
Foremost Concepts in Mechanisms of De Novo Post-Liver Transplantation Malignancy

 ,
, 
Abstract
1. Introduction
2. De Novo Malignancy in Patients after Liver Transplantation
3. Immunosuppression and Carcinogenesis
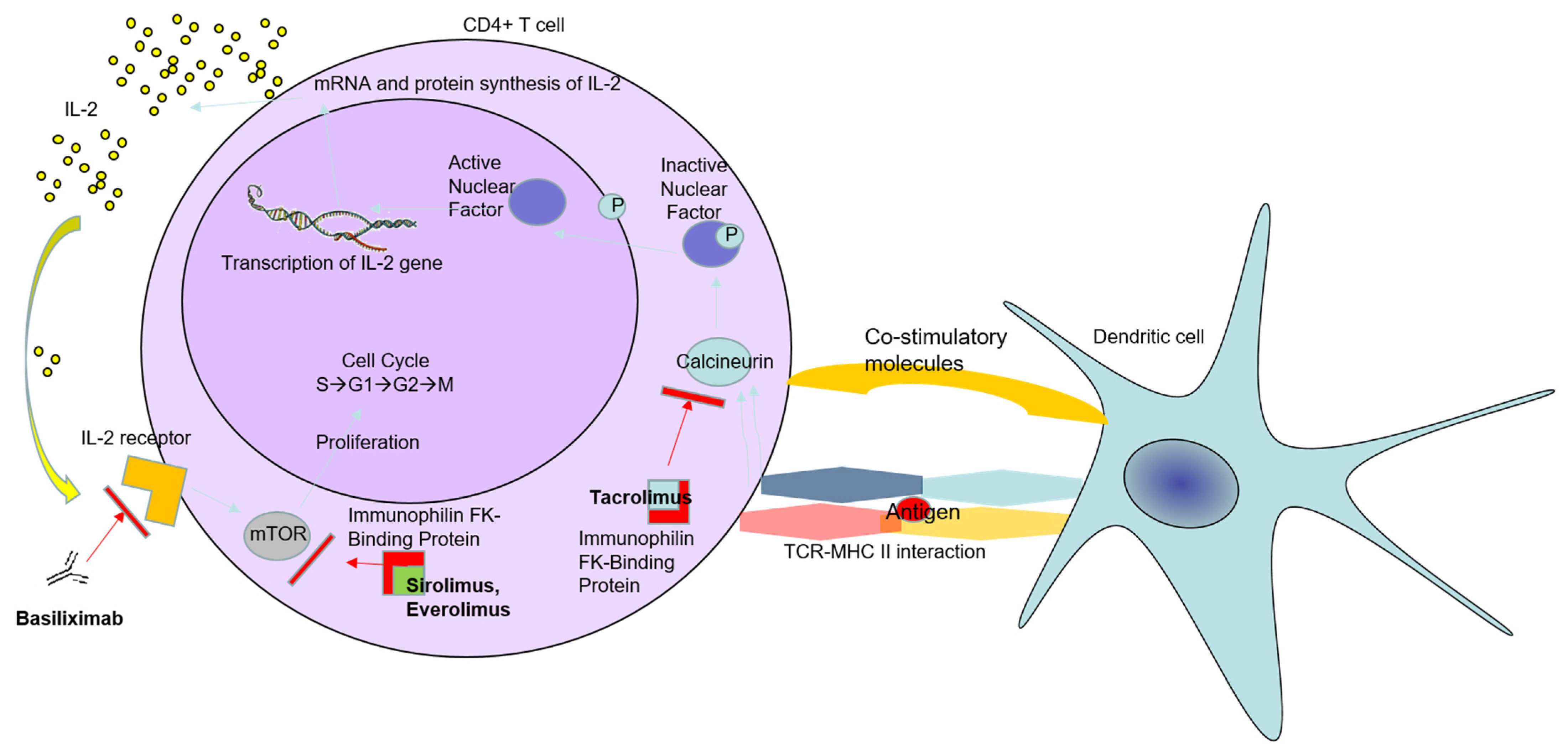
4. Immunosuppressive Drugs and Their Impact on the Immune System Tumor Control
4.1. Corticosteroids after LT
4.2. Tacrolimus after LT
4.3. Mycophenolate Mofetil after LT
4.4. Mammalian Target of Rapamycin (mTOR) Inhibitors after LT
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fox, A.N.; Brown, R.S., Jr. Is the patient a candidate for liver transplantation? Clin. Liver Dis. 2012, 16, 435–448. [Google Scholar] [CrossRef] [PubMed]
- Adam, R.; Karam, V.; Delvart, V.; O’Grady, J.; Mirza, D.; Klempnauer, J.; Castaing, D.; Neuhaus, P.; Jamieson, N.; Salizzoni, M.; et al. Evolution of indications and results of liver transplantation in Europe. A report from the European Liver Transplant Registry (ELTR). J. Hepatol. 2012, 57, 675–688. [Google Scholar] [CrossRef]
- Engels, E.A.; Pfeiffer, R.M.; Fraumeni, J.F., Jr.; Kasiske, B.L.; Israni, A.K.; Snyder, J.J.; Wolfe, R.A.; Goodrich, N.P.; Bayakly, A.R.; Clarke, C.A.; et al. Spectrum of cancer risk among US solid organ transplant recipients. JAMA 2011, 306, 1891–1901. [Google Scholar] [CrossRef] [PubMed]
- Na, R.; Grulich, A.E.; Meagher, N.S.; McCaughan, G.W.; Keogh, A.M.; Vajdic, C.M. Comparison of de novo cancer incidence in Australian liver, heart and lung transplant recipients. Am. J. Transplant. 2013, 13, 174–183. [Google Scholar] [CrossRef]
- Krynitz, B.; Edgren, G.; Lindelöf, B.; Baecklund, E.; Brattström, C.; Wilczek, H.; Smedby, K.E. Risk of skin cancer and other malignancies in kidney, liver, heart and lung transplant recipients 1970 to 2008—A Swedish population-based study. Int. J. Cancer 2013, 132, 1429–1438. [Google Scholar] [CrossRef]
- Carenco, C.; Faure, S.; Ursic-Bedoya, J.; Herrero, A.; Pageaux, G.P. Solid, non-skin, post-liver transplant tumors: Key role of lifestyle and immunosuppression management. World J. Gastroenterol. 2016, 22, 427–434. [Google Scholar] [CrossRef]
- Bakker, N.A.; van Imhoff, G.W.; Verschuuren, E.A.; van Son, W.J. Presentation and early detection of post-transplant lymphoproliferative disorder after solid organ transplantation. Transpl. Int. 2007, 20, 207–218. [Google Scholar] [CrossRef] [PubMed]
- Scientific Registry Transplant Recipients (SRTR). Transplant Center Search Results. Available online: http://www.srtr.org (accessed on 28 June 2020).
- European Liver Transplant Registry. Evolution of Liver Transplantation in Europe. Available online: http://www.eltr.org (accessed on 28 June 2020).
- Adam, R.; McMaster, P.; O’Grady, J.G.; Castaing, D.; Klempnauer, J.L.; Jamieson, N.; Neuhaus, P.; Lerut, J.; Salizzoni, M.; Pollard, S.; et al. European Liver Transplant Association. Evolution of liver transplantation in Europe: Report of the European Liver Transplant Registry. Liver Transpl. 2003, 9, 1231–1243. [Google Scholar] [CrossRef]
- Di Maira, T.; Coelho, L.E.; Berenguer, M. Immunosuppression in liver transplant. Best Pract. Res. Clin. Gastroenterol. 2020, 46–47, 101681. [Google Scholar] [CrossRef]
- Sherston, S.N.; Carroll, R.P.; Harden, P.N.; Wood, K.J. Predictors of cancer risk in the long-term solid-organ transplant recipient. Transplantation 2014, 97, 605–611. [Google Scholar] [CrossRef] [PubMed]
- Piselli, P.; Verdirosi, D.; Cimaglia, C.; Busnach, G.; Fratino, L.; Ettorre, G.M.; De Paoli, P.; Citterio, F.; Serraino, D. Epidemiology of de novo malignancies after solid-organ transplantation: Immunosuppression, infection and other risk factors. Best Pract. Res. Clin. Obstet. Gynaecol. 2014, 28, 1251–1265. [Google Scholar] [CrossRef]
- Altieri, M.; Sérée, O.; Lobbedez, T.; Segol, P.; Abergel, A.; Blaizot, X.; Boillot, O.; Boudjema, K.; Coilly, A.; Conti, F.; et al. Risk factors of de novo malignancies after liver transplantation: A French national study on 11004 adult patients. Clin. Res. Hepatol. Gastroenterol. 2021, 45, 101514. [Google Scholar] [CrossRef]
- Benlloch, S.; Berenguer, M.; Prieto, M.; Moreno, R.; San Juan, F.; Rayón, M.; Mir, J.; Segura, A.; Berenguer, J. De novo internal neoplasms after liver transplantation: Increased risk and aggressive behavior in recent years? Am. J. Transplant. 2004, 4, 596–604. [Google Scholar] [CrossRef]
- Das, R.; Kundu, S.; Laskar, S.; Choudhury, Y.; Ghosh, S.K. Assessment of DNA repair susceptibility genes identified by whole-exome sequencing in head and neck cancer. DNA Repair. 2018, 66–67, 50–63. [Google Scholar] [CrossRef]
- Shalaby, S.; Burra, P. De novo and recurrent malignancy. Best Pract. Res. Clin. Gastroenterol. 2020, 46–47, 101680. [Google Scholar] [CrossRef] [PubMed]
- Prendergast, G.C. Immune escape as a fundamental trait of cancer: Focus on IDO. Oncogene 2008, 27, 3889–3900. [Google Scholar] [CrossRef] [PubMed]
- Vajdic, C.M.; van Leeuwen, M.T. Cancer incidence and risk factors after solid organ transplantation. Int. J. Cancer 2009, 125, 1747–1754. [Google Scholar] [CrossRef] [PubMed]
- Lake, R.A.; van der Most, R.G. A better way for a cancer cell to die. N. Engl. J. Med. 2006, 354, 2503–2504. [Google Scholar] [CrossRef] [PubMed]
- Zitvogel, L.; Tesniere, A.; Kroemer, G. Cancer despite immunosurveillance: Immunoselection and immunosubversion. Nat. Rev. Immunol. 2006, 6, 715–727. [Google Scholar] [CrossRef]
- Dunn, G.P.; Koebel, C.M.; Schreiber, R.D. Interferons, immunity and cancer immunoediting. Nat. Rev. Immunol. 2006, 6, 836–848. [Google Scholar] [CrossRef]
- Glick, A.B.; Yuspa, S.H. Tissue homeostasis and the control of the neoplastic phenotype in epithelial cancers. Semin. Cancer Biol. 2005, 15, 75–83. [Google Scholar] [CrossRef]
- Ferro, M.; Ungaro, P.; Cimmino, A.; Lucarelli, G.; Busetto, G.M.; Cantiello, F.; Damiano, R.; Terracciano, D. Epigenetic Signature: A New Player as Predictor of Clinically Significant Prostate Cancer (PCa) in Patients on Active Surveillance (AS). Int. J. Mol. Sci. 2017, 18, 1146. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez-Dalmau, A.; Campistol, J.M. Immunosuppressive therapy and malignancy in organ transplant recipients: A systematic review. Drugs 2007, 67, 1167–1198. [Google Scholar] [CrossRef] [PubMed]
- Conti, F.; Morelon, E.; Calmus, Y. Immunosuppressive therapy in liver transplantation. J. Hepatol. 2003, 39, 664–678. [Google Scholar] [CrossRef]
- Haller, M.C.; Royuela, A.; Nagler, E.V.; Pascual, J.; Webster, A.C. Steroid avoidance or withdrawal for kidney transplant recipients. Cochrane Database Syst. Rev. 2016, 8, CD005632. [Google Scholar] [CrossRef]
- Rutz, H.P.; Herr, I. Interference of glucocorticoids with apoptosis signaling and host-tumor interactions. Cancer Biol. Ther. 2004, 3, 715–718. [Google Scholar] [CrossRef][Green Version]
- Pelletier, S.J.; Nadig, S.N.; Lee, D.D.; Ammori, J.B.; Englesbe, M.J.; Sung, R.S.; Magee, J.C.; Fontana, R.J.; Punch, J.D. A prospective, randomized trial of complete avoidance of steroids in liver transplantation with follow-up of over 7 years. HPB 2013, 15, 286–293. [Google Scholar] [CrossRef]
- Cillo, U.; De Carlism, L.; Del Gaudio, M.; De Simone, P.; Fagiuoli, S.; Lupo, F.; Tisone, G.; Volpes, R. Immunosuppressive regimens for adult liver transplant recipients in real-life practice: Consensus recommendations from an Italian Working Group. Hepatol. Int. 2020, 14, 930–943. [Google Scholar] [CrossRef]
- Bennett, J.; Cassidy, H.; Slattery, C.; Ryan, M.P.; McMorrow, T. Tacrolimus Modulates TGF-β Signaling to Induce Epithelial-Mesenchymal Transition in Human Renal Proximal Tubule Epithelial Cells. J. Clin. Med. 2016, 5, 50. [Google Scholar] [CrossRef]
- Dougan, M.; Dranoff, G. Immune therapy for cancer. Annu. Rev. Immunol. 2009, 27, 83–117. [Google Scholar] [CrossRef]
- Mortara, L.; Balza, E.; Bruno, A.; Poggi, A.; Orecchia, P.; Carnemolla, B. Anti-cancer Therapies Employing IL-2 Cytokine Tumor Targeting: Contribution of Innate, Adaptive and Immunosuppressive Cells in the Anti-tumor Efficacy. Front. Immunol. 2018, 9, 2905. [Google Scholar] [CrossRef] [PubMed]
- Angriman, I.; Furian, L.; Scarpa, M. Effects of immune suppression for transplantation on inflammatory colorectal cancer progression. Oncogenesis 2018, 7, 46. [Google Scholar] [CrossRef] [PubMed]
- Spolski, R.; Li, P.; Leonard, W.J. Biology and regulation of IL-2: From molecular mechanisms to human therapy. Nat. Rev. Immunol. 2018, 18, 648–659. [Google Scholar] [CrossRef]
- Burra, P.; Rodriguez-Castro, K.I. Neoplastic disease after liver transplantation: Focus on de novo neoplasms. World J. Gastroenterol. 2015, 21, 8753–8768. [Google Scholar] [CrossRef] [PubMed]
- Pillai, A.A.; Levitsky, J. Overview of immunosuppression in liver transplantation. World J. Gastroenterol. 2009, 15, 4225–4233. [Google Scholar] [CrossRef] [PubMed]
- Hojo, M.; Morimoto, T.; Maluccio, M.; Asano, T.; Morimoto, K.; Lagman, M.; Shimbo, T.; Suthanthiran, M. Cyclosporine induces cancer progression by a cell-autonomous mechanism. Nature 1999, 397, 530–534. [Google Scholar] [CrossRef] [PubMed]
- Yarosh, D.B.; Pena, A.V.; Nay, S.L.; Canning, M.T.; Brown, D.A. Calcineurin inhibitors decrease DNA repair and apoptosis in human keratinocytes following ultraviolet B irradiation. J. Investig. Dermatol. 2005, 125, 1020–1025. [Google Scholar] [CrossRef] [PubMed]
- Guba, M.; von Breitenbuch, P.; Steinbauer, M.; Koehl, G.; Flegel, S.; Hornung, M.; Bruns, C.J.; Zuelke, C.; Farkas, S.; Anthuber, M.; et al. Rapamycin inhibits primary and metastatic tumor growth by antiangiogenesis: Involvement of vascular endothelial growth factor. Nat. Med. 2002, 8, 128–135. [Google Scholar] [CrossRef]
- Maluccio, M.; Sharma, V.; Lagman, M.; Vyas, S.; Yang, H.; Li, B.; Suthanthiran, M. Tacrolimus enhances transforming growth factorbeta1 expression and promotes tumor progression. Transplantation 2003, 76, 597–602. [Google Scholar] [CrossRef]
- Verran, D.J.; Mulhearn, M.H.; Dilworth, P.J.; Balderson, G.A.; Munn, S.; Chen, J.W.; Fink, M.A.; Crawford, M.D.; McCaughan, G.W. Nature and outcomes of the increased incidence of colorectal malignancy after liver transplantation in Australasia. Med. J. Aust. 2013, 199, 610–612. [Google Scholar] [CrossRef][Green Version]
- Soleimanpour, S.A.; Crutchlow, M.F.; Ferrari, A.M.; Raum, J.C.; Groff, D.N.; Rankin, M.M.; Liu, C.; De León, D.D.; Naji, A.; Kushner, J.A.; et al. Calcineurin signaling regulates human islet {beta}-cell survival. J. Biol. Chem. 2010, 285, 40050–40059. [Google Scholar] [CrossRef]
- Levy, G.; Villamil, F.; Samuel, D.; Sanjuan, F.; Grazi, G.L.; Wu, Y.; Marotta, P.; Boillot, O.; Muehlbacher, F.; Klintmalm, G.; et al. Results of lis2t, a multicenter, randomized study comparing cyclosporine microemulsion with C2 monitoring and tacrolimus with C0 monitoring in de novo liver transplantation. Transplantation 2004, 77, 1632–1638. [Google Scholar] [CrossRef] [PubMed]
- El-Serag, H.B.; Hampel, H.; Javadi, F. The association between diabetes and hepatocellular carcinoma: A systematic review of epidemiologic evidence. Clin. Gastroenterol. Hepatol. 2006, 4, 369–380. [Google Scholar] [CrossRef]
- Carenco, C.; Assenat, E.; Faure, S.; Duny, Y.; Danan, G.; Bismuth, M.; Herrero, A.; Jung, B.; Ursic-Bedoya, J.; Jaber, S.; et al. Tacrolimus and the risk of solid cancers after liver transplant: A dose effect relationship. Am. J. Transplant. 2015, 15, 678–686. [Google Scholar] [CrossRef] [PubMed]
- Allison, A.C.; Eugui, E.M. Mycophenolate mofetil and its mechanisms of action. Immunopharmacology 2000, 47, 85–118. [Google Scholar] [CrossRef]
- Cohn, R.G.; Mirkovich, A.; Caulfield, J.; Eugui, E.M. Apoptosis of human activated peripheral T-cells and Tlymphocytic and promonocytic cell lines induced by mycophenolic acid, the active metabolite of CellCept. In Proceedings of the Basic Sciences Symposium of the Transplantation Society, Monterey, CA, USA, 25–29 August 1999; p. 173. [Google Scholar]
- Carter, S.B.; Franklin, T.J.; Jones, D.F.; Leonard, B.J.; Mills, S.D.; Turner, R.W.; Turner, W.B. Mycophenolic acid: An anti-cancer compound with unusual properties. Nature 1969, 223, 848–850. [Google Scholar] [CrossRef] [PubMed]
- Engl, T.; Makarević, J.; Relja, B.; Natsheh, I.; Müller, I.; Beecken, W.D.; Jonas, D.; Blaheta, R.A. Mycophenolate mofetil modulates adhesion receptors of the beta1 integrin family on tumor cells: Impact on tumor recurrence and malignancy. BMC Cancer 2005, 5, 4. [Google Scholar] [CrossRef]
- Francis, A.; Johnson, D.W.; Craig, J.; Teixeira-Pinto, A.; Wong, G. Post-transplant lymphoproliferative disease may be an adverse risk factor for patient survival but not graft loss in kidney transplant recipients. Kidney Int. 2018, 94, 809–817. [Google Scholar] [CrossRef]
- Koehl, G.E.; Wagner, F.; Stoeltzing, O.; Lang, S.A.; Steinbauer, M.; Schlitt, H.J.; Geissler, E.K. Mycophenolate mofetil inhibits tumor growth and angiogenesis in vitro but has variable antitumor effects in vivo, possibly related to bioavailability. Transplantation 2007, 83, 607–614. [Google Scholar] [CrossRef]
- De Simone, P.; Fagiuoli, S.; Cescon, M.; De Carlis, L.; Tisone, G.; Volpes, R.; Cillo, U.; Consensus Panel. Use of Everolimus in Liver Transplantation: Recommendations from a Working Group. Transplantation 2017, 101, 239–251. [Google Scholar] [CrossRef]
- Sharma, P.; Welch, K.; Eikstadt, R.; Marrero, J.A.; Fontana, R.J.; Lok, A.S. Renal outcomes after liver transplantation in the model for end-stage liver disease era. Liver Transpl. 2009, 15, 1142–1148. [Google Scholar] [CrossRef] [PubMed]
- Duvoux, C.; Toso, C. mTOR inhibitor therapy: Does it prevent HCC recurrence after liver transplantation? Transplant. Rev. 2015, 29, 168–174. [Google Scholar] [CrossRef]
- Jacinto, E.; Hall, M.N. Tor signalling in bugs, brain and brawn. Nat. Rev. Mol. Cell Biol. 2003, 4, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Granata, S.; Dalla, G.A.; Carraro, A.; Brunelli, M.; Stallone, G.; Lupo, A.; Zaza, G. Sirolimus and Everolimus Pathway: Reviewing Candidate Genes Influencing Their Intracellular Effects. Int. J. Mol. Sci. 2016, 17, 735. [Google Scholar] [CrossRef] [PubMed]
- Laplante, M.; Sabatini, D.M. mTOR signaling in growth control and disease. Cell 2012, 149, 274–293. [Google Scholar] [CrossRef]
- Yang, H.; Rudge, D.G.; Koos, J.D.; Vaidialingam, B.; Yang, H.J.; Pavletich, N.P. mTOR kinase structure, mechanism and regulation. Nature 2013, 497, 217–223. [Google Scholar] [CrossRef]
- Hu, T.H.; Huang, C.C.; Lin, P.R.; Chang, H.W.; Ger, L.P.; Lin, Y.W.; Changchien, C.S.; Lee, C.M.; Tai, M.H. Expression and prognostic role of tumor suppressor gene PTEN/MMAC1/TEP1 in hepatocellular carcinoma. Cancer 2003, 97, 1929–1940. [Google Scholar] [CrossRef]
- Cholongitas, E.; Mamou, C.; Rodríguez-Castro, K.I.; Burra, P. Mammalian target of rapamycin inhibitors are associated with lower rates of hepatocellular carcinoma recurrence after liver transplantation: A systematic review. Transpl. Int. 2014, 27, 1039–1049. [Google Scholar] [CrossRef]
- Toso, C.; Merani, S.; Bigam, D.L.; Shapiro, A.M.; Kneteman, N.M. Sirolimus-based immunosuppression is associated with increased survival after liver transplantation for hepatocellular carcinoma. Hepatology 2010, 51, 1237–1243. [Google Scholar] [CrossRef]
- Treiber, G. mTOR inhibitors for hepatocellular cancer: A forward-moving target. Expert Rev. Anticancer Ther. 2009, 9, 247–261. [Google Scholar] [CrossRef]
- Ferrín, G.; Guerrero, M.; Amado, V.; Rodríguez-Perálvarez, M.; De la Mata, M. Activation of mTOR Signaling Pathway in Hepatocellular Carcinoma. Int. J. Mol. Sci. 2020, 21, 1266. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Romero, C.; Manrique, A.; Marqués, E.; Calvo, J.; Sesma, A.G.; Cambra, F.; Abradelo, M.; Sterup, R.M.; Olivares, S.; Justo, I.; et al. Switching to sirolimus monotherapy for de novo tumors after liver transplantation. A preliminary experience. Hepatogastroenterology 2011, 58, 115–121. [Google Scholar] [PubMed]
- Funk-Debleds, P.; Ducroux, E.; Guillaud, O.; Ursic-Bedoya, J.; Decullier, E.; Vallin, M.; Euvrard, S.; Pageaux, G.P.; Boillot, O.; Dumortier, J. Subsequent nonmelanoma skin cancers and impact of immunosuppression in liver transplant recipients. J. Am. Acad. Dermatol. 2018, 79, 84–91. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Cancer Type | SIR |
|---|---|
| Kaposi’s sarcoma | 61.46–100 |
| Skin (non-melanoma) | >13.85 |
| Head and neck cancers | 2.5–24.8 |
| PTLD | 3.9–21 |
| Thyroid | 0.65–4.6 |
| Esophagus | 12–23.4 |
| Stomach | 0.5–3.7 |
| Pancreas and biliary tract | 1.1–6.4 |
| Colorectal overall | 1.24–12.5 |
| Colorectal in IBD/PSC | 3–5 |
| Colorectal in non-IBD/PSC | 1–1.8 |
| Anal cancer | 3.3–10 |
| Lung, trachea, and bronchus | 1.1–8 |
| Urological tract | 0.8–10.2 |
| Kidney | 1.8–30 |
| Prostate (in males) | 0.39–2.2 |
| Cervix (in females) | 1.03–30.7 |
| Vulva (in females) | 8–23.8 |
| Breast (in females) | 0.3–2.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peruhova, M.; Peshevska-Sekulovska, M.; Panayotova, G.; Velikova, T. Foremost Concepts in Mechanisms of De Novo Post-Liver Transplantation Malignancy. Gastroenterol. Insights 2021, 12, 283-292. https://doi.org/10.3390/gastroent12030025
Peruhova M, Peshevska-Sekulovska M, Panayotova G, Velikova T. Foremost Concepts in Mechanisms of De Novo Post-Liver Transplantation Malignancy. Gastroenterology Insights. 2021; 12(3):283-292. https://doi.org/10.3390/gastroent12030025
Chicago/Turabian StylePeruhova, Milena, Monika Peshevska-Sekulovska, Gabriela Panayotova, and Tsvetelina Velikova. 2021. "Foremost Concepts in Mechanisms of De Novo Post-Liver Transplantation Malignancy" Gastroenterology Insights 12, no. 3: 283-292. https://doi.org/10.3390/gastroent12030025
APA StylePeruhova, M., Peshevska-Sekulovska, M., Panayotova, G., & Velikova, T. (2021). Foremost Concepts in Mechanisms of De Novo Post-Liver Transplantation Malignancy. Gastroenterology Insights, 12(3), 283-292. https://doi.org/10.3390/gastroent12030025