
A SWOT Analysis of the Guidelines on Prevention of HIV/AIDS in Japan in the Context of COVID-19


{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
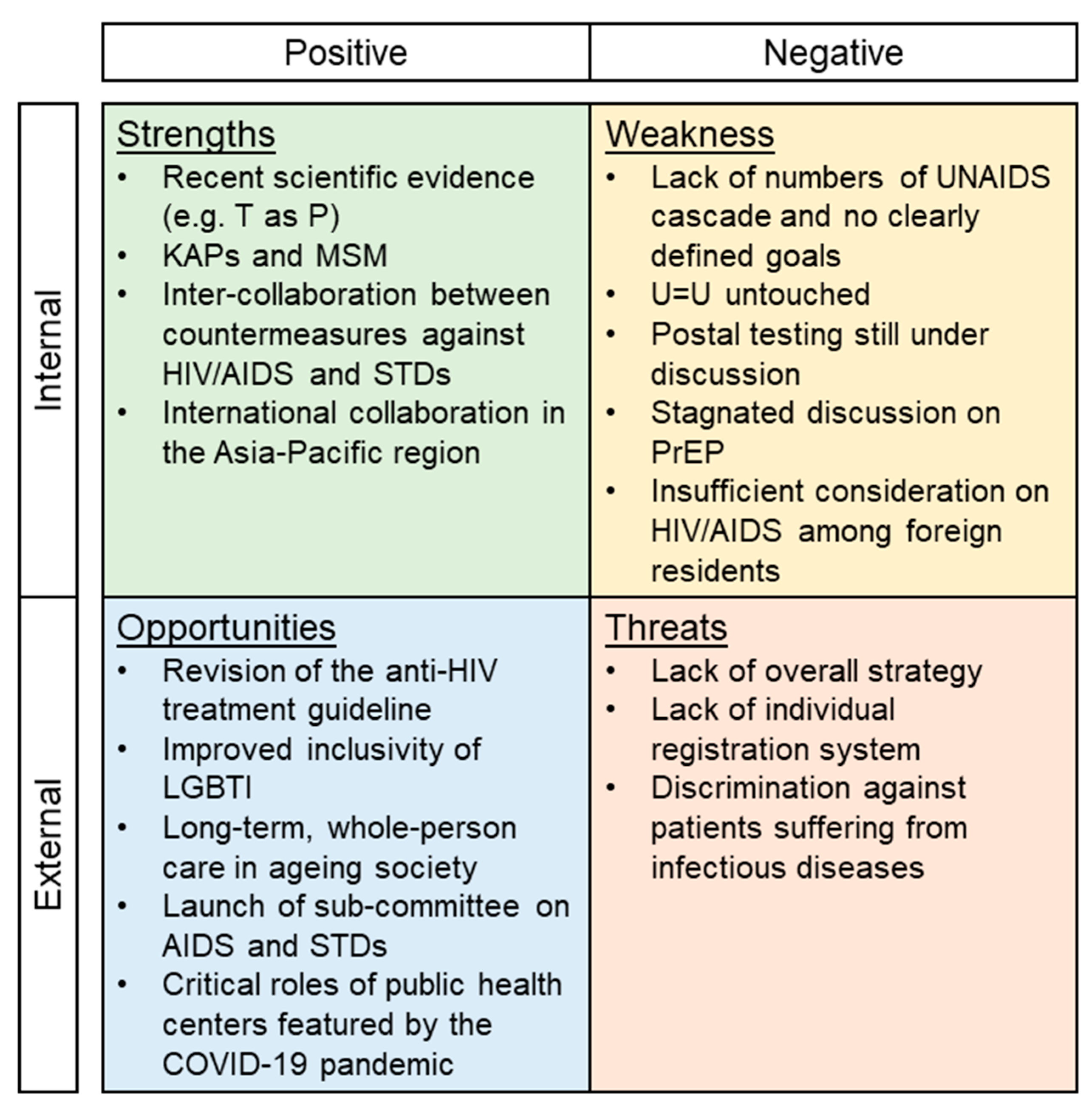
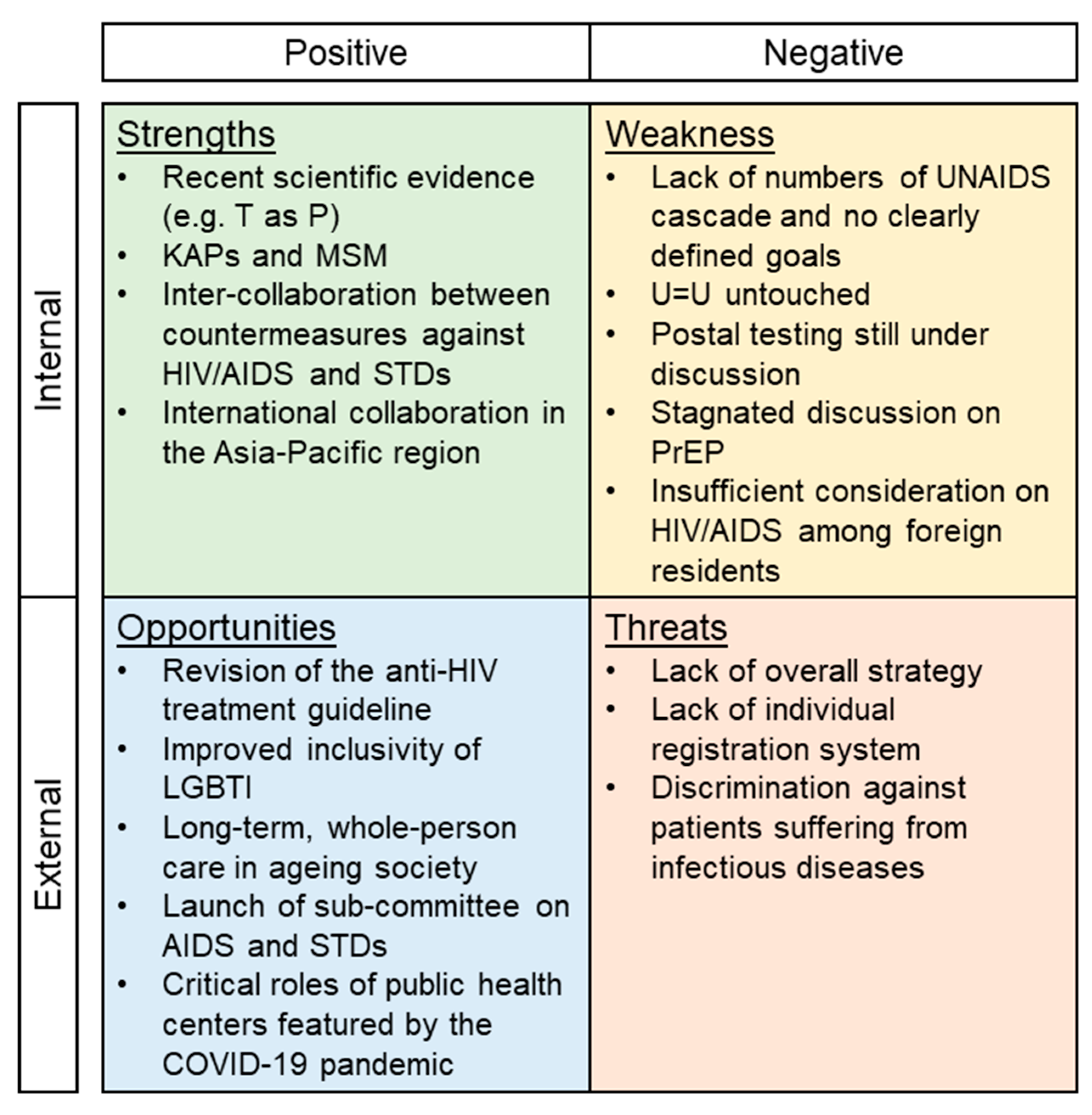
3. Results
3.1. Strengths
3.2. Weaknesses
3.3. Opportunities (External to the Guidelines)
3.4. Threats
4. Discussion
4.1. Prevention
4.2. Expanded Testing Opportunities and Antiretroviral Therapy
4.3. Leadership, Governance, and Funding
4.4. Limitations of This Study
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- The Tuberculosis and Infectious Diseases Control Division, Ministry of Health, Labour and Welfare, Japan. Annual Report of the National AIDS Surveillance Committee in 2020. Available online: https://api-net.jfap.or.jp/status/japan/data/2020/nenpo/2020nenpo.xlsx (accessed on 1 August 2021). (In Japanese).
- The Ministry of Health, Labour and Welfare, Japan. Prevention Measures for HIV/AIDS. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/kenkou_iryou/kenkou/kekkaku-kansenshou/aids/index.html (accessed on 1 August 2021). (In Japanese)
- UNAIDS. 90-90-90—An Ambitious Treatment Target to Help end the AIDS Epidemic; UNAIDS: Geneva, Switzerland, 2017; Available online: https://www.unaids.org/en/resources/documents/2017/90-90-90 (accessed on 31 October 2021).
- Shimizu, K.; Negita, M. Lessons Learned from Japan’s Response to the First Wave of COVID-19: A Content Analysis. Healthcare 2020, 8, 426. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, K.; Wharton, G.; Sakamoto, H.; Mossialos, E. Resurgence of Covid-19 in Japan. BMJ 2020, 370, m3221. [Google Scholar] [CrossRef] [PubMed]
- Ejima, K.; Koizumi, Y.; Yamamoto, N.; Rosenberg, M.; Ludema, C.; Bento, A.I.; Yoneoka, D.; Ichikawa, S.; Mizushima, D.; Iwami, S. HIV Testing by Public Health Centers and Municipalities and New HIV Cases During the COVID-19 Pandemic in Japan. J. Acquir. Immune Defic. Syndr. 2021, 87, e182–e187. [Google Scholar] [CrossRef] [PubMed]
- Holtgrave, D.R.; Greenwald, R. A SWOT Analysis of the Updated National HIV/AIDS Strategy for the U.S., 2015–2020. AIDS Behav. 2016, 20, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Wang, Z. Strengths, Weaknesses, Opportunities and Threats (SWOT) Analysis of China’s Prevention and Control Strategy for the COVID-19 Epidemic. Int. J. Environ. Res. Public Health 2020, 17, 2235. [Google Scholar] [CrossRef] [Green Version]
- Torri, E.; Sbrogiò, L.G.; Di Rosa, E.; Cinquetti, S.; Francia, F.; Ferro, A. Italian Public Health Response to the COVID-19 Pandemic: Case Report from the Field, Insights and Challenges for the Department of Prevention. Int. J. Environ. Res. Public Health 2020, 17, 3666. [Google Scholar] [CrossRef]
- Fusco, A.; Dicuonzo, G.; Dell’Atti, V.; Tatullo, M. Blockchain in Healthcare: Insights on COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 7167. [Google Scholar] [CrossRef]
- The Minister of Health, Labour and Welfare, Japan. The Guidelines on Prevention of Specified Infectious Diseases on AIDS in Japan. Available online: https://www.mhlw.go.jp/file/06-Seisakujouhou-10900000-Kenkoukyoku/0000191837.pdf (accessed on 1 August 2021). (In Japanese)
- Chang, M.C.; Baek, J.H.; Park, D. Lessons from South Korea Regarding the Early Stage of the COVID-19 Outbreak. Healthcare 2020, 8, 229. [Google Scholar] [CrossRef]
- Choi, H.; Cho, W.; Kim, M.-H.; Hur, J.-Y. Public Health Emergency and Crisis Management: Case Study of SARS-CoV-2 Outbreak. Int. J. Environ. Res. Public Health 2020, 17, 3984. [Google Scholar] [CrossRef]
- Mullen, L.; Potter, C.; Gostin, L.O.; Cicero, A.; Nuzzo, J.B. An analysis of international health regulations emergency committees and public health emergency of international concern designations. BMJ Glob. Health 2020, 5, e002502. [Google Scholar] [CrossRef]
- Prevention Access Campaign. Consensus Statement. Available online: https://www.preventionaccess.org/consensus (accessed on 1 August 2021).
- Takano, M.; Iwahashi, K.; Satoh, I.; Araki, J.; Kinami, T.; Ikushima, Y.; Fukuhara, T.; Obinata, H.; Nakayama, Y.; Kikuchi, Y.; et al. Assessment of HIV prevalence among MSM in Tokyo using self-collected dried blood spots delivered through the postal service. BMC Infect Dis. 2018, 18, 627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Organisation for Economic Co-Operation and Development. Over the Rainbow? The Road to LGBTI Inclusion–How Does Japan Compare? Available online: https://www.oecd.org/japan/OECD-LGBTI-2020-Over-The-Rainbow-JAPAN.pdf (accessed on 1 August 2021).
- Katsuda, N.; Hinohara, Y.; Tomita, K.; Hamajima, N. Structure and roles of public health centers (hokenjo) in Japan. Nagoya J. Med. Sci. 2011, 73, 59–68. [Google Scholar] [PubMed]
- Taniguchi, K.; Hashimoto, S.; Kawado, M.; Murakami, Y.; Izumida, M.; Ohta, A.; Tada, Y.; Shigematsu, M.; Yasui, Y.; Nagai, M. Overview of infectious disease surveillance system in Japan, 1999–2005. J. Epidemiol. 2007, 17, S3–S13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimizu, K.; Nishiura, H.; Imamura, A. Investigation of the Proportion of Diagnosed People Living with HIV/AIDS among Foreign Residents in Japan. J. Clin. Med. 2019, 8, 804. [Google Scholar] [CrossRef] [Green Version]
- Shimizu, K.; Lin, L. Defamation Against Healthcare Workers During COVID-19 Pandemic. Int. J. Health Policy Manag. 2020. [Google Scholar] [CrossRef] [PubMed]
- Piot, P.; Abdool Karim, S.S.; Hecht, R.; Legido-Quigley, H.; Buse, K.; Stover, J.; Resch, S.; Ryckman, T.; Møgedal, S.; Dybul, M.; et al. Defeating AIDS—Advancing global health. Lancet 2015, 386, 171–218. [Google Scholar] [CrossRef]
- Dehne, K.L.; Dallabetta, G.; Wilson, D.; Garnett, G.P.; Laga, M.; Benomar, E.; Fakoya, A.; Baggaley, R.C.; Nelson, L.J.; Kasedde, S.; et al. HIV Prevention 2020: A framework for delivery and a call for action. Lancet HIV 2016, 3, e323–e332. [Google Scholar] [CrossRef] [Green Version]
- Hidaka, Y.; Ichikawa, S.; Koyano, J.; Urao, M.; Yasuo, T.; Kimura, H.; Ono-Kihara, M.; Kihara, M. Substance use and sexual behaviours of Japanese men who have sex with men: A nationwide internet survey conducted in Japan. BMC Public Health 2006, 6, 239. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. What’s the 2 + 1 + 1? Event-Driven Oral Pre-Exposure Prophylaxis to Prevent HIV for Men Who Have Sex with Men: Update to WHO’s Recommendation on oral PrEP. Available online: https://www.who.int/publications/i/item/what-s-the-2-1-1-event-driven-oral-pre-exposure-prophylaxis-to-prevent-hiv-for-men-who-have-sex-with-men (accessed on 1 August 2021).
- Grant, R.M.; Lama, J.R.; Anderson, P.L.; McMahan, V.; Liu, A.Y.; Vargas, L.; Goicochea, P.; Casapía, M.; Guanira-Carranza, J.V.; Ramirez-Cardich, M.E.; et al. Preexposure chemoprophylaxis for HIV prevention in men who have sex with men. N. Engl. J. Med. 2010, 363, 2587–2599. [Google Scholar] [CrossRef] [Green Version]
- Baeten, J.M.; Donnell, D.; Ndase, P.; Mugo, N.R.; Campbell, J.D.; Wangisi, J.; Tappero, J.W.; Bukusi, E.A.; Cohen, C.R.; Katabira, E.; et al. Antiretroviral prophylaxis for HIV prevention in heterosexual men and women. N. Engl. J. Med. 2012, 367, 399–410. [Google Scholar] [CrossRef] [Green Version]
- Molina, J.M.; Charreau, I.; Spire, B.; Cotte, L.; Chas, J.; Capitant, C.; Tremblay, C.; Rojas-Castro, D.; Cua, E.; Pasquet, A.; et al. Efficacy, safety, and effect on sexual behaviour of on-demand pre-exposure prophylaxis for HIV in men who have sex with men: An observational cohort study. Lancet HIV 2017, 4, e402–e410. [Google Scholar] [CrossRef] [Green Version]
- Gilmour, S.; Peng, L.; Li, J.; Oka, S.; Tanuma, J. New strategies for prevention of HIV among Japanese men who have sex with men: A mathematical model. Sci. Rep. 2020, 10, 18187. [Google Scholar] [CrossRef] [PubMed]
- Iwamoto, A.; Taira, R.; Yokomaku, Y.; Koibuchi, T.; Rahman, M.; Izumi, Y.; Tadokoro, K. The HIV care cascade: Japanese perspectives. PLoS ONE 2017, 12, e0174360. [Google Scholar] [CrossRef] [PubMed]
- Nishiura, H. Estimating the incidence and diagnosed proportion of HIV infections in Japan: A statistical modeling study. Peer J. 2019, 7, e6275. [Google Scholar] [CrossRef]
- Hill, A.O.; Bavinton, B.R.; Armstrong, G. Prevalence and correlates of lifetime and recent HIV testing among men who have sex with men (MSM) who use mobile geo-social networking applications in Greater Tokyo. PLoS ONE 2019, 14, e0209933. [Google Scholar] [CrossRef]
- Eguchi, H.; Wada, K.; Smith, D.R. Sociodemographic factors and prejudice toward HIV and Hepatitis B/C status in a workingage population: Results from a national, cross-sectional study in Japan. PLoS ONE 2014, 9, e96645. [Google Scholar] [CrossRef]
- Ssentongo, P.; Heilbrunn, E.S.; Ssentongo, A.E.; Advani, S.; Chinchilli, V.M.; Nunez, J.J.; Du, P. Epidemiology and outcomes of COVID-19 in HIV-infected individuals: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 6283. [Google Scholar] [CrossRef]
- Shimizu, K.; Tokuda, Y.; Shibuya, K. Japan should aim to eliminate covid-19. BMJ 2021, 372, n294. [Google Scholar] [CrossRef]
- Shimizu, K.; Sridhar, D.; Taniguchi, K.; Shibuya, K. Reconsider this summer’s Olympic and Paralympic games. BMJ 2021, 373, n962. [Google Scholar] [CrossRef]
- UNAIDS. Global AIDS Strategy 2021-2026–End Inequalities; End AIDS; UNAIDS: Geneva, Switzerland, 2021; Available online: https://www.unaids.org/en/resources/documents/2021/2021-2026-global-AIDS-strategy (accessed on 31 October 2021).
- Kanchanachitra, C.; Tangcharoensathien, V. Health inequality across prefectures in Japan. Lancet 2017, 390, 1471–1473. [Google Scholar] [CrossRef] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shimizu, K. A SWOT Analysis of the Guidelines on Prevention of HIV/AIDS in Japan in the Context of COVID-19. Infect. Dis. Rep. 2021, 13, 949-956. https://doi.org/10.3390/idr13040087
Shimizu K. A SWOT Analysis of the Guidelines on Prevention of HIV/AIDS in Japan in the Context of COVID-19. Infectious Disease Reports. 2021; 13(4):949-956. https://doi.org/10.3390/idr13040087
Chicago/Turabian StyleShimizu, Kazuki. 2021. "A SWOT Analysis of the Guidelines on Prevention of HIV/AIDS in Japan in the Context of COVID-19" Infectious Disease Reports 13, no. 4: 949-956. https://doi.org/10.3390/idr13040087
APA StyleShimizu, K. (2021). A SWOT Analysis of the Guidelines on Prevention of HIV/AIDS in Japan in the Context of COVID-19. Infectious Disease Reports, 13(4), 949-956. https://doi.org/10.3390/idr13040087