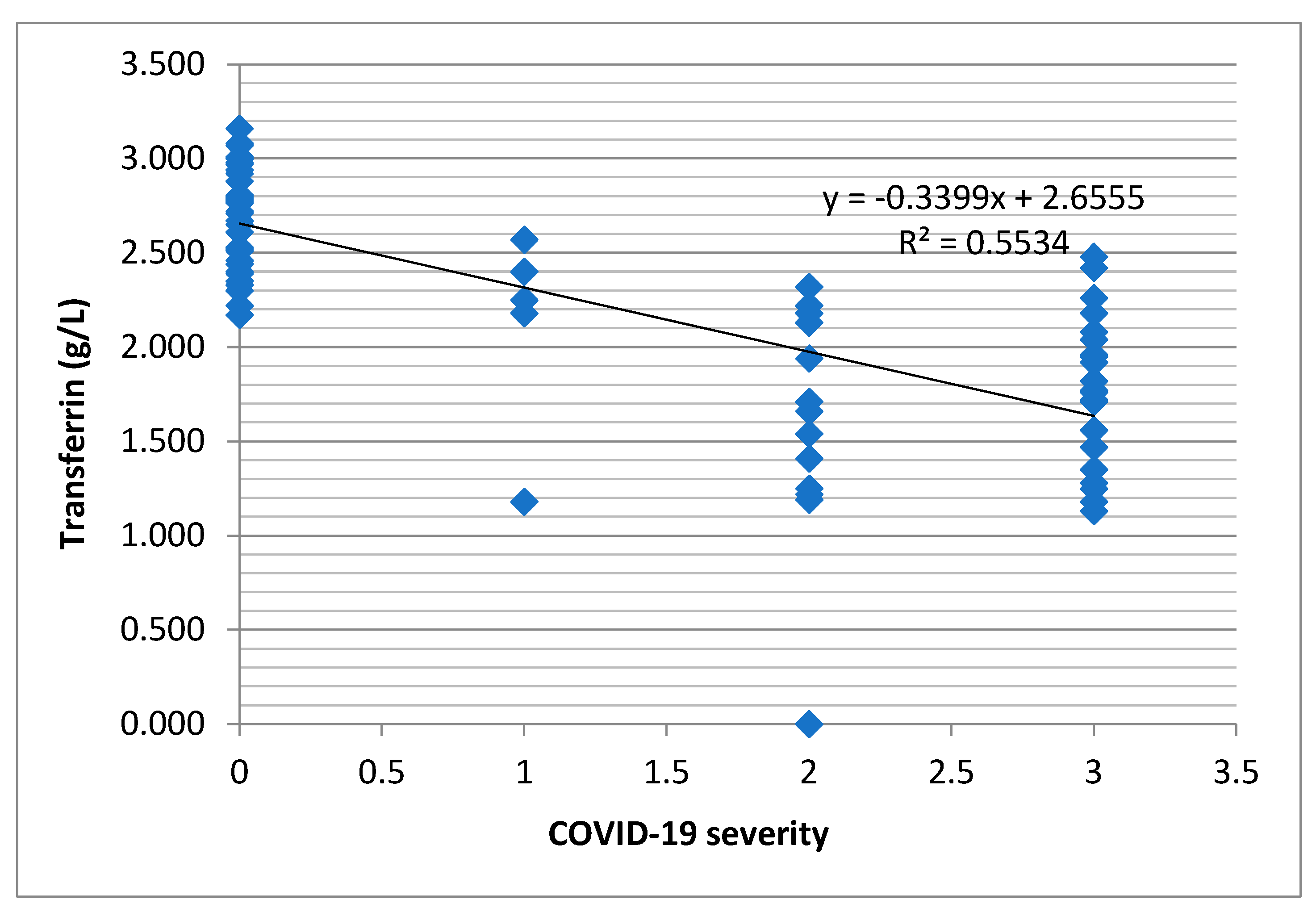
A strong and statistically significant but inverse correlation with the severity of COVID-19, IL-6, and age was observed in this study (
p = 0.001). Transferrin did not correlate significantly with serum ceruloplasmin (
Table 4). However, there was a decreasing tendency of the transferrin level depending on the severity of the COVID-19 infection (
Figure 3).
Age was strongly significant and directly correlated with IL-6. However, age correlated strongly and significantly but inversely with ACE, transferrin, and serum iron (
Table 5).
The ACE concentration was strongly correlated and statistically significant (
p = 0.001), but inversely correlated with the severity of COVID-19, age, and IL-6 (
Table 6).
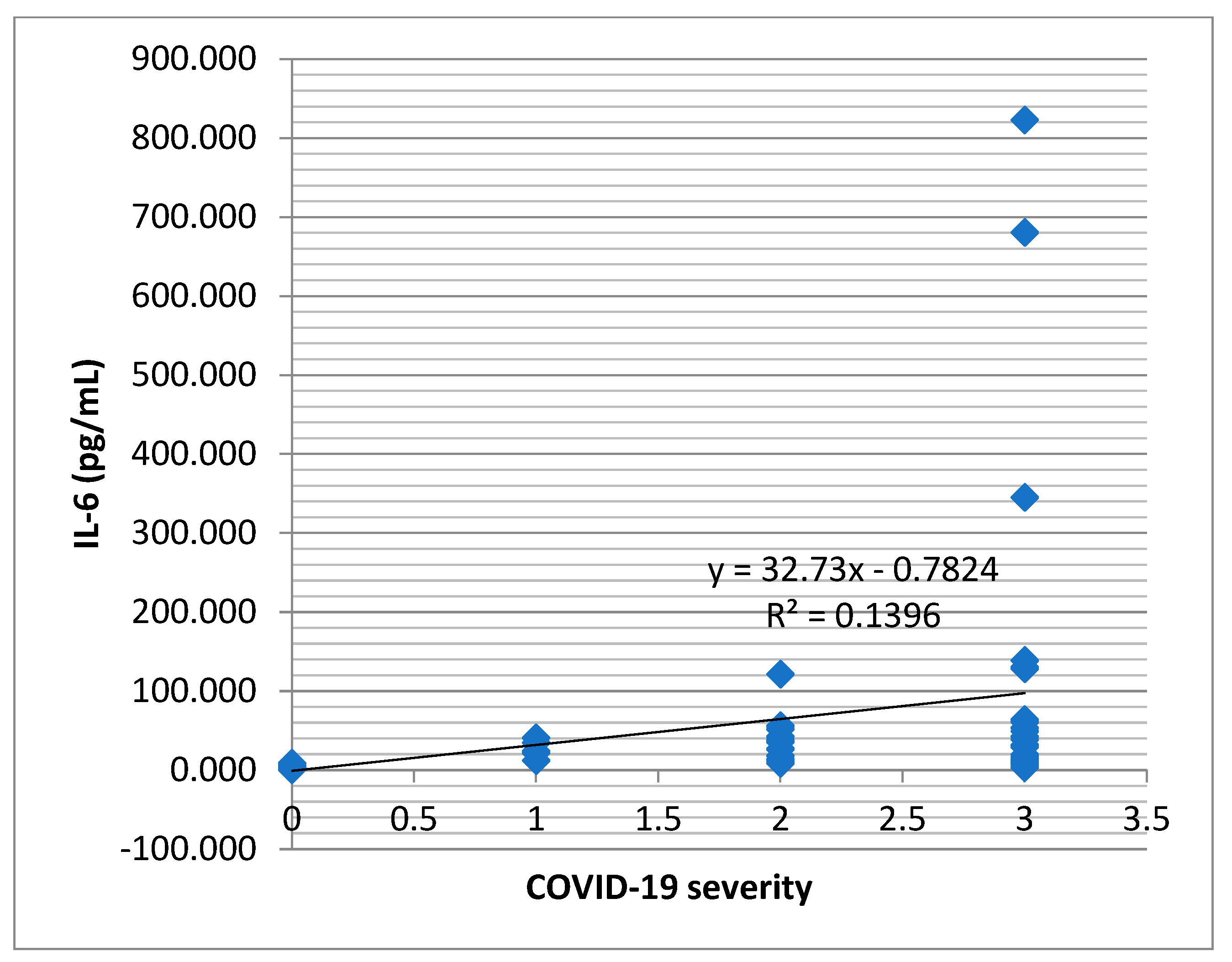
IL-6 correlated non-parametrically (Spearman) but was strongly statistically significant and directly correlated with the severity of the COVID-19 infection, age, and ceruloplasmin (
p < 0.001). An inverse correlation was noticed between IL-6 and transferrin, and ACE and serum iron. (
Table 7). An increasing tendency of the IL-6 concentration was observed to be dependent on the severity of the COVID-19 infection (
Figure 4).
The severity of COVID-19 correlated statistically significantly with all quantitative parameters of the study. Good (|Ro| > 0.5), very good (|Ro| > 0.75), and strongly statistically significant correlations were established between the COVID-19 severity and IL-6, age, and transferrin levels. In addition, the severity of COVID-19 correlated directly (Ro > 0) with IL-6, age, and ceruloplasmin levels. Inverse correlation (Ro < 0) appeared between the COVID-19 severity and serum iron, ACE, and transferrin levels (
Table 8).
Within the group of the diabetic patients with SARS-CoV-2 virus infections, we evaluated possible correlations between the serum level of CRP, LDH, D-dimers, number of lymphocytes, INR, ceruloplasmin, and the COVID-19 severity. Moreover, the severity of COVID-19 correlated strongly and significantly (
p < 0.01) with D-dimers and lymphocyte numbers (
Table 9).
For the patients with COVID-19, we observed that IL-6 correlated non-parametrically (Spearman) and significantly (
p < 0.05) with the numbers of neutrophils, platelets, and serum iron levels. Neutrophils, platelets, and serum iron showed a significant decreasing tendency when IL-6 increases (Spearman correlation coefficient Ro < 0). IL-6 correlated strongly and significantly (
p < 0.01) with CRP (
Table 10).
Serum iron, ACE, ceruloplasmin, and transferrin did not differ statistically or significantly for the female gender compared to the male gender (
p > 0.05) (
Table 11). In addition, ferritin, hemoglobin, RBC (red blood cell), glycemia, CRP, LDH, and fibrinogen did not differ statistically or significantly for the female gender compared to the male gender (
p > 0.05) (
Table 12).
The multiple linear regression model between serum iron (as the dependent parameter) and ceruloplasmin, hemoglobin, RBC, platelets number, and fibrinogen (as the independent parameters) can be expressed by the following equation:
The multiple correlation coefficient (R = 0.942, R
square = 0.871) in this model was strongly and statistically significant (
p < 0.001), indicating that the serum iron variation was due in a proportion of 87.1% to predictor parameters such as ceruloplasmin, hemoglobin, RBC, and platelets number. Therefore, this regression model gave a good enough estimation of serum iron parameters (
Table 13 and
Table 14).
4. Discussions
During the pandemic, certain markers of poor prognoses and increased mortality were identified in patients infected with the SARS-CoV-2 virus [
53,
54,
55,
56]. Among the first common markers of severity recognized in COVID-19 infection were advancing age, presence of metabolic and cardiovascular comorbidities, increased ferritin, and high levels of pro-inflammatory cytokines, especially increased IL-6 [
57,
58]. In the studies of patients with newly diagnosed type 2 diabetes and SARS-CoV-2, high ferritin levels, increased CRP, and decreased lymphocyte count were more evident than in patients without comorbidity (without type 2 diabetes) [
59,
60,
61]. In a recent article, it was stated that associations between significantly elevated levels of serum ferritin, D-dimers, and CRP in patients with COVID-19 requiring transfers to intensive care units have been reported in the literature [
62,
63].
In other studies, the link between high ferritin levels, decreased serum transferrin, and increased CRP levels in the pro-inflammatory state from the COVID-19 infection was presented [
64,
65]. In our study, the severity of COVID-19 was correlated strongly and significantly (
p < 0.01) with D-dimers and lymphocytes number.
In this research, ferritin, hemoglobin, RBC (red blood cell), glycemia, CRP, LDH, and fibrinogen did not differ statistically or significantly for the female gender compared to the male gender. In addition, serum iron, ACE, ceruloplasmin, and transferrin did not differ statistically or significantly for the female gender compared to the male gender.
There are studies about decreased serum transferrin and decreased transferrin saturation, but also increased hepcidin levels were associated with severe forms of COVID-19 infections [
66,
67,
68]. High levels of ferritin, as an acute phase reactant, have been reported in many studies as a negative prognostic marker [
69]. There are theories proposed for transferrin levels as a possible central element of pathogenicity in SARS-CoV-2 infections [
70].
The mechanism of action of serum iron in patients with COVID-19 is not fully elucidated; in the literature, it has been assumed that a decrease in serum iron may be associated with an increase in hepcidin level and with high ferritin levels [
71]. Concerning iron metabolism, there are certain studies demonstrating the decrease in serum iron as a marker associated with the increased risk of mortality due to SARS-CoV-2 infections [
72,
73]. Decreased serum iron has been shown to be a predictor of severe forms of COVID-19 infections [
74,
75,
76].
In the present study, we evaluated other new possible markers of COVID-19 severity at hospital admission and their associations by comparing serum levels of ceruloplasmin, IL-6, serum iron, transferrin, and ACE in 45 healthy control subjects versus 45 type-2 diabetic patients infected with the SARS-CoV-2 virus, all randomly chosen.
We identified that serum ceruloplasmin increased in severe forms of the infection, being a possible new marker of COVID-19 severity. We also found that there was a strong connection between increased serum ceruloplasmin and increased IL-6 levels. Thus, a possible explanation could be the fact that the increased level of ceruloplasmin could also signal a possible negative evolution, with cytokine storms in these patients, through the correlation with the high level of IL-6. Increased IL-6 level in patients with COVID-19 has been associated in other studies with the cytokine storm, with increased levels of pro-inflammatory cytokines such as IL-6, IL-7, IL-10, and IL-1B being present in patients with severe forms and with a negative impact on the endothelial function [
77,
78,
79,
80]. In our research, increased IL-6 was statistically significant and correlated with decreased serum iron, decreased serum ACE, and decreased transferrin. Julian Hackler et al. presented a possible connection between survival in COVID-19 infections, elevated serum copper levels, and a slight ceruloplasmin increase tendency [
81].
Analysis of serum iron in our study revealed a statistically significant correlation between decreased serum iron and the severity of the SARS-CoV-2 infection. We also found that the decrease in serum iron was correlated with the increase in serum ceruloplasmin, IL-6 level, and age. IL-6 is involved in the production of hepcidin, which is a peptide hormone that ensures iron homeostasis [
82]. Marco Ciotti et al. presented the association between hepcidin values and the transfer to intensive care in patients infected with the SARS-CoV-2 virus, but they did not identify significant differences in serum iron levels between survivors and deceased [
68].
For the patients included in our study, we observed that the decrease in the serum level of ACE was significantly correlated with severe forms of infection and with the increase in IL-6, so the low level of ACE could represent a new possible marker of severity in patients with COVID-19. We have not identified in the literature reliable data related to the role of ACE in patients with COVID-19 or in patients with type-2 diabetes and a SARS-CoV-2 virus infection, although the role of ACE 2 (angiotensin-converting enzyme 2) in the infection with the new coronavirus has been intensively studied and presented [
83,
84,
85]. ACE is produced by kidneys and lungs, present in vascular structures, a component of the renin-angiotensin-aldosterone system together with ACE2, and is important in cardiovascular and renal homeostasis. ACE and ACE2 are metallopeptidases, glycoproteins that metabolize circulating peptides, but ACE and ACE2 are functionally different. ACE mainly acts as a carboxypeptidase, converting angiotensin I into angiotensin II, by removing the terminal dipeptide C; also, through ACE, angiotensin 1-9 can be converted to angiotensin 1-7. ACE2 has an enzymatic role by regulating the renin-angiotensin-aldosterone system, but also the kinin-kallikrein system; ACE2 also has a non-enzymatic function representing the entry receptor of the SARS-CoV-2 virus into the human body. The serum level of ACE did not correlate statistically or significantly with the level of serum ceruloplasmin for the patients included in this study [
86,
87].
By analyzing new possible negative prognostic markers at hospital admission, and their association with the others severity markers in the infection with the new coronavirus, we identified a significant statistical correlation between ceruloplasmin (part of iron metabolism), severe forms of COVID-19, and the number of lymphocytes. Lymphopenia, as evidence of immune suppression and a marker of severity in COVID-19 infections, was identified in the patients from our study.
Other studies have shown the connection between the decrease in serum iron, hemoglobin, and hypoxia in patients with COVID-19, but also the connection between high ferritin levels and the stimulation of the expression of pro-inflammatory cytokines by macrophages including IL-6 [
88].
One of the findings of our study was the tendency for decreased numbers of platelets (as coagulation parameters), neutrophils count, and an association with increased IL-6 cytokine levels. On the other hand, the level of IL-6 was directly influenced by the increase in CRP level at hospitalization.
Data from the literature regarding patients with diabetes and COVID-19 infections also mentioned that the predictors of mortality such as lymphopenia, ferritinemia, and increased CRP and D-dimers were more evident than in nondiabetic patients [
89,
90,
91].
In other studies, troponin levels were an independent predictor of severity and mortality in patients with SARS-CoV-2 infections [
92,
93].
Another important finding from our study was that ceruloplasmin and transferrin (as parameters of iron metabolism) at admission and their connection with ACE could show the evolution in the direction of severe forms of COVID-19.
In this research, the regression model for serum iron and ceruloplasmin parameters was also analyzed and it was observed that serum ceruloplasmin, hemoglobin, erythrocytes, and platelets count strongly and significantly influenced serum iron in patients with the SARS-CoV-2 virus at hospital admission.
The limitations of this study include the following: quite low number of patients, single-center study, and parameters evaluated at hospital admission. Future studies on much larger groups and with other pro-inflammatory cytokine are needed.


 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}