
The Spectrum of Fungal Colonization and Their Attributable Effects on Cystic Fibrosis Patients with Rare CFTR Genetic Mutations


 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population and Ethical Approvals
2.2. Data Source
2.3. Variables of Interest
2.4. Lung Function Data
2.5. Genetics and Diagnosis of Complications
2.6. Statistical Methods
3. Results
3.1. Demographic Data of Adult CF Patients in Qatar
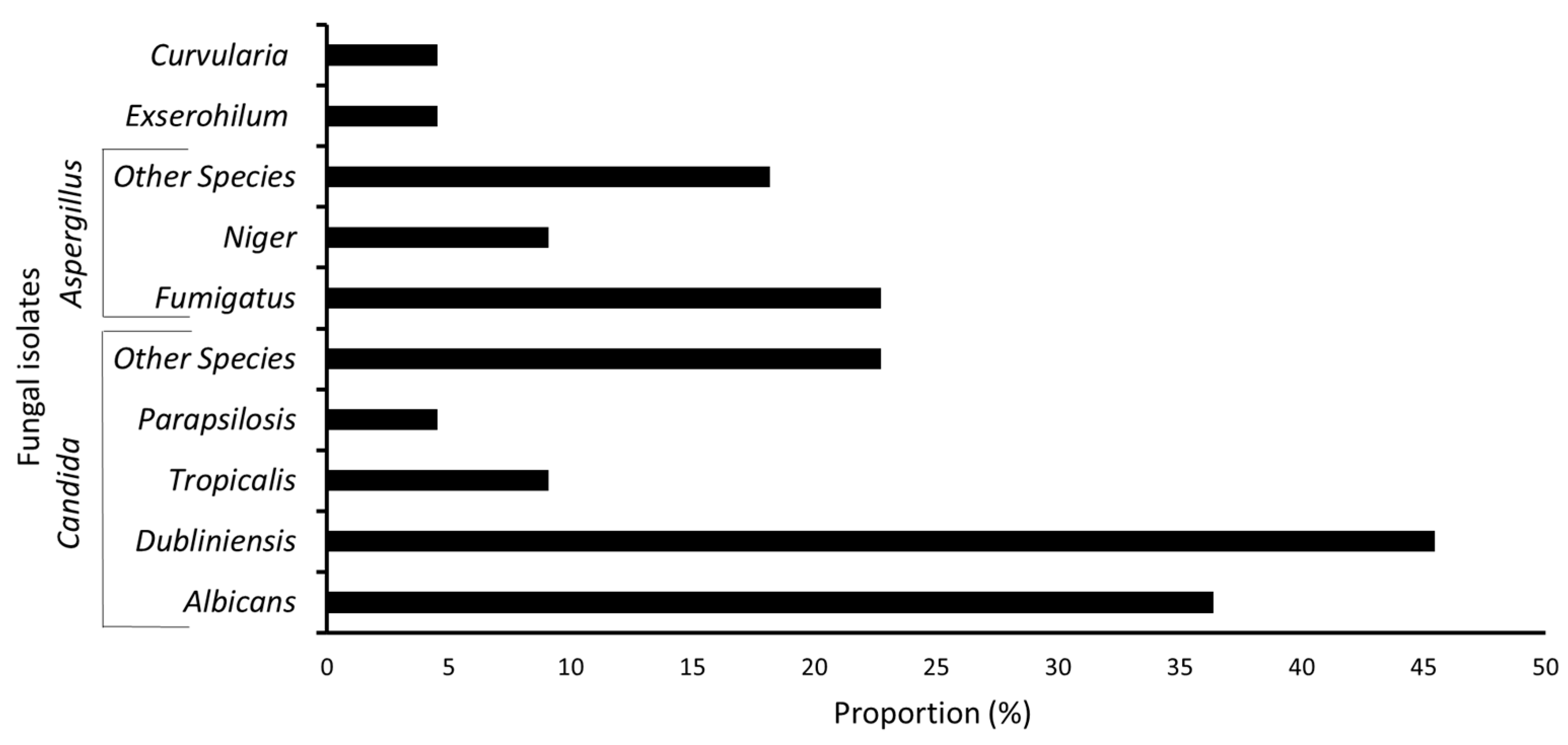
3.2. Fungal Colonization in CF Patients
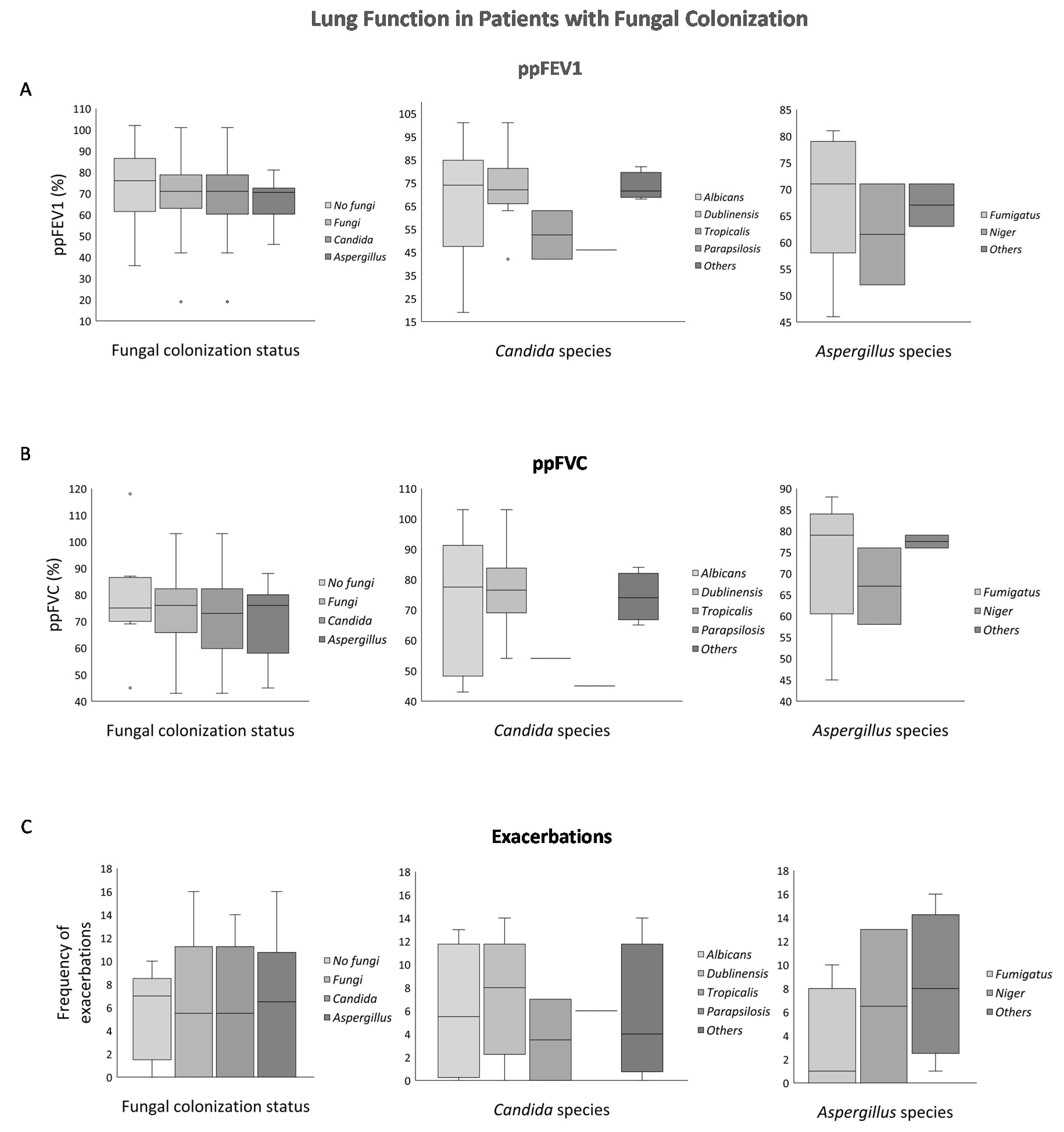
3.3. Lung Function in the Presence of Fungal Colonization
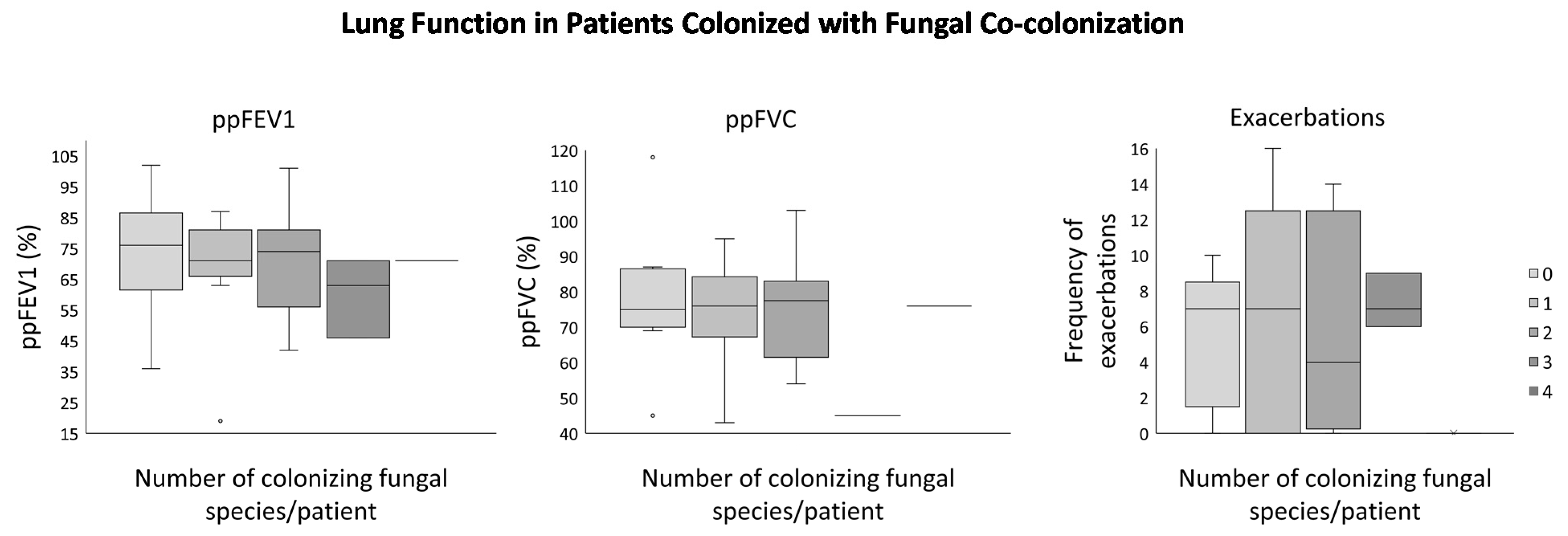
Lung Function in the Presence of Multiple Fungal Co-Colonization
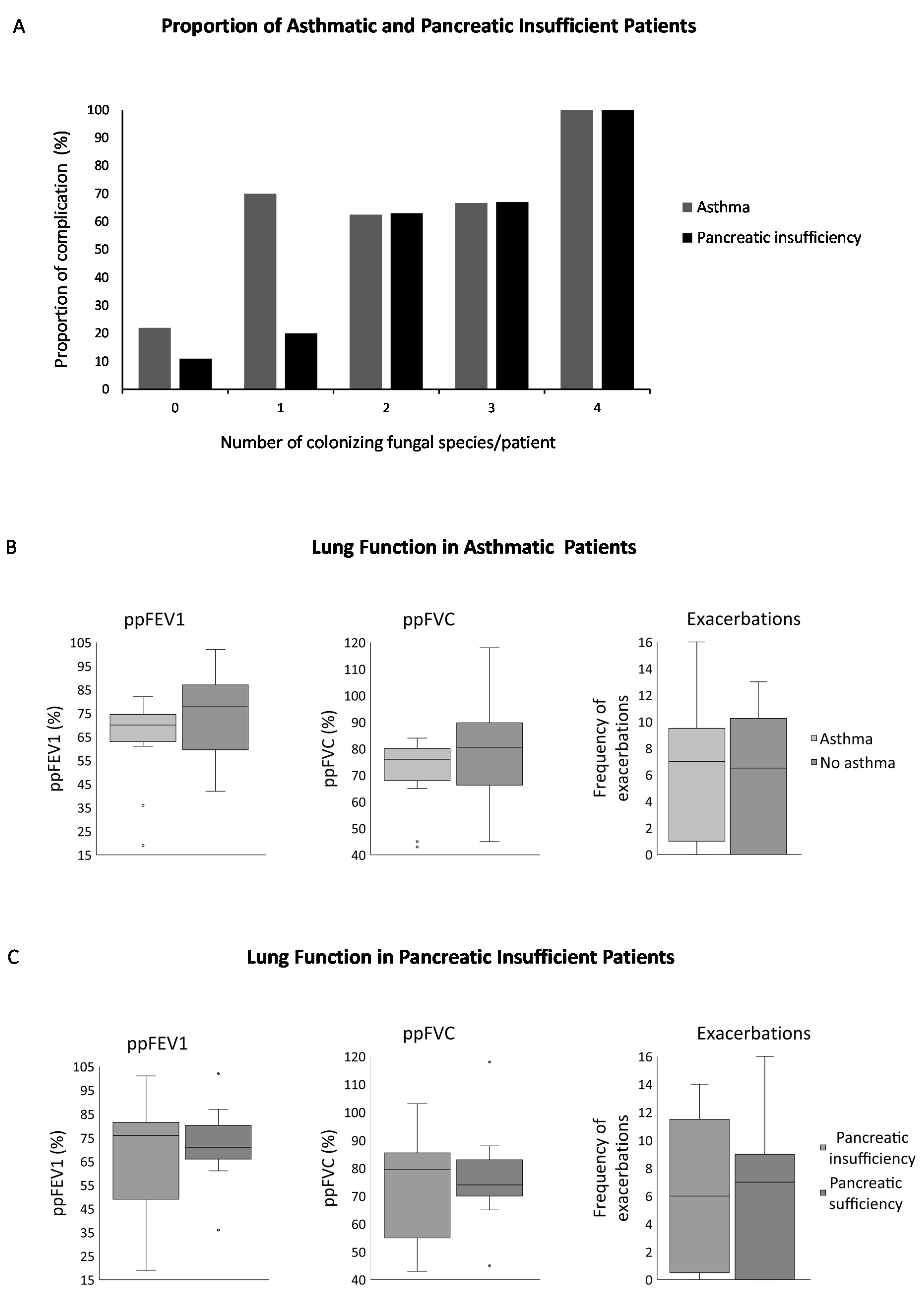
3.4. Asthma and Pancreatic Insufficiency in the Presence of Fungal Colonization
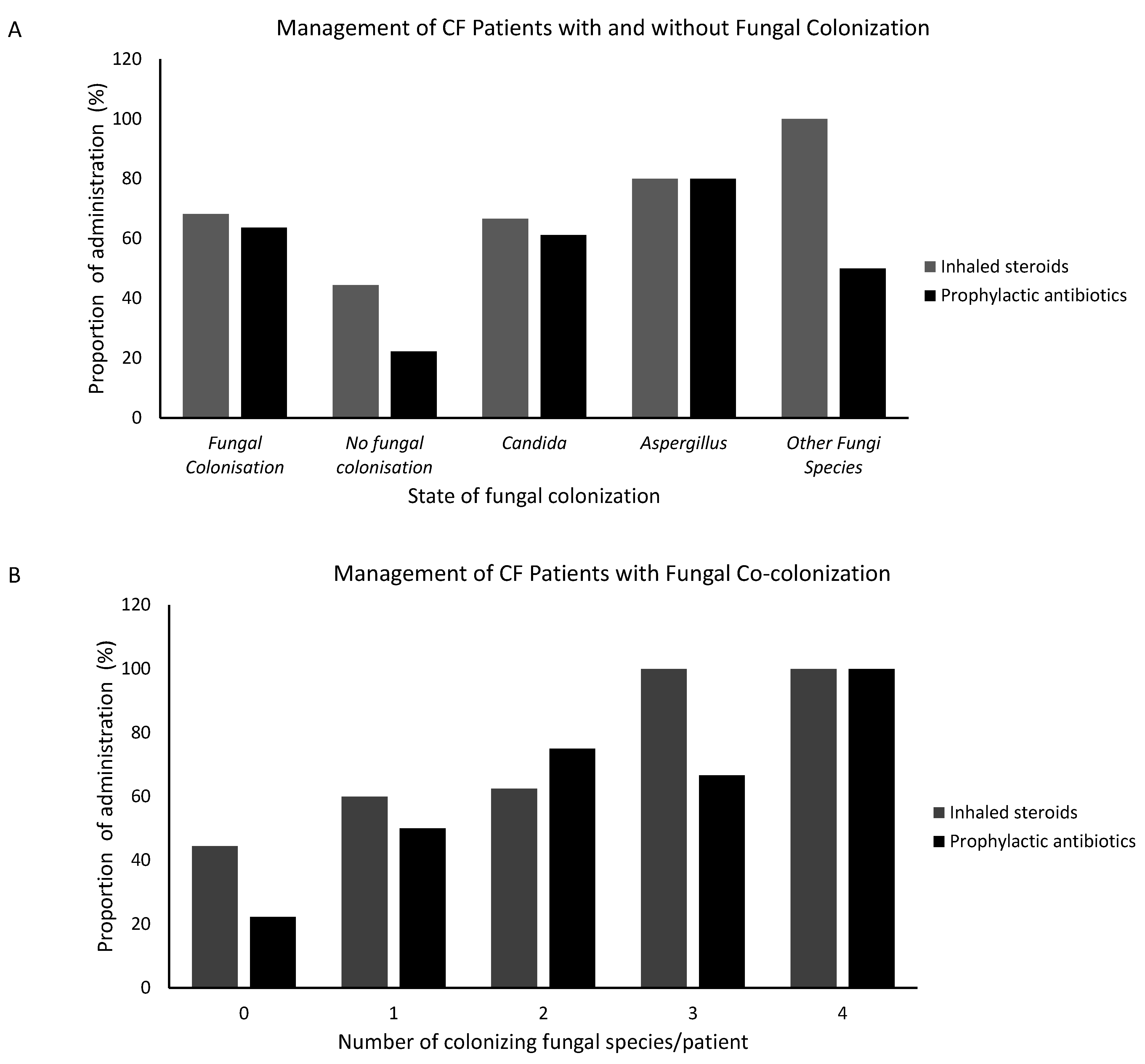
3.5. Prophylactic Antibiotics and Inhaled Steroids Management in Patients with or without Fungal Colonization
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Elborn, J.S. Cystic fibrosis. Lancet 2016, 388, 2519–2531. [Google Scholar] [CrossRef]
- WHO Human Genetics Programme. The Molecular Genetic Epidemiology of Cystic Fibrosis: Report of a Joint Meeting of WHO/IECFTN/ICF(M)A/ECFS, Genoa, Italy, 19 June 2002. World Health Organization. 2004. Available online: https://apps.who.int/iris/handle/10665/68702 (accessed on 12 July 2021).
- Wahab, A.A.; Al Thani, G.; Dawod, S.T.; Kambouris, M.; Al Hamed, M. Heterogeneity of the cystic fibrosis phenotype in a large kindred family in Qatar with cystic fibrosis mutation (I1234V). J. Trop. Pediatr. 2001, 47. [Google Scholar] [CrossRef]
- Hammoudeh, S.; Gadelhak, W.; Abdulwahab, A.; Al-Langawi, M.; Janahi, I.A. Approaching two decades of cystic fibrosis research in Qatar: A historical perspective and future directions. Multidiscip. Respir. Med. 2019, 14. [Google Scholar] [CrossRef]
- Hammoudeh, S.; Gadelhak, W.; AbdulWahab, A.; Al-Langawi, M.; Janahi, I.A. An Overview of the Homozygous Cystic Fibrosis Transmembrane Conductance Regulator Mutation c.3700 A>G (p.Ile1234Val) in Qatar. Curr. Genet. Med. Rep. 2019, 7. [Google Scholar] [CrossRef]
- Ehre, C.; Ridley, C.; Thornton, D.J. Cystic fibrosis: An inherited disease affecting mucin-producing organs. Int. J. Biochem. Cell Biol. 2014, 52, 136–145. [Google Scholar] [CrossRef]
- Lopes, S.P.; Ceri, H.; Azevedo, N.F.; Pereira, M.O. Antibiotic resistance of mixed biofilms in cystic fibrosis: Impact of emerging microorganisms on treatment of infection. Int. J. Antimicrob. Agents 2012, 40, 260–263. [Google Scholar] [CrossRef] [PubMed]
- Pihet, M.; Carrere, J.; Cimon, B.; Chabasse, D.; Delhaes, L.; Symoens, F.; Bouchara, J.P. Occurrence and relevance of filamentous fungi in respiratory secretions of patients with cystic fibrosis—A review. Sabouraudia 2009, 47, 387–397. [Google Scholar] [CrossRef]
- Barreiro, T.; Perillo, I. An Approach to Interpreting Spirometry. Am. Fam. Physician 2004, 69, 1107–1114. Available online: https://www.aafp.org/afp/2004/0301/p1107.html (accessed on 12 September 2020).
- Brandt, C.; Roehmel, J.; Rickerts, V.; Melichar, V.; Niemann, N.; Schwarz, C. Aspergillus bronchitis in patients with cystic fibrosis. Mycopathologia 2018, 183, 61–69. [Google Scholar] [CrossRef]
- Crapo, R.O.; Hankinson, J.L.; Irvin, C.; MacIntyre, N.R.; Voter, K.Z.; Wise, R.A.; Graham, B.; O’Donnell, C.; Paoletti, P.; Roca, J.; et al. Standardization of spirometry: 1994 update. Am. J. Respir. Crit. Care Med. 1995, 152, 1107–1136. [Google Scholar]
- Maria, I.; Jar, N. Cystic Fibrosis Pulmonary Exacerbation—Natural History, Causative Factors and Management. In Respiratory Disease and Infection—A New Insight. Available online: https://www.intechopen.com/books/respiratory-disease-and-infection-a-new-insight/cystic-fibrosis-pulmonary-exacerbation-natural-history-causative-factors-and-management (accessed on 12 July 2021).
- De Waele, J.J.; Vogelaers, D.; Blot, S.; Colardyn, F. Fungal Infections in Patients with Severe Acute Pancreatitis and the Use of Prophylactic Therapy. Clinical Infectious Diseases Virginia. Available online: https://pubmed.ncbi.nlm.nih.gov/12856213/ (accessed on 12 July 2021).
- Wahab, A.A.; Taj-Aldeen, S.J.; Kolecka, A.; ElGindi, M.; Finkel, J.S.; Boekhout, T. High prevalence of Candida dubliniensis in lower respiratory tract secretions from cystic fibrosis patients may be related to increased adherence properties. Int. J. Infect. Dis. 2014, 24. [Google Scholar] [CrossRef] [PubMed]
- Charlson, E.S.; Diamond, J.M.; Bittinger, K.; Fitzgerald, A.S.; Yadav, A.; Haas, A.R.; Bushman, F.D.; Collman, R.G. Lung-enriched organisms and aberrant bacterial and fungal respiratory microbiota after lung transplant. Am. J. Respir. Crit. Care Med. 2012, 186. [Google Scholar] [CrossRef]
- Bargon, J.; Dauletbaev, N.; Köhler, B.; Wolf, M.; Posselt, H.G.; Wagner, T.O.F. Prophylactic antibiotic therapy is associated with an increased prevalence of Aspergillus colonization in adult cystic fibrosis patients. Respir. Med. 1999, 93, 835–838. [Google Scholar] [CrossRef]
- Reece, E.; Segurado, R.; Jackson, A.; McClean, S.; Renwick, J.; Greally, P. Co-colonisation with Aspergillus fumigatus and Pseudomonas aeruginosa is associated with poorer health in cystic fibrosis patients: An Irish registry analysis. BMC Pulm. Med. 2017, 17, 70. [Google Scholar] [CrossRef] [PubMed]
- Leclair, L.W.; Hogan, D.A. Mixed bacterial-fungal infections in the CF respiratory tract. Med. Mycol. 2010, 48. [Google Scholar] [CrossRef]
- Hoerauf, A.; Hammer, S.; Müller-Myhsok, B.; Rupprecht, H. Intra-abdominal Candida infection during acute necrotizing pancreatitis has a high prevalence and is associated with increased mortality. Crit. Care Med. 1998, 26. [Google Scholar] [CrossRef] [PubMed]
- Boucher, B.A.; King, S.R.; Wandschneider, H.L.; Hickerson, W.L.; Hanes, S.D.; Herring, V.L.; Canada, T.W.; Hess, M.M. Fluconazole pharmacokinetics in burn patients. Antimicrob. Agents Chemother. 1998, 42. [Google Scholar] [CrossRef]
- Kochhar, R.; Ahammed, S.K.M.; Chakrabarti, A.; Ray, P.; Sinha, S.K.; Dutta, U.; Wig, J.D.; Singh, K. Prevalence and outcome of fungal infection in patients with severe acute pancreatitis. J. Gastroenterol. Hepatol. Aust. 2009, 24. [Google Scholar] [CrossRef]
- Huang, W.; de la Iglesia-García, D.; Baston-Rey, I.; Calviño-Suarez, C.; Lariño-Noia, J.; Iglesias-Garcia, J.; Shi, N.; Zhang, X.; Cai, W.; Deng, L.; et al. Exocrine Pancreatic Insufficiency Following Acute Pancreatitis: Systematic Review and Meta-Analysis. Dig. Dis. Sci. 2019, 64. [Google Scholar] [CrossRef] [PubMed]
- Gibson-Corley, K.N.; Meyerholz, D.K.; Engelhardt, J.F. Pancreatic pathophysiology in cystic fibrosis. J. Pathol. 2016, 238. [Google Scholar] [CrossRef]
- Olivier, A.K.; Yi, Y.; Sun, X.; Sui, H.; Liang, B.; Hu, S.; Xie, W.; Fisher, J.T.; Keiser, N.W.; Lei, D.; et al. Abnormal endocrine pancreas function at birth in cystic fibrosis ferrets. J. Clin. Investig. 2012, 122. [Google Scholar] [CrossRef]
- Navis, A.; Bagnat, M. Loss of cftr function leads to pancreatic destruction in larval zebrafish. Dev. Biol. 2015, 399. [Google Scholar] [CrossRef] [PubMed]
- Meyerholz, D.K.; Stoltz, D.A.; Pezzulo, A.A.; Welsh, M.J. Pathology of gastrointestinal organs in a porcine model of cystic fibrosis. Am. J. Pathol. 2010, 176. [Google Scholar] [CrossRef] [PubMed]
- Milla, C.E.; Warwick, W.J.; Moran, A. Trends in pulmonary function in patients with cystic fibrosis correlate with the degree of glucose intolerance at baseline. Am. J. Respir. Crit. Care Med. 2000, 162. [Google Scholar] [CrossRef] [PubMed]
- Arora, N.S.; Rochester, D.F. Respiratory muscle strength and maximal voluntary ventilation in undernourished patients. Am. Rev. Respir. Dis. 1982, 126. [Google Scholar] [CrossRef]
- Arora, N.S.; Rochester, D.F. Effect of body weight and muscularity on human diaphragm muscle mass, thickness, and area. J. Appl. Physiol. 1982, 52. [Google Scholar] [CrossRef]
- Alvarez, J.A.; Ziegler, T.R.; Millson, E.C.; Stecenko, A.A. Body composition and lung function in cystic fibrosis and their association with adiposity and normal-weight obesity. Nutrition 2016, 32, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Mancuso, P. Obesity and respiratory infections: Does excess adiposity weigh down host defense? Pulm. Pharmacol. Ther. 2013, 26. [Google Scholar] [CrossRef]
- Huttunen, R.; Karppelin, M.; Syrjänen, J. Obesity and nosocomial infections. J. Hosp. Infect. 2013, 85. [Google Scholar] [CrossRef]
- Falagas, M.E.; Kompoti, M. Obesity and infection. Lancet Infect. Dis. 2006, 6. [Google Scholar] [CrossRef]
- Hanna, R.M.; Weiner, D.J. Overweight and obesity in patients with cystic fibrosis: A center-based analysis. Pediatr. Pulmonol. 2015, 50. [Google Scholar] [CrossRef] [PubMed]
- Teichmann, J.; Riemann, J.F.; Lange, U. Prevalence of Exocrine Pancreatic Insufficiency in Women with Obesity Syndrome: Assessment by Pancreatic Fecal Elastase. ISRN Gastroenterol. 2011, 2011. [Google Scholar] [CrossRef] [PubMed]
- Dixon, A.E.; Holguin, F.; Sood, A.; Salome, C.M.; Pratley, R.E.; Beuther, D.A.; Celedón, J.C.; Shore, S.A.; Boulet, L.P.; O’Donnell, C.; et al. An Official American Thoracic Society Workshop Report: Obesity and Asthma. Proceedings of the American Thoracic Society New York, United States of America 7, No. 5. 2010, pp. 325–335. Available online: https://www.atsjournals.org/doi/10.1513/pats.200903-013ST (accessed on 8 April 2020).
- Farah, C.S.; Kermode, J.A.; Downie, S.R.; Brown, N.J.; Hardaker, K.M.; Berend, N.; King, G.G.; Salome, C.M. Obesity is a determinant of asthma control independent of inflammation and lung mechanics. Chest 2011, 140. [Google Scholar] [CrossRef]
- Mosen, D.M.; Schatz, M.; Magid, D.J.; Camargo, C.A. The relationship between obesity and asthma severity and control in adults. J. Allergy Clin. Immunol. 2008, 122. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Data | Patients Colonized with Fungi | Patients Not Colonized with Fungi | All CF Patients |
|---|---|---|---|
| Genetic mutation: n (%) | |||
| I1234V (c.3700A>G) | 18 (81.8) | 7 (77.8) | 25 (80.6) |
| Heterozygous R553X (c.1657C>T and c.1115A>T) | 3 (13.6) | 0 | 3 (9.7) |
| Homozygous (S307N(c.920G>A)) | 1 (4.5) | 2 (22.2) | 3 (9.7) |
| Nationality: n (%) | |||
| Qatari | 19 (86.4) | 9 (100.0) | 28 (90.3) |
| Non-Qatari | 3 (13.6) | 0 | 3 (9.7) |
| Age: median | 24.5 | 24 | 25.5 |
| Age group: n (%) | |||
| ≤20 | 3 (13.6) | 2 (22.3) | 5 (16.2) |
| >20–25 | 9 (40.9) | 3 (33.3) | 12 (38.7) |
| >25–30 | 5 (22.7) | 4 (44.4) | 9 (29.0) |
| >30–35 | 2 (9.1) | 0 | 2 (6.5) |
| >35–40 | 2 (9.1) | 0 | 2 (6.5) |
| >40–45 | 1 (4.5) | 0 | 1 (3.2) |
| BMI: median | 26.6 | 29.8 | 26.6 |
| BMI classes: n (%) | |||
| Underweight | 2 (9.1) | 0 | 2 (6.5) |
| Normal | 7 (31.8) | 4 (44.4) | 11 (35.5) |
| Overweight | 11 (50.0) | 1 (11.1) | 12 (38.7) |
| Obese (class I) | 2 (9.1) | 2 (22.2) | 4 (12.9) |
| Obese (class II) | 0 | 2 (22.2) | 2 (6.5) |
| Total | 22 | 9 | 31 (100) |
| Complications n (%) | ||||
|---|---|---|---|---|
| Microbial Colonization (n) | Asthma (n = 17) | p-Value | Pancreatic Insufficient (n = 13) | p-Value |
| Fungi colonization (n = 22) | 15 (88.0) | 0.044 | 12 (54.5) | 0.045 |
| Candida species (n = 18) | 12 (66.7) | 0.157 | 12 (66.7) | 0.002 |
| Aspergillus species (n = 10) | 7 (70.0) | 0.280 | 5 (50.0) | 0.701 |
| Other species (n = 2) | 2 (100.0) | 0.488 | 1 (50.0) | 1.000 |
| Complication and Number of Colonizing Fungal Species/Number of Patients (n) | ppFEV1 (%) | ppFVC (%) | Frequency of Exacerbations |
|---|---|---|---|
| Asthma (17) | 70 | 76 | 7 |
| 0 (2) | 48.5 | 58 | 8 |
| 1 (7) | 68 | 73 | 9 |
| 2 (5) | 77 | 79 | 3 |
| 3 (2) | 67 | N/A * | 8 |
| 4 (1) | 71 | 76 | 0 |
| No asthma (14) | 78 | 80.5 | 6.5 |
| 0 (7) | 80 | 86 | 7 |
| 1 (3) | 81 | 88 | 0 |
| 2 (3) | 52 | 58 | 11 |
| 3 (1) | 46 | 45 | 6 |
| 4 (0) | |||
| Pancreatic insufficiency (13) | 76 | 79.5 | 6 |
| 0 (1) | 76 | 86 | 10 |
| 1 (3) | 81 | 83 | 12 |
| 2 (6) | 77.5 | 79.5 | 4 |
| 3 (2) | 54.5 | 45 | 6.5 |
| 4 (1) | 71 | 76 | 0 |
| Pancreatic sufficiency (18) | 71 | 74 | 7 |
| 0 (8) | 75.5 | 74.5 | 7 |
| 1 (7) | 70 | 73 | 5 |
| 2 (2) | 69.5 | 74 | 7.5 |
| 3 (1) | 71 | ND | 9 |
| 4 (0) |
| Treatment-n(%) | |||||
|---|---|---|---|---|---|
| Microbial Colonization | Culture (n) | Prophylactic Antibiotics | p-Value | Inhaled Steroid | p-Value |
| Fungal species | P (22) | 14 | 0.054 | 15 | 0.253 |
| (63.6) | (68.2) | ||||
| A (9) | 2 | 4 | |||
| (22.2) | (44.4) | ||||
| Candida species | P (18) | 11 | 0.285 | 12 | 0.710 |
| (61.1) | (66.7) | ||||
| A (13) | 5 | 7 | |||
| (38.5) | (53.8) | ||||
| Aspergillus species | P (10) | 8 | 0.054 | 8 | 0.240 |
| (80.0) | (80.0) | ||||
| A (21) | 8 | 11 | |||
| (38.1) | (52.3) | ||||
| Other species | P (2) | 1 | 1.000 | 2 | 0.510 |
| (50.0) | (100) | ||||
| A (29) | 15 | 17 | |||
| (51.7) | (58.6) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thomas, M.; Aboukhalaf, S.; Darwish, T.; Ali, M.; Elsaied, O.; Al Bakri, M.; Najim, M.; Emara, M.M.; Al Langawi, M. The Spectrum of Fungal Colonization and Their Attributable Effects on Cystic Fibrosis Patients with Rare CFTR Genetic Mutations. Microbiol. Res. 2021, 12, 591-605. https://doi.org/10.3390/microbiolres12030042
Thomas M, Aboukhalaf S, Darwish T, Ali M, Elsaied O, Al Bakri M, Najim M, Emara MM, Al Langawi M. The Spectrum of Fungal Colonization and Their Attributable Effects on Cystic Fibrosis Patients with Rare CFTR Genetic Mutations. Microbiology Research. 2021; 12(3):591-605. https://doi.org/10.3390/microbiolres12030042
Chicago/Turabian StyleThomas, Merlin, Soha Aboukhalaf, Toqa Darwish, Menatalla Ali, Omar Elsaied, Mutaz Al Bakri, Mostafa Najim, Mohamed M. Emara, and Mona Al Langawi. 2021. "The Spectrum of Fungal Colonization and Their Attributable Effects on Cystic Fibrosis Patients with Rare CFTR Genetic Mutations" Microbiology Research 12, no. 3: 591-605. https://doi.org/10.3390/microbiolres12030042
APA StyleThomas, M., Aboukhalaf, S., Darwish, T., Ali, M., Elsaied, O., Al Bakri, M., Najim, M., Emara, M. M., & Al Langawi, M. (2021). The Spectrum of Fungal Colonization and Their Attributable Effects on Cystic Fibrosis Patients with Rare CFTR Genetic Mutations. Microbiology Research, 12(3), 591-605. https://doi.org/10.3390/microbiolres12030042