Evaluation of Helicobacter pylori Infection, Neutrophil–Lymphocyte Ratio and Platelet–Lymphocyte Ratio in Dyspeptic Patients


Abstract
1. Introduction
2. Materials and Methods
3. Endoscopic and Histopathologic Evaluation
4. Statistical Analyses
5. Results
6. Discussions
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Go, M.F. Natural history and epidemiology of Helicobacter pylori infection. Aliment. Pharmacol. Ther. 2002, 16 (Suppl. 1), 3–15. [Google Scholar] [CrossRef]
- Lúquez, M.A.; Otero, R.W.; Schmulson, M. Enfoque diagnóstico y terapéutico de dispepsia y dispepsia funcional: Qué hay nuevo en el 2019? [Diagnostic and therapeutic approach to dyspepsia and functional dyspepsia:what’s new in 2019?]. Rev. Gastroenterol. Peru. 2019, 39, 141–152. [Google Scholar]
- Balta, S.; Demirkol, S.; Unlu, M.; Arslan, Z.; Celik, T. Neutrophil to lymphocyte ratio may be predict of mortality in all conditions. Br. J. Cancer 2013, 109, 3125–3126. [Google Scholar] [CrossRef] [PubMed]
- Mosso, E.; Bonetto, S.; Longobardi, G.; Abenavoli, L.; Ribaldone, D.G.; Saracco, G.M.; Pellicano, R. Management of functional dyspepsia in the year 2020. A clinical point of view. Minerva Gastroenterol. Dietol. 2020. [Google Scholar] [CrossRef]
- Kang, S.J.; Park, B.; Shin, C.M. Helicobacter pylori Eradication Therapy for Functional Dyspepsia: A Meta-Analysis by Region and H. pylori Prevalence. J. Clin. Med. 2019, 8, 1324. [Google Scholar] [CrossRef]
- Liu, C.; Li, X. Stage-Dependent Changes in Albumin, NLR, PLR, and AFR are correlated with Shorter Survival in Patients with Gastric Cancer. Clin. Lab. 2019, 65. [Google Scholar] [CrossRef]
- Jafarzadeh, A.; Akbarpoor, V.; Nabizadeh, M.; Nemati, M.; Rezayati, M.T. Total leukocyte counts and neutrophil-lymphocyte count ratios among Helicobacter pylori-infected patients with peptic ulcers: Independent of bacterial CagA status. Southeast Asian J. Trop. Med. Public Health 2013, 44, 82–88. [Google Scholar]
- Bilge, M.; Yeşilova, A.M.; Adas, M.; Helvaci, A. Neutrophil- and Platelet- to Lymphocyte Ratio in Patients with Euthyroid Hashimoto’s Thyroiditis. Exp. Clin. Endocrinol. Diabetes 2019, 127, 545–549. [Google Scholar] [CrossRef]
- Pacifico, L.; Osborn, J.F.; Tromba, V.; Romaggioli, S.; Bascetta, S.; Chiesa, C. Helicobacter pylori infection and extragastric disorders in children: A critical update. World J. Gastroenterol. 2014, 20, 1379–1401. [Google Scholar] [CrossRef]
- Mendoza, E.; Duque, X.; Franco, J.I.H.; Reyes-Maldonado, E.; Morán, S.; Martínez, G.; Rodríguez, A.S.; Martinez, H. Association between Active H. pylori Infection and Iron Deficiency Assessed by Serum Hepcidin Levels in School-Age Children. Nutrients 2019, 11, 2141. [Google Scholar] [CrossRef]
- Oporto, M.; Pavez, M.; Troncoso, C.; Cerda, A.; Hofmann, E.; Sierralta, A.; Rios, E.; Coppelli, L.; Barrientos, L. Prevalence of Infection and Antibiotic Susceptibility of Helicobacter pylori: An Evaluation in Public and Private Health Systems of Southern Chile. Pathogens 2019, 8, 226. [Google Scholar] [CrossRef] [PubMed]
- Mentis, A.; Lehours, P.; Megraud, F. Epidemiology and Diagnosis of Helicobacter pylori infection. Helicobacter 2015, 20 (Suppl. 1), 1–7. [Google Scholar] [CrossRef]
- Breckan, R.K.; Paulssen, E.J.; Asfeldt, A.M.; Kvamme, J.-M.; Straume, B.; Florholmen, J. The All-Age Prevalence ofHelicobacter pyloriInfection and Potential Transmission Routes. A Population-Based Study. Helicobacter 2016, 21, 586–595. [Google Scholar] [CrossRef]
- Franceschi, F.; Covino, M.; Baudron, C.R. Review: Helicobacter pylori and extragastric diseases. Helicobacter 2019, 24 (Suppl. 1), e12636. [Google Scholar] [CrossRef]
- Mekonnen, H.D.; Fisseha, H.; Getinet, T.; Tekle, F.; Galle, P.R. Helicobacter pylori Infection as a Risk Factor for Hepatocellular Carcinoma: A Case-Control Study in Ethiopia. Int. J. Hepatol. 2018, 2018, 1–7. [Google Scholar] [CrossRef] [PubMed]
- He, C.; Yang, Z.; Lu, N.-H. Helicobacter pyloriinfection and diabetes: Is it a myth or fact. World J. Gastroenterol. 2014, 20, 4607–4617. [Google Scholar] [CrossRef] [PubMed]
- Jia, E.-Z.; Zhao, F.-J.; Hao, B.; Zhu, T.; Wang, L.-S.; Chen, B.; Cao, K.-J.; Huang, J.; Ma, W.-Z.; Yang, Z.; et al. Helicobacter pylori infection is associated with decreased serum levels of high density lipoprotein, but not with the severity of coronary atherosclerosis. Lipids Health Dis. 2009, 8, 59. [Google Scholar] [CrossRef] [PubMed]
- Robinson, K.; White, J.R.; Winter, J.A. Differential inflammatory response to Helicobacter pylori infection: Etiology and clinical outcomes. J. Inflamm. Res. 2015, 8, 137–147. [Google Scholar] [CrossRef] [PubMed]
- Rahtes, A.; Geng, S.; Lee, C.; Li, L. Cellular and molecular mechanisms involved in the resolution of innate leukocyte inflammation. J. Leukoc. Biol. 2018, 104, 535–541. [Google Scholar] [CrossRef] [PubMed]
- Guclu, M.; Agan, A.F. Association of Severity of Helicobacter pylori Infection with Peripheral Blood Neutrophil to Lymphocyte Ratio and Mean Platelet Volume. Euroasian J. Hepato-Gastroenterol. 2017, 7, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Nalbant, A.; Aydin, A. Association of Helicobacter pylori infection with vitamin D, hemogram parameters, and blood group. Turk. J. Acad. Gastroenterol. 2017, 16, 1–5. [Google Scholar]
- Asil, M.; Dertli, R. Neutrophil to lymphocyte ratio is increased in chronic helicobacter pylori infection and returns to normal after successful eradication. J. Turgut Ozal Med. Cent. 2016, 23, 409. [Google Scholar] [CrossRef]
- Krenn-Pilko, S.; Langsenlehner, U.; Thurner, E.-M.; Stojakovic, T.; Pichler, M.; Gerger, A.; Kapp, K.S.; Langsenlehner, T. The elevated preoperative platelet-to-lymphocyte ratio predicts poor prognosis in breast cancer patients. Br. J. Cancer 2014, 110, 2524–2530. [Google Scholar] [CrossRef]
- Zhang, H.; Gao, L.; Zhang, B.; Zhang, L.; Wang, C. Prognostic value of platelet to lymphocyte ratio in non-small cell lung cancer: A systematic review and meta-analysis. Sci. Rep. 2016, 6, 22618. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Cai, J.; Li, H.; Zeng, K.; He, L.; Fu, H.; Zhang, J.; Chen, L.; Yao, J.; Zhang, Y.; et al. Neutrophil to Lymphocyte Ratio and Platelet to Lymphocyte Ratio as Prognostic Predictors for Hepatocellular Carcinoma Patients with Various Treatments: A Meta-Analysis and Systematic Review. Cell. Physiol. Biochem. 2017, 44, 967–981. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Xie, Z.; Liu, X.; Huang, X.; Lin, J.; Huang, D.; Yu, B.; Hou, J. Association of Platelet to lymphocyte ratio with non-culprit atherosclerotic plaque vulnerability in patients with acute coronary syndrome: An optical coherence tomography study. BMC Cardiovasc. Disord. 2017, 17, 175. [Google Scholar] [CrossRef] [PubMed]
- Farah, R.; Khamisy-Farah, R. Association of Neutrophil to Lymphocyte Ratio with Presence and Severity of Gastritis Due to Helicobacter pylori Infection. J. Clin. Lab. Anal. 2014, 28, 219–223. [Google Scholar] [CrossRef]
- Farah, R.; Hamza, H.; Khamisy-Farah, R. A link between platelet to lymphocyte ratio and Helicobacter pylori infection. J. Clin. Lab. Anal. 2018, 32, e22222. [Google Scholar] [CrossRef]
- Shimoyama, Y.; Umegaki, O.; Agui, T.; Kadono, N.; Minami, T. Neutrophil to lymphocyte ratio and platelet to lymphocyte ratio are superior to other inflammation-based prognostic scores in predicting the mortality of patients with gastrointestinal perforation. JA Clin. Rep. 2017, 3, 49. [Google Scholar] [CrossRef]
- Umit, H.; Umit, E.G. Helicobacter pylori and mean platelet volume: A relation way before immune thrombocytopenia? Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 2818–2823. [Google Scholar]
- Burns, M.; Amaya, A.; Bodi, C.; Ge, Z.; Bakthavatchalu, V.; Ennis, K.; Wang, T.C.; Georgieff, M.; Fox, J.G. Helicobacter pylori infection and low dietary iron alter behavior, induce iron deficiency anemia, and modulate hippocampal gene expression in female C57BL/6 mice. PLoS ONE 2017, 12, e0173108. [Google Scholar] [CrossRef]
- Muhsen, K.; Cohen, D. Helicobacter pylori Infection and Iron Stores: A Systematic Review and Meta-analysis. Helicobacter 2008, 13, 323–340. [Google Scholar] [CrossRef]
- Hacihanefioglu, A.; Edebali, F.; Celebi, A.; Karakaya, T.; Senturk, O.; Hulagu, S. Improvement of complete blood count in patients with iron deficiency anemia and Helicobacter pylori infection after the eradication of Helicobacter pylori. Hepatogastroenterology 2004, 51, 313–315. [Google Scholar] [PubMed]
- Fiorini, G.; Bland, J.M.; Hughes, E.; Castelli, V.; Vaira, D. A Systematic Review on Drugs Absorption Modifications after Eradication in Helicobacter pylori Positive Patients undergoing Replacement Therapy. J. Gastrointest. Liver Dis. 2015, 24, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Beard, J.L. Iron biology in immune function, muscle metabolism and neuronal functioning. J. Nutr. 2001, 131, 568S–580S. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| H. pylori | p | |||
|---|---|---|---|---|
| Negative (185) Mean ± sd, n (%) | Positive (263) Mean ± sd, n (%) | |||
| Age (years) | 51.30 ± 14.10 | 47.87 ± 13.98 | a 0.011 * | |
| Gender | Male | 55 (29.7) | 75 (28.5) | c 0.781 |
| Female | 130 (70.3) | 188 (71.5) | ||
| HGB (g/dL) | 12.66 ± 1.56 | 12.59 ± 1.67 | b 0.501 | |
| MCV (fL) | 87.57 ± 6.85 | 86.55 ± 7.57 | b 0.185 | |
| Leukocyte (µL) | 682.70 ± 1607.57 | 6944.12 ± 1973.45 | b 0.647 | |
| Neutrophil (µL) | 3781.03 ± 1273.28 | 3995.82 ± 1555.09 | b 0.278 | |
| Lymphocyte (µL) | 2278.65 ± 580.43 | 2300.87 ± 1013.54 | b 0.373 | |
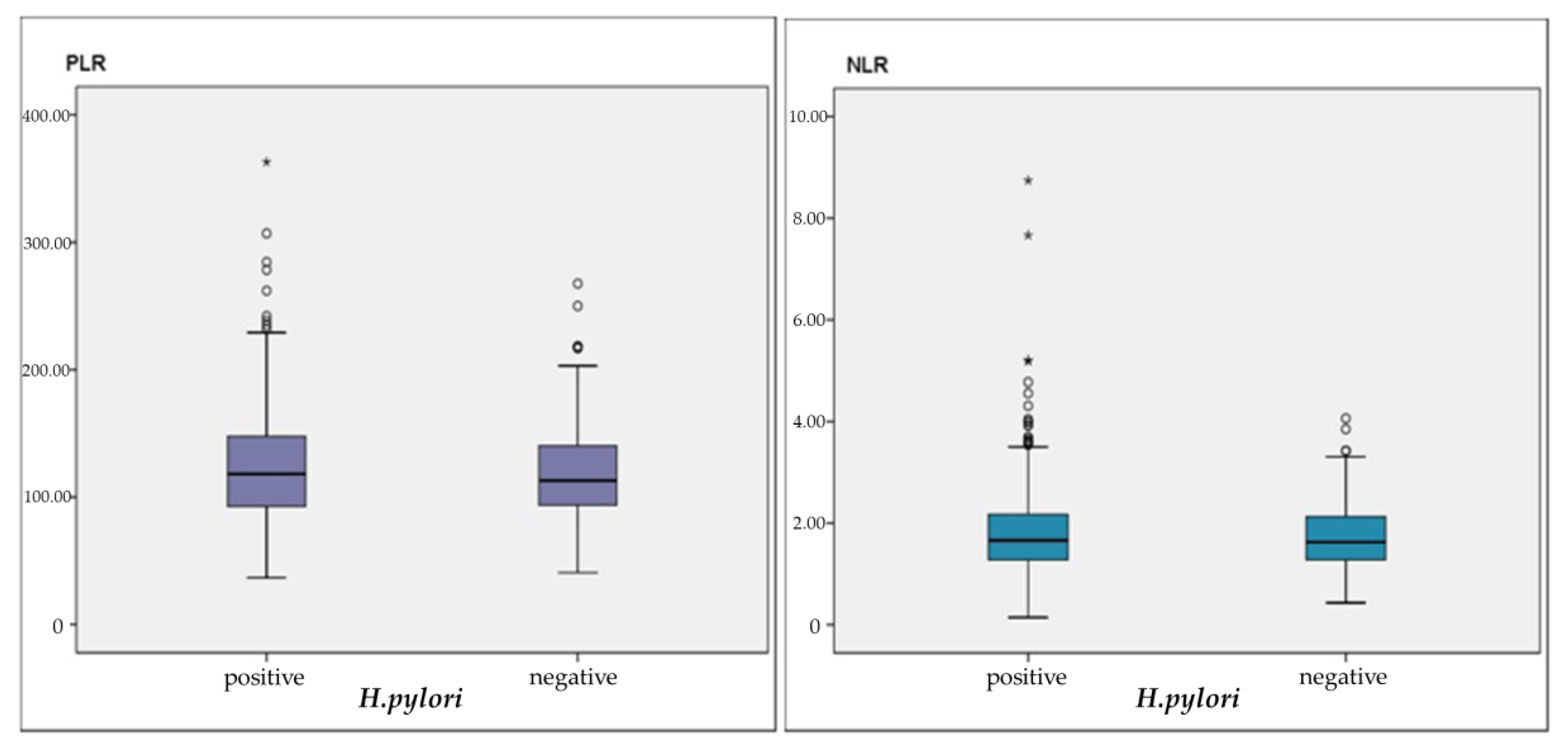
| NLR (%) | 1.74 ± 0.65 | 1.92 ± 1.00 | b 0.338 | |
| PLR (%) | 118.91 ± 38.66 | 125.59 ± 47.42 | b 0.237 | |
| Platelet (µL) | 258,718.92 ± 66,735.34 | 264,551.33 ± 75,162.24 | b 0.502 | |
| Iron (µg/dL) | 67.28 ± 39.82 | 56.45 ± 33.64 | b 0.029 * | |
| TIBC (µg/dL) | 356.01 ± 60.33 | 363.94 ± 60.20 | b 0.268 | |
| Ferritin (ng/mL) | 36.04 ± 42.36 | 30.11 ± 52.80 | b 0.003 ** | |
| B12 (pg/mL) | 268.77 ± 158.22 | 278.53 ± 186.21 | b 0.859 | |
| Folic acid (ng/mL) | 8.72 ± 4.15 | 7.27 ± 2.77 | b 0.081 | |
| CRP (mg/L) | 6.04 ± 6.22 | 5.28 ± 4.48 | b 0.530 | |
| Intestinal metaplasia | 26 (14.1) | 48 (18.3) | c 0.239 | |
| Atrophy | 6 (3.2) | 18 (6.8) | c 0.096 | |
| Gastritis | 156 (84.3) | 219 (83.3) | c 0.766 | |
| Gastric ulcer | 31 (16.8) | 45 (17.1) | c 0.933 | |
| Duodenal ulcer | 14 (7.6) | 27 (10.3) | c 0.329 | |
| Esophagitis | 49 (26.5) | 77 (29.3) | c 0.518 | |
| N | NLR | PLR | |||
|---|---|---|---|---|---|
| R | p | R | p | ||
| Age (years) | 263 | 0.020 | 0.743 | 0.054 | 0.386 |
| HGB | 263 | −0.133 | 0.031 * | −0.310 | 0.001 ** |
| MCV | 263 | −0.084 | 0.173 | −0.187 | 0.002 ** |
| Leukocyte (µL) | 263 | 0.302 | 0.001 ** | −0.144 | 0.020 * |
| Neutrophil (µL) | 263 | 0.644 | 0.001 ** | 0.064 | 0.301 |
| Lymphocyte (µL) | 263 | −0.596 | 0.001 ** | −0.622 | 0.001 ** |
| Platelet (µL) | 263 | 0.032 | 0.606 | 0.502 | 0.001 ** |
| Iron (µg/dL) | 131 | −0.270 | 0.002 ** | −0.335 | 0.001 ** |
| TIBC (µg/dL) | 129 | 0.016 | 0.853 | 0.072 | 0.416 |
| Ferritin (ng/mL) | 175 | −0.162 | 0.032 * | −0.290 | 0.001 ** |
| B12 (pg/mL) | 177 | −0.035 | 0.644 | −0.013 | 0.861 |
| Folic acid (ng/mL) | 81 | −0.078 | 0.490 | 0.066 | 0.561 |
| CRP (mg/L) | 52 | 0.006 | 0.967 | −0.085 | 0.548 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boyuk, B.; Saydan, D.; Mavis, O.; Erman, H. Evaluation of Helicobacter pylori Infection, Neutrophil–Lymphocyte Ratio and Platelet–Lymphocyte Ratio in Dyspeptic Patients. Gastroenterol. Insights 2020, 11, 2-9. https://doi.org/10.3390/gastroent11010002
Boyuk B, Saydan D, Mavis O, Erman H. Evaluation of Helicobacter pylori Infection, Neutrophil–Lymphocyte Ratio and Platelet–Lymphocyte Ratio in Dyspeptic Patients. Gastroenterology Insights. 2020; 11(1):2-9. https://doi.org/10.3390/gastroent11010002
Chicago/Turabian StyleBoyuk, Banu, Dogukan Saydan, Osman Mavis, and Hande Erman. 2020. "Evaluation of Helicobacter pylori Infection, Neutrophil–Lymphocyte Ratio and Platelet–Lymphocyte Ratio in Dyspeptic Patients" Gastroenterology Insights 11, no. 1: 2-9. https://doi.org/10.3390/gastroent11010002
APA StyleBoyuk, B., Saydan, D., Mavis, O., & Erman, H. (2020). Evaluation of Helicobacter pylori Infection, Neutrophil–Lymphocyte Ratio and Platelet–Lymphocyte Ratio in Dyspeptic Patients. Gastroenterology Insights, 11(1), 2-9. https://doi.org/10.3390/gastroent11010002