
Review of the Effectiveness of Various Adjuvant Therapies in Treating Mycobacterium tuberculosis

 ,
, 
Abstract
1. Introduction
2. Adjuvants
2.1. Glutathione
2.2. Everolimus
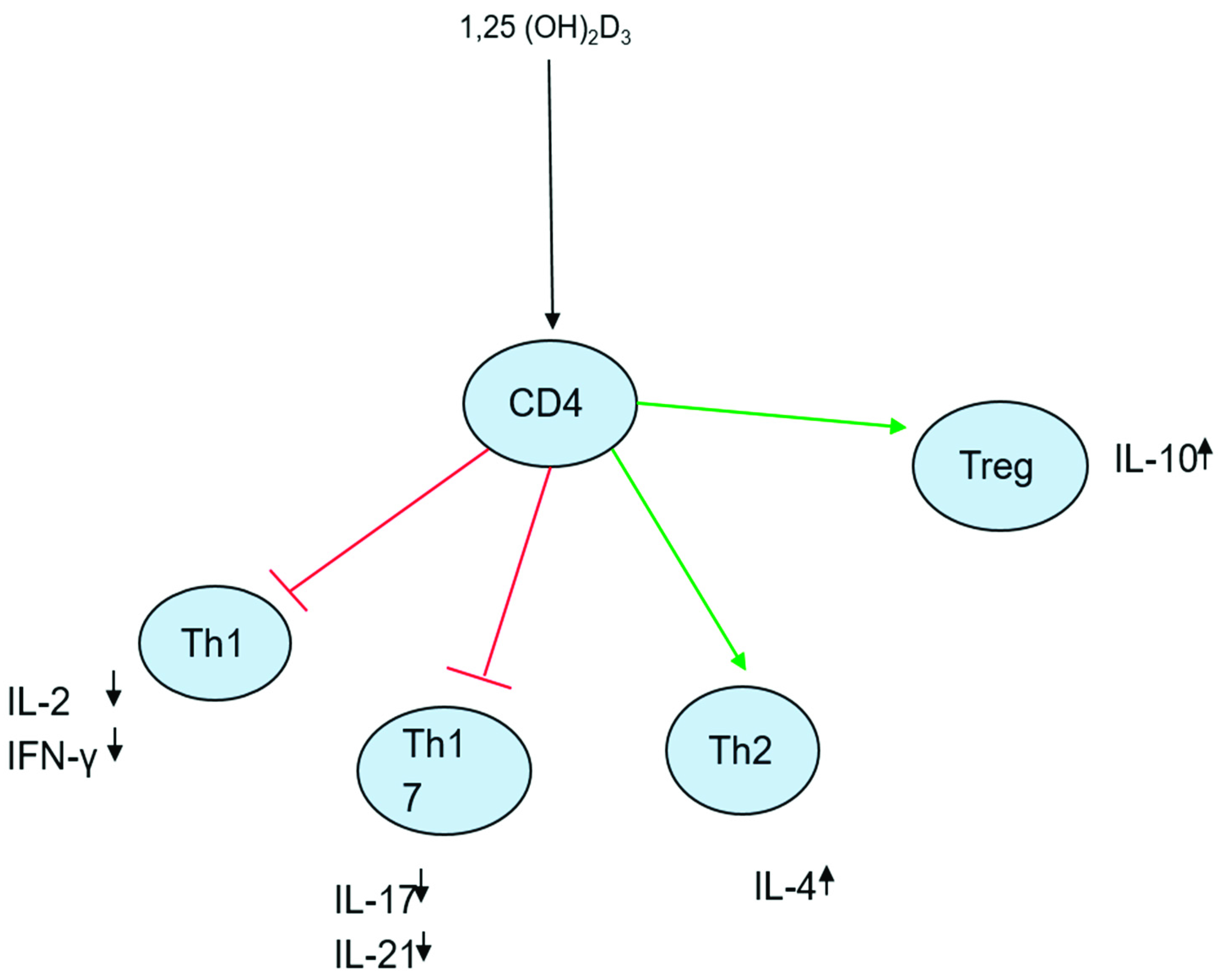
2.3. Vitamin D
2.4. Steroids
2.5. Aspirin
2.6. Statin
2.7. Metformin
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations List
| Multidrug resistant | (MDR) |
| Extensive drug resistant | (XDR) |
| Isoniazid | (INH) |
| Rifampin | (RIF) |
| Ethambutol | (EMB) |
| Pyrazinamide | (PZA) |
| Multidrug resistant TB | (MDR-TB) |
| Extensively drug-resistant TB | (XDR-TB) |
| Tuberculosis | (TB) |
| Mycobacterium tuberculosis | (Mtb) |
| Glutathione | (GSH) |
| Reduced glutathione | (GSH) |
| Oxidized glutathione | (GSSG) |
| Γ-glutamyltranspeptidase | (GGT) |
| Glutamate–cysteine ligase | (GCL) |
| Tumor necrosis factor alpha | (TNF-α) |
| Interferon gamma | (IFN-y) |
| Mammalian target of rapamycin | (mTOR) |
| T helper | (Th) |
| Toll-like receptors | (TLR) |
| Vitamin D receptors | (VDR) |
| Antigen-presenting cells | (APC) |
| Dendritic cells | (DC) |
| Mitogen-activated protein kinase phosphatase | (MKP-1) |
| Lymph node TB | (LNTB) |
| Prostaglandin E2 | (PGE2) |
| Low-density lipoprotein | (LDL) |
| Reactive oxygen species | (ROS) |
| Reactive nitrogen species | (RNS) |
| Adenosine monophosphate-activated protein kinase | (AMPK) |
| Mitochondrial ROS | (mROS) |
References
- Barberis, I.; Bragazzi, N.L.; Galluzzo, L.; Martini, M. The history of tuberculosis: From the first historical records to the isolation of Koch’s bacillus. J. Prev. Med. Hyg. 2017, 58, E9–E12. [Google Scholar]
- Chakaya, J.; Khan, M.; Ntoumi, F.; Aklillu, E.; Fatima, R.; Mwaba, P.; Kapata, N.; Mfinanga, S.; Hasnain, S.E.; Katoto, P.; et al. Global Tuberculosis Report 2020–Reflections on the Global TB burden, Treatment and Prevention Efforts. Available online: https://www.sciencedirect.com/science/article/pii/S1201971221001934 (accessed on 11 March 2021).
- Suárez, I.; Fünger, S.M.; Kröger, S.; Rademacher, J.; Fätkenheuer, G.; Rybniker, J. The Diagnosis and Treatment of Tuberculosis. Dtsch. Arztebl. Int. 2019, 116, 729–735. [Google Scholar] [CrossRef] [PubMed]
- Seung, K.J.; Keshavjee, S.; Rich, M. Multidrug-Resistant Tuberculosis and Extensively Drug-Resistant Tuberculosis. Cold Spring Harb. Perspect. Med. 2015, 5, a017863. [Google Scholar] [CrossRef]
- Zhang, Y.; Yew, W.-W. Mechanisms of drug resistance in Mycobacterium tuberculosis: Update 2015. Int. J. Tuberc. Lung Dis. 2015, 19, 1276–1289. [Google Scholar] [CrossRef]
- Pontali, E.; Raviglione, M.; Migliori, G.B.; the Writing Group Members of the Global TB Network Clinical Trials Committee. Regimens to treat multidrug-resistant tuberculosis: Past, present and future perspectives. Eur. Respir. Rev. Off. J. Eur. Respir. Soc. 2019, 28, 190035. [Google Scholar] [CrossRef] [PubMed]
- Meister, A. Glutathione metabolism and its selective modification. J. Biol. Chem. 1988, 263, 17205–17208. [Google Scholar] [CrossRef]
- Kaplowitz, N.; Aw, T.Y.; Ookhtens, M. The regulation of hepatic GSH. Annu. Rev. Pharmacol. Toxicol. 1985, 25, 714–744. [Google Scholar] [CrossRef]
- Meredith, M.J.; Reed, D.J. Status of the mitochondrial pool of glutathione in the isolated hepatocyte. J. Biol. Chem. 1982, 257, 3747–3753. [Google Scholar] [CrossRef]
- Hwang, C.; Sinskey, A.J.; Lodish, H.F. Oxidized redox state of glutathione in the endoplasmic reticulum. Science 1992, 257, 1496–1502. [Google Scholar] [CrossRef] [PubMed]
- Alton, M.; Anderson, M.E. Glutathione. Annu. Rev. Biochem. 1983, 52, 711–760. [Google Scholar]
- Suthanthiran, M.; Anderson, M.E.; Sharma, V.K.; Meister, A. Glutathione regulates activation-dependent DNA synthesis in highly purified normal human T lymphocytes stimulated via the CD2 and CD3 antigens. Proc. Natl. Acad. Sci. USA 1990, 87, 3343–3347. [Google Scholar] [CrossRef] [PubMed]
- Lu, S.C. Glutathione synthesis. Biochim. Biophys. Acta 2013, 1830, 3143–3153. [Google Scholar] [CrossRef] [PubMed]
- Oppenheimer, L.; Wellner, V.P.; Griffith, O.W.; Meister, A. Glutathione synthetase. Purification from rat kidney and mapping of the substrate binding sites. J. Biol. Chem. 1979, 254, 5184–5190. [Google Scholar] [CrossRef]
- Fernández-Checa, J.; Kaplowitz, N.; Garcia-Ruiz, C.; Colell, A.; Miranda, M.; Mai, M.; Ardite, E.; Morales, A. GSH transport in mitochondria: Defense against TNF-induced oxidative stress and alcohol-induced defect. Am. J. Physiol. 1997, 273, G7–G17. [Google Scholar] [CrossRef]
- Lu, S.C. Regulation of hepatic glutathione synthesis: Current concepts and controversies. FASEB J. 1999, 13, 1169–1183. [Google Scholar] [CrossRef]
- Volkman, H.E.; Clay, H.; Beery, D.; Chang, J.C.; Sherman, D.R.; Ramakrishnan, L. Tuberculous Granuloma Formation Is Enhanced by a Mycobacterium Virulence Determinant. PLoS Biol. 2004, 2, e367. [Google Scholar] [CrossRef]
- Domingo-Gonzalez, R.; Prince, O.; Cooper, A.; Khader, S.A. Cytokines and chemokines in Mycobacterium tuberculosis infection. Microbiol. Spectr. 2016, 4, 4–5. [Google Scholar] [CrossRef]
- Wallis, R. Reconsidering Adjuvant Immunotherapy for Tuberculosis. Clin. Infect. Dis. 2005, 41, 201–208. [Google Scholar] [CrossRef]
- Venketaraman, V.; Millman, A.; Salman, M.; Swaminathan, S.; Goetz, M.; Lardizabal, A.; Hom, D.; Connell, N.D. Glutathione levels and immune responses in tuberculosis patients. Microb. Pathog. 2008, 44, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Allen, M.; Bailey, C.; Cahatol, I.; Dodge, L.; Yim, J.; Kassissa, C.; Luong, J.; Kasko, S.; Pandya, S.; Venketaraman, V. Mechanisms of control of Mycobacterium tuberculosis by NK cells: Role of glutathione. Front. Immunol. 2015, 6, 508. [Google Scholar] [CrossRef]
- Ly, J.; Lagman, M.; Saing, T.; Singh, M.K.; Tudela, E.V.; Morris, D.; Anderson, J.; Daliva, J.; Ochoa, C.; Patel, N.; et al. Liposomal glutathione supplementation restores TH1 cytokine response to Mycobacterium tuberculosis infection in HIV-infected individuals. J. Interferon Cytokine Res. 2015, 35, 875–887. [Google Scholar] [CrossRef]
- Guerra, C.; Johal, K.; Morris, D.; Moreno, S.; Alvarado, O.; Gray, D.; Tanzil, M.; Pearce, D.; Venketeraraman, V. Control of Mycobacterium tuberculosis growth by activated natural killer cells. Clin. Exp. Immunol. 2012, 168, 142–152. [Google Scholar] [CrossRef] [PubMed]
- Greinert, U.; Ernst, M.; Schlaak, M.; Entzian, P. Interleukin-12 as successful adjuvant in tuberculosis treatment. Eur. Respir. J. 2001, 17, 1049–1051. [Google Scholar] [CrossRef]
- Cao, R.; Teskey, G.; Islamoglu, H.; Abrahem, R.; Munjal, S.; Gyurjian, K.; Zhong, L.; Venketaraman, V. Characterizing the Effects of Glutathione as an Immunoadjuvant in the Treatment of Tuberculosis. Antimicrob. Agents Chemother. 2018, 62, e01132-18. [Google Scholar] [CrossRef]
- Mootoo, A.; Stylianou, E.; Arias, M.A.; Reljic, R. TNF-α in Tuberculosis: A Cytokine with a Split Personality. Inflamm. Allergy-Drug Targets 2009, 8, 53–62. [Google Scholar] [CrossRef]
- Parul, S.; Bagchi, T. IL-10 modulates in vitro multinucleate giant cell formation in human tuberculosis. PLoS ONE 2013, 8, e77680. [Google Scholar]
- Hasskarl, J. Everolimus. Recent Results Cancer Res. 2018, 211, 101–123. [Google Scholar] [CrossRef]
- Guan, T.W.; Lin, Y.J.; Ou, M.Y.; Chen, K.B. Efficacy and safety of everolimus treatment on liver transplant recipients: A meta-analysis. Eur. J. Clin. Investig. 2019, 49, e13179. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Kim, S.G.; Blenis, J. Rapamycin: One Drug, Many Effects. Cell Metab. 2014, 19, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Cerni, S.; Shafer, D.; To, K.; Venketaraman, V. Investigating the Role of Everolimus in mTOR Inhibition and Autophagy Promotion as a Potential Host-Directed Therapeutic Target in Mycobacterium tuberculosis Infection. J. Clin. Med. 2019, 8, 232. [Google Scholar] [CrossRef]
- Singh, P.; Subbian, S. Harnessing the mTOR Pathway for Tuberculosis Treatment. Front. Microbiol. 2018, 9, 70. [Google Scholar] [CrossRef]
- Bento, C.F.; Empadinhas, N.; Mendes, V. Autophagy in the fight against tuberculosis. DNA Cell Biol. 2015, 34, 228–242. [Google Scholar] [CrossRef]
- Deretic, V. Autophagy in Tuberculosis. Cold Spring Harb. Perspect. Med. 2014, 4, a018481. [Google Scholar] [CrossRef] [PubMed]
- Mannick, J.B.; Del Giudice, G.; Lattanzi, M.; Valiante, N.M.; Praestgaard, J.; Huang, B.; Lonetto, M.A.; Maecker, H.T.; Kovarik, J.; Carson, S.; et al. mTOR inhibition improves immune function in the elderly. Sci. Transl. Med. 2014, 6, 268ra179. [Google Scholar] [CrossRef] [PubMed]
- Mannick, J.B.; Morris, M.; Hockey, H.P.; Roma, G.; Beibel, M.; Kulmatycki, K.; Watkins, M.; Shavlakadze, T.; Zhou, W.; Quinn, D.; et al. TORC1 inhibition enhances immune function and reduces infections in the elderly. Sci. Transl. Med. 2018, 10, eaaq1564. [Google Scholar] [CrossRef]
- Ashley, D.; Hernandez, J.; Cao, R.; To, K.; Yegiazaryan, A.; Abrahem, R.; Nguyen, T.; Owens, J.; Lambros, M.; Subbian, S.; et al. Antimycobacterial Effects of Everolimus in a Human Granuloma Model. J. Clin. Med. 2020, 9, 2043. [Google Scholar] [CrossRef] [PubMed]
- Wallis, R.S.; Ginindza, S.; Beattie, T.; Arjun, N.; Likoti, M.; Edward, V.A.; Rassool, M.; Ahmed, K.; Fielding, K.; Ahidjo, B.A.; et al. Adjunctive host-directed therapies for pulmonary tuberculosis: A prospective, open-label, phase 2, randomised controlled trial. Lancet Respir. Med. 2021, 9, 897–908. [Google Scholar] [CrossRef]
- Fijałkowska-Morawska, J.B.; Jagodzińska, M.; Nowicki, M. Pulmonary embolism and reactivation of tuberculosis during everolimus therapy in a kidney transplant recipient. Ann. Transplant. 2011, 16, 107–110. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.-Y.; Cheng, A.; Wang, S.M.; Tsai, M.K.; Chen, Y.S.; Wang, S.S.; Ho, C.M.; Hu, R.H.; Hsu, H.H.; Fang, C.T.; et al. 1383. Everolimus is Associated with an Increased Risk of Tuberculosis in Solid-Organ Transplant Recipients. Open Forum Infect. Dis. 2019, 6, S502. [Google Scholar] [CrossRef]
- Gupta, A.; Pant, G.; Mitra, K.; Madan, J.; Chourasia, M.K.; Misra, A. Inhalable particles containing rapamycin for induction of autophagy in macrophages infected with Mycobacterium tuberculosis. Mol. Pharm. 2014, 11, 1201–1207. [Google Scholar] [CrossRef]
- Cantorna, M.T.; Snyder, L.; Lin, Y.D.; Yang, L. Vitamin D and 1,25(OH)2D regulation of T cells. Nutrients 2015, 7, 3011–3021. [Google Scholar] [CrossRef]
- Liu, P.T.; Stenger, S.; Li, H.; Wenzel, L.; Tan, B.H.; Krutzik, S.R.; Ochoa, M.T.; Schauber, J.; Wu, K.; Meinken, C.; et al. Toll-like receptor triggering of a vitamin D-mediated human antimicrobial response. Science 2006, 311, 1770–1773. [Google Scholar] [CrossRef]
- Baeke, F.; Takiishi, T.; Korf, H.; Gysemans, C.; Mathieu, C. Vitamin D: Modulator of the immune system. Curr. Opin. Pharmacol. 2010, 10, 482–496. [Google Scholar] [CrossRef]
- Mathyssen, C.; Gayan-Ramirez, G.; Bouillon, R.; Janssens, W. Vitamin D supplementation in respiratory diseases: Evidence from randomized controlled trials. Pol. Arch. Intern. Med. 2017, 127, 775–784. [Google Scholar] [CrossRef][Green Version]
- Gou, X.; Lingli, P.; Tang, F.; Gao, H.; Xiao, D. The association between vitamin D status and tuberculosis in children: A meta-analysis. Medicine 2018, 97, e12179. [Google Scholar] [CrossRef]
- Aibana, O.; Huang, C.-C.; Aboud, S.; Arnedo-Pena, A.; Becerra, M.C.; Bellido-Blasco, J.B.; Bhosale, R.; Calderon, R.; Chiang, S.; Contreras, C.; et al. Vitamin D status and risk of incident tuberculosis disease: A nested case-control study, systematic review, and individual-participant data meta-analysis. PLoS Med. 2019, 16, e1002907. [Google Scholar] [CrossRef]
- Green, M. Cod liver oil and tuberculosis. BMJ 2011, 343, d7505. [Google Scholar] [CrossRef]
- Lu, P.; Liu, Q.; Martinez, L.; Yang, H.; Lu, W.; Ding, X.; Zhu, L. Time to sputum culture conversion and treatment outcome of patients with multidrug-resistant tuberculosis: A prospective cohort study from urban China. Eur. Respir. J. 2017, 49, 1601558. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Chen, C.; Yang, J. Effectiveness of vitamin D supplementation on the outcome of pulmonary tuberculosis treatment in adults: A meta-analysis of randomized controlled trials. Chin. Med. J. 2019, 132, 2950–2959. [Google Scholar] [CrossRef] [PubMed]
- Ganmaa, D.; Uyanga, B.; Zhou, X.; Gantsetseg, G. Vitamin D Supplements for Prevention of Tuberculosis Infection and Disease. N. Engl. J. Med. 2020, 383, 359–368. [Google Scholar] [CrossRef] [PubMed]
- Sudfeld, C.R.; Mugusi, F.; Muhihi, A.; Aboud, S.; Nagu, T.J.; Ulenga, N.; Hong, B.; Wang, M.; Fawzi, W.W. Efficacy of vitamin D3 supplementation for the prevention of pulmonary tuberculosis and mortality in HIV: A randomised, double-blind, placebo-controlled trial. Lancet HIV 2020, 7, e463–e471. [Google Scholar] [CrossRef]
- Janahi, I.A.; Rehman, A.; Baloch, N.U.-A. Corticosteroids and Their Use in Respiratory Disorders. In Corticosteroids; InTech Open: London, UK, 2018; pp. 47–57. [Google Scholar] [CrossRef]
- Cisneros, J.R.; Murray, K.M. Corticosteroids in tuberculosis. Ann. Pharmacother. 1996, 30, 1298–1303. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Wang, R.; Wang, H.; Yang, X.; Yang, J.; Xiong, W.; Wen, Q.; Ma, L. Glucocorticoids Suppress Antimicrobial Autophagy and Nitric Oxide Production and Facilitate Mycobacterial Survival in Macrophages. Sci. Rep. 2017, 7, 982. [Google Scholar] [CrossRef] [PubMed]
- Tükenmez, H.; Edström, I.; Kalsum, S.; Braian, C.; Ummanni, R.; Fick, S.B.; Sundin, C.; Lerm, M.; Elofsson, M.; Larsson, C. Corticosteroids protect infected cells against mycobacterial killing in vitro. Biochem. Biophys. Res. Commun. 2019, 511, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Gräb, J.; Suárez, I.; van Gumpel, E.; Winter, S.; Schreiber, F.; Esser, A.; Hölscher, C.; Fritsch, M.; Herb, M.; Schramm, M.; et al. Corticosteroids inhibit Mycobacterium tuberculosis-induced necrotic host cell death by abrogating mitochondrial membrane permeability transition. Nat. Commun. 2019, 10, 688. [Google Scholar] [CrossRef]
- Kadhiravan, T.; Deepanjali, S. Role of corticosteroids in the treatment of tuberculosis: An evidence-based update. Indian J. Chest Dis. Allied. Sci. 2010, 52, 153–158. [Google Scholar] [PubMed]
- Lee, C.H.; Kim, K.; Hyun, M.K.; Jang, E.J.; Lee, N.R.; Yim, J.J. Use of inhaled corticosteroids and the risk of tuberculosis. Thorax 2013, 68, 1105–1113. [Google Scholar] [CrossRef]
- Mayanja-Kizza, H.; Jones-Lopez, E.; Okwera, A.; Wallis, R.S.; Ellner, J.J.; Mugerwa, R.D.; Whalen, C.C. Uganda-Case Western Research Collaboration. Immunoadjuvant prednisolone therapy for HIV-associated tuberculosis: A phase 2 clinical trial in Uganda. J. Infect. Dis. 2005, 191, 856–865. [Google Scholar] [CrossRef]
- Smego, R.A.; Ahmed, N. A systematic review of the adjunctive use of systemic corticosteroids for pulmonary tuberculosis. Int. J. Tuberc. Lung. Dis. 2003, 7, 208–213. [Google Scholar] [PubMed]
- Critchley, J.A.; Orton, L.C.; Pearson, F. Adjunctive steroid therapy for managing pulmonary tuberculosis. Cochrane Database Syst. Rev. 2014, 11, CD011370. [Google Scholar] [CrossRef]
- World Health Organization. Guidelines for Treatment of Drug-Susceptible Tuberculosis and Patient Care. Available online: https://apps.who.int/iris/bitstream/handle/10665/255052/9789241550000-eng.pdf (accessed on 1 September 2021).
- Prasad, K.; Singh, M.B.; Ryan, H. Corticosteroids for managing tuberculous meningitis. Cochrane Database Syst. Rev. 2016, 4, CD002244-64. [Google Scholar] [CrossRef]
- Young, C.; Walzl, G.; Du Plessis, N. Therapeutic host-directed strategies to improve outcome in tuberculosis. Mucosal Immunol. 2019, 13, 190–204. [Google Scholar] [CrossRef] [PubMed]
- Isiguzo, G.; Du Bruyn, E.; Howlett, P.; Ntsekhe, M. Diagnosis and Management of Tuberculous Pericarditis: What Is New? Curr. Cardiol. Rep. 2020, 22, 2. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence (NICE). Tuberculosis (NICE Guideline 33); NICE: London, UK, 2016. [Google Scholar]
- Wiysonge, C.S.; Ntsekhe, M.; Thabane, L.; Volmink, J.; Majombozi, D.; Gumedze, F.; Pandie, S.; Mayosi, B.M. Interventions for treating tuberculous pericarditis. Cochrane Database Syst. Rev. 2017, 2017, CD000526. [Google Scholar] [CrossRef]
- Bunkar, M.L.; Agnihotri, S.P.; Gupta, P.R.; Arya, S. Add-on prednisolone in the management of cervical lymph node tuberculosis. Indian J. Tuberc. 2016, 63, 96–99. [Google Scholar] [CrossRef]
- Sharmin, A.; Hossain, A.; Islam, N.; Sarker, Z.H.; Hossain, S.S.; Khan, M.A. Outcome of lymph node tuberculosis management with conventional treatment with and without prednisolone. Trop. Dr. 2021, 10, 49475520984745. [Google Scholar] [CrossRef]
- Hybiak, J.; Broniarek, I.; Kiryczyński, G.; Los, L.D.; Rosik, J.; Machaj, F.; Sławiński, H.; Jankowska, K.; Urasińska, E. Aspirin and its pleiotropic application. Eur. J. Pharmacol. 2019, 866, 172762. [Google Scholar] [CrossRef] [PubMed]
- Kroesen, V.M.; Gröschel, M.I.; Martinson, N.; Zumla, A.; Maeurer, M.; van der Werf, T.S.; Vilaplana, C. Non-Steroidal Anti-inflammatory Drugs As Host-Directed Therapy for Tuberculosis: A Systematic Review. Front. Immunol. 2017, 8, 772. [Google Scholar] [CrossRef] [PubMed]
- Mortensen, R.; Clemmensen, H.S.; Woodworth, J.S.; Therkelsen, M.L.; Mustafa, T.; Tonby, K.; Jenum, S.; Agger, E.M.; Dyrhol-Riise, A.M.; Andersen, P. Cyclooxygenase inhibitors impair CD4 T cell immunity and exacerbate Mycobacterium tuberculosis infection in aerosol-challenged mice. Commun. Biol. 2019, 2, 5. [Google Scholar] [CrossRef] [PubMed]
- Byrne, S.T.; Denkin, S.M.; Zhang, Y. Aspirin and ibuprofen enhance pyrazinamide treatment of murine tuberculosis. J. Antimicrob. Chemother. 2006, 59, 313–316. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Du, Z.; Ni, M.; Wang, Z.; Liang, M.; Sheng, H.; Zhang, A.; Yang, J. Aspirin enhances the clinical efficacy of anti-tuberculosis therapy in pulmonary tuberculosis in patients with type 2 diabetes mellitus. Infect. Dis. 2020, 52, 721–729. [Google Scholar] [CrossRef]
- Yadav, R. Role of aspirin as an adjuvant therapy in tuberculous meningitis in adults: The time has come for a phase III randomized controlled trial. Neurol. India 2018, 66, 1678. [Google Scholar] [CrossRef]
- Parihar, S.P.; Guler, R.; Khutlang, R.; Lang, D.M.; Ramona, H.; Musa, M.M.; Suzuki, H.; Marais, A.D.; Brombacher, F. Statin therapy reduces the mycobacterium tuberculosis burden in human macrophages and in mice by enhancing autophagy and phagosome maturation. J. Infect. Dis. 2013, 209, 754–763. [Google Scholar] [CrossRef] [PubMed]
- Dara, Y.; Volcani, D.; Shah, K.; Shin, K.; Venketaraman, V. Potentials of Host-Directed Therapies in Tuberculosis Management. J. Clin. Med. 2019, 8, 1166. [Google Scholar] [CrossRef] [PubMed]
- Dutta, N.K.; Bruiners, N.; Zimmerman, M.D.; Tan, S.; Dartois, V.; Gennaro, M.L.; Karakousis, P.C. Adjunctive Host-Directed Therapy With Statins Improves Tuberculosis-Related Outcomes in Mice. J. Infect. Dis. 2019, 221, 1079–1087. [Google Scholar] [CrossRef]
- Dutta, N.K.; Bruiners, N.; Pinn, M.L.; Zimmerman, M.D.; Prideaux, B.; Dartois, V.; Gennaro, M.L.; Karakousis, P.C. Statin adjunctive therapy shortens the duration of TB treatment in mice. J. Antimicrob. Chemother. 2016, 71, 1570–1577. [Google Scholar] [CrossRef]
- Skerry, C.; Pinn, M.L.; Bruiners, N.; Pine, R.; Gennaro, M.L.; Karakousis, P.C. Simvastatin increases the in vivo activity of the first-line tuberculosis regimen. J. Antimicrob. Chemother. 2014, 69, 2453–2457. [Google Scholar] [CrossRef]
- Alffenaar, J.-W.C.; Akkerman, O.W.; Hest, R.V. Statin Adjunctive Therapy for Tuberculosis Treatment. Agents Chemother. 2016, 60, 7004. [Google Scholar] [CrossRef]
- Liao, K.-F.; Lin, C.L.; Lai, S.W. Population-Based Case-Control Study Assessing the Association between Statins Use and Pulmonary Tuberculosis in Taiwan. Front. Pharmacol. 2017, 8, 597. [Google Scholar] [CrossRef] [PubMed]
- Vashisht, R.; Brahmachari, S.K. Metformin as a potential combination therapy with existing front-line antibiotics for Tuberculosis. J. Transl. Med. 2015, 13, 83. [Google Scholar] [CrossRef]
- Lachmandas, E.; Eckold, C.; Böhme, J.; Koeken, V.A.C.M.; Marzuki, M.B.; Blok, B.; Arts, R.J.W.; Chen, J.; Teng, K.W.W.; Ratter, J.; et al. Metformin Alters Human Host Responses to Mycobacterium tuberculosis in Healthy Subjects. J. Infect. Dis. 2019, 220, 139–150. [Google Scholar] [CrossRef] [PubMed]
- Degner, N.R.; Wang, J.Y.; Golub, J.E.; Karakousis, P.C. Metformin Use Reverses the Increased Mortality Associated With Diabetes Mellitus during Tuberculosis Treatment. Clin. Infect. Dis. 2017, 66, 198–205. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, K.; Salgame, P. Host innate immune response to Mycobacterium tuberculosis. J. Clin. Immunol. 2007, 27, 347–362. [Google Scholar] [CrossRef] [PubMed]
- Singhal, A.; Jie, L.; Kumar, P.; Hong, G.S.; Leow, M.K.; Paleja, B.; Tsenova, L.; Kurepina, N.; Chen, J.; Zolezzi, F.; et al. Metformin as adjunct antituberculosis therapy. Sci. Transl. Med. 2014, 6, 263ra159. [Google Scholar] [CrossRef]
- Naicker, N.; Sigal, A.; Naidoo, K. Metformin as Host-Directed Therapy for TB Treatment: Scoping Review. Front. Microbiol. 2020, 11, 435. [Google Scholar] [CrossRef] [PubMed]
- Rayasam, G.V.; Tanjore, S.B. Exploring the potential of adjunct therapy in tuberculosis. Trends Pharmacol. Sci. 2015, 36, 506–513. [Google Scholar] [CrossRef]


{kind=link}
| Author | Population | Vitamin D Dose | Duration | Findings |
|---|---|---|---|---|
| Martineau et al. (Mathyssen, Carolien et al., 2017) | 146 adults | 2.5 mg at start, and at days 14, 28, and 42 | 56 days | No effect on sputum culture conversion on the overall population. |
| Wejse et al. (Mathyssen, Carolien et al., 2017) | 365 adults | 100,000 IU at start, 3 months, 5 months, and 8 months | 1 year | No effect on clinical outcome/mortality |
| Tukvadze et al. (Mathyssen, Carolien et al., 2017) | 199 adults | 50,000 IU 3×/week for 8 weeks, followed by every other week for another 8 weeks | 16 weeks | No improvement in sputum TB clearance |
| Ganmaa et al. (Ganmaa, Davaasambuu et al., 2020) [51] | 8851 children | 14,000 IU vitamin D3 or placebo | 3 years | Not lower risk of TB infection |
| Sudfeld et al. (Sudfeld, Christopher R et al., 2020) [52] | 6250 HIV+ adults | 50,000 IU Vitamin D3 for first month of ART followed by 2000 IU Vitamin D3 daily | 3 years | No overall effect of supplementation on mortality risk. No difference in incidence of pulmonary TB between Vitamin D3 vs. placebo |
| Morcos et al. [41] (Mathyssen, Carolien et al., 2017) | 24 children (<13 y/o) | 1000 IU daily. No placebo implemented | 8 weeks | Clinical improvement in radiography (X-ray and Ultrasound). Weight gain in patients |
| Nursyam et al. [41] (Mathyssen, Carolien et al., 2017) | 67 patients (15–59 y/o) | 0.25 mg daily × 6 weeks | 12 weeks | Increased rate of sputum conversion. Improved radiologic findings |
| Salahuddin et al. [41] (Mathyssen, Carolien et al., 2017) | 259 patients (>16 y/o) | 2 IM injections of 600,000 IU given at 1 month apart | 12 weeks | Faster clinical and radiographic improvement. Enhanced host immune activation |
| Hassanein et al. [41] (Mathyssen, Carolien et al., 2017) | 60 adults | 1 IM injection of 200,000 IU | 8 weeks | Enhanced TB score and more rapid sputum conversion rates |
| Author | Population | Metformin Dose | Duration | Findings |
|---|---|---|---|---|
| Lachmandas et al., 2019 | 11 healthy adults | Increasing dose starting at 500 mg to 1000 mg for 5 consecutive days. | 5 days |
|
| Marupuru et al., 2017 | Diabetics diagnosed with TB were the study group (SG = 152), and diabetics without TB were the control group (CG = 299). | 500 mg and 1000 mg | 8 months |
|
| Nicholas R Degner et al., 2018 [86] | 2416 patients ≥ 13 years old undergoing TB treatment | Variable among patients | Retrospective cohort study between 2000 and 2013 |
|
| Adjuvant | Findings/Conclusions |
|---|---|
| Glutathione | These findings suggest that GSH can be a potential adjunct treatment with the previously mentioned first line antibiotics to clear Mtb infection via decrease in TNF-α and restoring redox homeostasis |
| Everolimus | More studies should be conducted |
| Vitamin D | Shorten sputum conversion times, but more randomized control trials are needed. |
| Steroids | Additional studies with larger sample sizes must be conducted in order to come up with stronger conclusions supporting their use. |
| Aspirin | aspirin shows potential to be an effective adjuvant therapy when combined with first-line anti-TB agents by reducing inflammation and amplifying the effects of anti-TB agents. |
| Statins | more studies are needed with statins that lack drug–drug interactions with first-line anti-TB agents |
| Metformin | Metformin is a strong drug candidate to be used in conjunction with classic anti-TB medication to help better reduce the severity and mortality of TB through its proposed mechanism of inhibiting the mTOR and MAPK pathways. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amin, A.; Vartanian, A.; Yegiazaryan, A.; Al-Kassir, A.L.; Venketaraman, V. Review of the Effectiveness of Various Adjuvant Therapies in Treating Mycobacterium tuberculosis. Infect. Dis. Rep. 2021, 13, 821-834. https://doi.org/10.3390/idr13030074
Amin A, Vartanian A, Yegiazaryan A, Al-Kassir AL, Venketaraman V. Review of the Effectiveness of Various Adjuvant Therapies in Treating Mycobacterium tuberculosis. Infectious Disease Reports. 2021; 13(3):821-834. https://doi.org/10.3390/idr13030074
Chicago/Turabian StyleAmin, Arman, Artin Vartanian, Aram Yegiazaryan, Abdul Latif Al-Kassir, and Vishwanath Venketaraman. 2021. "Review of the Effectiveness of Various Adjuvant Therapies in Treating Mycobacterium tuberculosis" Infectious Disease Reports 13, no. 3: 821-834. https://doi.org/10.3390/idr13030074
APA StyleAmin, A., Vartanian, A., Yegiazaryan, A., Al-Kassir, A. L., & Venketaraman, V. (2021). Review of the Effectiveness of Various Adjuvant Therapies in Treating Mycobacterium tuberculosis. Infectious Disease Reports, 13(3), 821-834. https://doi.org/10.3390/idr13030074