
Effectiveness of a Cognitive Stimulation Program in Older Adults with Mild Neurocognitive Disorder: Insights from fNIRS Analysis in a Randomized Controlled Trial

 ,
,  ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Intervention
2.3. Instruments
2.4. Functional Study of the Prefrontal Cortex with fNIRS
2.5. Data Analysis
3. Results
3.1. Sociodemographic and Clinical Characteristics
3.2. Results in Behavioral and Cognitive Dimensions
3.2.1. Mini-Mental State Examination (MMSE)
3.2.2. Frontal Assessment Battery (FAB)
3.2.3. Geriatric Depression Scale-15 (GDS-15)
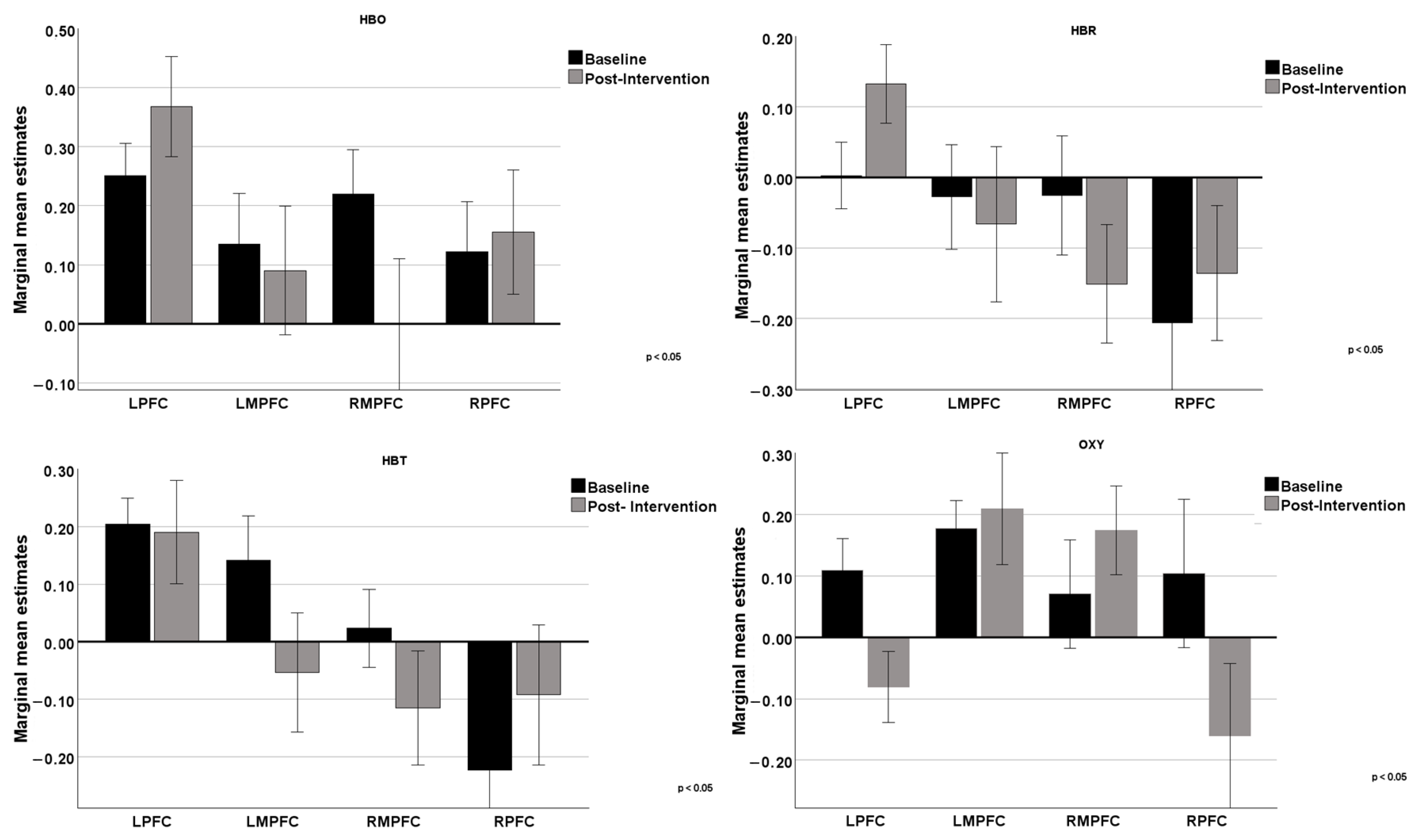
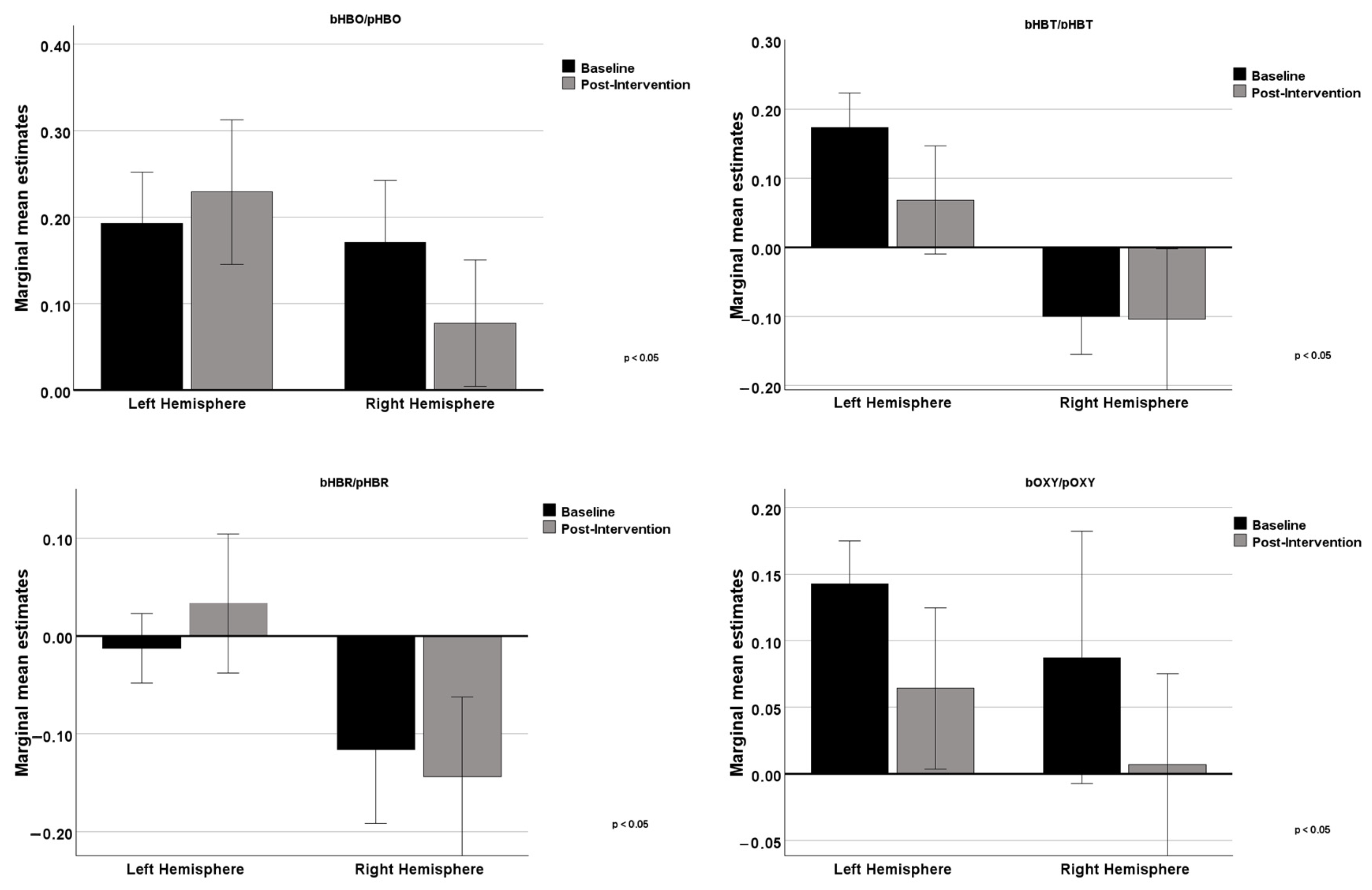
3.3. Results of Prefrontal Cortex Oxygenation in the Intervention Group
3.4. Adherence to Intervention
3.5. Degree of Collaboration During the Intervention
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations Department of Economic and Social Affairs, Population Division 2024. World Population Prospects 2024: Summary of Results. Available online: https://www.un.org/development/desa/pd/sites/www.un.org.development.desa.pd/files/undesa_pd_2024_wpp_2024_advance_unedited_0.pdf (accessed on 14 December 2024).
- United Nations Department of Economic and Social Affairs, Population Division 2023. World Population Ageing 2023: Challenges and Opportunities of Population Ageing in the Least Developed Countries. Available online: https://www.un.org/development/desa/pd/sites/www.un.org.development.desa.pd/files/undesa_pd_2024_wpa2023-report.pdf (accessed on 14 December 2024).
- Hascup, E.R.; Hascup, K.N. Does SARS-CoV-2 infection cause chronic neurological complications? GeroScience 2020, 42, 1083–1087. [Google Scholar] [CrossRef] [PubMed]
- Alnefeesi, Y.; Siegel, A.; Lui, L.M.W.; Teopiz, K.M.; Ho, R.C.M.; Lee, Y.; Nasri, F.; Gill, H.; Lin, K.; Cao, B.; et al. Impact of SARS-CoV-2 Infection on Cognitive Function: A Systematic Review. Front. Psychiatry 2021, 11, 621773. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association (APA). Diagnostic Statistical Manual of Mental Disorders, 5th ed.; APA: Arlington County, VA, USA, 2022. [Google Scholar] [CrossRef]
- Kales, H.C.; Gitlin, L.N.; Lyketsos, C.G. Management of neuropsychiatric symptoms of dementia in clinical settings: Recommendations from a multidisciplinary expert panel. J. Am. Geriatr. Soc. 2014, 62, 762–769. [Google Scholar] [CrossRef] [PubMed]
- Gitlin, L.N.; Winter, L.; Dennis, M.P.; Hodgson, N.; Hauck, W.W. Targeting and managing behavioral symptoms in individuals with dementia: A randomized trial of a nonpharmacological intervention. J. Am. Geriatr. Soc. 2010, 58, 1465–1474. [Google Scholar] [CrossRef] [PubMed]
- Guerchet, M.; Prince, M.; Prina, M. Numbers of People with Dementia Around the World. 2020. Available online: https://www.alzint.org/resource/numbers-of-people-with-dementia-worldwide/ (accessed on 6 January 2025).
- Livingston, G.; Sommerlad, A.; Orgeta, V.; Costafreda, S.G.; Huntley, J.; Ames, D.; Ballard, C.; Banerjee, S.; Burns, A.; Cohen-Mansfield, J.; et al. Dementia prevention, intervention, and care. Lancet 2017, 390, 2673–2734. [Google Scholar] [CrossRef] [PubMed]
- Orgeta, V.; Mukadam, N.; Sommerlad, A.; Livingston, G. The lancet commission on dementia prevention, intervention, and care: A call for action. Ir. J. Psychol. Med. 2019, 36, 85–88. [Google Scholar] [CrossRef] [PubMed]
- Yeung, M.K.; Chan, A.S. Functional near-infrared spectroscopy reveals decreased resting oxygenation levels and task-related oxygenation changes in mild cognitive impairment and dementia: A systematic review. J. Psychiatr. Res. 2020, 124, 58–76. [Google Scholar] [CrossRef] [PubMed]
- Pereira, T.; Castro, M.A.; Villafaina, S.; Carvalho Santos, A.; Fuentes-García, J.P. Dynamics of the prefrontal cortex during chess-based problem-solving tasks in competition-experienced chess players: An fNIR study. Sensors 2020, 20, 3917. [Google Scholar] [CrossRef] [PubMed]
- Jobson, D.D.; Hase, Y.; Clarkson, A.N.; Kalaria, R.N. The role of the medial prefrontal cortex in cognition, ageing and dementia. Brain Commun. 2021, 3, fcab125. [Google Scholar] [CrossRef] [PubMed]
- Teo, W.; Rantalainen, T.; Nuzum, N.; Valente, L.; Macpherson, H. Altered prefrontal cortex responses in older adults with subjective memory complaints and dementia during dual-task gait: An fNIRS study. Eur. J. Neurosci. 2021, 53, 1324–1333. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.L.; Wagner, J.; Heugel, N.; Sugar, J.; Lee, Y.W.; Conant, L.; Malloy, M.; Heffernan, J.; Quirk, B.; Zinos, A.; et al. Functional near-infrared spectroscopy and its clinical application in the field of neuroscience: Advances and future directions. Front. Neurosci. 2020, 14, 724. [Google Scholar] [CrossRef] [PubMed]
- Clare, L.; Woods, R.T. Cognitive training and cognitive rehabilitation for people with early-stage Alzheimer’s disease: A review. Neuropsychol. Rehabil. 2004, 14, 385–401. [Google Scholar] [CrossRef]
- Olazarán, J.; Reisberg, B.; Clare, L.; Cruz, I.; Peña-Casanova, J.; del Ser, T.; Woods, B.; Beck, C.; Auer, S.; Lai, C.; et al. Nonpharmacological therapies in Alzheimer’s disease: A systematic review of efficacy. Dement. Geriatr. Cogn. Disord. 2010, 30, 161–178. [Google Scholar] [CrossRef] [PubMed]
- Silva, R.; Bobrowicz-Campos, E.; Cardoso, D.; Costa, P.; Couto, F.; Camarneiro, A.P.; Abrunheiro, S.; Almeida, M.; Apóstolo, J. Effects of caregiver-provided individual cognitive interventions on cognition, social functioning and quality of life in older adults with major neurocognitive disorders: A systematic review. JBI Evid. Synth. 2020, 18, 743–806. [Google Scholar] [CrossRef] [PubMed]
- Woods, B.; Rai, H.K.; Elliott, E.; Aguirre, E.; Orrell, M.; Spector, A. Cognitive stimulation to improve cognitive functioning in people with dementia. Cochrane Database Syst. Rev. 2023, 2, CD005562. [Google Scholar] [CrossRef]
- Justo-Henriques, S.I. Individual intervention protocol based on cognitive stimulation therapy for older adults with mild neurocognitive disorder. Rev. Enferm. Ref. 2021, 5, e20100. [Google Scholar] [CrossRef]
- Justo-Henriques, S.I.; Marques-Castro, A.E.; Otero, P.; Vázquez, F.; Torres, Á.J. Long-term individual cognitive stimulation program in patients with mild neurocognitive disorder: A pilot study. Rev. Neurol. 2019, 68, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Justo-Henriques, S.I.; Otero, P.; Torres, A.J.; Vázquez, F.L. Effect of long-term individual cognitive stimulation program for people with mild neurocognitive disorder. Rev. Neurol. 2021, 73, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Silva, R.; Santos-Costa, P.; Bobrowicz-Campos, E.; Gil, I.; Cardoso, D.; Apóstolo, J. Individual cognitive stimulation in people with dementia: Good practices. In International Workshop on Gerontechnology; Springer Nature: Cham, Switzerland, 2022; pp. 92–101. [Google Scholar]
- Boutron, I.; Altman, D.G.; Moher, D.; Schulz, K.F.; Ravaud, P. CONSORT Statement for Randomized Trials of Nonpharmacologic Treatments: A 2017 Update and a CONSORT Extension for Nonpharmacologic Trial Abstracts. Ann. Intern. Med. 2017, 167, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Schulz, K.F.; Altman, D.G.; Moher, D.; the CONSORT Group. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. BMC Med. 2010, 8, 18. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Guerreiro, M.; Silva, A.P.; Botelho, M.A.; Leitão, O.; Castro-Caldas, A.; Garcia, C. Adaptação à população portuguesa da tradução do “Mini Mental State Examination” (MMSE) [Adaptation to the Portuguese population of the translated “Mini Mental State Examination” (MMSE)]. Rev. Port. Neurol. 1994, 1, 9–10. [Google Scholar]
- Morgado, J.; Rocha, C.S.; Maruta, C.; Guerreiro, M.; Martins, I.P. Novos valores normativos do Mini-Mental State Examination [New normative values of Mini-Mental State Examination]. Sinapse 2009, 2, 10–16. [Google Scholar]
- Dubois, B.; Slachevsky, A.; Litvan, I.; Pillon, B. The FAB: A frontal assessment battery at bedside. Neurology 2000, 55, 1621–1626. [Google Scholar] [CrossRef] [PubMed]
- Lima, C.F.; Meireles, L.P.; Fonseca, R.; Castro, S.L.; Garrett, C. The frontal assessment battery (FAB) in Parkinson’s disease and correlations with formal measures of executive functioning. J. Neurol. 2008, 255, 1756–1761. [Google Scholar] [CrossRef] [PubMed]
- Yesavage, J.A.; Brinck, R.L.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and validation of a geriatric depression screening scale: A preliminary report. J. Psychiatr. Res. 1983, 17, 37–49. [Google Scholar] [CrossRef] [PubMed]
- Apóstolo, J.L.; Loureiro, L.M.J.; Carvalho, I.A.; Alves, I.; Batista, D.F.; Sfetcu, R. Contribuição para a adaptação da Geriatric Depression Scale −15 para a língua portuguesa [Contribution to the adaptation of the Geriatric Depression Scale −15 into Portuguese]. Rev. Enferm. Ref. 2014, 3, 65–73. [Google Scholar] [CrossRef]
- Apóstolo, J.L.A.; Bobrowicz-Campos, E.M.; Carvalho dos Reis, I.A.; Henriques, S.J.; Veiga Correia, C.A. Exploring a capacity to screen of the European Portuguese version of the 15-item geriatric depression scale. Rev. Psicopatología Psicol. Clínica 2018, 23, 99–107. [Google Scholar] [CrossRef]
- Justo-Henriques, S.I.; Pérez-Sáez, E.; Carvalho, J.O.; Bobrowicz-Campos, E.; Apóstolo, J.L.A.; Otero, P.; Vázquez, F.L. Reliability and validity of the Geriatric Depression Scale in a sample of Portuguese older adults with mild-to-moderate cognitive impairmental. Brain Sci. 2023, 13, 1160. [Google Scholar] [CrossRef] [PubMed]
- Ayaz, H. Analytical Software and Stimulus-Presentation Platform to Utilize, Visualize and Analyze Near-Infrared Spectroscopy Measures. Master’s Thesis, Drexel University, Philadelphia, PA, USA, 2005. [Google Scholar]
- Liang, L.-Y.; Shewokis, P.A.; Getchell, N. Brain activation in the prefrontal cortex during motor and cognitive tasks in adults. J. Behav. Brain Sci. 2016, 6, 463–474. [Google Scholar] [CrossRef]
- Dolu, N.; Altınkaynak, M.; Güven, A.; Özmen, S.; Demirci, E.; İzzetoğlu, M.; Pektaş, F. Effects of methylphenidate treatment in children with ADHD: A multimodal EEG/fNIRS approach. Psychiatry Clin. Psychopharmacol. 2019, 29, 285–292. [Google Scholar] [CrossRef]
- Pinti, P.; Scholkmann, F.; Hamilton, A.; Burgess, P.W.; Tachtsidis, I. Current status and issues regarding pre-processing of fNIRS neuroimaging data: An investigation of diverse signal filtering methods within a general linear model framework. Front. Hum. Neurosci. 2019, 12, 505. [Google Scholar] [CrossRef] [PubMed]
- Wong, Y.L.; Cheng, C.P.W.; Wong, C.S.M.; Wong, S.N.; Wong, H.L.; Tse, S.; Wong, G.H.Y.; Chan, W.C. Cognitive stimulation for Persons with dementia: A systematic review and meta-analysis. East Asian Arch. Psychiatry 2021, 31, 55–66. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.; Kim, D.; Kim, S.; Kim, H.J.; Chung, U.S.; Lee, J.J. Cognitive training based on functional near-infrared spectroscopy neurofeedback for the elderly with mild cognitive impairment: A preliminary study. Front. Aging Neurosci. 2023, 15, 1168815. [Google Scholar] [CrossRef] [PubMed]
- Kassab, A.; Le Lan, J.; Tremblay, J.; Vannasing, P.; Dehbozorgi, M.; Pouliot, P.; Gallagher, A.; Lesage, F.; Sawan, M.; Nguyen, D.K. Multichannel wearable fNIRS-EEG system for long-term clinical monitoring. Hum. Brain Mapp. 2018, 39, 7–23. [Google Scholar] [CrossRef] [PubMed]
- Miguel, H.O.; Condy, E.E.; Nguyen, T.; Zeytinoglu, S.; Blick, E.; Bress, K.; Khaksari, K.; Dashtestani, H.; Millerhagen, J.; Shahmohammadi, S.; et al. Cerebral hemodynamic response during a live action-observation and action-execution task: A fNIRS study. PLoS ONE 2021, 16, e0253788. [Google Scholar] [CrossRef] [PubMed]
- Binder, J.R.; Desai, R.H.; Graves, W.W.; Conant, L.L. Where is the semantic system? A critical review and meta-analysis of 120 functional neuroimaging studies. Cereb. Cortex 2009, 19, 2767–2796. [Google Scholar] [CrossRef] [PubMed]
- Fedorenko, E.; Thompson-Schill, S.L. Reworking the language network. Trends Cogn. Sci. 2014, 18, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Gluhm, S.; Goldstein, J.; Loc, K.; Colt, A.; Liew, C.; Van Corey-Bloom, J. Cognitive performance on the Mini-Mental State Examination and the Montreal Cognitive Assessment across the healthy adult lifespan. Cogn. Behav. Neurol. 2013, 26, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Justo-Henriques, S.I.; Pérez-Sáez, E.; Carvalho, J.O.; Lemos, R.; Ribeiro, O. Effects of an individual cognitive stimulation intervention on global cognition, memory, and executive function in older adults with mild to moderate Alzheimer’s disease. Clin. Neuropsychol. 2024, 1–9. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Duration. | Contents | Materials and Activities |
|---|---|---|
| 5 min | Start of session | Greeting Mood assessment Session agenda |
| 10 min | Orientation | Temporal and physical orientation |
| 25 min | Stimulation of cognitive domains | Scheduled main session activities (presented in digital format via Microsoft PowerPoint) covering six themes: - Portuguese language (identify missing letters in words, synonyms or associated words, alphabetize, memorize words (timed), develop a related theme); - Mathematics (calculations, memorize results or numbers (timed), simulate purchase transactions, sort numbers); - Daily activities (naming objects, timed memorization of objects, comparing utensils, categorizing (e.g., clothing, footwear, food, medication, technical aids, personal hygiene products, kitchen utensils, and rooms in a house)); - The past (identify, name, and associate images from the present and the past, such as modes of transportation, appliances, housing, media, professions, clothing, celebrities, politics, regional and local references, identify similarities and differences, memorize (timed) past historical images; - Fruit (identify fruits through images or riddles, memorize (timed) the fruits presented and their sequence, associate fruits with the harvest seasons, associate fruits with other products derived from them, associate images of fruits with words); - Sounds (associating sounds with images, memorizing (timed) sounds and sequences, associating musical themes with interpreters; identifying names of musical themes; associating musical themes with geographical areas, such as cities, regions, archipelagos; identifying and counting words in a musical theme). |
| 5 min | End of session | Processing and debriefing Session evaluation Closing |
| Overall Sample (N = 36) | iCS Group (n = 18) | Control Group (n = 18) | t, χ2 | Fisher Exact Test | p-Value | d, φ, U | |
|---|---|---|---|---|---|---|---|
| Age in years, Mean (SD) [range] | 75.3 (7.81) [65–90] | 74.8 (7.76) [65–84] | 75.8 (8.05) [65–90] | t = −0.38 | 0.719 | U = 174.00 | |
| Gender (%) | |||||||
| Male | 11 (30.6) | 6 (33.3) | 5 (27.8) | χ2 = 0.13 | 0.717 | φ = 0.06 | |
| Female | 25 (69.4) | 12 (66.7) | 13 (72.2) | ||||
| Educational level (%) | |||||||
| 1 to 4 years | 28 (77.8) | 13 (72.2) | 15 (83.3) | 0.570 | φ = 0.31 | ||
| 5 to 6 years | 2 (5.6) | 2 (11.1) | 0 (0) | ||||
| 7 to 11 years | 1 (2.8) | 1 (5.6) | 0 (0) | ||||
| more 11 years | 5 (13.9) | 2 (11.1) | 3 (16.7) | ||||
| Marital status (%) | |||||||
| No partner | 20 (55.6) | 11 (61.1) | 9 (50) | χ2 = 0.45 | 0.502 | φ = 0.11 | |
| With partner | 16 (44.4) | 7 (38.9) | 9 (50) | ||||
| Household members (%) | |||||||
| Alone | 13 (36.1) | 7 (38.9) | 6 (33.3) | χ2 = 0.17 | 0.920 | φ = 0.07 | |
| Spouse | 12 (33.3) | 6 (33.3) | 6 (33.3) | ||||
| With relatives | 11 (30.6) | 5 (27.8) | 6 (33.3) | ||||
| Type of social care institution attended (%) | |||||||
| Day care | 12 (33.3) | 7 (38.9) | 5 (27.8) | χ2 = 0.50 | 0.480 | φ = 0.12 | |
| None | 24 (66.7) | 11 (61.1) | 13 (72.2) | ||||
| Clinical condition (%) | |||||||
| mNCD_Alzheimer disease | 16 (44.4) | 9 (50) | 7 (38.9) | 0.738 | φ = 0.25 | ||
| mNCD_TBI | 1 (2.8) | 0 (0) | 1 (5.6) | ||||
| mNCD_FTD | 1 (2.8) | 0 (0) | 1 (5.6) | ||||
| None | 18 (50) | 9 (50) | 9 (50) | ||||
| Outcome | |||||||
| MMSE score, Mean (SD) [range] | 26.86 (2.10) [23–30] | 26.50 (2.26) [23–30] | 27.22 (1.93) [24–30] | t = −1.03 | 0.309 | d = −0.34 | |
| FAB score, Mean (SD) [range] | 10.44 (2.72) [6–17] | 10.39 (2.95) [6–17] | 10.50 (2.55) [7–15] | t = −0.12 | 0.905 | d = −0.04 | |
| GDS-15 score, Mean (SD) [range] | 7.03 (3.17) [0–12] | 6.89 (3.25) [1–12] | 7.17 (3.17) [0–12] | t = −0.26 | 0.797 | d = −0.09 |
| iCS (n = 18) | Control (n =17) | Group × Time | Pairwise Comparisons | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| T0 Mean (SD) | T1 Mean (SD) | T0 Mean (SD) | T1 Mean (SD) | F | p-Value | ηp2 | T0 | T1 | iCS | Control | |
| iCS vs. Control | iCS vs Control | T0 vs. T1 | T0 vs. T1 | ||||||||
| MMSE | 26.50 (2.26) | 28.56 (1.29) | 27.24 (1.99) | 26.59 (2.29) | 20.103 | <0.001 | 0.379 | 0.315 | 0.003 | <0.001 | 0.144 |
| FAB | 10.39 (2.95) | 12.94 (2.94) | 10.65 (2.55) | 9.41 (3.04) | 30.153 | <0.001 | 0.477 | 0.784 | 0.001 | <0.001 | 0.018 |
| FAB subtests: | |||||||||||
| Conceptualization | 0.94 (0.54) | 1.83 (0.92) | 1.53 (0.94) | 1.47 (0.80) | 11.406 | 0.002 | 0.257 | 0.030 | 0.224 | <0.001 | 0.772 |
| Mental flexibility | 2.39 (0.92) | 2.33 (0.77) | 2.06 (0.66) | 1.53 (0.87) | 3.771 | 0.061 | 0.103 | ||||
| Motor programming | 1.56 (0.86) | 2.06 (0.73) | 1.65 (0.93) | 1.29 (0.59) | 6.482 | 0.016 | 0.164 | 0.764 | 0.002 | 0.040 | 0.151 |
| Sensitivity to interference | 1.78 (1.22) | 2.11 (0.96) | 2.00 (1.17) | 1.24 (0.97) | 7.720 | 0.009 | 0.190 | 0.586 | 0.011 | 0.235 | 0.011 |
| Inhibitory control | 0.83 (1.04) | 1.83 (0.99) | 0.47 (0.87) | 1.41 (0.94) | 0.027 | 0.870 | 0.001 | ||||
| Environmental autonomy | 2.89 (0.32) | 2.78 (0.43) | 2.94 (0.24) | 2.47 (0.51) | 4.653 | 0.038 | 0.124 | 0.594 | 0.063 | 0.346 | <0.001 |
| GDS-15 | 6.89 (3.25) | 4.67 (2.85) | 6.94 (3.11) | 7.29 (3.02) | 18.945 | <0.001 | 0.365 | 0.962 | 0.012 | <0.001 | 0.411 |
| Attendance | n = 18 |
|---|---|
| Sessions attended | |
| Mean (SD) | 23.83 (0.51) |
| Number of sessions attended (%) | |
| From 0 to 20 | 0 (0.0) |
| From 21 to 22 | 1 (5.6) |
| From 23 to 24 | 17 (94.4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Justo-Henriques, S.I.; Silva, R.C.G.; Carvalho, J.O.; Apóstolo, J.L.A.; Nogueira, D.; Pereira, T.A.S. Effectiveness of a Cognitive Stimulation Program in Older Adults with Mild Neurocognitive Disorder: Insights from fNIRS Analysis in a Randomized Controlled Trial. Neurol. Int. 2025, 17, 108. https://doi.org/10.3390/neurolint17070108
Justo-Henriques SI, Silva RCG, Carvalho JO, Apóstolo JLA, Nogueira D, Pereira TAS. Effectiveness of a Cognitive Stimulation Program in Older Adults with Mild Neurocognitive Disorder: Insights from fNIRS Analysis in a Randomized Controlled Trial. Neurology International. 2025; 17(7):108. https://doi.org/10.3390/neurolint17070108
Chicago/Turabian StyleJusto-Henriques, Susana I., Rosa C. G. Silva, Janessa O. Carvalho, João L. A. Apóstolo, Débora Nogueira, and Telmo A. S. Pereira. 2025. "Effectiveness of a Cognitive Stimulation Program in Older Adults with Mild Neurocognitive Disorder: Insights from fNIRS Analysis in a Randomized Controlled Trial" Neurology International 17, no. 7: 108. https://doi.org/10.3390/neurolint17070108
APA StyleJusto-Henriques, S. I., Silva, R. C. G., Carvalho, J. O., Apóstolo, J. L. A., Nogueira, D., & Pereira, T. A. S. (2025). Effectiveness of a Cognitive Stimulation Program in Older Adults with Mild Neurocognitive Disorder: Insights from fNIRS Analysis in a Randomized Controlled Trial. Neurology International, 17(7), 108. https://doi.org/10.3390/neurolint17070108