Increased Overall Mortality in Patients Admitted for Gastrointestinal Bleeding and COVID-19 Infection Compared to No COVID-19 Infection: A Systematic Review and Meta-Analysis

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
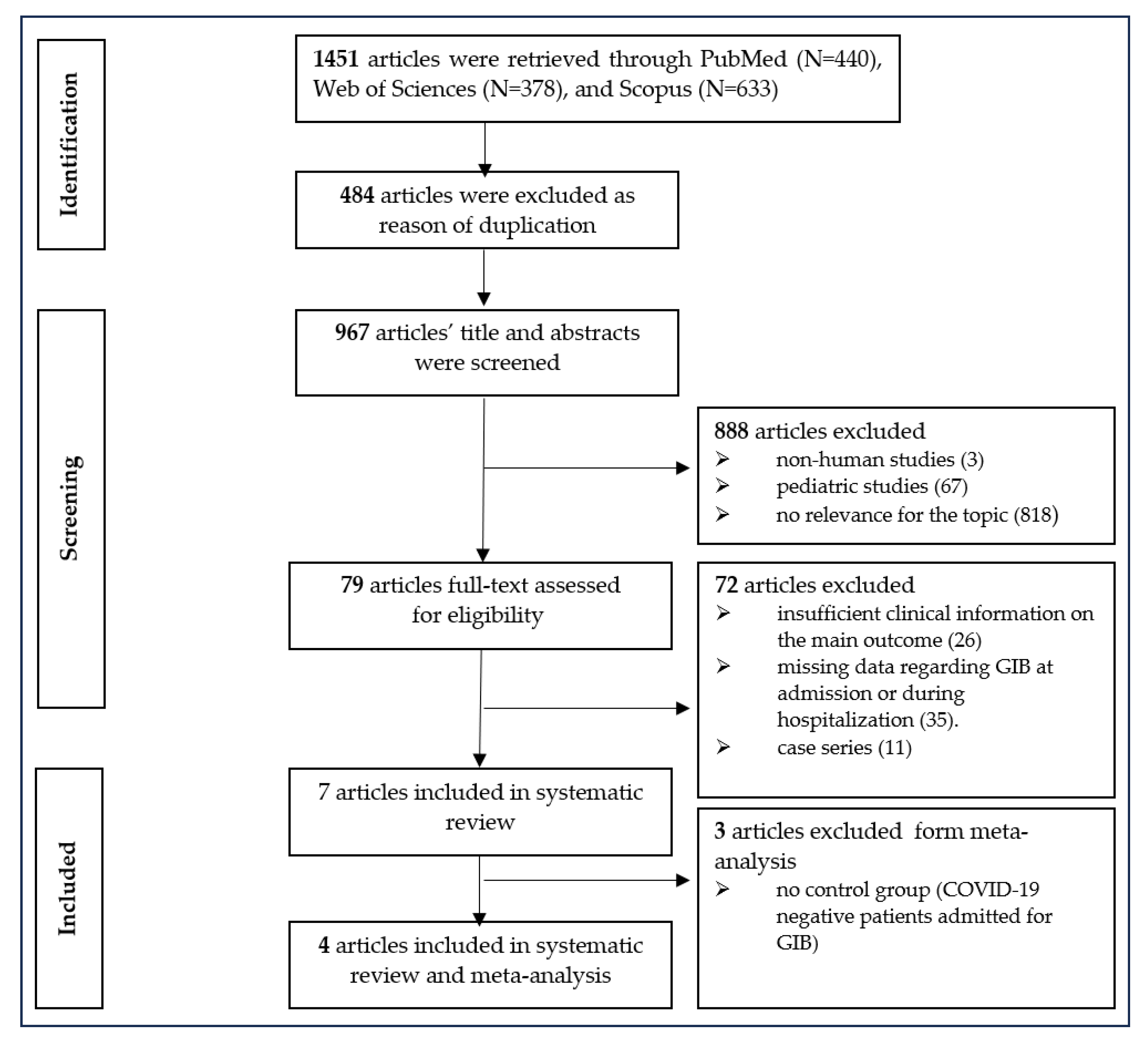
2.1. Search Strategies
2.2. Outcome Variables and Data Extraction
2.3. Statistical Analysis
3. Results
3.1. Characteristics of the Included Studies
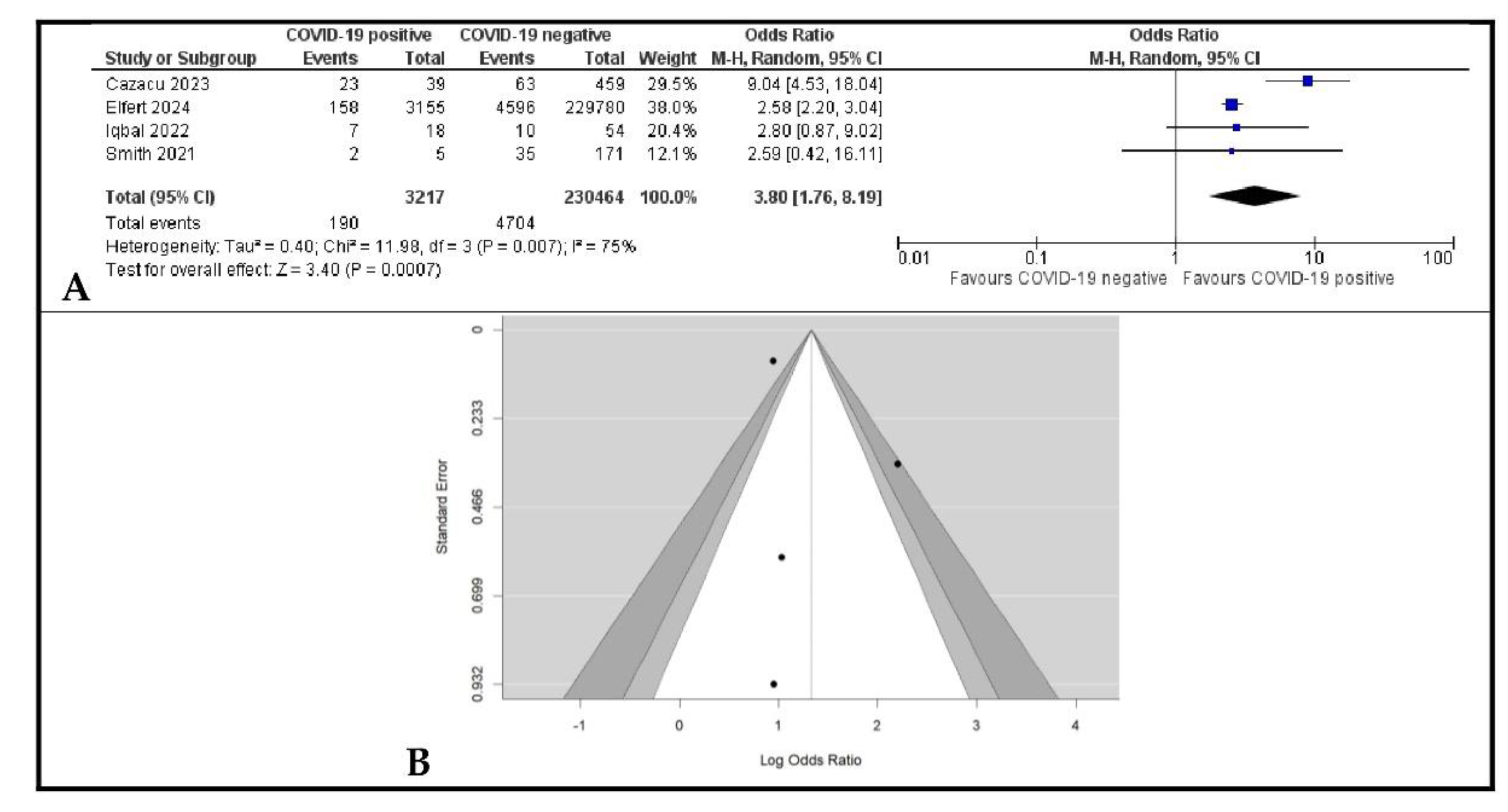
3.2. The Impact of COVID-19 on the Overall Mortality of Patients with GIB
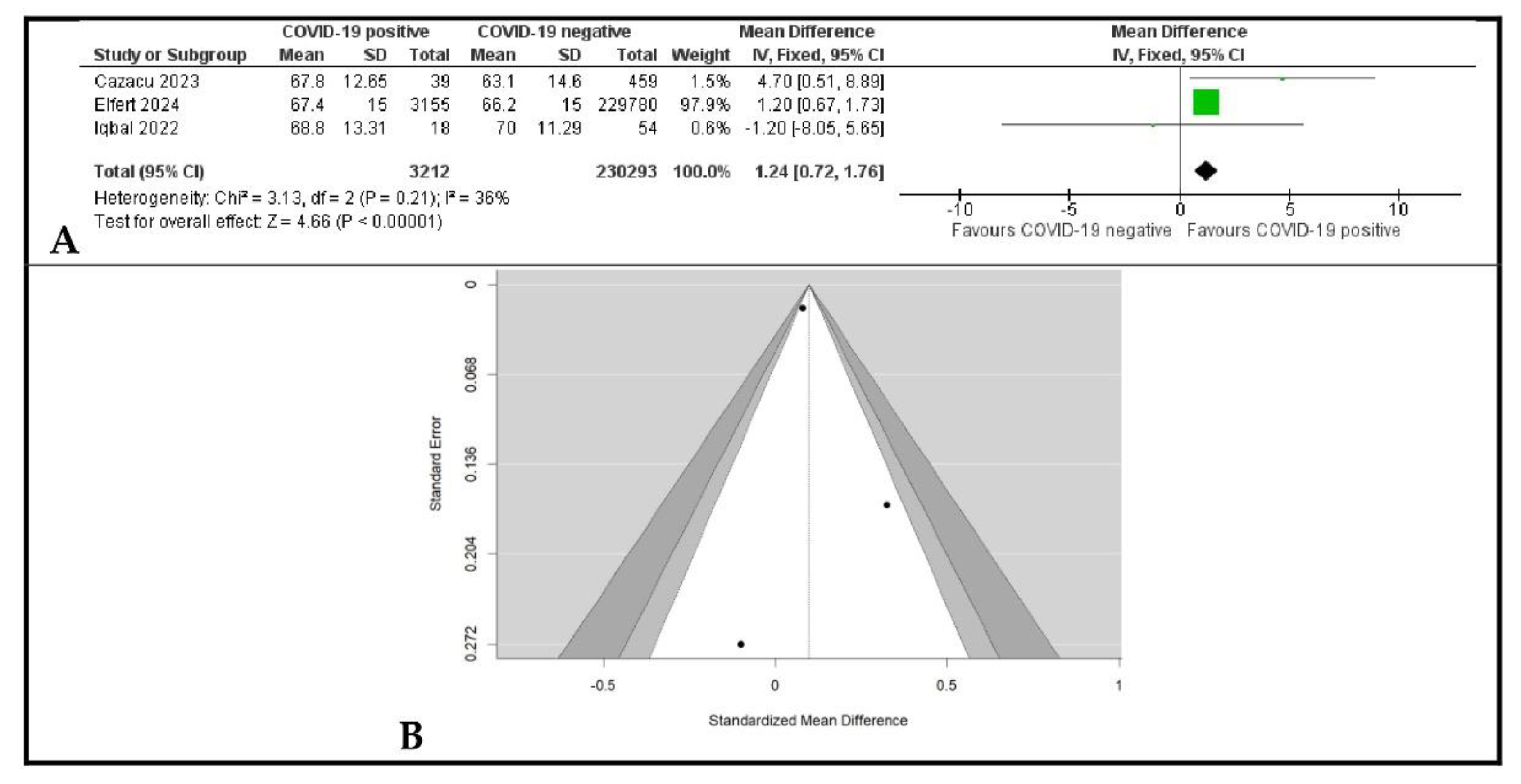
3.3. The Association Between Age and COVID-19 Positivity
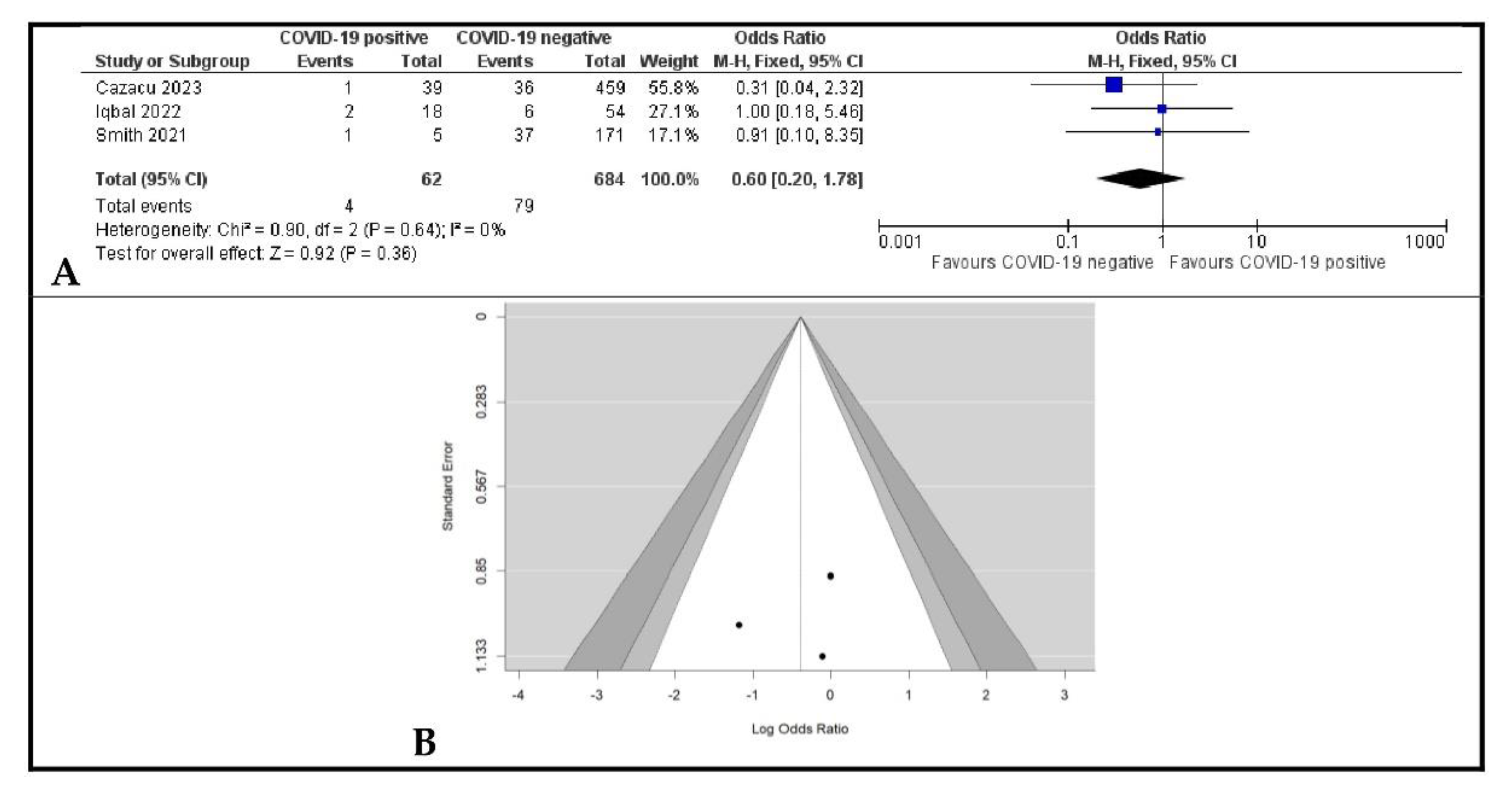
3.4. The Impact of COVID-19 Positivity on Rebleeding in Patients with GIB
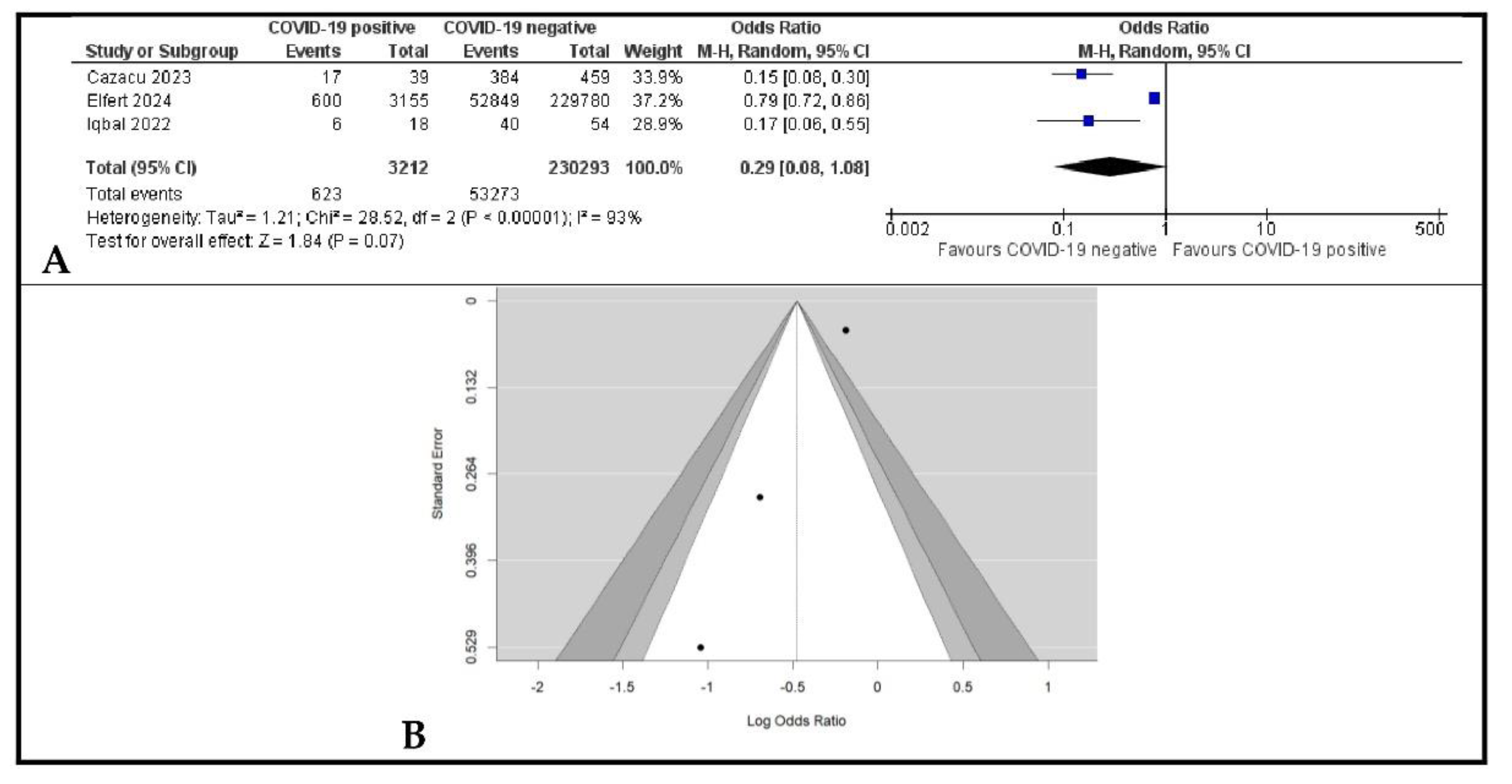
3.5. The Impact of COVID-19 Positivity on the Rate of Diagnostic Upper Digestive Endoscopy in Patients with GIB
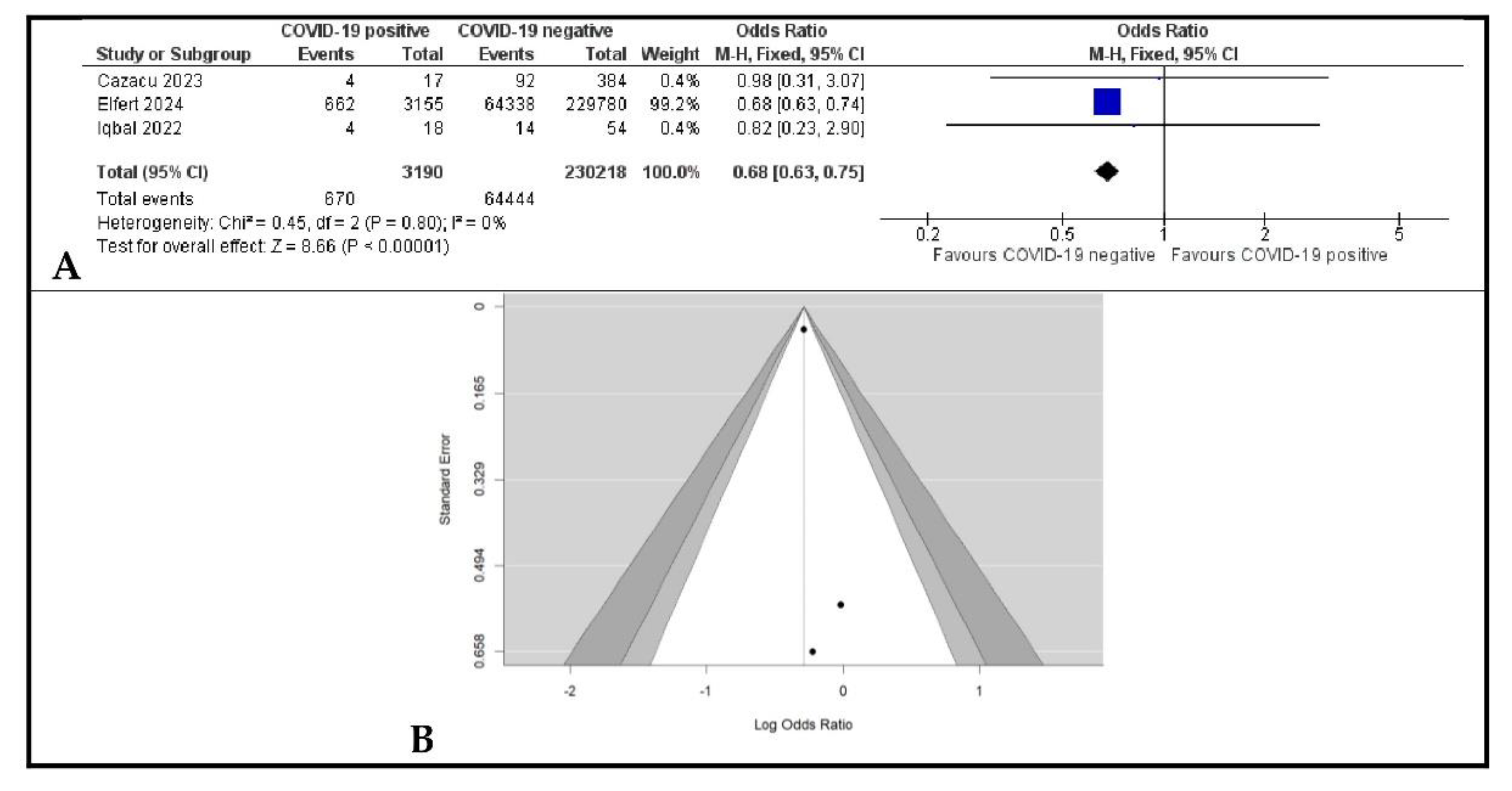
3.6. The Impact of COVID-19 Positivity on Therapeutic Upper Digestive Endoscopy in Patients with GIB
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Karlafti, E.; Tsavdaris, D.; Kotzakioulafi, E.; Protopapas, A.A.; Kaiafa, G.; Netta, S.; Savopoulos, C.; Michalopoulos, A.; Paramythiotis, D. The Prevalence of Gastrointestinal Bleeding in COVID-19 Patients: A Systematic Review and Meta-Analysis. Medicina 2023, 59, 1500. [Google Scholar] [CrossRef]
- Marasco, G.; Maida, M.; Morreale, G.C.; Licata, M.; Renzulli, M.; Cremon, C.; Stanghellini, V.; Barbara, G. Gastrointestinal Bleeding in COVID-19 Patients: A Systematic Review with Meta-Analysis. Can. J. Gastroenterol. Hepatol. 2021, 2021, 2534975. [Google Scholar] [CrossRef]
- Iqbal, U.; Anwar, H.; Siddiqui, H.U.; Khan, M.A.; Kamal, F.; Confer, B.D.; Khara, H.S. Acute Gastrointestinal Bleeding in COVID-19 Patients: A Systematic Review and Meta-Analysis. Clin. Endosc. 2021, 54, 534–541. [Google Scholar] [CrossRef]
- Elshazli, R.M.; Kline, A.; Elgaml, A.; Aboutaleb, M.H.; Salim, M.M.; Omar, M.; Munshi, R.; Mankowski, N.; Hussein, M.H.; Attia, A.S.; et al. Gastroenterology manifestations and COVID-19 outcomes: A meta-analysis of 25,252 cohorts among the first and second waves. J. Med. Virol. 2021, 93, 2740–2768. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Hang, Y. Characteristics, risk factors and outcomes of gastrointestinal hemorrhage in COVID-19 patients: A meta-analysis. Pak. J. Med. Sci. 2021, 37, 1524–1531. [Google Scholar] [CrossRef] [PubMed]
- Velev, V.; Popov, M.; Velikov, P.; Dinkova, M.; Ilieva, V.; Gospodinova, G.; Tcherveniakova, T.; Pavlova, M. COVID-19 and gastrointestinal injury: A brief systematic review and data from Bulgaria. Le Infez. Med. 2020, 28 (Suppl. S1), 37–41. [Google Scholar]
- Mehta, D.; Kelkar, R.; Patel, N.; Trivedi, P.D.; Dawoodi, S.; Patel, D.; Solanki, D.; Hussain, A.; Nagaraj, S.; Khayat, A.; et al. Gastrointestinal Manifestations and Outcomes of COVID-19: A Comprehensive Systematic Review and Meta-analysis. Cureus 2023, 15, e47028. [Google Scholar] [CrossRef]
- Ashktorab, H.; Russo, T.; Oskrochi, G.; Latella, G.; Massironi, S.; Luca, M.; Chirumamilla, L.G.; Laiyemo, A.O.; Brim, H. Clinical and Endoscopic Outcomes in Coronavirus Disease-2019 Patients With Gastrointestinal Bleeding. Gastro Hep Adv. 2022, 1, 487–499. [Google Scholar] [CrossRef]
- Bisen, A.C.; Agrawal, S.; Sanap, S.N.; Ravi Kumar, H.G.; Kumar, N.; Gupta, R.; Bhatta, R.S. COVID-19 retreats and world recovers: A silver lining in the dark cloud. Health Care Sci. 2023, 2, 264–285. [Google Scholar] [CrossRef]
- Dhama, K.; Nainu, F.; Frediansyah, A.; Yatoo, M.I.; Mohapatra, R.K.; Chakraborty, S.; Zhou, H.; Islam, M.R.; Mamada, S.S.; Kusuma, H.I.; et al. Global emerging Omicron variant of SARS-CoV-2: Impacts, challenges and strategies. J. Infect. Public Health 2023, 16, 4–14. [Google Scholar] [CrossRef]
- Marginean, C.M.; Popescu, M.; Vasile, C.M.; Cioboata, R.; Mitrut, P.; Popescu, I.A.S.; Biciusca, V.; Docea, A.O.; Mitrut, R.; Marginean, I.C.; et al. Challenges in the Differential Diagnosis of COVID-19 Pneumonia: A Pictorial Review. Diagnostics 2022, 12, 2823. [Google Scholar] [CrossRef] [PubMed]
- Ye, L.; Yang, Z.; Liu, J.; Liao, L.; Wang, F. Digestive system manifestations and clinical significance of coronavirus disease 2019: A systematic literature review. J. Gastroenterol. Hepatol. 2021, 36, 1414–1422. [Google Scholar] [CrossRef] [PubMed]
- Sweed, D.; Abdelsameea, E.; Khalifa, E.A.; Abdallah, H.; Moaz, H.; Moaz, I.; Abdelsattar, S.; Abdel-Rahman, N.; Mosbeh, A.; Elmahdy, H.A.; et al. SARS-CoV-2-associated gastrointestinal and liver diseases: What is known and what is needed to explore. Egypt. Liver J. 2021, 11, 64. [Google Scholar] [CrossRef]
- Aslan, A.T.; Şimşek, H. Clinical Features and Pathophysiological Mechanisms of COVID-19-associated Gastrointestinal Manifestations. Euroasian J. Hepato-Gastroenterol. 2021, 11, 81–86. [Google Scholar] [CrossRef]
- Orpen-Palmer, J.; Stanley, A.J. Update on the management of upper gastrointestinal bleeding. BMJ Med. 2022, 1, e000202. [Google Scholar] [CrossRef]
- Negro, A.; Villa, G.; Rolandi, S.; Lucchini, A.; Bambi, S. Gastrointestinal Bleeding in COVID-19 Patients: A Rapid Review. Gastroenterol. Nurs. 2022, 45, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Holster, I.L.; Kuipers, E.J. Management of acute nonvariceal upper gastrointestinal bleeding: Current policies and future perspectives. World J. Gastroenterol. 2012, 18, 1202–1207. [Google Scholar] [CrossRef]
- Jafar, W.; Jafar, A.J.N.; Sharma, A. Upper gastrointestinal haemorrhage: An update. Frontline Gastroenterol. 2016, 7, 32–40. [Google Scholar] [CrossRef]
- Cazacu, S.M.; Alexandru, D.O.; Statie, R.C.; Iordache, S.; Ungureanu, B.S.; Iovănescu, V.F.; Popa, P.; Sacerdoțianu, V.M.; Neagoe, C.D.; Florescu, M.M. The Accuracy of Pre-Endoscopic Scores for Mortality Prediction in Patients with Upper GI Bleeding and No Endoscopy Performed. Diagnostics 2023, 13, 1188. [Google Scholar] [CrossRef]
- Martin, T.A.; Wan, D.W.; Hajifathalian, K.; Tewani, S.; Shah, S.L.; Mehta, A.; Kaplan, A.; Ghosh, G.; Choi, A.J.; Krisko, T.I.; et al. Gastrointestinal Bleeding in Patients With Coronavirus Disease 2019: A Matched Case-Control Study. Off. J. Am. Coll. Gastroenterol. 2020, 115, 1609–1616. [Google Scholar] [CrossRef]
- Cazacu, S.M.; Burtea, D.E.; Iovănescu, V.F.; Florescu, D.N.; Iordache, S.; Turcu-Stiolica, A.; Sacerdotianu, V.M.; Ungureanu, B.S. Outcomes in Patients Admitted for Upper Gastrointestinal Bleeding and COVID-19 Infection: A Study of Two Years of the Pandemic. Life 2023, 13, 890. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rathore, S.S.; Wint, Z.S.; Goyal, A.; Jeswani, B.M.; Farrukh, A.M.; Nieto-Salazar, M.A.; Thugu, T.R.; Erva, S.; Mehmood, R.; Toro-Velandia, A.C.; et al. Prevalence and outcomes of upper gastrointestinal bleeding in COVID-19: A systematic review and meta-analysis. Rev. Med. Virol. 2024, 34, e2509. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Higgins, J.; Green, S. Cochrane Collaboration. In Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2008. [Google Scholar]
- Viechtbauer, W. Conducting Meta-Analyses in R with the metafor Package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef]
- Shalimar Vaishnav, M.; Elhence, A.; Kumar, R.; Mohta, S.; Palle, C.; Kumar, P.; Ranjan, M.; Vajpai, T.; Prasad, S.; Yegurla, J. Outcome of Conservative Therapy in Coronavirus disease-2019 Patients Presenting With Gastrointestinal Bleeding. J. Clin. Exp. Hepatol. 2021, 11, 327–333. [Google Scholar] [CrossRef]
- Rosevics, L.; Fossati, B.S.; Teixeira, S.; Bem, R.S.; Souza, R.C.A. COVID-19 and digestive endoscopy: Emergency endoscopic procedures and risk factors for upper gastrointestinal bleeding. Arq. Gastroenterol. 2021, 58, 337–343. [Google Scholar] [CrossRef]
- Iqbal, U.; Patel, P.D.; Pluskota, C.A.; Berger, A.L.; Khara, H.S.; Confer, B.D. Outcomes of Acute Gastrointestinal Bleeding in Patients With COVID-19: A Case-Control Study. Gastroenterol. Res. 2022, 15, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.; Brooks, C.; Rammage, J. Short report on acute gastro-intestinal bleeding admissions during the COVID-19 pandemic. JGH Open 2022, 6, 263–265. [Google Scholar] [CrossRef]
- Elfert, K.; Malik, M.; Aboursheid, T.; Mohamed, M.; Elfert, Y.; Beran, A.; Jaber, F.; Elromisy, E.; Al-Taee, A.; Kahaleh, M. Impact of COVID-19 infection on patients admitted with nonvariceal upper gastrointestinal bleeding: An analysis from the National Inpatient Sample. Bayl. Univ. Med. Cent. Proc. 2023, 37, 36–41. [Google Scholar] [CrossRef]
- Ion, D.; Paduraru, D.; Bolocan, A.; Musat, F.; Andronic, O.; Palcău, C.A. Gastro-Intestinal Bleeding in COVID-19 Patients—Is There Any Causal Relation? Chirurgia 2021, 116 (Suppl. S6), S69–S76. [Google Scholar]
- Gadiparthi, C.; Perisetti, A.; Sayana, H.; Tharian, B.; Inamdar, S.; Korman, A. Gastrointestinal Bleeding in Patients with Severe SARS-CoV-2. Am. J. Gastroenterol. 2020, 115, 1283–1285. [Google Scholar] [CrossRef] [PubMed]
- Barrett, L.F.; Lo, K.B.; Stanek, S.R.; Walter, J.W. Self-limited gastrointestinal bleeding in COVID-19. Clin. Res. Hepatol. Gastroenterol. 2020, 44, e77–e80. [Google Scholar] [CrossRef] [PubMed]
- Dioscoridi, L.; Giannetti, A.; Massad, M.T.; Forti, E.; Pugliese, F.; Cintolo, M.; Bonato, G.; Rosa, R.; Mutignani, M. A “double-hit” damage mechanism can explain self-limited GI bleeding in COVID-19 pneumonia. Gastrointest. Endosc. 2021, 93, 1192–1193. [Google Scholar] [CrossRef]
- Mohamed, A.K.; Tang, Y.C. Demographics and characteristics of endoscopic findings among COVID-19 patients with upper gastrointestinal bleeding in a single centre. Med. J. Malays. 2023, 78, 893–896. [Google Scholar]
- Merza, N.; Masoud, A.T.; Ahmed, Z.; Dahiya, D.S.; Nawras, A.; Kobeissy, A. Trends of Upper Gastrointestinal Bleeding Mortality in the United States Before and During the COVID-19 Era: Estimates From the Centers for Disease Control WONDER Database. Gastroenterol. Res. 2023, 16, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Abowali, H.; Pacifico, A.; Erdinc, B.; Elkholy, K.; Burkhanova, U.; Aroriode, T.; Watson, A.; Ahmed, M.F.; Uwagbale, E.; Visweshwar, N.; et al. Assessment of Bleeding Risk in Hospitalized COVID-19 Patients: A Tertiary Hospital Experience during the Pandemic in a Predominant Minority Population-Bleeding Risk Factors in COVID-19 Patients. J. Clin. Med. 2022, 11, 2754. [Google Scholar] [CrossRef]
- Zellmer, S.; Hanses, F.; Muzalyova, A.; Classen, J.; Braun, G.; Piepel, C.; Erber, J.; Pilgram, L.; Walter, L.; Göpel, S.; et al. Gastrointestinal Bleeding and Endoscopic Findings in Critically and Non-Critically Ill Patients with Corona Virus Disease 2019 (COVID-19): Results from Lean European Open Survey on SARS-CoV-2 (LEOSS) and COKA Registries. United Eur. Gastroenterol. J. 2021, 9, 1081–1090. [Google Scholar] [CrossRef]
- Qiu, C.; Li, T.; Wei, G.; Xu, J.; Yu, W.; Wu, Z.; Li, D.; He, Y.; Chen, T.; Zhang, J.; et al. Hemorrhage and venous thromboembolism in critically ill patients with COVID-19. SAGE Open Med. 2021, 9, 20503121211020167. [Google Scholar] [CrossRef]
- Hibiya, S.; Fujii, T.; Fujii, T.; Suzuki, S.; Kondo, M.; Ooka, S.; Furumoto, Y.; Azuma, S.; Tanaka, K.; Kurata, H.; et al. COVID-19 severity is associated with the risk of gastrointestinal bleeding. BMJ Open Gastroenterol. 2023, 10, e001199. [Google Scholar] [CrossRef]
- Goyal, H.; Sachdeva, S.; Perisetti, A.; Mann, R.; Chandan, S.; Inamdar, S.; Tharian, B. Management of gastrointestinal bleeding during COVID-19: Less is more! Eur. J. Gastroenterol. Hepatol. 2021, 33, 1230–1232. [Google Scholar] [CrossRef]
- Tavabie, O.D.; Clough, J.N.; Blackwell, J.; Bashyam, M.; Martin, H.; Soubieres, A.; Direkze, N.; Graham, D.; Groves, C.; Preston, S.L.; et al. Reduced survival after upper gastrointestinal bleed endoscopy in the COVID-19 era is a secondary effect of the response to the global pandemic: A retrospective cohort study. Frontline Gastroenterol. 2020, 12, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Rasheed, W.; Dharmarpandi, G.; Al-Jobory, O.; Dweik, A.; Anil, M.; Islam, S. Increasing inpatient mortality of nonvariceal upper gastrointestinal bleeding during the COVID-19 pandemic: A nationwide retrospective cohort study. Bayl. Univ. Med. Cent. Proc. 2023, 36, 286–291. [Google Scholar] [CrossRef]
- Kwei-Nsoro, R.; Ojemolon, P.; Laswi, H.; Ebhohon, E.; Ufeh, A.O.; Nieto, A.; Mir, W.A.; Shaka, A.; Shaka, H. Effect of the COVID-19 pandemic on the epidemiological trends and outcomes of gastrointestinal bleeding: A nationwide study. Bayl. Univ. Med. Cent. Proc. 2023, 36, 145–150. [Google Scholar] [CrossRef]
- Han, L.; Shi, H.; Li, Y.; Qi, H.; Wang, Y.; Gu, J.; Wu, J.; Zhao, S.; Cao, P.; Xu, L.; et al. Excess Deaths of Gastrointestinal, Liver, and Pancreatic Diseases During the COVID-19 Pandemic in the United States. Int. J. Public Health 2023, 68, 1606305. [Google Scholar] [CrossRef]
- Khan, R.; Saha, S.; Gimpaya, N.; Bansal, R.; Scaffidi, M.A.; Razak, F.; Verma, A.A.; Grover, S.C. Outcomes for upper gastrointestinal bleeding during the first wave of the COVID-19 pandemic in the Toronto area. J. Gastroenterol. Hepatol. 2022, 37, 878–882. [Google Scholar] [CrossRef] [PubMed]
- Dunne, P.; Livie, V.; McGowan, A.; Siu, W.; Chaudhary, S.; Groome, M.; Phull, P.; Fraser, A.; Morris, A.J.; Penman, I.D.; et al. Increasing the low-risk threshold for patients with upper gastrointestinal bleeding during the COVID-19 pandemic: A prospective, multicentre feasibility study. Frontline Gastroenterol. 2021, 13, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Reddy, S.; Patel, B.; Baldelli, L.; Majithia, R.T.; Dougherty, M.K. Decreased Rate of Presentation, but Worsened Racial-Ethnic Disparity in Acute Gastrointestinal Bleeding During Coronavirus 2019 Shutdown: A Retrospective Cohort Study. Clin. Exp. Gastroenterol. 2022, 15, 67–77. [Google Scholar] [CrossRef]
- Sobani, Z.A.; Paleti, S.; Khalid, S.; Perez, E.T.; Rustagi, T. Trends in upper gastrointestinal bleeding during the COVID-19 pandemic. Ann. Gastroenterol. 2020, 33, 543–544. [Google Scholar] [CrossRef]
- Kim, J.; Doyle, J.B.; Blackett, J.W.; May, B.; Hur, C.; Lebwohl, B.; Faye, A.S.; Laszkowska, M.; Silver, E.R. HIRE study group. Effect of the Coronavirus 2019 Pandemic on Outcomes for Patients Admitted with Gastrointestinal Bleeding in New York City. Gastroenterology 2020, 159, 1155–1157.e1. [Google Scholar] [CrossRef]
- Mohamed, M.; Nassar, M.; Nso, N.; Alfishawy, M. Massive gastrointestinal bleeding in a patient with COVID-19. Arab. J. Gastroenterol. 2021, 22, 177–179. [Google Scholar] [CrossRef]
- Pradhan, F.; Alishahi, Y. Gastrointestinal Bleeding and Endoscopic Outcomes in Patients with SARS-CoV-2. Clin. Endosc. 2021, 54, 428–431. [Google Scholar] [CrossRef]
- Gulen, M.; Satar, S. Uncommon presentation of COVID-19: Gastrointestinal bleeding. Clin. Res. Hepatol. Gastroenterol. 2020, 44, e72–e76. [Google Scholar] [CrossRef] [PubMed]
- Papanikolaou, I.S.; Lazaridis, L.D.; Rizos, E.; Miltiadou, C.; Triantafyllou, K. Untying the knot: Acute variceal bleeding in a COVID-19 patient. What should the gastroenterologist keep in mind? Eur. J. Gastroenterol. Hepatol. 2021, 33, 450–451. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Huang, S.; Lu, J.; Lai, R.; Zhang, Z.; Lin, X.; Zheng, X.; Shan, H. Upper Gastrointestinal Bleeding Caused by SARS-CoV-2 Infection. Am. J. Gastroenterol. 2020, 115, 1541–1542. [Google Scholar] [CrossRef] [PubMed]
- Melazzini, F.; Lenti, M.V.; Mauro, A.; De Grazia, F.; Di Sabatino, A. Peptic Ulcer Disease as a Common Cause of Bleeding in Patients with Coronavirus Disease 2019. Am. J. Gastroenterol. 2020, 115, 1139–1140. [Google Scholar] [CrossRef]
- Pérez Roldán, F.; Malik Javed, Z.; Yagüe Compadre, J.L.; Navarro López, M.D.C.; Rodríguez-Bobada Caraballo, D.; Fernández Visier, I.; Burgos Andeliz, M.; González Carro, P.S. Gastric ulcers with upper gastrointestinal bleeding in patients with severe SARS-CoV-2. Rev. Esp. Enfermadades Dig. 2021, 113, 122–124. [Google Scholar] [CrossRef]
- Rehana, R.W.; Fahad, H.; Sadiq, O.; Schairer, J. Outcomes of Gastrointestinal Bleeding During the COVID-19 Pandemic. Gastro Hep Adv. 2022, 1, 342–343. [Google Scholar] [CrossRef]
- Fanning, J.P.; Weaver, N.; Fanning, R.B.; Griffee, M.J.; Cho, S.-M.; Panigada, M.; Obonyo, N.G.; Zaaqoq, A.M.; Rando, H.; Chia, Y.W.; et al. Hemorrhage, Disseminated Intravascular Coagulopathy, and Thrombosis Complications Among Critically Ill Patients with COVID-19: An International COVID-19 Critical Care Consortium Study. Crit. Care Med. 2023, 51, 619–631. [Google Scholar] [CrossRef]
- Abulawi, A.; Al-Tarbsheh, A.; Leamon, A.; Feustel, P.; Chopra, A.; Batool, A. Clinical Characteristics of Hospitalized COVID-19 Patients Who Have Gastrointestinal Bleeds Requiring Intervention: A Case-Control Study. Cureus 2022, 14, e26538. [Google Scholar] [CrossRef]
- Attah, E.; Martin, T.A.; Smith, E.S.; Tewani, S.; Hajifathalian, K.; Sharaiha, R.Z.; Crawford, C.V.; Wan, D. Observed risk of recurrent bleeding and thromboembolic disease in COVID-19 patients with gastrointestinal bleeding. Endosc. Int. Open 2021, 9, E1435–E1444. [Google Scholar] [CrossRef]
- Makker, J.; Mantri, N.; Patel, H.K.; Abbas, H.; Baiomi, A.; Sun, H.; Choi, Y.; Chilimuri, S.; Nayudu, S.K. The Incidence and Mortality Impact of Gastrointestinal Bleeding in Hospitalized COVID-19 Patients. Clin. Exp. Gastroenterol. 2021, 14, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Wiedel, N.A.; Sayles, H.; Larson, J.; Wardian, J.L.; Hewlett, A.; McClay, J.; Ge, J.; Anzalone, A.J. N3C consortium. Associations between COVID-19 therapies and inpatient gastrointestinal bleeding: A multisite retrospective study. J. Med. Virol. 2023, 95, e29100. [Google Scholar] [CrossRef]
- Holzwanger, E.A.; Bilal, M.; Stallwood, C.G.; Sterling, M.J.; Yacavone, R.F. Acute lower gastrointestinal bleeding during the COVID-19 pandemic—Less is more! Endoscopy 2020, 52, 816–817. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Tong, Z.; Ma, Z.; Luo, L.; Tang, Y.; Teng, Y.; Yu, H.; Meng, H.; Peng, C.; Zhang, Q.; et al. Gastrointestinal Bleeding, but Not Other Gastrointestinal Symptoms, Is Associated With Worse Outcomes in COVID-19 Patients. Front. Med. 2021, 8, 759152. [Google Scholar] [CrossRef] [PubMed]
- Rustgi, S.D.; Yang, J.Y.; Luther, S.; David, Y.; Dixon, R.E.; Simoes, P.K.; Kumta, N.A. Anticoagulation does not increase risk of mortality or ICU admission in hospitalized COVID-19 patients with gastrointestinal bleeding: Results from a New York health system. Clin. Res. Hepatol. Gastroenterol. 2021, 45, 101602. [Google Scholar] [CrossRef]
- Trindade, A.J.; Izard, S.; Coppa, K.; Hirsch, J.S.; Lee, C.; Satapathy, S.K. Northwell COVID-19 Research Consortium Gastrointestinal bleeding in hospitalized COVID-19 patients: A propensity score matched cohort study. J. Intern. Med. 2021, 289, 887–894. [Google Scholar] [CrossRef]
- Alkhamis, A.; Alshamali, Y.; Alyaqout, K.; Lari, E.; Alkhamis, M.A.; Althuwaini, S.; Lari, A.; Alfili, M.; Alkhayat, A.; Jamal, M.H.; et al. Prevalence, predictors and outcomes of bleeding events in patients with COVID-19 infection on anticoagulation: Retrospective cohort study. Ann. Med. Surg. 2021, 68, 102567. [Google Scholar] [CrossRef]
- Alakuş, Ü.; Kara, U.; Taşçı, C.; Eryılmaz, M. Upper gastrointestinal system bleedings in COVID-19 patients: Risk factors and management/a retrospective cohort study. Turk. J. Trauma Emerg. Surg. 2022, 28, 762–768. [Google Scholar] [CrossRef]
- Prasoppokakorn, T.; Kullavanijaya, P.; Pittayanon, R. Risk factors of active upper gastrointestinal bleeding in patients with COVID-19 infection and the effectiveness of PPI prophylaxis. BMC Gastroenterol. 2022, 22, 465. [Google Scholar] [CrossRef]
- Luu, M.N.; Dang, T.P.; Vo, M.H.; Quach, D.T. Prevalence, causes, medical interventions, and mortality outcome of acute gastrointestinal bleeding among COVID-19 inpatients. Curr. Med. Res. Opin. 2023, 39, 731–737. [Google Scholar] [CrossRef]
- Shafieipour, S.; Mohammadi, E.; Rezaei Zadeh, R.M.; Momenai, R.; Lashkarizadeh, M.; Zahedi, M.; Mahdi, M.; Abbasi, H.; Darvish-Moghadam, S.; Mehdi, S.; et al. Gastrointestinal Bleeding: Prevalence, Etiology, and Outcomes in COVID-19 Inpatients. Iran. J. Gastroenterol. Hepatol. 2023, 28, 30–35. [Google Scholar]
- Arif, F.; Kim, C.K.; Karim, K. Gastrointestinal Bleeding In Patients With COVID-19: Risk Factors And Therapeutic Outcomes. Surg. Chron. 2022, 27, 471–472. [Google Scholar]
- Mauro, A.; De Grazia, F.; Lenti, M.V.; Penagini, R.; Frego, R.; Ardizzone, S.; Savarino, E.; Radaelli, F.; Bosani, M.; Orlando, S.; et al. Upper gastrointestinal bleeding in COVID-19 inpatients: Incidence and management in a multicenter experience from Northern Italy. Clin. Res. Hepatol. Gastroenterol. 2021, 45, 101521. [Google Scholar] [CrossRef] [PubMed]
- González, R.G.; Jacob, J.; Miró, Ò.; Llorens, P.; Jiménez, S.; del Castillo, J.G.; Burillo-Putze, G.; Martín, A.; Martín-Sánchez, F.J.; Lamberechts, J.G.; et al. Incidence, Clinical Characteristics, Risk Factors, and Outcomes of Upper Gastrointestinal Bleeding in Patients With COVID-19: Results of the UMC-19-S12. J. Clin. Gastroenterol. 2022, 56, e38–e46. [Google Scholar] [CrossRef]
- Ungureanu, B.S.; Gheonea, D.I.; Florescu, D.N.; Iordache, S.; Cazacu, S.M.; Iovanescu, V.F.; Rogoveanu, I.; Turcu-Stiolica, A. Predicting mortality in patients with nonvariceal upper gastrointestinal bleeding using machine learning. Front. Med. 2023, 10, 1134835. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year, Country | Study Period (Publication Year) | Patients Bleeding Type | Control Group | Gender (%Males) | Age (Mean ± Stdev) | Endoscopy No (%) | Therapeutic Endoscopy (%) | Mortality | Rebleeding |
|---|---|---|---|---|---|---|---|---|---|
| Martin 2020 USA [20] | 4 March–23 April 2020, (2020) | 41 (31 UGIB, 10 LGIB) | COVID-19 without GIB | 27 (66%) vs. 54 (66%) | 68.7 (15.1) vs. 67.6 (14.3) | 10/31 (32%) UGIB 5/10 (50%) LGIB | 40 | 8 (26% UGIB), 2 (20% LGIB) | 4 (13%) UGIB 1 (10%) LGIB |
| Cazacu 2023, Romania [21] | March 2020–December 2021, (2023) | 39 UGIB | 459 UGIB without COVID-19 | 22/39 (56.4%) vs. 312/459 (68%) | 67.8 (12.65) vs. 63.1 (14.60) | 17/39 (43.6%) vs. 384/459 (83.7%) | 23.5 vs. 24 | 23 (59%) vs. 13.7% | 1 (2.6%) vs. 44 (7.8%) |
| Shalimar 2021, India [26] | 22 April–22 July 2020, (2021) | 24 UGIB | No control group | 17/24 (70.8%) | 45.8 (12.7) | 4% (1/24) | 100 | 3 (13%) | 2 (8.7%) |
| Rosevics 2021 Brasil [27] | March–August 2020, (2021) | 9 UGIB | COVID-19 without GIB | 5/9 (55.6) vs. 296/539 (54.9%) | 58 (10.2) vs. 57 (15.1) | 100% (9/9) | 20 | 4 (44.4%) | - |
| Iqbal 2022, USA [28] | March 2020–February 2021, (2022) | 18 GIB | 54 GIB without COVID-19 | 12 (66.7) vs. 36 (66.7) | 68.8 (13.31) vs. 70.0 (11.29) | 6/18 (33.3%) vs. 40/54 (74.1%) | 22.2 vs. 25.9 | 7 (38.9%) vs. 18.5% | 3 (16.7%) vs. 6 (11.3%) |
| Smith 2022, USA [29] | January 2020–March 2021, (2022) | 5 UGIB | 171 UGIB without COVID-19 | NA | NA | 2/5 (40%) vs. 171/171 (100%) | 100 | 2 (40%) vs. 20.47% | 1 (20%) |
| Elfert 2023, USA [30] | January–December 2020, (2024) | 3155 UGIB Non-variceal | 229790 NVUGIB without COVID-19 | 1700 (54%) vs. 126575 (55%) | 67.4 (15) vs. 66.2 (15) | 39% vs. 49% | 21 vs. 28 | 158 (5%) vs. 2% | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cazacu, S.M.; Turcu-Stiolica, A.; Marginean, C.M.; Rogoveanu, I. Increased Overall Mortality in Patients Admitted for Gastrointestinal Bleeding and COVID-19 Infection Compared to No COVID-19 Infection: A Systematic Review and Meta-Analysis. Gastroenterol. Insights 2025, 16, 20. https://doi.org/10.3390/gastroent16030020
Cazacu SM, Turcu-Stiolica A, Marginean CM, Rogoveanu I. Increased Overall Mortality in Patients Admitted for Gastrointestinal Bleeding and COVID-19 Infection Compared to No COVID-19 Infection: A Systematic Review and Meta-Analysis. Gastroenterology Insights. 2025; 16(3):20. https://doi.org/10.3390/gastroent16030020
Chicago/Turabian StyleCazacu, Sergiu Marian, Adina Turcu-Stiolica, Cristina Maria Marginean, and Ion Rogoveanu. 2025. "Increased Overall Mortality in Patients Admitted for Gastrointestinal Bleeding and COVID-19 Infection Compared to No COVID-19 Infection: A Systematic Review and Meta-Analysis" Gastroenterology Insights 16, no. 3: 20. https://doi.org/10.3390/gastroent16030020
APA StyleCazacu, S. M., Turcu-Stiolica, A., Marginean, C. M., & Rogoveanu, I. (2025). Increased Overall Mortality in Patients Admitted for Gastrointestinal Bleeding and COVID-19 Infection Compared to No COVID-19 Infection: A Systematic Review and Meta-Analysis. Gastroenterology Insights, 16(3), 20. https://doi.org/10.3390/gastroent16030020