
Pre-Procedural Predictors of Successful Endoscopic Sleeve Gastroplasty: A Retrospective Study


Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Setting
2.3. Procedure
2.4. Participants
2.4.1. Inclusion Criteria
2.4.2. Exclusion Criteria
2.5. End Points and Assessments
2.5.1. Primary End Point
2.5.2. Secondary End Points
2.6. Ethics Approval
2.7. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chooi, Y.C.; Ding, C.; Magkos, F. The epidemiology of obesity. Metab. Clin. Exp. 2019, 92, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Heymsfield, S.B.; Wadden, T.A. Mechanisms, pathophysiology, and management of obesity. N. Engl. J. Med. 2017, 376, 254–266. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M.; Hawkes, C. Sweetening of the global diet, particularly beverages: Patterns, trends, and policy responses. Lancet Diabetes Endocrinol. 2016, 4, 174–186. [Google Scholar] [CrossRef] [PubMed]
- Pigeyre, M.; Yazdi, F.T.; Kaur, Y. Recent progress in genetics, epigenetics and metagenomics unveils the pathophysiology of human obesity. Clin. Sci. 2016, 130, 943–986. [Google Scholar] [CrossRef] [PubMed]
- van der Klaauw, A.A.; Farooqi, I.S. The hunger genes: Pathways to obesity. Cell 2015, 161, 119–132. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.; Li, H. Obesity: Epidemiology, pathophysiology, and therapeutics. Front. Endocrinol. 2021, 12, 706978. [Google Scholar] [CrossRef]
- Acosta, A.; Camilleri, M.; Abu Dayyeh, B. Selection of Antiobesity Medications Based on Phenotypes Enhances Weight Loss: A Pragmatic Trial in an Obesity Clinic. Obesity 2021, 29, 662–671. [Google Scholar] [CrossRef]
- Sharaiha, R.Z.; Kumta, N.A.; Saumoy, M. Endoscopic sleeve gastroplasty significantly reduces body mass index and metabolic complications in obese patients. Clin. Gastroenterol. Hepatol. 2017, 15, 504–510. [Google Scholar] [CrossRef]
- Cheskin, L.J.; Hill, C.; Adam, A. Endoscopic sleeve gastroplasty versus high-intensity diet and lifestyle therapy: A case-matched study. Gastrointest. Endosc. 2020, 91, 342–349. [Google Scholar] [CrossRef]
- Dayyeh, B.K.A.; Acosta, A.; Camilleri, M. Endoscopic sleeve gastroplasty alters gastric physiology and induces loss of body weight in obese individuals. Clin. Gastroenterol. Hepatol. 2017, 15, 37–43. [Google Scholar] [CrossRef]
- Panel, O.E. American College of Cardiology, & American Heart Association Task Force on Practice Guidelines. Expert Panel Report: Guidelines (2013) for the management of overweight and obesity in adults. Obesity 2014, 22, S41–S410. [Google Scholar]
- Yanovski, S.Z.; Yanovski, J.A. Long-term drug treatment for obesity: A systematic and clinical review. Jama 2014, 311, 74–86. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.M.; Kushner, R.F. A proposed clinical staging system for obesity. Int. J. Obes. 2009, 33, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Nuttall, F.Q. Body mass index: Obesity, BMI, and health: A critical review. Nutr. Today 2015, 50, 117. [Google Scholar] [CrossRef] [PubMed]
- Phillips, C.M.; Dillon, C.; Harrington, J.M. Defining metabolically healthy obesity: Role of dietary and lifestyle factors. PLoS ONE 2013, 8, e76188. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Nava, G.; Sharaiha, R.Z.; Vargas, E.J. Endoscopic sleeve gastroplasty for obesity: A multicenter study of 248 patients with 24 months follow-up. Obes. Surg. 2017, 27, 2649–2655. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, A.; Al-Darwish, A.; Mahmoud, A.E. Short-term outcomes of endoscopic sleeve gastroplasty in 1000 consecutive patients. Gastrointest. Endosc. 2019, 89, 1132–1138. [Google Scholar] [CrossRef] [PubMed]
- Hedjoudje, A.; Dayyeh, B.K.A.; Cheskin, L.J. Efficacy and safety of endoscopic sleeve gastroplasty: A systematic review and meta-analysis. Clin. Gastroenterol. Hepatol. 2020, 18, 1043–1053. [Google Scholar] [CrossRef]
- Abd Ellatif, M.E.; Abdallah, E.; Askar, W. Long term predictors of success after laparoscopic sleeve gastrectomy. Int. J. Surg. 2014, 12, 504–508. [Google Scholar] [CrossRef]
- Livhits, M.; Mercado, C.; Yermilov, I. Preoperative predictors of weight loss following bariatric surgery: Systematic review. Obes. Surg. 2012, 22, 70–89. [Google Scholar] [CrossRef]
- Goldenshluger, M.; Goldenshluger, A.; Keinan-Boker, L. Postoperative outcomes, weight loss predictors, and late gastrointestinal symptoms following laparoscopic sleeve gastrectomy. J. Gastrointest. Surg. 2017, 21, 2009–2015. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Nava, G.; Galvao, M.; Bautista-Castaño, I. Endoscopic sleeve gastroplasty with 1-year follow-up: Factors predictive of success. Endosc. Int. Open 2016, 4, E222–E227. [Google Scholar] [CrossRef] [PubMed]
- Barrichello, S.; de Moura, D.T.H.; de Moura, E.G.H. Endoscopic sleeve gastroplasty in the management of overweight and obesity: An international multicenter study. Gastrointest. Endosc. 2019, 90, 770–780. [Google Scholar] [CrossRef] [PubMed]
- Tak, Y.J.; Lee, S.Y. Long-term efficacy and safety of anti-obesity treatment: Where do we stand? Curr. Obes. Rep. 2021, 10, 14–30. [Google Scholar] [CrossRef] [PubMed]
- Saumoy, M. Cost-effectiveness of endoscopic, surgical and pharmacological obesity therapies: A microsimulation and threshold analyses. Gut 2023, 72, 2250–2259. [Google Scholar] [CrossRef] [PubMed]
- Azuri, J.; Hammerman, A.; Aboalhasan, E. Liraglutide versus semaglutide for weight reduction-a cost needed to treat analysis. Obesity 2023, 31, 1510–1513. [Google Scholar] [CrossRef] [PubMed]
- Haseeb, M. Semaglutide vs Endoscopic Sleeve Gastroplasty for Weight Loss. JAMA Netw. Open 2024, 7, e246221. [Google Scholar] [CrossRef] [PubMed]
- Dolan, R.D.; Jirapinyo, P.; Thompson, C.C. Endoscopic versus surgical gastrojejunal revision for weight regain in Roux-en-Y gastric bypass patients: 5-year safety and efficacy comparison. Gastrointest. Endosc. 2021, 94, 945–950. [Google Scholar] [CrossRef]
- Acosta, A.; Camilleri, M. A working paradigm for the treatment of obesity in gastrointestinal practice. Tech. Gastrointest. Endosc. 2017, 19, 52–60. [Google Scholar] [CrossRef]
- Fayad, L. Endoscopic sleeve gastroplasty versus intragastric balloon insertion: Efficacy, durability, and safety. Endoscopy 2019, 51, 532–539. [Google Scholar] [CrossRef]
- Mohan, B.P. Current status of endoscopic sleeve gastroplasty: An opinion review. World J. Gastroenterol. 2020, 26, 1107–1112. [Google Scholar]
- Chiolero, A.; Faeh, D.; Paccaud, F. Consequences of smoking for body weight, body fat distribution, and insulin resistance. Am. J. Clin. Nutr. 2008, 87, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Matteo, M.V. Success Predictors of Endoscopic Sleeve Gastroplasty. Obes. Surg. 2024, 34, 1496–1504. [Google Scholar] [CrossRef] [PubMed]
- Lafortuna, C.L.; Maffiuletti, N.A.; Agosti, F. Gender variations of body composition, muscle strength and power output in morbid obesity. Int. J. Obes. 2005, 29, 833–841. [Google Scholar] [CrossRef]
- Blundell, J.E.; Finlayson, G. Is susceptibility to weight gain characterized by homeostatic or hedonic risk factors for overconsumption? Physiol. Behav. 2004, 82, 21–25. [Google Scholar] [CrossRef]
- Avena, N. Hedonic Eating: How the Pleasure of Food Affects Our Brains and Behavior; Oxford University Press: Oxford, UK, 2015. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Number of Patients (N = 76) | Successful ESG Mean (SD) | ESG Failure Mean (SD) | p-Value * |
|---|---|---|---|---|
| Age | 46.6 (10.1) | 45.9 (10.9) | 0.802 | |
| Gender (female) | 62 | 19 | 43 | 0.216 |
| Gender (male) | 14 | 2 | 12 | |
| Hypertension | 9 | 3 | 6 | 0.684 |
| Diabetes mellitus | 8 | 3 | 5 | 0.509 |
| Smoking | 7 | 6 | 1 | <0.001 |
| Ischemic heart disease | 1 | 0 | 1 | 0.534 |
| Non-alcoholic fatty liver disease | 26 | 7 | 19 | 0.921 |
| HDL | 76 | 48.8 (13.7) | 49.7 (12.1) | 0.784 |
| Triglycerides | 76 | 121.5 (38.6) | 133 (70.8) | 0.483 |
| Creatinine | 76 | 0.7 (0.1) | 0.9 (1.6) | 0.566 |
| AST | 76 | 26.8 (13.8) | 23.1 (10.4) | 0.949 |
| ALT | 76 | 23.3 (12.5) | 23.5 (13.8) | 0.949 |
| ALK-P | 72 | 90.5 (28.6) | 84.6 (27.1) | 0.414 |
| GGT | 57 | 27.4 (18.6) | 23.5 (14.8) | 0.411 |
| A1C | 65 | 5.8 (0.8) | 5.6 (0.6) | 0.234 |
| TSH | 68 | 2.3 (1.5) | 2.3 (1.4) | 0.837 |
| Cholesterol | 75 | 182.2 (40.5) | 177.9 (35.6) | 0.651 |
| LDL | 73 | 108 (34.4) | 96.8 (30.6) | 0.184 |
| Folic acid | 58 | 19.9 (11.2) | 17.5 (10.0) | 0.439 |
| Vitamin B12 | 69 | 380.7 (274.9) | 324.8 (156.7) | 0.285 |
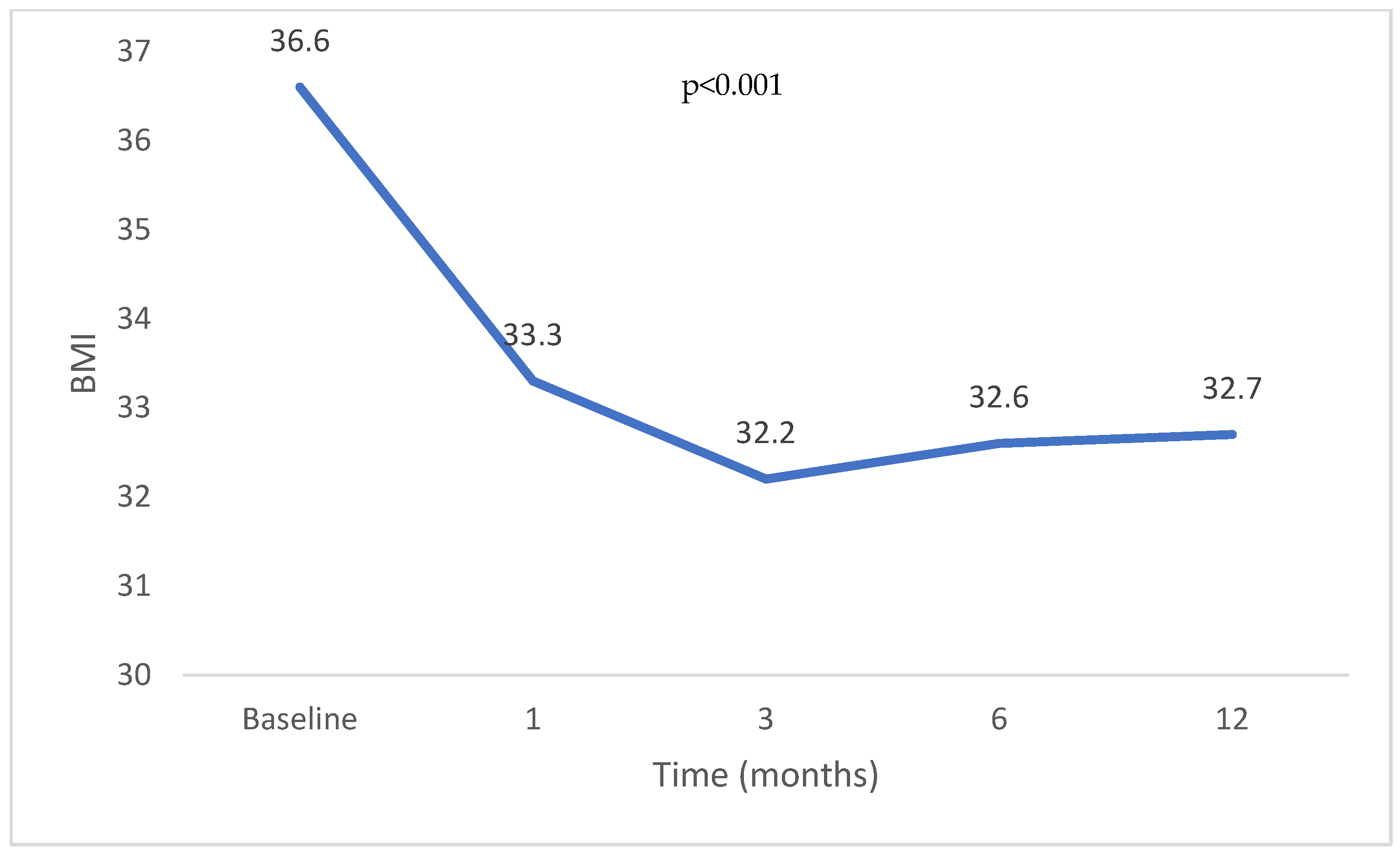
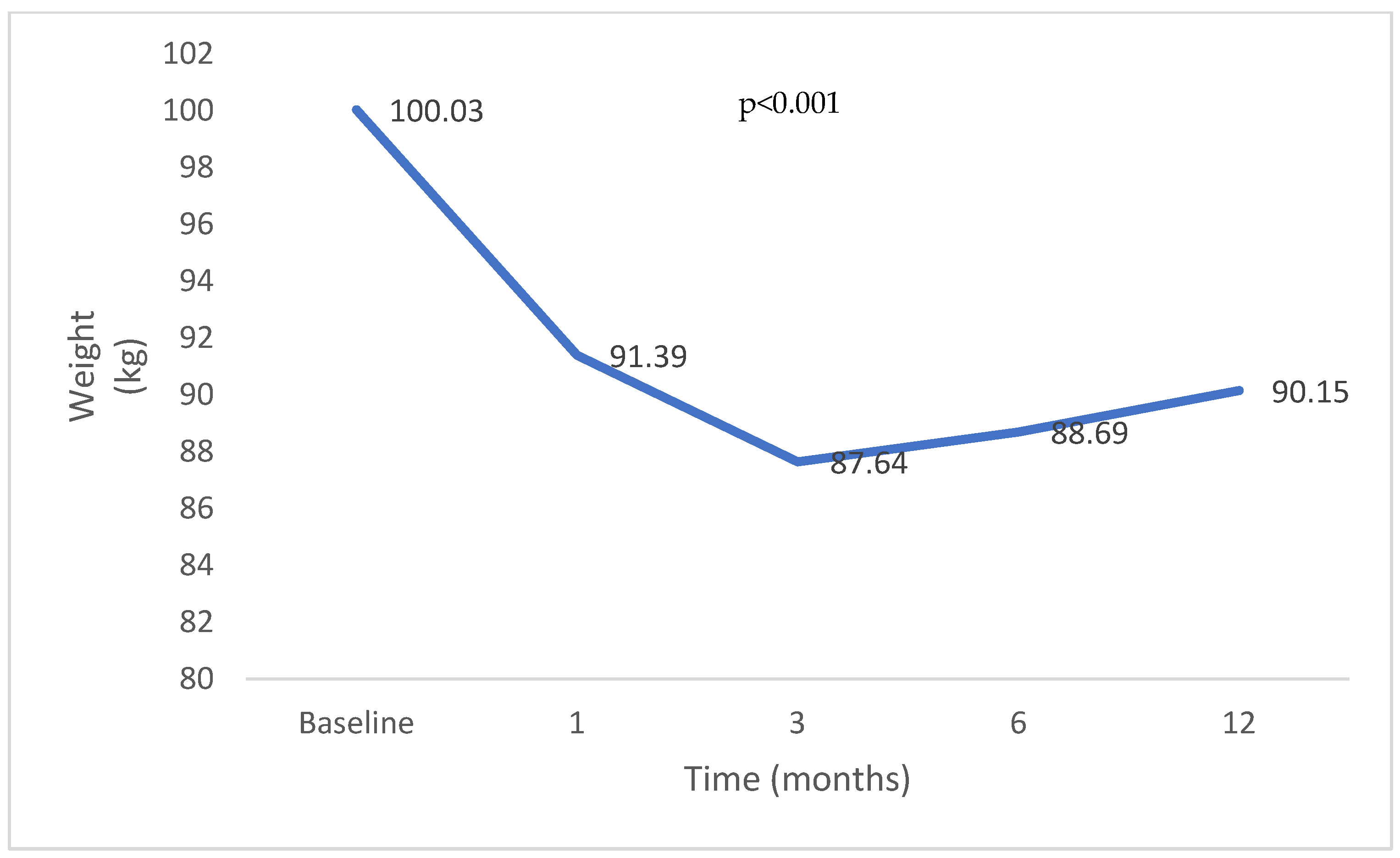
| Total Body Weight | Total Body Weight Loss (%) | BMI | BMI Change (%) | |
|---|---|---|---|---|
| Baseline (n = 76) | 100 | 36.6 | ||
| 1 months (n = 69) | 91.4 | 8.6% | 33.3 | 9.0% |
| 3 months (n = 48) | 87.7 | 12.3% | 32.1 | 12.1% |
| 6 months (n = 33) | 88.7 | 11.3% | 32.5 | 11.0% |
| 12 months (n = 13) | 90.2 | 9.8% | 32.6 | 10.7% |
| Variable | Odds Ratio (95% CI) |
|---|---|
| NAFLD | 0.69 (0.14–3.38) |
| smoking | 41.48 (2.17–794.19) |
| DM | 20.89 (0.89–492.37) |
| HTN | 0.52 (0.03–8.5) |
| Arab (vs. Jewish) | 0.18 (0.02–1.76) |
| Female | 15.12 (0.55–419.13) |
| Age | 1.03 (0.96–1.1) |
| BMI before procedure | 1.18 (0.97–1.43) |
| Triglycerides | 1 (0.98–1.02) |
| cholesterol | 0.97 (0.89–1.06) |
| HDL | 0.99 (0.89–1.1) |
| LDL | 1.03 (0.95–1.12) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Charach, L.; Peleg, N.; Abuhasira, R.; Shamah, S. Pre-Procedural Predictors of Successful Endoscopic Sleeve Gastroplasty: A Retrospective Study. Gastroenterol. Insights 2024, 15, 459-470. https://doi.org/10.3390/gastroent15020033
Charach L, Peleg N, Abuhasira R, Shamah S. Pre-Procedural Predictors of Successful Endoscopic Sleeve Gastroplasty: A Retrospective Study. Gastroenterology Insights. 2024; 15(2):459-470. https://doi.org/10.3390/gastroent15020033
Chicago/Turabian StyleCharach, Lior, Noam Peleg, Ran Abuhasira, and Steven Shamah. 2024. "Pre-Procedural Predictors of Successful Endoscopic Sleeve Gastroplasty: A Retrospective Study" Gastroenterology Insights 15, no. 2: 459-470. https://doi.org/10.3390/gastroent15020033
APA StyleCharach, L., Peleg, N., Abuhasira, R., & Shamah, S. (2024). Pre-Procedural Predictors of Successful Endoscopic Sleeve Gastroplasty: A Retrospective Study. Gastroenterology Insights, 15(2), 459-470. https://doi.org/10.3390/gastroent15020033