

Assessment of Cognitive Function in Romanian Patients with Chronic Alcohol Consumption


 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Selection of Patients
2.2. Clinical Evaluation
2.3. Definition of NAFLD and Ultrasound Assessment
2.4. Biological Analyses
2.5. Treatments
2.6. Statistical Analysis
3. Results
- 20 to 29 years: 5 patients (5.6%);
- 30 to 39 years: 17 patients (18.9%);
- 40 to 49 years: 25 patients (27.8%);
- 50 to 59 years: 30 patients (33.3%);
- 60 to 69 years: 10 patients (11.1%);
- 70 to 79 years: 3 patients (3.3%).
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ilhan, M.N.; Yapar, D. Alcohol Consumption and Alcohol Policy. Turk. J. Med. Sci. 2020, 50, 1197–1202. [Google Scholar] [CrossRef]
- Ritchie, H.; Roser, M. Alcohol Consumption. 2023. Available online: https://ourworldindata.org/alcohol-consumption (accessed on 16 February 2024).
- Fama, R. Alcohol’s Unique Effects on Cognition in Women: A 2020 (Re)View to Envision Future Research and Treatment. Alcohol Res. 2020, 40, 3. [Google Scholar] [CrossRef] [PubMed]
- Griswold, M.G.; Fullman, N.; Hawley, C.; Arian, N.; Zimsen, S.R.M.; Tymeson, H.D.; Venkateswaran, V.; Tapp, A.D.; Forouzanfar, M.H.; Salama, J.S.; et al. Alcohol Use and Burden for 195 Countries and Territories, 1990–2016: A Systematic Analysis for the Global Burden of Disease Study 2016. Lancet 2018, 392, 1015–1035. [Google Scholar] [CrossRef]
- Eurostat Alcohol Consumption Statistics, 2021. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Alcohol_consumption_statistics#Frequency_of_alcohol_consumption (accessed on 15 February 2024).
- Pelletier, S.; Nalpas, B.; Alarcon, R.; Rigole, H.; Perney, P. Investigation of Cognitive Improvement in Alcohol-Dependent Inpatients Using the Montreal Cognitive Assessment (MoCA) Score. J. Addict. 2016, 2016, 1539096. [Google Scholar] [CrossRef]
- Bernardin, F.; Maheut-Bosser, A.; Paille, F. Cognitive Impairments in Alcohol-Dependent Subjects. Front. Psychiatry 2014, 5, 78. [Google Scholar] [CrossRef] [PubMed]
- Ihara, H. Group and Case Study of the Dysexecutive Syndrome in Alcoholism without Amnesia. J. Neurol. Neurosurg. Psychiatry 2000, 68, 731–737. [Google Scholar] [CrossRef]
- Green, A.; Garrick, T.; Sheedy, D.; Blake, H.; Shores, E.A.; Harper, C. The Effect of Moderate to Heavy Alcohol Consumption on Neuropsychological Performance as Measured by the Repeatable Battery for the Assessment of Neuropsychological Status. Alcohol. Clin. Exp. Res. 2010, 34, 443–450. [Google Scholar] [CrossRef] [PubMed]
- Sterling, S.A.; Palzes, V.A.; Lu, Y.; Kline-Simon, A.H.; Parthasarathy, S.; Ross, T.; Elson, J.; Weisner, C.; Maxim, C.; Chi, F.W. Associations Between Medical Conditions and Alcohol Consumption Levels in an Adult Primary Care Population. JAMA Netw. Open 2020, 3, e204687. [Google Scholar] [CrossRef]
- Bruijnen, C.J.W.H.; Dijkstra, B.A.G.; Walvoort, S.J.W.; Markus, W.; VanDerNagel, J.E.L.; Kessels, R.P.C.; DE Jong, C.A.J. Prevalence of Cognitive Impairment in Patients with Substance Use Disorder. Drug Alcohol Rev. 2019, 38, 435–442. [Google Scholar] [CrossRef]
- Stavro, K.; Pelletier, J.; Potvin, S. Widespread and Sustained Cognitive Deficits in Alcoholism: A Meta-analysis. Addict. Biol. 2013, 18, 203–213. [Google Scholar] [CrossRef] [PubMed]
- Schulte, T.; Oberlin, B.G.; Kareken, D.A.; Marinkovic, K.; Müller-Oehring, E.M.; Meyerhoff, D.J.; Tapert, S. How Acute and Chronic Alcohol Consumption Affects Brain Networks: Insights from Multimodal Neuroimaging. Alcohol. Clin. Exp. Res. 2012, 36, 2017–2027. [Google Scholar] [CrossRef] [PubMed]
- Janke van Holst, R.; Schilt, T. Drug-Related Decrease in Neuropsychological Functions of Abstinent Drug Users. Curr. Drug Abus. Rev. 2011, 4, 42–56. [Google Scholar] [CrossRef] [PubMed]
- Loeber, S.; Duka, T.; Welzel Marquez, H.; Nakovics, H.; Heinz, A.; Mann, K.; Flor, H. Effects of Repeated Withdrawal from Alcohol on Recovery of Cognitive Impairment under Abstinence and Rate of Relapse. Alcohol Alcohol. 2010, 45, 541–547. [Google Scholar] [CrossRef]
- Fein, G.; McGillivray, S. Cognitive Performance in Long-Term Abstinent Elderly Alcoholics. Alcohol. Clin. Exp. Res. 2007, 31, 1788–1799. [Google Scholar] [CrossRef] [PubMed]
- Kish, G.B.; Hagen, J.M.; Woody, M.M.; Harvey, H.L. Alcoholics’ Recovery from Cerebral Impairment as a Function of Duration of Abstinence. J. Clin. Psychol. 1980, 36, 584–589. [Google Scholar] [CrossRef] [PubMed]
- Yohman, J.R.; Parsons, O.A.; Leber, W.R. Lack of Recovery in Male Alcoholics’ Neuropsychological Performance One Year after Treatment. Alcohol. Clin. Exp. Res. 1985, 9, 114–117. [Google Scholar] [CrossRef] [PubMed]
- Day, E.; Daly, C. Clinical Management of the Alcohol Withdrawal Syndrome. Addiction 2022, 117, 804–814. [Google Scholar] [CrossRef] [PubMed]
- Jesse, S.; Bråthen, G.; Ferrara, M.; Keindl, M.; Ben-Menachem, E.; Tanasescu, R.; Brodtkorb, E.; Hillbom, M.; Leone, M.A.; Ludolph, A.C. Alcohol Withdrawal Syndrome: Mechanisms, Manifestations, and Management. Acta Neurol. Scand. 2017, 135, 4–16. [Google Scholar] [CrossRef] [PubMed]
- Băloşeanu, C.L.; Streba, C.T.; Vere, C.C.; Comănescu, V.; Rogoveanu, I. Association between Liver Histology, Carotid Ultrasonography and Retinal Vascular Changes in Patients with Nonalcoholic Fatty Liver Disease (NAFLD). Rom. J. Morphol. Embryol. 2012, 53, 609–614. [Google Scholar]
- Stepan, M.D.; Vintilescu, Ș.B.; Streață, I.; Podeanu, M.A.; Florescu, D.N. The Role of Vitamin D in Obese Children with Non-Alcoholic Fatty Liver Disease and Associated Metabolic Syndrome. Nutrients 2023, 15, 2113. [Google Scholar] [CrossRef]
- Kim, D.; Cholankeril, G.; Loomba, R.; Ahmed, A. Prevalence of Fatty Liver Disease and Fibrosis Detected by Transient Elastography in Adults in the United States, 2017–2018. Clin. Gastroenterol. Hepatol. 2021, 19, 1499–1501.e2. [Google Scholar] [CrossRef] [PubMed]
- Kjærgaard, K.; Mikkelsen, A.C.D.; Wernberg, C.W.; Grønkjær, L.L.; Eriksen, P.L.; Damholdt, M.F.; Mookerjee, R.P.; Vilstrup, H.; Lauridsen, M.M.; Thomsen, K.L. Cognitive Dysfunction in Non-Alcoholic Fatty Liver Disease—Current Knowledge, Mechanisms and Perspectives. J. Clin. Med. 2021, 10, 673. [Google Scholar] [CrossRef]
- Weinstein, A.A.; de Avila, L.; Paik, J.; Golabi, P.; Escheik, C.; Gerber, L.; Younossi, Z.M. Cognitive Performance in Individuals with Non-Alcoholic Fatty Liver Disease and/or Type 2 Diabetes Mellitus. Psychosomatics 2018, 59, 567–574. [Google Scholar] [CrossRef] [PubMed]
- George, E.S.; Sood, S.; Daly, R.M.; Tan, S.-Y. Is There an Association between Non-Alcoholic Fatty Liver Disease and Cognitive Function? A Systematic Review. BMC Geriatr. 2022, 22, 47. [Google Scholar] [CrossRef] [PubMed]
- Eslam, M.; Newsome, P.N.; Sarin, S.K.; Anstee, Q.M.; Targher, G.; Romero-Gomez, M.; Zelber-Sagi, S.; Wai-Sun Wong, V.; Dufour, J.-F.; Schattenberg, J.M.; et al. A New Definition for Metabolic Dysfunction-Associated Fatty Liver Disease: An International Expert Consensus Statement. J. Hepatol. 2020, 73, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Boccatonda, A.; Andreetto, L.; D’Ardes, D.; Cocco, G.; Rossi, I.; Vicari, S.; Schiavone, C.; Cipollone, F.; Guagnano, M.T. From NAFLD to MAFLD: Definition, Pathophysiological Basis and Cardiovascular Implications. Biomedicines 2023, 11, 883. [Google Scholar] [CrossRef]
- Peng, H.; Pan, L.; Ran, S.; Wang, M.; Huang, S.; Zhao, M.; Cao, Z.; Yao, Z.; Xu, L.; Yang, Q.; et al. Prediction of MAFLD and NAFLD Using Different Screening Indexes: A Cross-Sectional Study in U.S. Adults. Front. Endocrinol. 2023, 14, 1083032. [Google Scholar] [CrossRef] [PubMed]
- Patten, S.B.; Fick, G.H. Clinical Interpretation of the Mini-Mental State. Gen. Hosp. Psychiatry 1993, 15, 254–259. [Google Scholar] [CrossRef]
- Gluhm, S.; Goldstein, J.; Loc, K.; Colt, A.; Liew, C.; Van Corey-Bloom, J. Cognitive Performance on the Mini-Mental State Examination and the Montreal Cognitive Assessment Across the Healthy Adult Lifespan. Cogn. Behav. Neurol. 2013, 26, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Anandan, P.; Rengarajan, S.; Venkatachalam, S.; Pattabi, S.; Jones, S.; Prabhu, K.; Krishna, V.; Prasanth, K. Neuroprotection by Cerebrolysin and Citicoline Through the Upregulation of Brain-Derived Neurotrophic Factor (BDNF) Expression in the Affected Neural Cells: A Preliminary Clue Obtained through an In Vitro Study. Cureus 2024, 16, e54665. [Google Scholar] [CrossRef]
- Jarosz, K.; Kojder, K.; Skonieczna-Żydecka, K.; Andrzejewska, A.; Sołek-Pastuszka, J.; Jurczak, A. The Effects of Neuromonitoring and Cerebrolysin Administration on Outcomes in Patients with Traumatic Brain Injury-An Interventional Pilot Study. J. Clin. Med. 2024, 13, 353. [Google Scholar] [CrossRef]
- Kang, D.H.; Choi, B.Y.; Lee, S.H.; Kho, A.R.; Jeong, J.H.; Hong, D.K.; Kang, B.S.; Park, M.K.; Song, H.K.; Choi, H.C.; et al. Effects of Cerebrolysin on Hippocampal Neuronal Death After Pilocarpine-Induced Seizure. Front. Neurosci. 2020, 14, 568813. [Google Scholar] [CrossRef] [PubMed]
- Morega, S.; Gresita, A.; Mitran, S.I.; Musat, M.I.; Boboc, I.K.S.; Gheorman, V.; Udristoiu, I.; Albu, C.V.; Streba, C.T.; Catalin, B.; et al. Cerebrolysin Use in Patients with Liver Damage—A Translational Study. Life 2022, 12, 1791. [Google Scholar] [CrossRef] [PubMed]
- Ziganshina, L.E.; Abakumova, T.; Nurkhametova, D.; Ivanchenko, K. Cerebrolysin for Acute Ischaemic Stroke. Cochrane Database Syst. Rev. 2023, 10, CD007026. [Google Scholar] [CrossRef] [PubMed]
- Soto, C.; Salinas, P.; Muñoz, D.; Olivares, S.; González, J.; Sáez, V.; Romero, V. A Retrospective Study of Cerebrolysin in Patients with Moderate to Severe Traumatic Brain Injury: Cognitive and Functional Outcomes. J. Med. Life 2023, 16, 1017–1021. [Google Scholar] [CrossRef]
- Chen, H.; Zhao, M.; Lin, L.; Wang, J.; Sun-Waterhouse, D.; Dong, Y.; Zhuang, M.; Su, G. Identification of Antioxidative Peptides from Defatted Walnut Meal Hydrolysate with Potential for Improving Learning and Memory. Food Res. Int. 2015, 78, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Vaghef, L.; Farajdokht, F.; Erfani, M.; Majdi, A.; Sadigh-Eteghad, S.; Karimi, P.; Sandoghchian Shotorbani, S.; Seyedi Vafaee, M.; Mahmoudi, J. Cerebrolysin Attenuates Ethanol-Induced Spatial Memory Impairments through Inhibition of Hippocampal Oxidative Stress and Apoptotic Cell Death in Rats. Alcohol 2019, 79, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Tuttolomondo, A.; Petta, S.; Casuccio, A.; Maida, C.; Corte, V.D.; Daidone, M.; Di Raimondo, D.; Pecoraro, R.; Fonte, R.; Cirrincione, A.; et al. Reactive Hyperemia Index (RHI) and Cognitive Performance Indexes Are Associated with Histologic Markers of Liver Disease in Subjects with Non-Alcoholic Fatty Liver Disease (NAFLD): A Case Control Study. Cardiovasc. Diabetol. 2018, 17, 28. [Google Scholar] [CrossRef]
- Crum, R.M.; Anthony, J.C.; Bassett, S.S.; Folstein, M.F. Population-Based Norms for the Mini-Mental State Examination by Age and Educational Level. JAMA 1993, 269, 2386–2391. [Google Scholar] [CrossRef] [PubMed]
- Cobb, J.L.; D’Agostino, R.B.; Wolf, P.A. Norms for the Mini-Mental State Examination. JAMA 1993, 270, 2178. [Google Scholar]
- Ghai, P.; Magan, D.; Aneja, J.; Sharma, H.; Choudhary, A. Effect of Alcohol-Dependence on Cognitive Performance in Middle-Aged Men: Preliminary Results. Indian. J. Physiol. Pharmacol. 2023, 67, 303–309. [Google Scholar] [CrossRef]
- Perneczky, R.; Wagenpfeil, S.; Komossa, K.; Grimmer, T.; Diehl, J.; Kurz, A. Mapping Scores Onto Stages: Mini-Mental State Examination and Clinical Dementia Rating. Am. J. Geriatr. Psychiatry 2006, 14, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Tao, X.; Zeng, M.; Mi, Y.; Xu, L. Clinical and Histological Features under Different Nomenclatures of Fatty Liver Disease: NAFLD, MAFLD, MASLD and MetALD. J. Hepatol. 2024, 80, e64–e66. [Google Scholar] [CrossRef] [PubMed]
- Morega, S.; Cătălin, B.; Simionescu, C.E.; Sapalidis, K.; Rogoveanu, I. Cerebrolysin Prevents Brain Injury in a Mouse Model of Liver Damage. Brain Sci. 2021, 11, 1622. [Google Scholar] [CrossRef] [PubMed]
- Morris, H.; Larsen, J.; Catterall, E.; Moss, A.C.; Dombrowski, S.U. Peer Pressure and Alcohol Consumption in Adults Living in the UK: A Systematic Qualitative Review. BMC Public Health 2020, 20, 1014. [Google Scholar] [CrossRef] [PubMed]
- Mahalik, J.R.; Locke, B.D.; Ludlow, L.H.; Diemer, M.A.; Scott, R.P.J.; Gottfried, M.; Freitas, G. Development of the Conformity to Masculine Norms Inventory. Psychol. Men. Masc. 2003, 4, 3–25. [Google Scholar] [CrossRef]
- White, A. Gender Differences in the Epidemiology of Alcohol Use and Related Harms in the United States. Alcohol Res. 2020, 40, 1. [Google Scholar] [CrossRef] [PubMed]
- Goh, C.M.J.; Asharani, P.V.; Abdin, E.; Shahwan, S.; Zhang, Y.; Sambasivam, R.; Vaingankar, J.A.; Ma, S.; Chong, S.A.; Subramaniam, M. Gender Differences in Alcohol Use: A Nationwide Study in a Multiethnic Population. Int. J. Ment. Health Addict. 2022. [Google Scholar] [CrossRef]
- Nasui, B.A.; Popa, M.; Buzoianu, A.D.; Pop, A.L.; Varlas, V.N.; Armean, S.M.; Popescu, C.A. Alcohol Consumption and Behavioral Consequences in Romanian Medical University Students. Int. J. Environ. Res. Public. Health 2021, 18, 7531. [Google Scholar] [CrossRef] [PubMed]
- Watfa, G.; Husson, N.; Buatois, S.; Laurain, M.C.; Miget, P.; Benetos, A. Study of Mini-Mental State Exam Evolution in Community-Dwelling Subjects Aged over 60 Years without Dementia. J. Nutr. Health Aging 2011, 15, 901–904. [Google Scholar] [CrossRef] [PubMed]
- Jastrzębska, I.; Zwolak, A.; Szczyrek, M.; Wawryniuk, A.; Skrzydło-Radomańska, B.; Daniluk, J. Biomarkers of Alcohol Misuse: Recent Advances and Future Prospects. Prz. Gastroenterol. 2016, 11, 78–89. [Google Scholar] [CrossRef]
- Tynjälä, J.; Kangastupa, P.; Laatikainen, T.; Aalto, M.; Niemelä, O. Effect of Age and Gender on the Relationship between Alcohol Consumption and Serum GGT: Time to Recalibrate Goals for Normal Ranges. Alcohol. Alcohol. 2012, 47, 558–562. [Google Scholar] [CrossRef] [PubMed]
- Sueyoshi, S.; Sawai, S.; Satoh, M.; Seimiya, M.; Sogawa, K.; Fukumura, A.; Tsutsumi, M.; Nomura, F. Fractionation of Gamma-Glutamyltransferase in Patients with Nonalcoholic Fatty Liver Disease and Alcoholic Liver Disease. World J. Hepatol. 2016, 8, 1610. [Google Scholar] [CrossRef]
- Pipitone, R.M.; Ciccioli, C.; Infantino, G.; La Mantia, C.; Parisi, S.; Tulone, A.; Pennisi, G.; Grimaudo, S.; Petta, S. MAFLD: A Multisystem Disease. Ther. Adv. Endocrinol. Metab. 2023, 14, 204201882211455. [Google Scholar] [CrossRef] [PubMed]
- Yu, Q.; He, R.; Jiang, H.; Wu, J.; Xi, Z.; He, K.; Liu, Y.; Zhou, T.; Feng, M.; Wan, P.; et al. Association between Metabolic Dysfunction-Associated Fatty Liver Disease and Cognitive Impairment. J. Clin. Transl. Hepatol. 2022, 10, 1034. [Google Scholar] [CrossRef] [PubMed]
- Jalili, V.; Poorahmadi, Z.; Hasanpour Ardekanizadeh, N.; Gholamalizadeh, M.; Ajami, M.; Houshiarrad, A.; Hajipour, A.; Shafie, F.; Alizadeh, A.; Mokhtari, Z.; et al. The Association between Obesity with Serum Levels of Liver Enzymes, Alanine Aminotransferase, Aspartate Aminotransferase, Alkaline Phosphatase and Gamma-glutamyl Transferase in Adult Women. Endocrinol. Diabetes Metab. 2022, 5, e367. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-H.; Chan, C.; Lee, H.-W.; Huang, C.; Chen, Y.-J.; Liu, P.-C.; Lu, S.-N.; Chuang, W.-L.; Huang, J.-F.; Yu, M.-L.; et al. Influence of Nonalcoholic Fatty Liver Disease with Increased Liver Enzyme Levels on the Risk of Cirrhosis and Hepatocellular Carcinoma. Clin. Gastroenterol. Hepatol. 2023, 21, 960–969.e1. [Google Scholar] [CrossRef]
- Fujii, H.; Doi, H.; Ko, T.; Fukuma, T.; Kadono, T.; Asaeda, K.; Kobayashi, R.; Nakano, T.; Doi, T.; Nakatsugawa, Y.; et al. Frequently Abnormal Serum Gamma-Glutamyl Transferase Activity Is Associated with Future Development of Fatty Liver: A Retrospective Cohort Study. BMC Gastroenterol. 2020, 20, 217. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Ma, X.; Jiang, Z.; Zhang, K.; Zhang, M.; Li, Y.; Zhao, X.; Xiong, H. Liver Enzymes and Metabolic Syndrome: A Large-Scale Case-Control Study. Oncotarget 2015, 6, 26782–26788. [Google Scholar] [CrossRef] [PubMed]
- Alatalo, P.; Koivisto, H.; Puukka, K.; Hietala, J.; Anttila, P.; Bloigu, R.; Niemela, O. Biomarkers of Liver Status in Heavy Drinkers, Moderate Drinkers and Abstainers. Alcohol Alcohol. 2009, 44, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Jia, W.; Wang, H.; Li, C.; Shi, J.; Yong, F.; Jia, H. Association between Dietary Vitamin B1 Intake and Cognitive Function among Older Adults: A Cross-Sectional Study. J. Transl. Med. 2024, 22, 165. [Google Scholar] [CrossRef] [PubMed]
- Hanna, M.; Jaqua, E.; Nguyen, V.; Clay, J. B Vitamins: Functions and Uses in Medicine. Perm. J. 2022, 26, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.H.; Lee, J.; Shin, Y.-I.; Ko, M.-H.; Kim, D.Y.; Sohn, M.K.; Kim, J.; Kim, Y.-H. Cerebrolysin Combined with Rehabilitation Enhances Motor Recovery and Prevents Neural Network Degeneration in Ischemic Stroke Patients with Severe Motor Deficits. J. Pers. Med. 2021, 11, 545. [Google Scholar] [CrossRef] [PubMed]
- Roschel, H.; Gualano, B.; Ostojic, S.M.; Rawson, E.S. Creatine Supplementation and Brain Health. Nutrients 2021, 13, 586. [Google Scholar] [CrossRef]
- Godwin Elechi, J.O.; Abrego Guandique, D.M.; Cannataro, R. Creatine in Cognitive Performance: A Commentary. Curr. Mol. Pharmacol. 2024, 17, e18761429272915. [Google Scholar] [CrossRef] [PubMed]
- Lowe, M.T.; Kim, E.H.; Faull, R.L.; Christie, D.L.; Waldvogel, H.J. Dissociated Expression of Mitochondrial and Cytosolic Creatine Kinases in the Human Brain: A New Perspective on the Role of Creatine in Brain Energy Metabolism. J. Cereb. Blood Flow. Metab. 2013, 33, 1295–1306. [Google Scholar] [CrossRef] [PubMed]
- Abrego-Guandique, D.M.; Bonet, M.L.; Caroleo, M.C.; Cannataro, R.; Tucci, P.; Ribot, J.; Cione, E. The Effect of Beta-Carotene on Cognitive Function: A Systematic Review. Brain Sci. 2023, 13, 1468. [Google Scholar] [CrossRef] [PubMed]
- Lenka, A.; Jankovic, J. Tremor Syndromes: An Updated Review. Front. Neurol. 2021, 12, 684835. [Google Scholar] [CrossRef] [PubMed]
- Canver, B.R.; Newman, R.K.; Gomez, A.E. Alcohol Withdrawal Syndrome. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. Available online: https://www.ncbi.nlm.nih.gov/books/NBK441882/ (accessed on 15 March 2024).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | AWS | NAFLD | ||
|---|---|---|---|---|
| Patients | 120 | 90 | 30 | |
| Age (years) * | 51.12 ± 13.303 | 47.49 ± 11.762 | 62 ± 11.756 | |
| Hospitalization period (days) * | - | 20.44 ± 14.59 | 1.8 ± 0.95 | |
| Gender | Male | 89 | 75 | 14 |
| Female | 31 | 15 | 16 | |
| Alcohol consumers | Yes | 90 | 90 | 0 |
| No | 30 | 0 | 30 | |
| Environment | Rural | 68 | 57 | 11 |
| Urban | 52 | 33 | 19 | |
| Total | Minimum | Maximum | Mean ± SD | |
|---|---|---|---|---|
| AST (U/L) | 90 | 22 | 919 | 127.73 ± 118.879 |
| ALT (U/L) | 90 | 16 | 1924 | 115.93 ± 207.302 |
| GGT (U/L) | 90 | 18 | 1680 | 261.23 ± 262.799 |
| MMSE at admission | 90 | 7 | 29 | 16.60 ± 4.097 |
| MMSE at 2 weeks | 90 | 17 | 30 | 24.60 ± 2.832 |
| Total | Minimum | Maximum | Mean ± SD | |
|---|---|---|---|---|
| AST (U/L) | 30 | 17 | 235 | 46.17 ± 44.135 |
| ALT (U/L) | 30 | 13 | 212 | 51.07 ± 53.067 |
| GGT (U/L) | 30 | 9 | 259 | 60.43 ± 61.525 |
| MMSE at admission | 30 | 28 | 30 | 29.27 ± 0.785 |
| Mean | SD | Std. Error | Minimum | Maximum | ||
|---|---|---|---|---|---|---|
| MMSE t0 | 20–29 | 15.60 | 5.079 | 2.272 | 9 | 22 |
| 30–39 | 18.06 | 5.517 | 1.338 | 7 | 29 | |
| 40–49 | 16.36 | 3.315 | 0.663 | 9 | 23 | |
| 50–59 | 16.40 | 3.519 | 0.643 | 11 | 29 | |
| 60–69 | 16.80 | 4.492 | 1.420 | 8 | 25 | |
| 70–79 | 14.00 | 2.000 | 1.155 | 12 | 16 | |
| Total | 16.62 | 4.060 | 0.428 | 7 | 29 | |
| MMSE t2 weeks | 20–29 | 23.60 | 4.669 | 2.088 | 17 | 29 |
| 30–39 | 24.94 | 3.230 | 0.783 | 18 | 29 | |
| 40–49 | 24.52 | 2.859 | 0.572 | 19 | 29 | |
| 50–59 | 24.43 | 2.344 | 0.428 | 20 | 29 | |
| 60–69 | 25.60 | 2.836 | 0.897 | 19 | 30 | |
| 70–79 | 23.33 | 2.082 | 1.202 | 21 | 25 | |
| Total | 24.60 | 2.832 | 0.298 | 17 | 30 | |
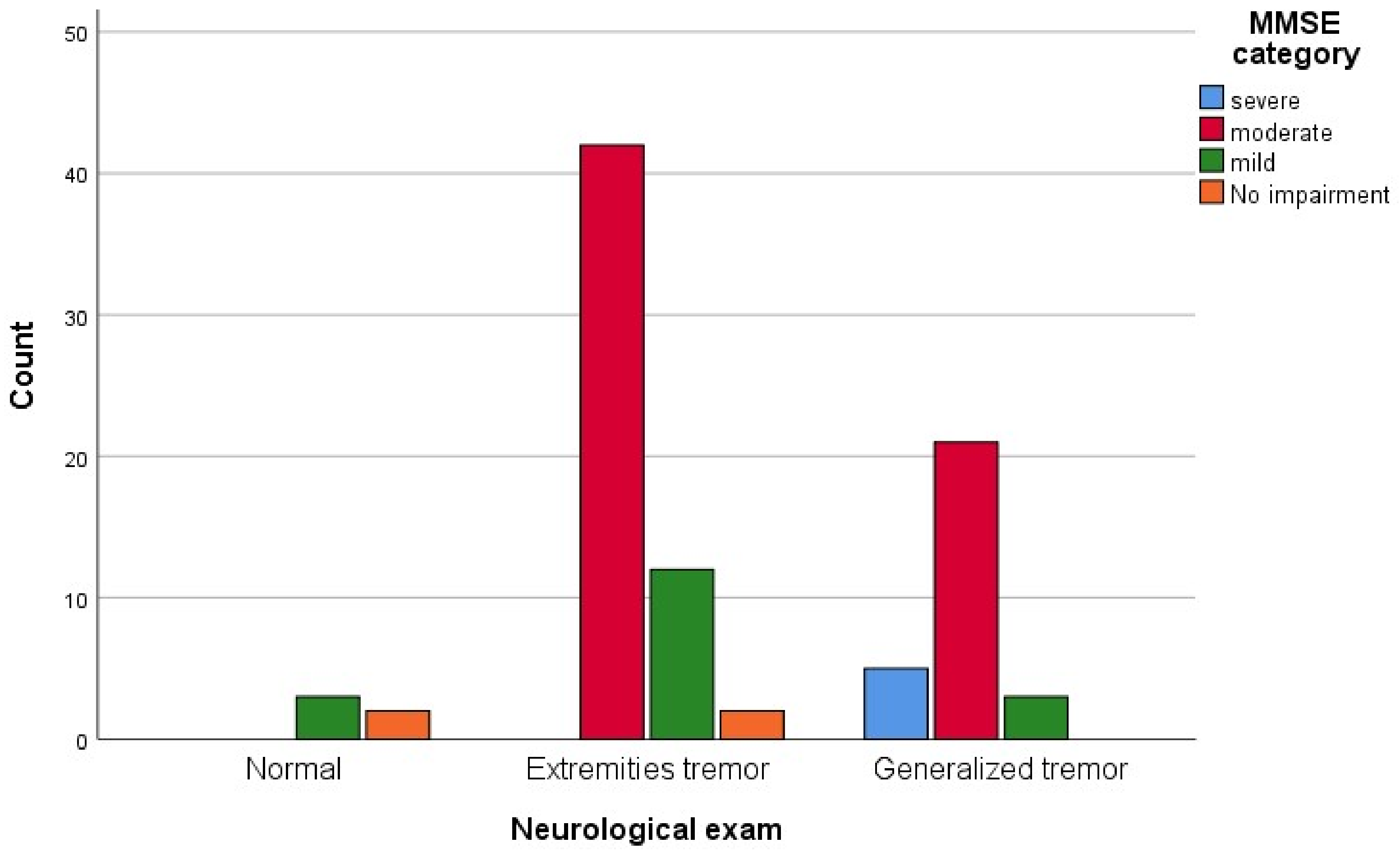
| Neurological Exam | MMSE Category | |||
|---|---|---|---|---|
| Severe | Moderate | Mild | No Impairment | |
| Normal | 0 | 0 | 3 | 2 |
| Extremities tremor | 0 | 42 | 12 | 2 |
| Generalized tremor | 5 | 21 | 3 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morega, S.; Ionele, C.-M.; Podeanu, M.-A.; Florescu, D.-N.; Rogoveanu, I. Assessment of Cognitive Function in Romanian Patients with Chronic Alcohol Consumption. Gastroenterol. Insights 2024, 15, 433-446. https://doi.org/10.3390/gastroent15020031
Morega S, Ionele C-M, Podeanu M-A, Florescu D-N, Rogoveanu I. Assessment of Cognitive Function in Romanian Patients with Chronic Alcohol Consumption. Gastroenterology Insights. 2024; 15(2):433-446. https://doi.org/10.3390/gastroent15020031
Chicago/Turabian StyleMorega, Shandiz, Claudiu-Marinel Ionele, Mihaela-Andreea Podeanu, Dan-Nicolae Florescu, and Ion Rogoveanu. 2024. "Assessment of Cognitive Function in Romanian Patients with Chronic Alcohol Consumption" Gastroenterology Insights 15, no. 2: 433-446. https://doi.org/10.3390/gastroent15020031
APA StyleMorega, S., Ionele, C.-M., Podeanu, M.-A., Florescu, D.-N., & Rogoveanu, I. (2024). Assessment of Cognitive Function in Romanian Patients with Chronic Alcohol Consumption. Gastroenterology Insights, 15(2), 433-446. https://doi.org/10.3390/gastroent15020031