1. Introduction
Despite significant advancements in reducing mortality rates, particularly within specialized centers, pancreaticoduodenectomy (PD) is still associated with increased morbidity and mortality [
1]. Postoperative infections, especially those involving multidrug-resistant bacteria (MDR), play a pivotal role in contributing to postoperative complications and mortality. An increasing body of literature focuses on the impact of postoperative MDR infections on short-term outcomes in patients undergoing pancreatic surgery [
2,
3].
The global dissemination of multidrug-resistant organisms within healthcare facilities is a significant and growing concern, not only because it has a substantial impact on the outcomes of surgical patients but also on the economy and sustainability of the healthcare system [
4,
5]. For these reasons, studies evaluating the potential role of MDR contamination on postoperative complications after general surgery and possible mitigation strategies have been advocated by clinicians and healthcare providers [
6].
Interestingly, multidrug-resistant infections are exhibited more frequent after pancreaticoduodenectomy (PD) compared to other abdominal surgeries [
7]. A better understanding of the mechanisms behind this specific finding is mandatory, especially considering the impact of MDR on such a complex procedure [
8].
Preoperative biliary stent (PBS) placement, in most cases, results in biliary contamination that seems to play a major role in postoperative infections after pancreaticoduodenectomy [
9,
10,
11]. The routine preoperative biliary stent (PBS) placement often results in biliary contamination and is emerging as a key factor in postoperative infections following pancreaticoduodenectomy [
9,
10,
11]. The use of PBS as a ‘bridge’ therapy before pancreaticoduodenectomy in patients with obstructive jaundice remains controversial. One the hand, it allows patients to undergo neoadjuvant treatments or be referred to high-volume centres, and on the other hand, PBS placement is associated with an elevated risk of postoperative morbidity [
12]. This can be attributed to the communication established by PBS between the digestive and biliary tracts, allowing bacterial migration from the duodenum to the biliary tract and resulting in biliary contamination. The chronic nature of this contamination, often necessitating antibiotic therapy, could result in the selection of multidrug-resistant strains. In order to counteract this phenomenon, it is fundamental to gather information on the bacterial strains involved and the mechanisms that could lead to the development of MDR.
The aim of this study is to investigate the impact of MDR contamination on short-term postoperative outcomes in patients undergoing PD, elucidating the intricate relationship between MDR bacteria, PBS, and bile contaminations. Through a comprehensive exploration of these dynamics, our ultimate goal is to provide insights that may contribute at mitigating the adverse effects of MDR contamination in the postoperative period following PD, ultimately enhancing patient outcomes and alleviating the burden of postoperative complications.
2. Methods
This is a retrospective study based on a prospectively maintained database of 825 consecutive patients who underwent pancreaticoduodenectomies (PDs) between January 2010 and December 2020 at our institution. All patients provided informed consent for the collection of their clinical data for scientific purposes.
Demographic and perioperative variables, including age, sex, American Society of Anesthesiologists (ASA) score, Body Mass Index (BMI), preoperative biliary stent, and the use of neoadjuvant chemotherapy, were collected. Intraoperative parameters (pancreatic texture, Wirsung’s diameter, estimated blood loss, operative time) and postoperative factors (pathological diagnosis, postoperative complications) were also analyzed.
All procedures were performed by experienced pancreatic surgeons at a high-volume center. The postoperative management of patients was carried out according to international guidelines and followed the same perioperative enhanced recovery protocol. Reconstruction was routinely realized with a manual end-to-side pancreatico-jejunostomy (PJ) in double layers, with or without duct-to-mucosa anastomosis. Additionally, an end-to-side hepatico-jejunostomy (HJ) and duodeno/gastro-jejunostomy (DJ) were fashioned on the same jejunal loop according to Child’s modified method. However, patients with a high risk of pancreatic fistula (POPF) development due to soft texture and Wirsung’s diameter < 3 mm underwent a pancreatico-jejunostomy Roux-en-Y.
Antibiotic prophylaxis was standardized for all patients according to center protocols, designed by infectious disease specialists considering international guidelines and antibiotic resistance profiles of common pathogens isolated in our center during previous studies [
10]. Patients without preoperative biliary stents (PBS) received intraoperative amoxicillin + clavulanic acid (two grams intravenously), with the first dose administered before skin incision and repeated every three hours until the end of the procedure or the third dose. Patients with biliary stenting received a single administration of gentamicin (3 milligrams/kg) before skin incision. For penicillin-allergic patients, a combination of clindamycin 600 mg every 6 h and gentamicin was administered.
Intraoperative bile culture was routinely performed in every patient. Bile collection was performed by needle aspiration before the transection of the common bile duct. Bacterial contamination of surgical drains was routinely evaluated through microbiological tests performed on the drain material. The evaluation was consistently performed on postoperative day 5 for the drain placed posteriorly to the pancreatico-jejunal anastomosis.
Multidrug-resistant bacteria (MDR) were defined as any bacteria resistant to at least one agent in three or more antimicrobial categories, according to the definition proposed by an international expert committee and published in 2012 in Clinical Microbiology and Infections [
13].
Surgical site infection was defined as wound infection or organ/space infection occurring during hospitalization or within 30 days after surgery, according to the description provided by the US Centers for Disease Control and Prevention (CDC) [
14].
Postoperative complications within 90 days were classified according to the Clavien–Dindo classification, and considered major (MPC) if grade equal to or greater than 3 [
15].
Postoperative pancreatic fistula (POPF) was defined according to the International Study Group on Pancreatic Surgery classification [
16]. Clinically relevant POPF (CR-POPF) was defined as grade B and C [
16].
Statistical Analysis
Statistical analysis was conducted using SPSS software (IBM SPSS Statistics for Windows, Version 26.0, Armonk, NY, USA: IBM Corp). Statistical significance was defined for p-values less than 0.05. Univariate analyses employed the Chi-square test and Fisher’s exact test for comparing categorical variables, while Student’s t-test and Mann–Whitney U were utilized for comparing continuous variables, depending on the distribution of the variable. Logistic regression models were applied for both univariate and multivariate analyses. The data were presented as percentages or as median and interquartile range [IQR].
3. Results
A total of 825 patients were evaluated, with 442 patients (53.6%) undergoing stent placement and 383 patients (46.4%) without stents. Overall bile contamination was observed in 54.1% (446/825) of cases. Among patients with bile contamination, 98% (437/446) had a previous stent placement, while only 2% (9/446) did not have a previous stent placement (
p < 0.001). Detailed characteristics of the overall population are presented in
Table 1.
MDR isolation in intraoperative bile cultures: MDR bacteria were present in 18.9% (156/825) of bile cultures, exclusively in the stented group.
Among patients with metallic stents, 44.3% (71/160) had MDR bacteria in the bile compared to 18.2% (36/198) with plastic stents (p < 0.001). No other specific patient characteristics in our cohort seemed to correlate with the presence of MDR in the bile at the time of the operation. Factors such as age (68.9 vs. 65.8 years), BMI (23.3 vs. 24.1), sex, ASA ≥ 3 (26.0% vs. 21.3%), history of diabetes (20.6% vs. 21.1%), malignant disease (52.6% vs. 52.1%), year of the procedure, or undergoing neoadjuvant treatment (22.7% vs. 18.1) did not show a clear prevalence in the MDR group. Moreover, no significant correlation with the length of time between stent placement and surgical procedure and MDR bile contamination was found (for MDR bile + was 66 [interquartile range 45.5] vs. 46.5 [98.5] days p = 0.475).
When MDR bacteria were present in the bile, the CR-POPF rate was 28.2%, compared to 19.0% in the remaining patients (
p = 0.01). Reintervention was necessary in 11% compared to 1.3% (
p < 0.001). Furthermore, at the multivariate analysis, the development of a major postoperative complication (MPC) was correlated with the presence of MDR bacteria in the bile (OR 1.66, 95% CI: 1.1–2.52;
p = 0.02). Results are summarized in
Table 2 and
Table 3. Among MDR bile-positive patients, the 28.0% had an uneventful postoperative period. Regarding the postoperative length of stay (LOS), patients with MDR bacteria in the bile had a prolonged LOS compared to patients without, with a median of 13 [11] days vs. 11 [8] (
p = 0.017).
3.1. MDR Isolation in Surgical Drain
MDR bacteria were identified in the surgical drainage during our routine evaluation on the fifth postoperative day in 144 out of 825 patients (17.4%). Among these, 72.2% had a previous biliary stent placement, while 27.8% were non-stented (p < 0.001).
When considering variables such as age, BMI, sex, ASA ≥ 3, past history of diabetes, diagnosis, year of the procedure, or neoadjuvant treatment, only patients with ASA ≥ 3 showed a statistically significant difference in the group of patients with MDR contamination of the surgical drain, with a higher rate of ASA ≥ 3 (27.7% vs. 17.1%; p = 0.017).
The major postoperative complication (MPC) rate was 29.2% when MDR was found in the drain, compared to 18.5% in patients without MDR contamination of the drain (
p = 0.006). In patients with MDR drain contamination, CR-POPF was 29.2% compared to 18.5% (
p = 0.004), wound infection was 13.2% vs. 5.3% (
p < 0.001), and the reintervention rate was 12.5% vs. 4.3% (
p < 0.001). Furthermore, at the multivariate analysis (including pancreas consistency, Wirsung diameter, ASA score, BMI, and age), the development of an MPC was independently correlated with the presence of MDR bacteria in the drainage (OR = 1.81, 95% CI: 1.21–2.73,
p = 0.0042). Results are summarized in
Table 3 and
Table 4. In this subgroup of patients, 24.3% had an uneventful postoperative period. Also, in this case, patients with MDR bacteria isolated in the surgical drain showed a prolonged length of stay (LOS) compared to patients without, with a median of 13.5 [11] days vs. 11 [7] (
p = 0.001).
The presence of an Extended-Spectrum Beta-Lactamase (ESBL) bacteria contaminating the surgical site on the fifth postoperative day had a statistically significant impact on MPC, with a rate of 30.4% vs. 20.7%. We did not observe a statistically significant effect on MPC by vancomycin-resistant enterococci (VRE) (33.3% vs. 22.3%), carbapenemase-producing enterobacteriaceae (CPE) (25.5% vs. 22.2%), and methicillin-resistant S. aureus (MRSA) (21.1% vs. 22.4%).
On the other hand, the higher impact on the length of stay was observed in patients with early VRE contamination in the surgical drain, with 18 [27] days compared to ESBL (14 (11) days), CPE (13 (12) days), and MRSA (13 (5) days). Unfortunately, only one of these observations reached statistical significance.
3.2. MDR Isolation
The incidence of major postoperative complications (MPC) increases when patients have MDR in both bile and drainage. Specifically, the MPC rate is 17.1% for patients without MDR, 27.5% for patients with MDR in the bile, 29.3% for patients with MDR in the drainage, and 33.3% for patients with MDR in both bile and drainage (
p = 0.002). Results are presented in
Table 5.
Among patients without MDR contamination in the intraoperative bile or drain on the fifth postoperative day, only 2.3% experienced subsequent MDR contamination in the postoperative period.
In our cohort, the rate of MDR contaminations developed after POD 5 (in patients with no evidence of MDR in bile intraoperatively and drain at POD V) is 2.3%.
3.3. MDR Bacteria
Among MDR bacteria in both bile and drainage, the most frequently isolated bacteria belonged to the Extended-Spectrum β-Lactamases category (53.8% vs. 13.6%), followed by carbapenemase-producing enterobacteriaceae (1.9% vs. 5.7%).
These bacteria were found in both bile and drainage in 67.2% of MDR patients.
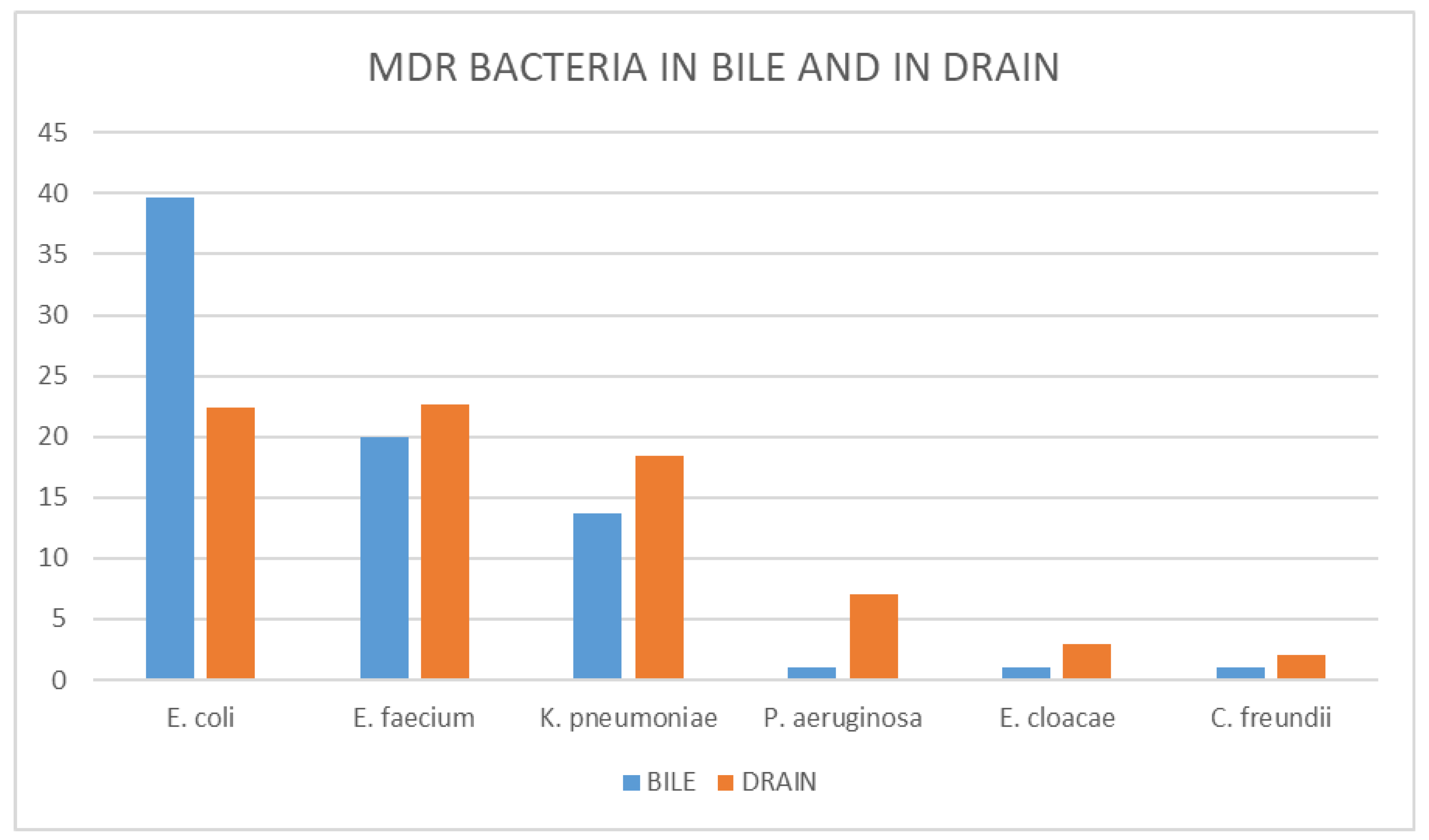
The most common MDR bacteria in bile and drainage were
E. coli (39.7% vs. 22.4%),
E. faecium (19.9% vs. 27.2%), and
K. pneumoniae (13.7% vs. 18.4%). The complete list is provided in
Figure 1.
The percentage of MDR for specific pathogens in our series, considering surgical drain isolation, is 36.4% for E. coli, 31.5% for E. faecium, 40.3% for K. pneumoniae, 35.0% for P. aeruginosa, and 40.4% for E. cloacae.
The prevalence of MDR traits for specific pathogens in our series, considering the most common MDR and naïve bacteria in bile isolation, is 47.1% for E. coli, 28.7% for E. faecium, 38.5% for K. pneumoniae, 56.2% for P. aeruginosa, 33.3% for E. cloacae, 8.4% for E. faecalis, and 1.5% for C. freundii.
Without considering the MDR trait, the most common bacteria in the bile in our population are E. faecalis, C. freundii, and E. coli, with a prevalence among the bile samples of 60.7%, 47.8%, and 24.9%, respectively.
3.4. Antibiotic Therapy
In accordance with our clinical and institutional policy, asymptomatic bacterial bile colonization was not routinely treated.
A tailored antibiotic therapy was started when patients developed clinical signs of infection, and when available, cultural findings guided the selection of specific drugs. The choice of antibiotic therapy was guided on the antimicrobial susceptibility tests and discussed with the infectious disease specialist.
Antibiotic treatment was required in 47.3% of the overall population, 38.5% of non-stented patients, and 53.1% of those who underwent biliary stenting (p = 0.001); moreover, it was needed in 58.2% of patients with MDR bacteria in the bile, with 70.2% of these requiring multidrug therapy. Only 44.4% of patients without MDR in the bile needed antibiotics in the postoperative period (p = 0.001).
Among patients with MDR bacteria in the drainage, 72.9% required antibiotic therapy, while 27.3% of patients without MDR bacteria in the drainage needed antibiotics (
p < 0.001). In patients with MDR bacteria in the drainage, the most frequently used antibiotics were β-Lactam antibiotics, followed by Fluoroquinolones and Carbapenems. Specific antibiotic therapy rates and the number of lines of therapy are detailed in
Table 6.
4. Discussion
Pancreaticoduodenectomy is a complex and technically demanding procedure associated with a high risk of postoperative complications, including infections caused by multidrug-resistant (MDR) bacteria. MDR bacteria seem to contaminate patients undergoing pancreaticoduodenectomy more frequently than in other surgical procedures. In our experience, this contamination occurs even before commonly known risk factors, such as prolonged postoperative antibiotic therapy and ICU stay [
17], can take effect, as demonstrated by the finding of MDR bacteria intraoperatively and on postoperative day 5 (POD V).
In our cohort, the rate of MDR contaminations developed after POD 5 (in patients with no evidence of MDR in bile intraoperatively and drain at POD V) is 2.3%, an incidence similar to other abdominal surgical procedures [
18], and markedly different from the 17.4% MDR contamination rate of the surgical site observed on POD V in our series. These specific findings suggest that the increased rate of MDR infection after pancreaticoduodenectomy could be related to pre-existing MDR contamination, mainly at the level of the biliary tract. Previous studies have demonstrated that bile infection is associated with interventional biliary endoscopy, which is associated with an increased rate of postoperative infections [
19,
20]. Our findings are consistent with previous studies reporting an increase in MDR bacteria in the bile of patients with biliary stents [
21,
22]. We demonstrated that MDR bacteria were only present in the bilicultures of the stented group, and MDR bacteria in the drainage were mostly found in the stented group, with the same MDR bacteria isolated in the bile and in the drain in 67.2% of cases. This finding for the first time underlines that the mitigation strategies aimed to reduce the MDR infection rate after PD had to focus after the stent placement to achieve more relevant results.
Our study has some limitations. Given the retrospective design, we could not analyze the specific mechanisms underlying our observations. However, the rate of MDR bacteria after pancreaticoduodenectomy, their presence at the time of the procedure in the bile, and their finding on the fifth postoperative day in the surgical drain, indicating the surgical site, clearly identify the preoperative and early postoperative period as the timeframe in which MDR bacteria colonize patients undergoing pancreaticoduodenectomy. Direct contamination during the surgical procedure or bacteremia could be the main factors that prompt the diffusion of MDR to the surgical site. However, MDR isolation in the surgical drain five days after the index operation suggests that other mechanisms may be responsible for the bacterial virulence despite intraoperative antibiotic prophylaxis and the immune system activity.
Furthermore, our study confirms that the presence of MDR contamination worsens short-term outcomes of patients undergoing pancreaticoduodenectomy. Moreover, the timing of the MDR finding (introperatively or POD5) precedes almost any MPC registered in out cohort. When MDR bacteria are isolated in the bile and in the drainage, there is a statistically significant increase in major postoperative complications. These findings are in line with a previous study by Zhang et al. [
4], which showed that MDR infections were associated with postoperative in-hospital death within 30 days, postoperative hospital stay, and postpancreatectomy hemorrhage. Our study confirmed that MDR infections worsened the outcome of patients undergoing pancreaticoduodenectomy, specifically in clinically relevant postoperative pancreatic fistula, wound infections, and the reintervention rate. The last finding aligns with a study by Bodro et al. [
23], which demonstrated that surgical re-operation after pancreas transplantation was independently associated with the development of infections by MDR organisms. Also, the length of stay, as reported in other studies [
24,
25], is deeply affected by the presence of MDR bacteria. This observation emphasizes the urgent need for a standardized approach to reduce the incidence and impact of MDR in patients undergoing pancreaticoduodenectomy.
Interestingly, the presence of MDR in the drain seems to correlate with patient frailty, (ASA ≥ 3). MDR infections are more frequent in frail patients, who are also a high-risk population in the postoperative period [
26]. On the other hand, we did not observe the same correlation with bile MDR bacteria contamination. It could be hypothesized that the contamination at the level of the bile is related to PBS and other multiple factors, but the early contamination of the same bacteria at the level of the surgical site could be facilitated by the frailty of the patients.
In our cohort, MDR bacteria isolated in the bile and drainage were
E. coli,
E. faecium, and
K. pneumoniae. These findings could be explained by an ascending bacterial migration from the duodenum to the biliary system due to biliary stenting, with subsequent bile contamination. These results are similar to a previous study by Cortes et al. [
27], who reported that the most frequent organisms in cultures of intraoperative bile were
Enterococcus species, followed
by E. coli and
Klebsiella species. Interestingly, the microorganisms isolated more frequently in the bile,
E. faecalis and
C. freundii, are not the same species responsible for the majority of the MDR contamination. Specific bacteria, such as
Enterobacters,
E. coli,
K. pneumoniae, and
P. aeruginosa, show impressive rates of MDR compared to the susceptible strains; one in two or one in three of these pathogens were MDR in our analysis, a rate far higher than reported in the literature. Specific bacteria seem more prone to develop MDR strains in the preoperative period in stented patients; in this setting, a selective pressure seems to promote the contamination by these specific subgroups of pathogens.
Patients with MDR infections usually received multiple antimicrobial agents compared to patients with postoperative infections caused by non-resistant bacteria. The complex antimicrobial regimen used to treat MDR bacteria imposes a significant economic burden on the healthcare system and undermines the efficacy of these same drugs in the near future. Our findings suggest that in the specific case of pancreaticoduodenectomy, in order to avoid damage to the patients and the health system due to MDR contamination, the crucial point could be the pre- and intraoperative period more than the postoperative period. Studies on the intraoperative antibiotic prophylaxis in these specific settings are needed, as well as the implementation of the actual stenting device to mitigate bacterial contamination, as has been carried out with other medical devices (e.g., urinary catheters). More recently, the early detection of MDR bacteria by rectal swab evaluation has been routinely used in clinical practice, leading to the isolation of patients with such contamination at the moment of admission [
28]. This strategy should be considered, especially in patients who underwent pancreaticoduodenectomy after biliary stent placement, but studies are needed to evaluate its cost effectiveness and efficacy for the health system. Moreover, the possibility to associate other more therapeutic approaches or management protocols in this subgroup of patients needs to be assessed to improve their short-term outcomes.
Our study also highlights that MDR bacteria in the bile were most commonly found in patients with metallic stents rather than in patients with plastic stents even if the time window between the stent placement and the surgical procedure seem not to affect the contamination rate. Several studies [
29,
30,
31] suggest the superiority of metallic stents to plastic stents due to their longer patency, potentially avoiding replacement and stent-related problems in patients who are subjected to a delayed schedule or underwent neoadjuvant chemotherapy. The efficacy of metallic stents is still debated in the preoperative setting. However, the larger diameter of metallic stents might help in resolving cholestasis or obstructed bile flow. At the same time, compared to the plastic stents, it might favour the upstream migration of microbes from the gastrointestinal tract into the biliary tree. On the other hand, metallic stents are the common choice in patients who will maintain the stent longer and usually in patients who will undergo neoadjuvant therapy. This prolonged stay could represent the main cause of the increased rate of MDR bacteria contamination observed, even if in our series, we did not observe a correlation between MDR contamination of the bile and neoadjuvant therapies. Further studies must focus on the correlation with MDR contamination with the cholangitis/infections rate and use of antibiotics between stent placement and PD.
This study has some limitations. First, it is a single-center retrospective study, while multi-center prospective studies will be necessary to confirm our results. However, a single-center series grants a uniformity of treatment management and a standardized clinical and surgical approach that could be difficult to obtain in a multicenter setting. Second, the choice to perform microbiological tests only on POD 5 and only from the pancreatic surgical drain was not based on previous experience or literature because none was available. We chose this timeframe to detect early clinically relevant contamination, not simple direct contamination by biliary intraoperative spillage. Third, it covers 10 years of experience, and even if no major changes had occurred in surgical technique and antibiotic therapy in our center, still, the rate of neoadjuvant therapy had increased drastically through the years, and this variability could have partially affected our observation. On the other hand, the high number of patients involved in this study allowed a subgroup analysis and the evaluation of even more rare pathogens such as VRE.
In conclusion, we confirm that early MDR contamination worsens the short-term outcomes of patients undergoing pancreaticoduodenectomy. MDR contamination increases postoperative major complications, length of stay, and multiple antibiotic therapy. Our data suggest that the majority of MDR surgical site infections derive from the preoperative period, probably from biliary contamination resulting after the placement of a biliary stent. Under specific conditions, these bacteria contaminate the surgical site early, affecting patients’ short-term outcomes. Further comprehensive studies are needed to investigate which factors might play a role in MDR bile contamination and how to mitigate this phenomenon to reduce postoperative morbidity.


 ,
, 

{kind=link}