
Antibacterial, Antibiofilm, and Anti-Inflammatory Activities of Ginger Extract against Helicobacter pylori

Abstract
:1. Introduction
2. Materials and Methods
2.1. Zingiber officinale
Extraction of Z. officinale (ZO) Preparation
2.2. Antibiotic Susceptibility of H. pylori Isolates
2.3. Anti H. pylori Activity of (ZO) Extract
2.3.1. Determination of Minimum Inhibitory Concentrations (MICs) of (ZO) Extract
2.3.2. Checkerboard Assay
2.4. Antibiofilm Activity of Methanolic Extract of Z. officinale
2.5. Anti-Inflammatory Assay by Human RBCs
2.6. Identification of Chemicals That Constitute Z. officinale Extract by GC-MS
2.7. Statistical Analysis
3. Results and Discussion
3.1. Antibiotics Profile of H. pylori Isolates
3.2. Antibacterial Activity and Minimum Inhibitory Concentration of Z. officinale Extract
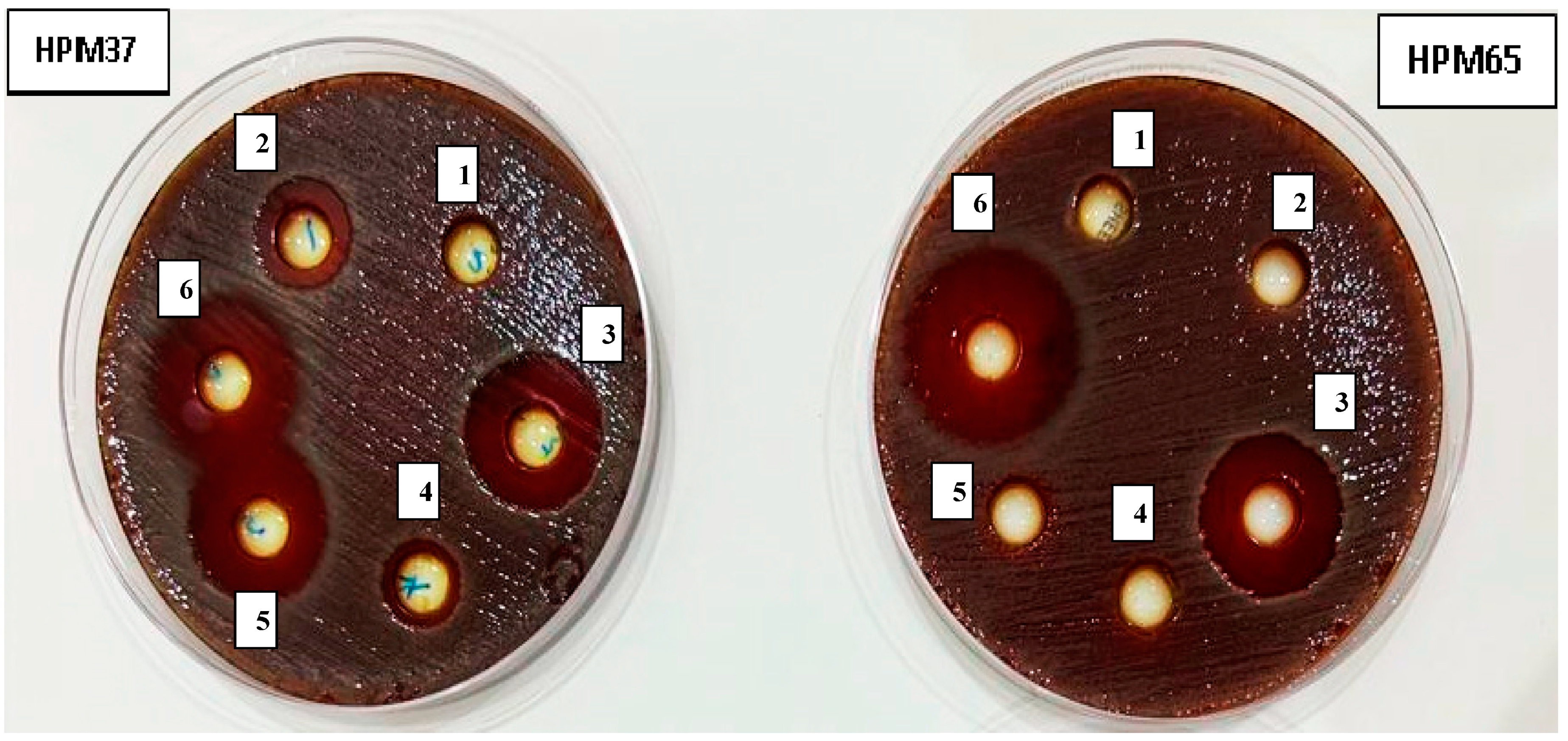
3.3. Synergistic Effect of Gentamicin Combination with Z. officinale Extract against Resistant H. pylori Isolate HPM72
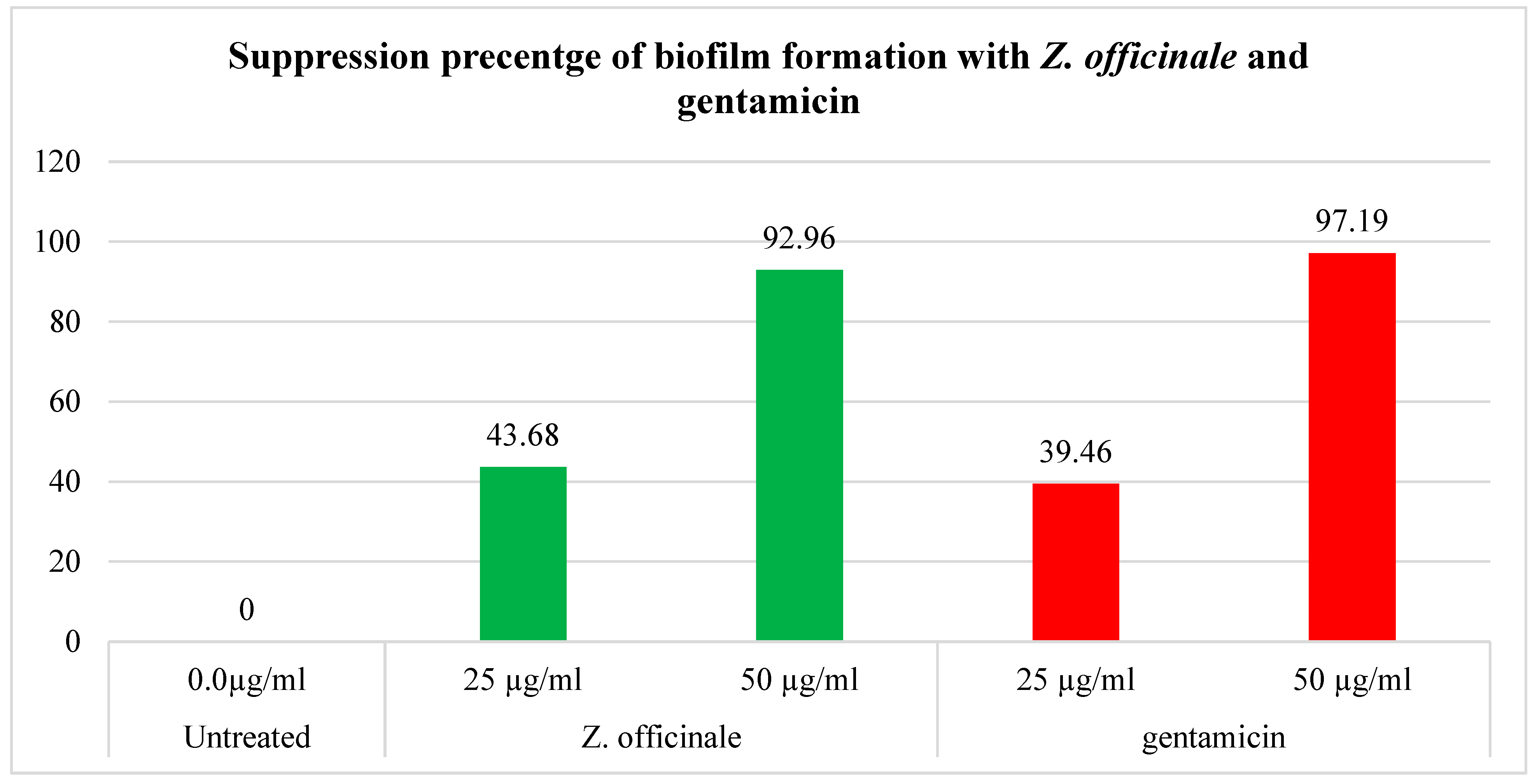
3.4. Antibiofilm Activity of Z. officinale Extract
3.5. Anti-Inflammatory Activity of Z. officinale Extract
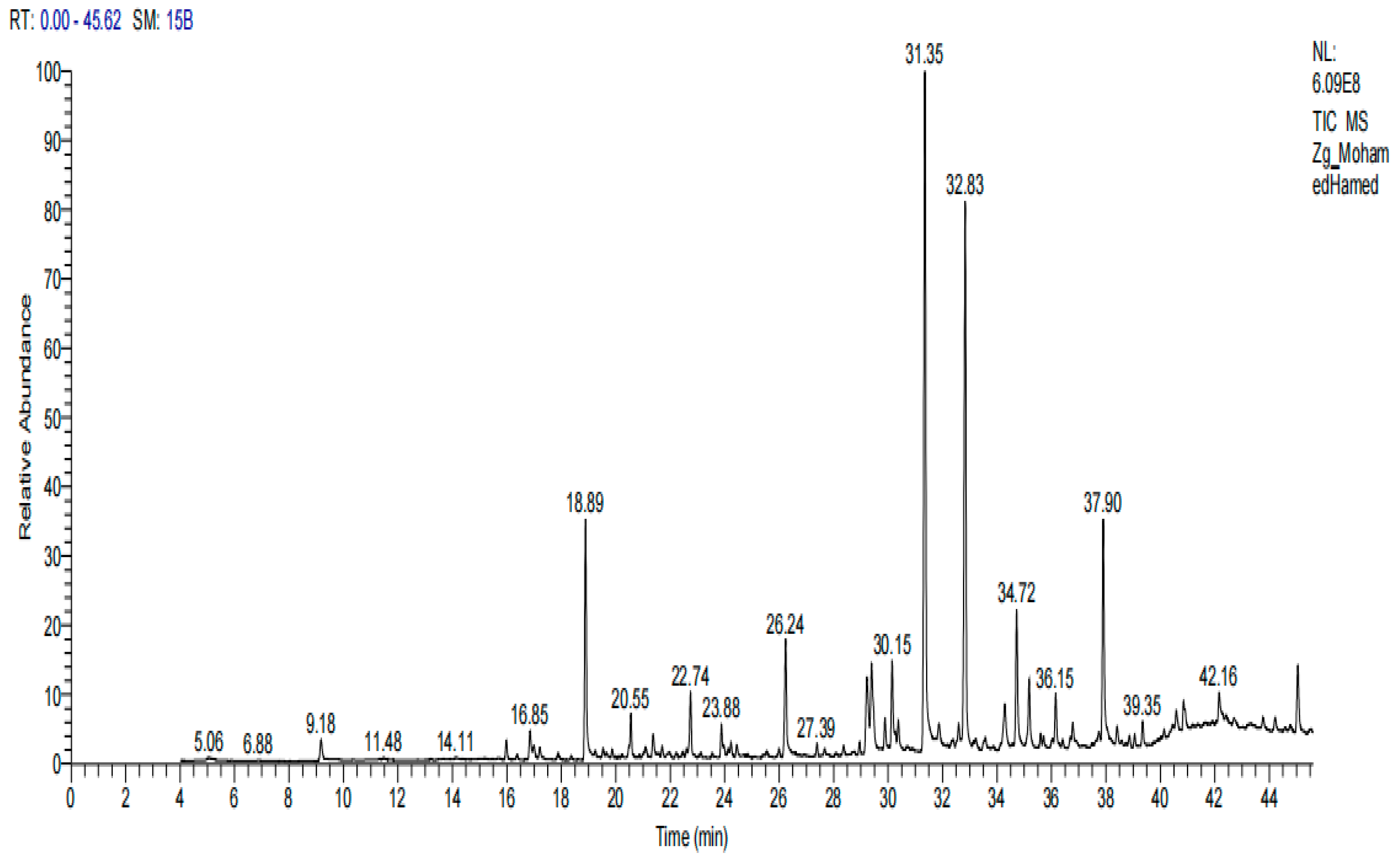
3.6. Chemical Composition of Z. officinale Extract
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- El-Sherbiny, G.M.; Mahmoud, K.M. A review—Plant essential oils active against Helicobacter pylori. J. Essent. Oil Res. 2022, 34, 203–215. [Google Scholar] [CrossRef]
- Hou, C.; Yin, F.; Wang, S.; Zhao, A.; Li, Y.; Liu, Y. Helicobacter pylori Biofilm-Related Drug Resistance and New Developments in Its Anti-Biofilm Agents. Infect. Drug Resist. 2022, 15, 1561–1571. [Google Scholar] [CrossRef] [PubMed]
- Hathroubi, S.; Zerebinski, J.; Clarke, A.; Ottemann, K.M. Helicobacter pylori biofilm confers antibiotic tolerance in part via a protein-dependent mechanism. Antibiotics 2020, 9, 355. [Google Scholar] [CrossRef] [PubMed]
- Okshevsky, M.; Meyer, R.L. The role of extracellular DNA in the establishment, maintenance and perpetuation of bacterial biofilms. Crit. Rev. Microbiol. 2015, 41, 341–352. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.F.; Hager, P.W.; Howell, M.L.; Phibbs, P.V.; Hassett, D.J. Cloning and characterization of the Pseudomonas aeruginosa zwf gene encoding glucose-6-phosphate dehydrogenase, an enzyme important in resistance to methyl viologen (paraquat). J. Bacteriol. 1998, 180, 1741–1749. [Google Scholar] [CrossRef] [PubMed]
- Dunn, B.E.; Cohen, H.; Blaser, M.J. Helicobacter pylori. Clin. Microbiol. Rev. 1997, 10, 720–741. [Google Scholar] [CrossRef]
- Blaser, M.J. Helicobacter pylori: Its role in disease. Clin. Infect. Dis. 1992, 15, 386–393. [Google Scholar] [CrossRef]
- Graham, D.Y. Campylobacter pylori and peptic ulcer disease. Gastroenterology 1989, 96 (Suppl. S2), 615–625. [Google Scholar] [CrossRef] [PubMed]
- Parsonnet, J.; Friedman, G.D.; Vandersteen, D.P.; Chang, Y.; Vogelman, J.H.; Orentreich, N.; Sibley, R.K. Helicobacter pylori infection and the risk of gastric carcinoma. N. Engl. J. Med. 1991, 325, 1127–1131. [Google Scholar] [CrossRef]
- Wotherspoon, A.C.; Diss, T.C.; Pan, L.; Isaacson, P.G.; Doglioni, C.; Moschini, A.; De Boni, M. Regression of primary low-grade-B-cell gastric lymphoma of mucosa associated lymphoid tissue type after eradication of Helicobacter pylori. Lancet 1993, 342, 575–577. [Google Scholar] [CrossRef]
- International Agency for Research on Cancer (IARC); World Health Organization. Schistosomes, liver flukes, and Helicobacter pylori. In Monographs on the Evaluation of Carcinogenic Risks; WHO: Geneva, Switzerland, 1994. [Google Scholar]
- Bonifácio, B.V.; dos Santos Ramos, M.A.; Da Silva, P.B.; Bauab, T.M. Antimicrobial activity of natural products against Helicobacter pylori: A review. Ann. Clin. Microbiol. Antimicrob. 2014, 13, 54. [Google Scholar] [CrossRef]
- Stark, R.M.; Gerwig, G.J.; Pitman, R.S.; Potts, L.F.; Williams, N.A.; Greenman, J.; Weinzweig, I.P.; Hirst, T.R.; Millar, M.R. Biofilm formation by Helicobacter pylori. Lett. Appl. Microbiol. 1999, 28, 121–126. [Google Scholar] [CrossRef]
- Cole, S.P.; Harwood, J.; Lee, R.; She, R.; Guiney, D.G. Characterization of monospecies biofilm formation by Helicobacter pylori. J. Bacteriol. 2004, 186, 3124–3132. [Google Scholar] [CrossRef] [PubMed]
- Cellini, L.; Grande, R.; Di Campli, E.; Di Bartolomeo, S.; Di Giulio, M.; Traini, T.; Trubiani, O. Characterization of a Helicobacter pylori environmental strain. J. Appl. Microbiol. 2008, 105, 761–769. [Google Scholar] [CrossRef]
- Hsu, P.I.; Wu, D.C.; Chen, W.C.; Tseng, H.H.; Yu, H.C.; Wang, H.M.; Kao, S.S.; Lai, K.H.; Chen, A.; Tsay, F.W. Randomized controlled trial comparing 7-day triple, 10-day sequential, and 7-day concomitant therapies for Helicobacter pylori infection. Antimicrob. Agents Chemother. 2014, 58, 5936–5942. [Google Scholar] [CrossRef] [PubMed]
- Sharaf, M.H.; El-Sherbiny, G.M.; Moghannem, S.A.; Abdelmonem, M.; Elsehemy, I.A.; Metwaly, A.M.; Kalaba, M.H. New combination approaches to combat methicillin-resistant Staphylococcus aureus (MRSA). Sci. Rep. 2021, 11, 4240. [Google Scholar] [CrossRef]
- Vale, F.F.; Oleastro, M. Overview of the phytomedicine approach against Helicobacter pylori. World J. Gastroenterol. 2014, 20, 5594–5609. [Google Scholar] [CrossRef]
- Wang, Y.C. Medicinal plant activity on Helicobacter pylori-related diseases. World J. Gastroenterol. 2014, 20, 10368–10382. [Google Scholar] [CrossRef]
- Mahady, G.B.; Pendland, S.L.; Yun, G.S.; Lu, Z.; Stoia, A. Ginger (Zingiber officinale Roscoe) and the Gingerols Inhibit the Growth of Cag A+ Strains of Helicobacter pylori. Anticancer Res. 2003, 23, 3699–3702. [Google Scholar] [PubMed]
- Ohno, T.; Kita, M.; Yamaoka, Y.; Imamura, S.; Yamamoto, T.; Mitsufuji, S.; Kodoma, K.; Kashima, T.; Imanishi, J. Antimicrobial activity of essential oils against Helicobacter pylori. Helicobacter 2003, 8, 207–215. [Google Scholar] [CrossRef]
- Song, M.Y.; Lee, D.Y.; Park, S.Y.; Seo, S.A.; Hwang, J.S.; Heo, S.H.; Kim, E.H. Steamed Ginger Extract Exerts Anti-inflammatory Effects in Helicobacter pylori-infected Gastric Epithelial Cells through Inhibition of NF-κB. J. Cancer Prev. 2021, 26, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Clinical and Laboratory Standards Institute (CLSI). 2020 Guidelines (M7-A5); CLSI: Wayne, PA, USA, 2020. [Google Scholar]
- Parekh, J.; Chanda, S. Antibacterial phytochemical studies on twelve species of Indian medicinal plants. Afr. J. Biomed. Res. 2007, 10, 175–181. [Google Scholar] [CrossRef]
- Foda, A.M.; Kalaba, M.H.; El-Sherbiny, G.M.; Moghannem, S.A.; El-Fakharany, E.M. Antibacterial activity of essential oils for combating colistin-resistant bacteria Expert Rev. Anti-Infect. Ther. 2022, 20, 1351–1364. [Google Scholar] [CrossRef] [PubMed]
- Kodori, M.; Nikmanesh, B.; Hakimi, H.; Ghalavand, Z. Antibiotic Susceptibility and Biofilm Formation of Bacterial Isolates Derived from Pediatric Patients with Cystic Fibrosis from Tehran, Iran. Arch. Razi Inst. 2021, 76, 397–406. [Google Scholar]
- Rahman, H.; Eswaraiah, M.C.; Dutta, A. In-vitro anti-inflammatory and anti-arthritic activity of Oryza sativa Var. joha rice (an aromatic indigenous rice of Assam). Am. Eurasian J. Agric Environ. Sci. 2015, 15, 115–121. [Google Scholar]
- El-Sherbiny, G.M.; Gazelly, A.M.; Sharaf, M.H.; Moghannemm, S.A.; Shehata, M.; Ismail, M.K.A.; El-Hawary, A.S. Exploitation of the antibacterial, antibiofilm and antioxidant activities of Salvadora persica (Miswak) extract. J. Bioresour. Bioprod. 2022, 8, 59–65. [Google Scholar] [CrossRef]
- Thung, I.; Aramin, H.; Vavinskaya, V.; Gupta, S.; Park, J.Y.; Crowe, S.E.; Valasek, M.A. Review article: The global emergence of Helicobacter pylori antibiotic resistance. Aliment. Pharmacol. Ther. 2016, 43, 514–533. [Google Scholar] [CrossRef]
- Rasheed, F.; Campbel, B.J.; Alfizah, H.; Varro, A.; Zahra, R.; Yamaoka, Y.; Mark, D. Pritchard Analysis of Clinical Isolates of Helicobacter pylori in Pakistan Reveals High Degrees of Pathogenicity and High Frequencies of Antibiotic Resistance. Helicobacter 2014, 19, 387–399. [Google Scholar] [CrossRef]
- Tan, B.; Yang, J.C.; Young, C.L.; Bishu, S.; Owyang, S.Y.; El-Zaatari, M.; Zhang, M.; Grasberger, H.; Qian, J.M.; Kao, J.Y. Helicobacter pylori Antimicrobial Susceptibility Testing-Guided Salvage Therapy in the USA: A Real Life Experience. Dig. Dis. Sci. 2018, 63, 437–445. [Google Scholar] [CrossRef]
- Tshibangu-Kabamba, E.; Yamaoka, Y. Helicobacter pylori infection and antibiotic resistance—From biology to clinical implications. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 613–629. [Google Scholar] [CrossRef]
- Gaynor, M.; Mankin, A.S. Macrolide antibiotics: Binding site, mechanism of action, resistance. Curr. Top. Med. Chem. 2003, 3, 949–960. [Google Scholar] [CrossRef]
- Correia, S.; Poeta, P.; Hébraud, M.; Capelo, J.L.; Igrejas, G. Mechanisms of quinolone action and resistance: Where do we stand? J. Med. Microbiol. 2017, 66, 551–559. [Google Scholar] [CrossRef]
- Mori, H.; Suzuki, H.; Matsuzaki, J.; Masaoka, T.; Kanai, T. Acquisition of double mutation in gyrA caused high resistance to sitafloxacin in Helicobacter pylori after unsuccessful eradication with sitafloxacin-containing regimens. United Eur. Gastroenterol. J. 2018, 6, 391–397. [Google Scholar] [CrossRef]
- EL-Sherbiny, G.M. Antimicrobial Susceptibility of Bacteria Detected from the Root Canal Infection (Before and After) Root-Filled Teeth: An in Vitro Study. Int. J. Dent. Sci. Res. 2015, 3, 4–9. [Google Scholar] [CrossRef]
- Chakotiya, A.S.; Tanwar, A.; Narula, A.; Sharma, R.K. Zingiber officinale: Its antibacterial activity on Pseudomonas aeruginosa and mode of action evaluated by flow cytometry. Microb. Pathog. 2017, 107, 254–260. [Google Scholar] [CrossRef] [PubMed]
- Jing, Y.; Cheng, W.; Ma, Y.; Zhang, Y.; Li, M.; Zheng, Y.; Zhang, D.; Wu, L. Structural Characterization, Antioxidant and Antibacterial Activities of a Novel Polysaccharide from Zingiber officinale and Its Application in Synthesis of Silver Nanoparticles. Front. Nutr. 2022, 9, 917094. [Google Scholar] [CrossRef]
- Bhattamisra, S.K.; Yean, V.L.; Lee, C.K.; Kuean, C.H.; Candasamy, M.; Liew, Y.K.; Sahu, P.S. Protective activity of geraniol against acetic acid and Helicobacter pylori-induced gastric ulcers in rats. J. Tradit. Complement. Med. 2019, 9, e206–e214. [Google Scholar] [CrossRef]
- Azadi, M.; Ebrahimi, A.; Khaledi, A.; Esmaeili, D. Study of inhibitory effects of the mixture of cinnamon and ginger extracts on cagA gene expression of Helicobacter pylori by Real-Time RT-PCR technique. Gene Rep. 2019, 17, 100493. [Google Scholar] [CrossRef]
- Fatemi, N.; Sharifmoghadam, M.R.; Bahreini, M.; Khameneh, B.; Shadifar, H. Antibacterial and Synergistic Effects of Herbal Extracts in Combination with Amikacin and Imipenem Against Multidrug-Resistant Isolates of Acinetobacter. Curr. Microbiol. 2020, 77, 1959–1967. [Google Scholar] [CrossRef]
- Khameneh, B.; Iranshahy, M.; Ghandadi, M.; Ghoochi Atashbeyk, D.; Fazly Bazzaz, B.S.; Iranshahi, M. Investigation of the antibacterial activity and efflux pump inhibitory effect of co-loaded piperine and gentamicin nanoliposomes in methicillin-resistant Staphylococcus aureus. Drug Dev. Ind. Pharm. 2015, 41, 989–994. [Google Scholar] [CrossRef]
- Lakshmi, B.V.S.; Sudhakar, M. Protective Effect of Zingiber officinale on Gentamicin-Induced Nephrotoxicity in Rats. Int. J. Pharmacol. 2010, 6, 58–62. [Google Scholar]
- Sharma, S.; Mohler, J.; Mahajan, S.D.; Schwartz, S.A.; Bruggemann, L.; Aalinkeel, R. Microbial Biofilm: A Review on Formation, Infection, Antibiotic Resistance, Control Measures, and Innovative Treatment. Microorganisms 2023, 11, 1614. [Google Scholar] [CrossRef] [PubMed]
- Hoyle, B.D.; Wong, C.K.; Costerton, J.W. Disparate efficacy of tobramycin on Ca2+-, Mg2+-, and HEPES-treated Pseudomonas aeruginosa biofilms. Can. J. Microbiol. 1992, 38, 1214–1218. [Google Scholar] [CrossRef] [PubMed]
- Aghazadeh, M.; Bialvaei, A.Z.; Aghazadeh, M.; Kabiri, F.; Saliani, N.; Yousefi, M.; Eslami, H.; Kafil, H.S. Survey of the Antibiofilm and Antimicrobial Effects of Zingiber officinale (in Vitro Study). Jundishapur. J. Microbiol. 2016, 9, e30167. [Google Scholar] [CrossRef]
- Faria, T.R.B.; Furletti-Goes, V.F.; Franzini, C.M.; de Aro, A.A.; de Andrade, T.A.M.; Sartoratto, A.; de Menezes, C.C. Anti-inflammatory and antimicrobial effects of Zingiber officinale mouthwash on patients with fixed orthodontic appliances. Am. J. Orthod. Dentofac. Orthop. 2021, 159, 21–29. [Google Scholar] [CrossRef]
- Kim, H.-S.; Park, H.-D. Ginger Extract Inhibits Biofilm Formation by Pseudomonas aeruginosa PA14. PLoS ONE 2013, 8, e76106. [Google Scholar] [CrossRef]
- Mackay, W.; Gribbon, L.; Barer, M.; Reid, D. Biofilms in drinking water systems: A possible reservoir for Helicobacter pylori. J. Appl. Microbiol. 1998, 85, 52S–59S. [Google Scholar]
- Sarem, M.; Corti, R. Role of Helicobacter pylori coccoid forms in infection and recrudescence. Gastroenterol. Hepatol. 2016, 39, 28–35. [Google Scholar] [CrossRef]
- Elbestawy, M.K.M.; El-Sherbiny, G.M.; Moghannem, S.A. Antibacterial, Antibiofilm and Anti-Inflammatory Activities of Eugenol Clove Essential Oil against Resistant Helicobacter pylori. Molecules 2023, 28, 2448. [Google Scholar] [CrossRef]
- Kadkhodaei, S.; Siavoshi, F.; Akbari Noghabi, K. Mucoid and coccoid Helicobacter pylori with fast growth and antibiotic resistance. Helicobacter 2020, 25, e12678. [Google Scholar]
- Ali, B.H.; Blunden, G.; Tanira, M.O.; Nemmar, A. Some phytochemical, pharmacological and toxicological properties of ginger (Zingiber officinale Roscoe): A review of recent research. Food Chem. Toxicol. 2008, 46, 409–420. [Google Scholar] [CrossRef]
- Charlier, C.; Michaux, C. Dual inhibition of cyclooxygenase-2 (COX-2) and 5-lipoxygenase (5-LOX) as a new strategy to provide safer non-steroidal anti-inflammatory drugs. Eur. J. Med. Chem. 2003, 38, 645–659. [Google Scholar] [CrossRef]
- Grzanna, R.; Lindmark, L.; Frondoza, C.G. Ginger—An herbal medicinal product with broad anti-inflammatory actions. J. Med. Food 2005, 8, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Elbashir, D.M.M.; Kehail, M.A.A.; Mohamed, A.I.A.; Ali, A.E.H. Phytochemistry and GC-MS Screening and Biocidal Potentiality of Ginger (Zingiber officinale) Rhizome against Mosquito’s Larvae. Int. J. Sci. Res. Arch. 2021, 3, 90–96. [Google Scholar] [CrossRef]
- Chinonye, I.I.; Oze, R.N.; Lynda, O.U.; Nkwoada, A.; Adanma, A.U. Phytochemical and GC/MS Analysis of the Rhizome of Zingiber officinale Plant Grown in Eastern Part of Nigeria. Afr. J. Biol. Med. Res. 2018, 1, 43–54. [Google Scholar]
- Choudhari, S.S.; Kareppa, B.M. Identification of Bioactive Compounds of Z. Officinale Roscoe Rhizomes through Gas Chromatography and Mass Spectrometry. Intern. J. Pharmac. Res. Dev. 2013, 5, 16–20. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Class of Antibiotics and Mode of Action | Antibiotic | Potency µg/Disk | Antibiotics Susceptibility | Zone Diameter Breakpoints | H. pylori NCTC 11637 | ||||
|---|---|---|---|---|---|---|---|---|---|
| S. N (%) | I. N (%) | R. N (%) | S | I | R | ||||
| Inhibition of bacterial nucleic acid synthesis | |||||||||
| Fluoroquinolone | Ciprofloxacin | 5 | 45 (58.95) | 0 (0.0) | 31 (40.61) | ≥21 | 16–20 | ≤15 | 22.40 |
| Quinolone | Levofloxacin | 5 | 39 (51.09) | 9 (11.79) | 28 (36.68) | ≥17 | 13–16 | <12 | 20.0 |
| Inhibition of bacterial protein synthesis | |||||||||
| Aminoglycosides | Gentamicin | 10 | 22 (28.82) | 16 (20.96) | 38 (50.0) | ≥15 | 13–14 | ≤12 | 19.70 |
| Neomycin | 30 | 16 (20.96) | 27 (35.37) | 33 (43.23) | 21.0 | ||||
| Macrolides | Erythromycin | 15 | 30 (39.30) | 12 (15.72) | 34 (44.54) | ≥23 | 14–22 | ≤13 | 20.50 |
| Clarithromycin | 15 | 37 (48.47) | 9 (11.79) | 30 (39.30) | ≥21 | 15–20 | ≤14 | 21–70 | |
| Tetracyclines | Tetracycline | 30 | 19 (24.89) | 22 (28.82) | 35 (45.85) | ≥19 | 15–18 | ≤14 | 23–80 |
| Inhibitors of bacterial cell wall synthesis | |||||||||
| Amoxicillin | 25 | 43 (56.33) | 8 (10.48) | 25 (32.75) | ≥13 | 11–12 | ≤10 | 24.30 | |
| Penicillin combination | Amoxicillin-clavulanate | 20/10 | 56 (73.36) | 2 (2.62.) | 18 (23.58) | >19 | - | <20 | 26.30 |
| Metabolic antagonism | |||||||||
| Nitroimidazoles | Metronidazole | 5 | 15 (19.65) | 18 (23.58) | 43 (56.33) | >21 | 16–21 | <16 | 18.70 |
| No. | Strains Code | Minimum Inhibitory Concentration (μg/mL) | No. | Strains Code | Minimum Inhibitory Concentration (μg/mL) | ||
|---|---|---|---|---|---|---|---|
| Z. officinale Extract | Gentamicin | Z. officinale Extract | Gentamicin | ||||
| 1 | HPM4 | 25.0 | 13.0 | 14 | HPM48 | 39.0 | 17.0 |
| 2 | HPM7 | 27.0 | 13.0 | 15 | HPM51 | 28.0 | 13.0 |
| 3 | HPM9 | 22.0 | 13.0 | 16 | HPM54 | 23.0 | 15.0 |
| 4 | HPM12 | 25.0 | 13.0 | 17 | HPM57 | 29.0 | 15.0 |
| 5 | HPM15 | 29.0 | 13.0 | 18 | HPM62 | 38.0 | 18.0 |
| 6 | HPM16 | 32.0 | 15.0 | 19 | HPM63 | 50.0 | 15.0 |
| 7 | HPM19 | 22.0 | 12.0 | 20 | HPM65 | 27.0 | 15.0 |
| 8 | HPM26 | 23.0 | 12.0 | 21 | HPM66 | 33.0 | 15.0 |
| 9 | HPM37 | 33.0 | 15.0 | 22 | HPM70 | 46.0 | 19.0 |
| 10 | HPM44 | 26.0 | 15.0 | 23 | HPM72 | 42.0 | 17.0 |
| 11 | HPM48 | 35.0 | 15.0 | 24 | HPM73 | 35.0 | 15.0 |
| 12 | HPM52 | 37.0 | 16.0 | 25 | HPM75 | 48.0 | 19.0 |
| 13 | HPM56 | 44.0 | 17.0 | 26 | H. pylori NCTC 11637 | 20.0 | 7.0 |
| No. | Strains Code | Mean of Inhibition Zone Diameter (mm ± SD) | No. | Strains Code | Mean of Inhibition Zone Diameter (mm ± SD) | ||
|---|---|---|---|---|---|---|---|
| Z. officinale Extract | Gentamicin 10 µg/mL | Z. officinale Extract | Gentamicin 10 µg/ml | ||||
| 1 | HPM4 | 14 ± 00 | 0.0 | 14 | HPM48 | 12 ± 05 | 0.0 |
| 2 | HPM7 | 13 ± 09 | 0.0 | 15 | HPM51 | 15 ± 20 | 0.0 |
| 3 | HPM9 | 12 ± 05 | 0.0 | 16 | HPM54 | 24 ± 04 | 0.0 |
| 4 | HPM12 | 11 ± 05 | 0.0 | 17 | HPM57 | 14 ± 06 | 0.0 |
| 5 | HPM15 | 15 ± 09 | 0.0 | 18 | HPM62 | 12 ± 04 | 0.0 |
| 6 | HPM16 | 13 ± 03 | 0.0 | 19 | HPM63 | 13 ± 06 | 0.0 |
| 7 | HPM19 | 15 ± 00 | 0.0 | 20 | HPM65 | 16 ± 00 | 0.0 |
| 8 | HPM26 | 12 ± 04 | 0.0 | 21 | HPM66 | 11 ± 04 | 0.0 |
| 9 | HPM37 | 16 ± 00 | 0.0 | 22 | HPM70 | 10 ± 03 | 0.0 |
| 10 | HPM44 | 11 ± 06 | 0.0 | 23 | HPM72 | 12 ± 07 | 0.0 |
| 11 | HPM48 | 15 ± 08 | 0.0 | 24 | HPM73 | 14 ± 08 | 0.0 |
| 12 | HPM52 | 12 ± 00 | 0.0 | 25 | HPM75 | 15 ± 08 | 0.0 |
| 13 | HPM56 | 14 ± 06 | 0.0 | 26 | H. pylori NCTC 11637 | 17 ± 06 | 20 ± 04 |
| No. | MIC Gentamicin + MIC ZO Extract | Gentamicin + ZO Extract (µg/mL) | FICI Gentamicin + FICI ZO Extract | FICI | Interpretation |
|---|---|---|---|---|---|
| 1 | MIC + MIC | 42 + 33 | 1 + 1 | 2 | Indifference |
| 2 | MIC + 1/2MIC | 42 + 16.5 | 1 + 0.5 | 1.5 | additive |
| 3 | MIC + 1/4MIC | 42 + 8.25 | 1 + 0.25 | 1.25 | additive |
| 4 | MIC + 1/8MIC | 42 + 4.13 | 1 + 0.125 | 1.125 | additive |
| 5 | MIC + 1/16MIC | 42 + 2.06 | 1 + 0.062 | 1.062 | additive |
| 6 | MIC + 1/32MIC | 42 + 1.03 | 1 + 0.031 | 1.031 | additive |
| 7 | MIC + 1/64MIC | 42 + 0.51 | 1 + 0.015 | 1.015 | additive |
| 8 | MIC + 1/128MIC | 42 + 0.25 | 1 + 0.007 | 1.007 | additive |
| 9 | 1/2MIC + MIC | 21 + 33 | 0.5 + 1 | 1.5 | additive |
| 10 | 1/2MIC + 1/2MIC | 21 + 16.5 | 0.5 + 0.5 | 1 | partial synergy |
| 11 | 1/2MIC + 1/4MIC | 21 + 8.25 | 0.5 + 0.25 | 0.75 | partial synergy |
| 12 | 1/2MIC + 1/8MIC | 21 + 4.13 | 0.5 + 0.125 | 0.625 | partial synergy |
| 13 | 1/2MIC + 1/16MIC | 21 + 2.06 | 0.5 + 0.062 | 0.562 | partial synergy |
| 14 | 1/2MIC + 1/32MIC | 21 + 1.03 | 0.5 + 0.031 | 0.531 | partial synergy |
| 15 | 1/2MIC + 1/64MIC | 21 + 0.51 | 0.5 + 0.015 | 0.515 | partial synergy |
| 16 | 1/4MIC + MIC | 10.5 + 33 | 0.25 + 1 | 1.25 | additive |
| 17 | 1/4MIC + 1/2MIC | 10.5 + 16.5 | 0.25 + 0.5 | 0.75 | partial synergy |
| 18 | 1/4MIC + 1/4MIC | 10.5 + 8.25 | 0.25 + 0.25 | 0.5 | synergy |
| 19 | 1/4MIC + 1/8MIC | 10.5 + 4.13 | 0.25 + 0.125 | 0.375 | synergy |
| 20 | 1/4MIC + 1/16MIC | 10.5 + 2.06 | 0.25 + 0.062 | 0.312 | synergy |
| 21 | 1/4MIC + 1/32MIC | 10.5 + 1.03 | 0.25 + 0.031 | 0.281 | synergy |
| 22 | 1/8MIC + MIC | 5.25 + 33 | 0.125 + 1 | 1.125 | additive |
| 23 | 1/8MIC + 1/2MIC | 5.25 + 16.5 | 0.125 + 0.5 | 0.625 | partial synergy |
| 24 | 1/8MIC + 1/4MIC | 5.25 + 8.25 | 0.125 + 0.25 | 0.375 | synergy |
| 25 | 1/8MIC + 1/8MIC | 5.25 + 4.14 | 0.125 + 0.125 | 0.25 | synergy |
| 26 | 1/8MIC + 1/16MIC | 5.25 + 2.06 | 0.125 + 0.062 | 0.187 | synergy |
| 27 | 1/16MIC + MIC | 2.62 + 33 | 0.062 + 1 | 1.062 | additive |
| 28 | 1/16MIC + 1/2MIC | 2.62 + 16.5 | 0.062 + 0.5 | 0.562 | partial synergy |
| 29 | 1/16MIC + 1/4MIC | 2.62 + 8.25 | 0.062 + 0.25 | 0.312 | synergy |
| 30 | 1/32MIC + MIC | 1.31 + 33 | 0.031 + 1 | 1.031 | additive |
| 31 | 1/32MIC + 1/2MIC | 1.31 + 16.5 | 0.031 + 0.5 | 0.531 | partial synergy |
| 32 | 1/32MIC + 1/4MIC | 1.31 + 8.25 | 0.031 + 0.25 | 0.281 | synergy |
| 33 | 1/64MIC + MIC | 0.65 + 33 | 0.015 + 1 | 1.015 | additive |
| 34 | 1/64MIC + 1/2MIC | 0.65 + 16.5 | 0.015 + 0.5 | 0.515 | partial synergy |
| 35 | 1/64MIC + 1/4MIC | 0.65 + 8.25 | 0.015 + 0.25 | 0.265 | synergy |
| 36 | 1/128MIC + MIC | 0.22 + 33 | 0.007 + 1 | 1.007 | additive |
| 37 | 1/128MIC + 1/2MIC | 0.32 + 16.5 | 0.007 + 0.5 | 0.507 | partial synergy |
| 38 | 1/128MIC + 1/4MIC | 0.32 + 8.25 | 0.007 + 0.25 | 0.257 | synergy |
| Treatment | Number of Bacterial Isolates Biofilm Formation (%) | Degree (%) | |||
|---|---|---|---|---|---|
| Weak (%) | Moderate (%) | Strong (%) | |||
| Untreated | 0.0 µg/mL | 71 (93.36) | 23.93 | 60.54 | 15.48 |
| Z. officinale | 25 µg/mL | 40 (52.6) | 30.0 | 45.0 | 25.0 |
| 50 µg/mL | 5 (6.31) | 0.0 | 40.0 | 60.0 | |
| Gentamicin | 25 µg/mL | 43 (56.54) | 25.57 | 44.17 | 30.22 |
| 50 µg/mL | 2 (2.63) | 0.0 | 100 | 0.0 | |
| Treatment | Concentration (μg/mL) | Absorbance 560 nm | Percentage Inhibition |
|---|---|---|---|
| Control | 0.0 | 1.246 | 0.0 |
| Z. officinale | 4 | 0.625 | 49.83% |
| 8 | 0.536 | 56.68% | |
| 16 | 0.501 | 59.79% | |
| 32 | 0.480 | 61.47% | |
| Sodium diclofenac | 4 | 0.452 | 63.72% |
| 8 | 0.405 | 67.49% | |
| 16 | 0.384 | 69.18% | |
| 32 | 0.357 | 71.43% |
| Peak | Rotation Time | Contents% | Compound Name | Molecular Formula | Molecular Weight |
|---|---|---|---|---|---|
| 1 | 9.18 | 0.68 | Decanal | C10H20O | 156 |
| 2 | 16.85 | 0.98 | Dodecanamine, N, N-dimethyl- | C14H31N | 213 |
| 3 | 18.89 | 10.50 | Thymol | C10H14O | 150 |
| 4 | 20.55 | 3.26 | Phenol, 2-methyl-5-(1-methylethyl)- Carvacrol | C10H14O | 150 |
| 5 | 22.74 | 2.32 | Eugenol | C10H12O2 | 166 |
| 6 | 23.88 | 0.47 | Alpha-terpineol | C10H20O | 156 |
| 7 | 26.24 | 2.14 | Butanedioic acid, 2,3-bis(acetyloxy) | C8H14O8 | 182 |
| 8 | 27.39 | 0.76 | Benzenediamine, 2,5-dimethoxy-alpha | C12H17NO2 | 207 |
| 8 | 30.15 | 6.55 | Shogaol | C19H28O3 | 304 |
| 10 | 31.35 | 45.05 | Gingerol | C17H28O4 | 246 |
| 12 | 32.83 | 16.05 | Zingiberene | C15H27 | 207 |
| 13 | 34.72 | 3.44 | Beta-bisabolene | C15H22 | 200 |
| 14 | 36.15 | 2.26 | E-11-hexadecenoic acid, ethyl ester | C18H34O2 | 282 |
| 15 | 37.90 | 6.69 | Cyclohexane, 3-(1,5-dimethyl-4-hexenyl)- | C15H24 | 204 |
| 16 | 39.35 | 1.25 | Farnesyl acetone | C18H27O | 269 |
| 17 | 42.16 | 1.26 | Desoxo-9x-hydroxy-7-ketoingol 3,8,9,12-tetraacetate | C28H38O10 | 534 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elbestawy, M.K.M.; El-Sherbiny, G.M.; Moghannem, S.A.; Farghal, E.E. Antibacterial, Antibiofilm, and Anti-Inflammatory Activities of Ginger Extract against Helicobacter pylori. Microbiol. Res. 2023, 14, 1124-1138. https://doi.org/10.3390/microbiolres14030075
Elbestawy MKM, El-Sherbiny GM, Moghannem SA, Farghal EE. Antibacterial, Antibiofilm, and Anti-Inflammatory Activities of Ginger Extract against Helicobacter pylori. Microbiology Research. 2023; 14(3):1124-1138. https://doi.org/10.3390/microbiolres14030075
Chicago/Turabian StyleElbestawy, Mahmoud K. M., Gamal M. El-Sherbiny, Saad A. Moghannem, and Eman E. Farghal. 2023. "Antibacterial, Antibiofilm, and Anti-Inflammatory Activities of Ginger Extract against Helicobacter pylori" Microbiology Research 14, no. 3: 1124-1138. https://doi.org/10.3390/microbiolres14030075
APA StyleElbestawy, M. K. M., El-Sherbiny, G. M., Moghannem, S. A., & Farghal, E. E. (2023). Antibacterial, Antibiofilm, and Anti-Inflammatory Activities of Ginger Extract against Helicobacter pylori. Microbiology Research, 14(3), 1124-1138. https://doi.org/10.3390/microbiolres14030075