The Role of Centralized Sexual Assault Care Centers in HIV Post-Exposure Prophylaxis Treatment Adherence: A Retrospective Single Center Analysis

 , ,
, ,
Abstract
1. Introduction
2. Methods
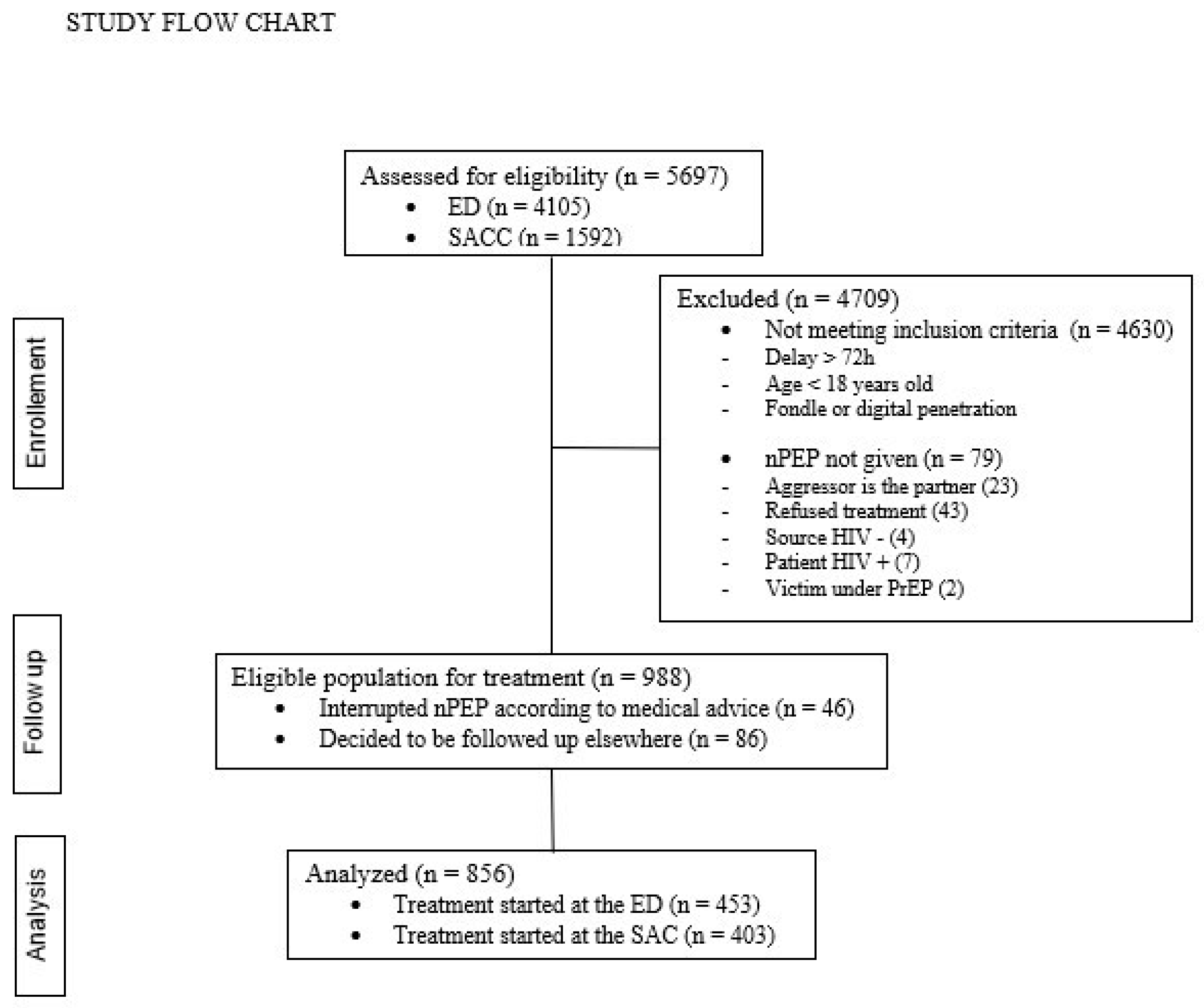
2.1. Study Design and Participants
2.2. Care Pathways
2.3. Data Collection
2.4. Laboratory Procedures
2.5. Outcome Measures
2.6. Statistical Analysis
3. Results
3.1. Multivariable Regression
3.2. Secondary Outcome
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Miele, C.; Maquigneau, A.; Joyal, C.C.; Bertsch, I.; Gangi, O.; Gonthier, H.; Rawlinson, C.; Vigourt-Oudart, S.; Symphorien, E.; Heasman, A.; et al. International guidelines for the prevention of sexual violence: A systematic review and perspective of WHO, UN Women, UNESCO, and UNICEF’s publications. Child Abus. Negl. 2023, 146, 106497. [Google Scholar] [CrossRef]
- Keygnaert, I.; De Schrijver, L.; Cismaru Inescu, A.; Schapansky, E.; Nobels, A.; Hahaut, B.; Stappers, C.; Debauw, Z.; Lemonne, A.; Renard, B.; et al. Understanding the Mechanism, Nature, Magnitude and Impact of Sexual Violence in Belgium; Final Report; Belgian Science Policy: Brussels, Belgium, 2021; 117p.
- Silverman, J.G.; Decker, M.R.; Saggurti, N.; Balaiah, D.; Raj, A. Intimate Partner Violence and HIV Infection Among Married Indian Women. JAMA 2008, 300, 703–710. [Google Scholar] [CrossRef]
- Seña, A.C.; Hsu, K.K.; Kellogg, N.; Girardet, R.; Christian, C.W.; Linden, J.; Griffith, W.; Marchant, A.; Jenny, C.; Hammerschlag, M.R. Sexual Assault and Sexually Transmitted Infections in Adults, Adolescents, and Children. Clin. Infect. Dis. 2015, 61, S856–S864. [Google Scholar] [CrossRef]
- Miller, C.J.; Li, Q.; Abel, K.; Kim, E.-Y.; Ma, Z.-M.; Wietgrefe, S.; La Franco-Scheuch, L.; Compton, L.; Duan, L.; Shore, M.D.; et al. Propagation and Dissemination of Infection after Vaginal Transmission of Simian Immunodeficiency Virus. J. Virol. 2005, 79, 9217–9227. [Google Scholar] [CrossRef]
- Ford, N.; Irvine, C.; Shubber, Z.; Baggaley, R.; Beanland, R.; Vitoria, M.; Doherty, M.; Mills, E.J.; Calmy, A. Adherence to HIV postexposure prophylaxis: A systematic review and meta-analysis. AIDS 2014, 28, 2721–2727. [Google Scholar] [CrossRef]
- Chacko, L.; Ford, N.; Sbaiti, M.; Siddiqui, R. Adherence to HIV post-exposure prophylaxis in victims of sexual assault: A systematic review and meta-analysis. Sex. Transm. Infect. 2012, 88, 335–341. [Google Scholar] [CrossRef]
- Tsai, C.-C.; Emau, P.; Follis, K.E.; Beck, T.W.; Benveniste, R.E.; Bischofberger, N.; Lifson, J.D.; Morton, W.R. Effectiveness of Postinoculation (R)-9-(2-Phosphonylmethoxypropyl)Adenine Treatment for Prevention of Persistent Simian Immunodeficiency Virus SIVmne Infection Depends Critically on Timing of Initiation and Duration of Treatment. J. Virol. 1998, 72, 4265–4273. [Google Scholar] [CrossRef]
- McAllister, J.; Beardsworth, G.; Lavie, E.; MacRae, K.; Carr, A. Financial stress is associated with reduced treatment adherence in HIV-infected adults in a resource-rich setting. HIV Med. 2012, 14, 120–124. [Google Scholar] [CrossRef]
- Shubber, Z.; Mills, E.J.; Nachega, J.B.; Vreeman, R.; Freitas, M.; Bock, P.; Nsanzimana, S.; Penazzato, M.; Appolo, T.; Doherty, M.; et al. Patient-Reported Barriers to Adherence to Antiretroviral Therapy: A Systematic Review and Meta-Analysis. PLoS Med. 2016, 13, e1002183. [Google Scholar] [CrossRef]
- Libois, A.; Florence, E.; Derdelinckx, I.; Yombi, J.C.; Henrard, S.; Uurlings, F.; Vandecasteele, S.; Allard, S.D.; Demeester, R.; Van Wanzeele, F.; et al. Belgian guidelines for non-occupational HIV post-exposure prophylaxis 2017. Acta Clin. Belg. 2018, 73, 275–280. [Google Scholar] [CrossRef]
- Campbell, R.; Patterson, D.; Lichty, L.F. The Effectiveness of Sexual Assault Nurse Examiner (SANE) Programs: A Review of Psychological, Medical, Legal, and Community Outcomes. Trauma Violence Abus. 2005, 6, 313–329. [Google Scholar] [CrossRef]
- Kim, J.C.; Askew, I.; Muvhango, L.; Dwane, N.; Abramsky, T.; Jan, S.; Ntlemo, E.; Chege, J.; Watts, C. Comprehensive care and HIV prophylaxis after sexual assault in rural South Africa: The Refentse intervention study. BMJ 2009, 338, 1559. [Google Scholar] [CrossRef]
- Greeson, M.R.; Campbell, R. Sexual Assault Response Teams (SARTs): An Empirical Review of Their Effectiveness and Challenges to Successful Implementation. Trauma Violence Abus. 2012, 14, 83–95. [Google Scholar] [CrossRef]
- Baert, S.; Gilles, C.; Van Belle, S.; Bicanic, I.; Roelens, K.; Keygnaert, I. Piloting sexual assault care centres in Belgium: Who do they reach and what care is offered? Eur. J. Psychotraumatol. 2021, 12, 1935592. [Google Scholar] [CrossRef] [PubMed]
- Malinverni, S.; Bédoret, F.; Bartiaux, M.; Gilles, C.; De Wit, S.; Libois, A. Single-tablet regimen of emtricitabine/tenofovir disoproxil fumarate plus cobicistat-boosted elvitegravir increase adherence for HIV postexposure prophylaxis in sexual assault victims. Sex. Transm. Infect. 2020, 97, 329–333. [Google Scholar] [CrossRef] [PubMed]
- Malinverni, S.; Gennotte, A.-F.; Schuster, M.; De Wit, S.; Mols, P.; Libois, A. Adherence to HIV post-exposure prophylaxis: A multivariate regression analysis of a 5 years prospective cohort. J. Infect. 2018, 76, 78–85. [Google Scholar] [CrossRef]
- Lederer, D.J.; Bell, S.C.; Branson, R.; Chalmers, J.D.; Marshall, R.; Maslove, D.M.; Ost, D.E.; Punjabi, N.M.; Schatz, M.; Smyth, A.R.; et al. Control of confounding and reporting of results in causal inference studies. Ann. Am. Thorac. Soc. 2019, 16, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Nisida, I.V.V.; Boulos, M.-I.C.; da Silva, L.M.B.; Mayaud, P.; Avelino-Silva, V.I.; Segurado, A.C. Predictors of Adherence to HIV Post-Exposure Prophylaxis and Retention in Care After an Episode of Sexual Violence in Brazil. AIDS Patient Care STDs 2019, 33, 399–405. [Google Scholar] [CrossRef]
- Martin, S.L.; Young, S.K.; Billings, D.L.; Bross, C.C. Health Care-Based Interventions for Women Who Have Experienced Sexual Violence: A Review of the Literature. Trauma Violence Abus. 2007, 8, 3–18. [Google Scholar] [CrossRef]
- Roland, M.E.; Myer, L.; Martin, L.J.; Maw, A.; Batra, P.; Arend, E.; Coates, T.J.; Denny, L.A. Preventing Human Immunodeficiency Virus Infection Among Sexual Assault Survivors in Cape Town, South Africa: An Observational Study. AIDS Behav. 2012, 16, 990–998. [Google Scholar] [CrossRef]
- Vandenberghe, A.; Hendriks, B.; Peeters, L.; Roelens, K.; Keygnaert, I. Establishing Sexual Assault Care Centres in Belgium: Health professionals’ role in the patient-centred care for victims of sexual violence. BMC Health Serv. Res. 2018, 18, 807. [Google Scholar] [CrossRef]
- Stokbæk, S.; Kristensen, C.L.; Astrup, B.S. Police reporting in cases of sexual assault—A 10-year study of reported cases, unreported cases, and cases with delayed reporting. Forensic Sci. Med. Pathol. 2021, 17, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Inciarte, A.; Leal, L.; Masfarre, L.; Gonzalez, E.; Diaz-Brito, V.; Lucero, C.; Garcia-Pindado, J.; León, A.; García, F.; the Sexual Assault Victims Study Group. Post-exposure prophylaxis for HIV infection in sexual assault victims. HIV Med. 2020, 21, 43–52. [Google Scholar] [CrossRef]
- Bentz, L.; Enel, P.; Dunais, B.; Durant, J.; Poizot-Martin, I.; Tourette-Turgis, C.; Rébillon, M.; Le Duff, F.; Dellamonica, P.; Pradier, C. Evaluating counseling outcome on adherence to prophylaxis and follow-up after sexual HIV-risk exposure: A randomized controlled trial. AIDS Care Psychol. Socio-Med. Asp. AIDS/HIV 2010, 22, 1509–1516. [Google Scholar] [CrossRef]
- Rothbaum, B.O.; Foa, E.B.; Riggs, D.S.; Murdock, T.; Walsh, W. A prospective examination of post-traumatic stress disorder in rape victims. J. Trauma. Stress 1992, 5, 455–475. [Google Scholar] [CrossRef]
- Jordan, C.E.; Campbell, R.; Follingstad, D. Violence and Women’s Mental Health: The Impact of Physical, Sexual, and Psychological Aggression. Annu. Rev. Clin. Psychol. 2010, 6, 607–628. [Google Scholar] [CrossRef] [PubMed]
- Olmastroni, E.; Galimberti, F.; Tragni, E.; Catapano, A.L.; Casula, M. Impact of COVID-19 Pandemic on Adherence to Chronic Therapies: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 3825. [Google Scholar] [CrossRef]
- Katz, I.T.; E Ryu, A.; Onuegbu, A.G.; Psaros, C.; Weiser, S.D.; Bangsberg, D.R.; Tsai, A.C. Impact of HIV-related stigma on treatment adherence: Systematic review and meta-synthesis. J. Int. AIDS Soc. 2013, 16, 18640. [Google Scholar] [CrossRef]
- Peeters, L.; Vandenberghe, A.; Hendriks, B.; Gilles, C.; Roelens, K.; Keygnaert, I. Current care for victims of sexual violence and future sexual assault care centres in Belgium: The perspective of victims. BMC Int. Health Hum. Rights 2019, 19, 21. [Google Scholar] [CrossRef]
- Hughes, E.; Domoney, J.; Knights, N.; Price, H.; Rutsito, S.; Stefanidou, T.; Majeed-Ariss, R.; Papamichail, A.; Ariss, S.; Gilchrist, G.; et al. The effectiveness of sexual assault referral centres with regard to mental health and substance use: A national mixed-methods study—The MiMoS Study. Health Soc. Care Deliv. Res. 2023, 11, 1–117. [Google Scholar] [CrossRef]

{kind=link}
| Total Study Population | ED | SAC | p Value | |
|---|---|---|---|---|
| (No. = 856) | (No. = 403) | (No. = 453) | ||
| Median age, years (IQR) | 25.5 (21–33) | 24 (20–32) | 26 (21–34) | 0.000 |
| Female, No. (%) | 769 (89.8) | 370 (91.8) | 399 (88.1) | 0.071 |
| Sexual orientation, No. (%) | 0.369 | |||
| Homosexual | 61 (7.2) | 24 (6.0) | 37 (8.4) | |
| Heterosexual | 745 (88.6) | 362 (90.0) | 383 (87.2) | |
| Bisexual | 35 (4.2) | 16 (4.0) | 19 (4.3) | |
| Migrant, No. (%) | 418 (48.9) | 214 (53.1) | 204 (45.2) | 0.022 |
| Health insurance, No. (%) | 731 (90.0) | 324 (80.4) | 407 (98.5) | 0.000 |
| Time to presentation, hours (IQR) | 16 (7–34) | 15 (7–29) | 17 (7–36) | 0.000 |
| Office hours, No. (%) | 267 (31.2) | 104 (25.9) | 163 (36.0) | 0.428 |
| Treatment, No. (%) | 0.000 | |||
| STT (EVG/COBI/FTC/TDF) | 546 (63.8) | 187 (46.4) | 359 (79.2) | |
| LPV/d4T/3TC | 216 (25.2) | 216 (53.6) | 0 (0) | |
| TDF/FTC/RAL | 94 (11) | 0 (0) | 94 (20.8) | |
| Total Study Population | ED | SAC | p Value | |
|---|---|---|---|---|
| Receptive anal, No. (%) | 240 (27.9%) | 115 (28.5%) | 125 (27.6%) | 0.759 |
| Receptive vaginal, No. (%) | 643 (75.1%) | 341 (84.6%) | 302 (66.7%) | 0.000 |
| Receptive oral, No. (%) | 229 (26.8%) | 106 (26.3%) | 123 (27.2%) | 0.769 |
| Multiple aggressors, No. (%) | 137 (16%) | 81 (20.1%) | 56 (12.4%) | 0.002 |
| Knowing the aggressor, No. (%) | 312 (36.4) | 101 (25.1) | 211 (46.6) | 0.000 |
| Adherence | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| Yes (No. = 440) | No (No. = 416) | OR (95% CI) | p Value | OR (95% CI) | p Value | |
| Median age, age (IQR) | 25 (21–32) | 26 (21–34) | 0.99 (0.98–1.00) | 0.110 | 0.99 (0.97–1.00) | 0.067 |
| Male, No. (%) | 43 (9.95) | 18 (4.40) | 1.46 (0.93–2.29) | 0.099 | ||
| Homosexual, No. (%) | 62 (14.35) | 34 (8.31) | 2.42 (1.37–4.28) | 0.002 | 2.74 (1.49–5.05) | 0.001 |
| Bisexual, No. (%) | 19 (4.40) | 16 (3.91) | 1.20 (0.61–2.38) | 0.594 | 1.11 (0.54–2.27) | 0.783 |
| SAC, No. (%) | 236 (53.64) | 217 (52.16) | 1.06 (0.81–1.39) | 0.666 | 0.81 (0.58–1.11) | 0.193 |
| Health insurance, No. (%) | 395 (92.94) | 336 (85.93) | 2.16 (1.35–3.44) | 0.001 | 2.05 (1.22–3.45) | 0.007 |
| Migrant, No. (%) | 200 (45.66) | 218 (52.40) | 0.76 (0.58–1.00) | 0.049 | 0.80 (0.59–1.08) | 0.140 |
| Multiple aggressors, No. (%) | 57 (12.95) | 80 (19.23) | 0.63 (0.43–0.90) | 0.012 | 0.66 (0.44–0.98) | 0.040 |
| Amnesia, No. (%) | 198 (45.41) | 161 (39.17) | 1.29 (0.98–1.70) | 0.066 | 1.28 (0.95–1.73) | 0.111 |
| Knowing the aggressor, No (%) | 159 (36.14) | 153 (36.78) | 0.97 (0.74–1.28) | 0.845 | 1.06 (0.90–1.26) | 0.469 |
| Office hours, No. (%) | 147 (33.49) | 120 (28.85) | 1.24 (0.93–1.66) | 0.144 | 1.22 (0.89–1.67) | 0.224 |
| Psychological support within 5 days, No. (%) | 171 (39.13) | 107 (26.03) | 1.83 (1.36–2.45) | 0.000 | 2.02 (1.45–2.79) | 0.000 |
| Psychological support within 28 days, No. (%) | 278 (64.20) | 158 (37.98) | 2.93 (2.22–3.87) | 0.000 | ||
| STT, No. (%) | 303 (68. 86) | 243 (58.41) | 1.57 (1.19–2.08) | 0.002 | 1.57 (1.14–2.17) | 0.006 |
| Total Study Population | ED | SAC | p Value | |
|---|---|---|---|---|
| (No. = 856) | (No. = 403) | (No. = 453) | ||
| Within 5 days, No. (%) | 278 (32.8) | 85 (21.5) | 193 (42.7) | 0.000 |
| Within 28 days, No. (%) | 436 (51.4) | 136 (33.7) | 300 (67.3) | 0.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malinverni, S.; Kargar Samani, S.; Gilles, C.; Libois, A.; Bédoret, F. The Role of Centralized Sexual Assault Care Centers in HIV Post-Exposure Prophylaxis Treatment Adherence: A Retrospective Single Center Analysis. Infect. Dis. Rep. 2025, 17, 77. https://doi.org/10.3390/idr17040077
Malinverni S, Kargar Samani S, Gilles C, Libois A, Bédoret F. The Role of Centralized Sexual Assault Care Centers in HIV Post-Exposure Prophylaxis Treatment Adherence: A Retrospective Single Center Analysis. Infectious Disease Reports. 2025; 17(4):77. https://doi.org/10.3390/idr17040077
Chicago/Turabian StyleMalinverni, Stefano, Shirine Kargar Samani, Christine Gilles, Agnès Libois, and Floriane Bédoret. 2025. "The Role of Centralized Sexual Assault Care Centers in HIV Post-Exposure Prophylaxis Treatment Adherence: A Retrospective Single Center Analysis" Infectious Disease Reports 17, no. 4: 77. https://doi.org/10.3390/idr17040077
APA StyleMalinverni, S., Kargar Samani, S., Gilles, C., Libois, A., & Bédoret, F. (2025). The Role of Centralized Sexual Assault Care Centers in HIV Post-Exposure Prophylaxis Treatment Adherence: A Retrospective Single Center Analysis. Infectious Disease Reports, 17(4), 77. https://doi.org/10.3390/idr17040077