

Non-Verbal Working Memory in Post-Stroke Motor Aphasia: A Pilot Study Using the Tactual Span


Abstract
1. Introduction
2. Method
2.1. Participants
2.2. Instruments
2.2.1. Confirmation of Aphasia Diagnosis
Bedside Western Aphasia Battery
2.2.2. Assessment of General Intellectual Ability
Raven’s Colored Progressive Matrices Test (RCPMT)
2.2.3. Assessment of WM
Tactual Span—One Hand
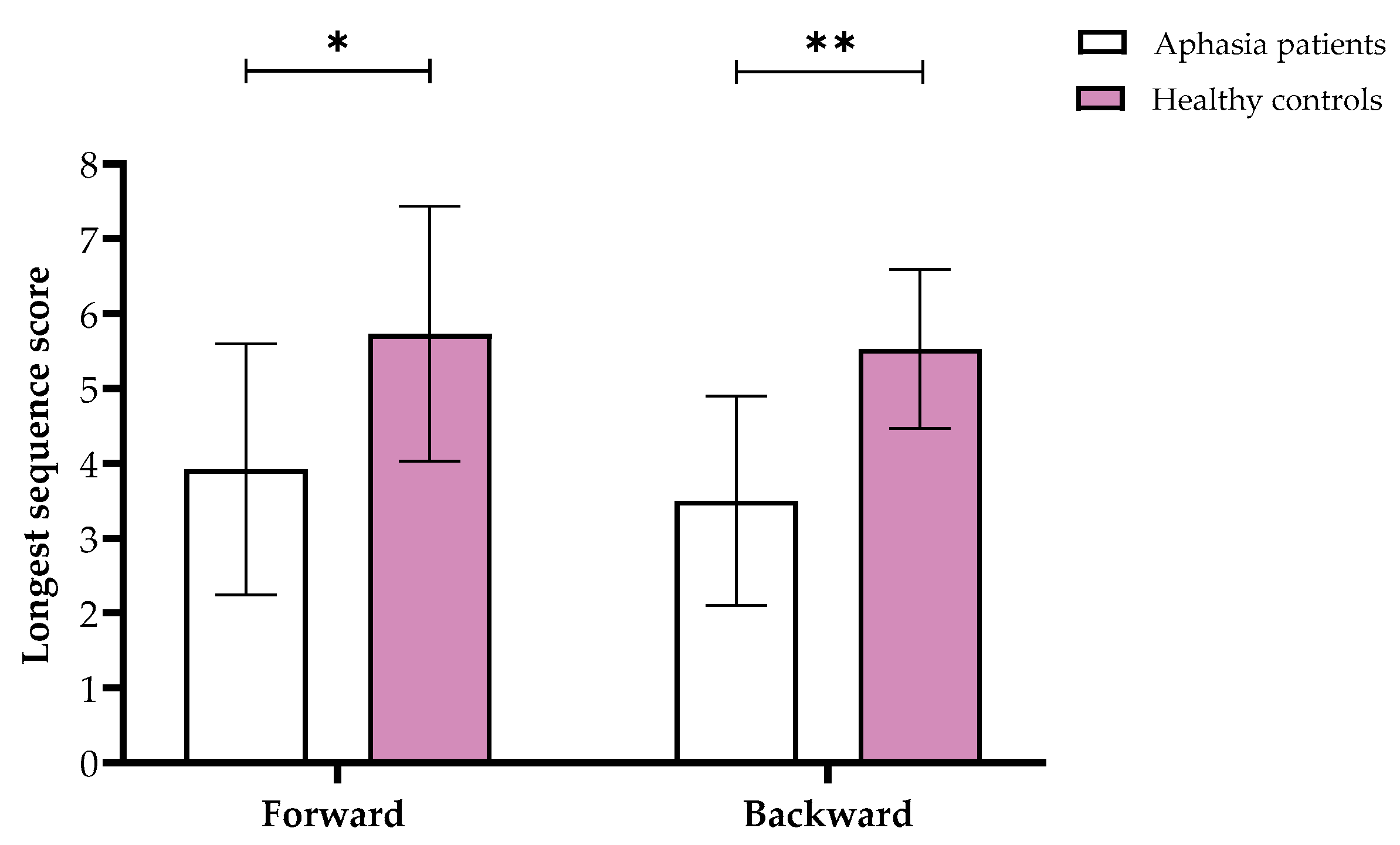
Visuospatial Span
1-Back Task
2.3. Procedure
2.4. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| Variable | Aphasia Patients | Control Group | ||
| Shapiro–Wilk | df | Shapiro–Wilk | df | |
| Tactual Span forward | 0.88 | 14 | 0.89 | 15 |
| Visuospatial Span forward | 0.93 | 14 | 0.94 | 15 |
| Tactual Span backward | 0.93 | 14 | 0.95 | 15 |
| Visuospatial Span backward | 0.91 | 14 | 0.87 | 15 |
| 1-Back task | 0.97 | 14 | 0.88 | 15 |
| Note: df = degrees of freedom. | ||||
References
- Fonseca, J.; Ferreira, J.J.; Pavão Martins, I. Cognitive performance in aphasia due to stroke: A systematic review. Int. J. Disabil. Hum. Dev. 2017, 16, 127–139. [Google Scholar] [CrossRef]
- Kasselimis, D.S. Working Memory and Aphasia. Int. J. Neurol. Res. 2015, 1, 188–190. [Google Scholar] [CrossRef]
- Yao, J.; Liu, X.; Liu, Q.; Wang, J.; Ye, N.; Lu, X.; Zhao, Y.; Chen, H.; Han, Z.; Yu, M.; et al. Characteristics of Non-linguistic Cognitive Impairment in Post-stroke Aphasia Patients. Front. Neurol. 2020, 11, 1038. [Google Scholar] [CrossRef] [PubMed]
- Ardila, A.; Bernal, B.; Rosselli, M. Why Broca’s Area Damage Does Not Result in Classical Broca’s Aphasia. Front. Hum. Neurosci. 2016, 10, 249. [Google Scholar] [CrossRef] [PubMed]
- Berthier, M.L. Poststroke aphasia: Epidemiology, pathophysiology and treatment. Drugs Aging 2005, 22, 163–182. [Google Scholar] [CrossRef]
- McNeil, M.R.; Pratt, S.R. Defining aphasia: Some theoretical and clinical implications of operating from a formal definition. Aphasiology 2001, 15, 901–911. [Google Scholar] [CrossRef]
- Potagas, C.; Kasselimis, D.; Evdokimidis, I. Short-term and working memory impairments in aphasia. Neuropsychologia 2011, 49, 2874–2878. [Google Scholar] [CrossRef]
- Ardila, A.; Rubio-Bruno, S. Aphasia from the inside: The cognitive world of the aphasic patient. Appl. Neuropsychol. Adult 2018, 25, 434–440. [Google Scholar] [CrossRef]
- Christensen, S.C.; Wright, H.H.; Ratiu, I. Working memory in aphasia: Peeling the onion. J. Neurolinguistics 2018, 48, 117–132. [Google Scholar] [CrossRef]
- Mole, J.A.; Demeyere, N. The relationship between early post-stroke cognition and longer term activities and participation: A systematic review. Neuropsychol. Rehabil. 2020, 30, 346–370. [Google Scholar] [CrossRef]
- Murray, L.; Salis, C.; Martin, N.; Dralle, J. The use of standardised short-term and working memory tests in aphasia research: A systematic review. Neuropsychol. Rehabil. 2018, 28, 309–351. [Google Scholar] [CrossRef] [PubMed]
- Baddeley, A.D. Developing the concept of working memory: The role of neuropsychology. Arch. Clin. Neuropsychol. 2021, 36, 861–873. [Google Scholar] [CrossRef] [PubMed]
- Shahouzaie, N.; Farzadfar, M.T.; Jamali, J.; Sobhani-Rad, D. The impact of subcortical stroke-related aphasia on executive functions and working memory: Subcortical aphasia affects executive functions and working memory. Appl. Neuropsychol. Adult 2023, 32, 412–418. [Google Scholar] [CrossRef] [PubMed]
- Van Ede, F.; Nobre, A.C. Turning Attention Inside Out: How Working Memory Serves Behavior. Annu. Rev. Psychol. 2023, 74, 137–165. [Google Scholar] [CrossRef]
- Diamond, A. Understanding Executive Functions: What Helps or Hinders Them and How Executive Functions and Language Development Mutually Support One Another. Perspect. Lang. Lit. 2014, 40, 7–11. [Google Scholar]
- Vernucci, S.; Aydmune, Y.; Andrés, M.L.; Burin, D.I.; Canet-Juric, L. Working memory and fluid intelligence predict reading comprehension in school-age children: A one-year longitudinal study. Appl. Cogn. Psychol. 2021, 35, 1115–1124. [Google Scholar] [CrossRef]
- Mayer, J.F.; Murray, L.L. Measuring working memory deficits in aphasia. J. Commun. Disord. 2012, 45, 325–339. [Google Scholar] [CrossRef]
- Salis, C.; Kelly, H.; Code, C. Assessment and treatment of short-term and working memory impairments in stroke aphasia: A practical tutorial. Int. J. Lang. Commun. Disord. 2015, 50, 721–736. [Google Scholar] [CrossRef]
- Frankel, T.; Penn, C.; Ormond-Brown, D. Executive dysfunction as an explanatory basis for conversation symptoms of aphasia: A pilot study. Aphasiology 2007, 21, 814–828. [Google Scholar] [CrossRef]
- Martin, N.; Reilly, J. Short-term/working memory impairments in aphasia: Data, models, and their application to aphasia rehabilitation. Aphasiology 2012, 26, 253–257. [Google Scholar] [CrossRef]
- Ahveninen, J.; Uluç, I.; Raij, T.; Nummenmaa, A.; Mamashli, F. Spectrotemporal content of human auditory working memory represented in functional connectivity patterns. Commun. Biol. 2023, 6, 294. [Google Scholar] [CrossRef] [PubMed]
- Deldar, Z.; Gevers-Montoro, C.; Gevers-Montoro, C.; Khatibi, A.; Khatibi, A.; Deldar, Z.; Ghazi-Saidi, L. The interaction between language and working memory: A systematic review of fMRI studies in the past two decades. AIMS Neurosci. 2020, 8, 1–32. [Google Scholar] [CrossRef] [PubMed]
- Ghaleh, M.; Lacey, E.H.; Fama, M.E.; Anbari, Z.; Demarco, A.T.; Turkeltaub, P.E. Dissociable Mechanisms of Verbal Working Memory Revealed through Multivariate Lesion Mapping. Cereb. Cortex 2020, 30, 2542–2554. [Google Scholar] [CrossRef] [PubMed]
- Miller, H.E.; Cordella, C.; Collins, J.A.; Ezzo, R.; Quimby, M.; Hochberg, D.; Tourville, J.A.; Dickerson, B.C.; Guenther, F.H. Neural substrates of verbal repetition deficits in primary progressive aphasia. Brain Commun. 2021, 3, fcab015. [Google Scholar] [CrossRef]
- Deschamps, I.; Baum, S.R.; Gracco, V.L. On the role of the supramarginal gyrus in phonological processing and verbal working memory: Evidence from rTMS studies. Neuropsychologia 2014, 53, 39–46. [Google Scholar] [CrossRef]
- Majerus, S.; Cowan, N.; Péters, F.; Van Calster, L.; Phillips, C.; Schrouff, J. Cross-Modal Decoding of Neural Patterns Associated with Working Memory: Evidence for Attention-Based Accounts of Working Memory. Cereb. Cortex 2016, 26, 166–179. [Google Scholar] [CrossRef]
- Choinski, M.; Szelag, E.; Wolak, T.; Szymaszek, A. Working Memory in Aphasia: The Role of Temporal Information Processing. Front. Hum. Neurosci. 2020, 14, 589802. [Google Scholar] [CrossRef]
- Kasselimis, D.S.; Simos, P.G.; Economou, A.; Peppas, C.; Evdokimidis, I.; Potagas, C. Are memory deficits dependent on the presence of aphasia in left brain damaged patients? Neuropsychologia 2013, 51, 1773–1776. [Google Scholar] [CrossRef]
- Tamè, L.; Wühle, A.; Petri, C.D.; Pavani, F.; Braun, C. Concurrent use of somatotopic and external reference frames in a tactile mislocalization task. Brain Cogn. 2017, 111, 25–33. [Google Scholar] [CrossRef]
- Toba, M.N.; Godefroy, O.; Jarrett Rushmore, R.; Zavaglia, M.; Maatoug, R.; Hilgetag, C.C.; Valero-Cabré, A. Revisiting “brain modes” in a new computational era: Approaches for the characterization of brain-behavioural associations. Brain 2020, 143, 1088–1098. [Google Scholar] [CrossRef]
- Brekke, F. Non-Verbal Working Memory: A Functional Near-Infrared Spectroscopy (fNIRS) and Functional Magnetic Resonance Imaging (fMRI) Comparison. Master’s Thesis, University of Bergen, Bergen, Norway, 2023. [Google Scholar]
- Martin, N.; Ayala, J. Measurements of auditory-verbal STM span in aphasia: Effects of item, task, and lexical impairment. Brain Lang. 2004, 89, 464–483. [Google Scholar] [CrossRef] [PubMed]
- Baldo, J.V.; Cronkers, N.F. The role of inferior parietal and inferior frontal cortex in working memory. Neuropsychology 2006, 20, 529–538. [Google Scholar] [CrossRef]
- DeDe, G.; Ricca, M.; Knilans, J.; Trubl, B. Construct validity and reliability of working memory tasks for people with aphasia. Aphasiology 2014, 28, 692–712. [Google Scholar] [CrossRef]
- Lee, B.; Pyun, S.-B. Characteristics of Cognitive Impairment in Patients With Post-stroke Aphasia. Ann. Rehabil. Med. 2014, 38, 759–765. [Google Scholar] [CrossRef]
- Schumacher, R.; Halai, A.D.; Lambon Ralph, M.A. Assessing executive functions in post-stroke aphasia—Utility of verbally based tests. Brain Commun. 2022, 4, fcac107. [Google Scholar] [CrossRef]
- Fonseca, J.; Raposo, A.; Martins, I.P. Cognitive functioning in chronic post-stroke aphasia. Appl. Neuropsychol. Adult 2018, 26, 355–364. [Google Scholar] [CrossRef]
- Baum, C.M.; Lau, S.C.L.; Heinemann, A.W.; Connor, L.T. Functional Cognition: Distinct from Fluid and Crystallized Cognition? Am. J. Occup. Ther. 2023, 77, 7703205020. [Google Scholar] [CrossRef]
- Corsi, P.M. Human Memory and the Medial Temporal Region of the Brain. Ph.D. Thesis, McGill University, Montreal, QC, Canada, 1972. [Google Scholar]
- Conway, A.R.A.; Kane, M.J.; Bunting, M.F.; Hambrick, D.Z.; Wilhelm, O.; Engle, R.W. Working memory span tasks: A methodological review and user’s guide. Psychon. Bull. Rev. 2005, 12, 769–786. [Google Scholar] [CrossRef]
- Snyder, H.R.; Miyake, A.; Hankin, B.L. Advancing understanding of executive function impairments and psychopathology: Bridging the gap between clinical and cognitive approaches. Front. Psychol. 2015, 6, 328. [Google Scholar] [CrossRef]
- Heled, E.; Ohayon, M.; Oshri, O. Working memory in intact modalities among individuals with sensory deprivation. Heliyon 2022, 8, e09558. [Google Scholar] [CrossRef]
- Heled, E.; Levi, O. Aging’s Effect on Working Memory—Modalities Comparison. Biomedicines 2024, 12, 835. [Google Scholar] [CrossRef] [PubMed]
- Nicholas, J.T.; Johannessen, A.M.; van Nunen, T. Tactile Working Memory Scale; Nordic Welfare Centre: Västerås, Sweden, 2019; ISBN 978-91-88213-45-7. [Google Scholar]
- Gallace, A.; Spence, C. Touch with the Future: The Sense of Touch from Cognitive Neuroscience to Virtual Reality; Oxford University Press: Oxford, UK, 2014. [Google Scholar]
- Schmidt, T.T.; Blankenburg, F. Brain regions that retain the spatial layout of tactile stimuli during working memory—A ‘tactospatial sketchpad’? NeuroImage 2018, 178, 531–539. [Google Scholar] [CrossRef] [PubMed]
- Keil, K.; Baldo, J.; Kaplan, E.; Kramer, J.; Delis, D.C. Role of frontal cortex in inferential reasoning: Evidence from the Word Context Test. J. Int. Neuropsychol. Soc. 2005, 11, 426–433. [Google Scholar] [CrossRef] [PubMed]
- Kasselimis, D.; Angelopoulou, G.; Simos, P.; Petrides, M.; Peppas, C.; Velonakis, G.; Tavernarakis, A.; Evdokimidis, I.; Potagas, C. Working memory impairment in aphasia: The issue of stimulus modality. J. Neurolinguistics 2018, 48, 104–116. [Google Scholar] [CrossRef]
- Baldo, J.V.; Klostermann, E.C.; Dronkers, N.F. It’s either a cook or a baker: Patients with conduction aphasia get the gist but lose the trace. Brain Lang. 2008, 105, 134–140. [Google Scholar] [CrossRef]
- Heled, E.; Rotberg, S.; Yavich, R.; Hoofien, A.D. Introducing the Tactual Span: A New Task for Assessing Working Memory in the Teactile Modality. Assessment 2021, 28, 1018–1031. [Google Scholar] [CrossRef]
- Heled, E. Forward versus backward recall: Modality testing. Appl. Neuropsychol. Adult 2024, 1–7. [Google Scholar] [CrossRef]
- Bliss, I.; Hämäläinen, H. Different working memory capacity in normal young adults for visual and tactile letter recognition task. Scand. J. Psychol. 2005, 46, 247–251. [Google Scholar] [CrossRef]
- Heled, E.; Israeli, R.; Margalit, D. Working memory development in different modalities in children and young adults. J. Exp. Child Psychol. 2022, 220, 105422. [Google Scholar] [CrossRef]
- Heled, E.; Oshri, O. Validation of the Tactual Span in individuals with congenital and acquired blindness. Br. J. Vis. Impair. 2021, 41, 328–342. [Google Scholar] [CrossRef]
- Heled, E.; Ohayon, M. Visuospatial and Tactile Working Memory in Individuals with Congenital Deafness. J. Deaf Stud. Deaf Educ. 2021, 26, 314–321. [Google Scholar] [CrossRef] [PubMed]
- Heled, E. Laterality in tactile working memory: The one-hand version of the Tactual Span. J. Neuropsychol. 2024, 19, 67–80. [Google Scholar] [CrossRef] [PubMed]
- Kirchner, W.K. Age differences in short-term retention of rapidly changing information. J. Exp. Psychol. 1958, 55, 352–358. [Google Scholar] [CrossRef]
- dos Santos, R.B.; Fiedler, A.; Badwal, A.; Legasto-Mulvale, J.M.; Sibley, K.M.; Olaleye, O.A.; Diermayr, G.; Salbach, N.M. Standardized tools for assessing balance and mobility in stroke clinical practice guidelines worldwide: A scoping review. Front. Rehabil. Sci. 2023, 4, 1084085. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G* Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]
- Kang, H. Sample size determination and power analysis using the G* Power software. J. Educ. Eval. Health Prof. 2021, 18, 1149215. [Google Scholar] [CrossRef]
- Coemans, S.; Keulen, S.; Savieri, P.; Tsapkini, K.; Engelborghs, S.; Chrispeels, N.; Vandenborre, D.; Paquier, P.; Wilssens, I.; Declerck, M. Executive functions in primary progressive aphasia: A meta-analysis. Cortex 2022, 157, 304–322. [Google Scholar] [CrossRef]
- Salis, C.; Murray, L.; Bakas, K. An international survey of assessment practices for short-term and working memory deficits in aphasia. Am. J. Speech-Lang. Pathol. 2018, 27, 574–591. [Google Scholar] [CrossRef]
- van Asselen, M.; Kessels, R.P.; Neggers, S.F.; Kappelle, L.J.; Frijns, C.J.; Postma, A. Brain areas involved in spatial working memory. Neuropsychologia 2006, 44, 1185–1194. [Google Scholar] [CrossRef]
- Kertesz, A. Western Aphasia Battery Test Manual; Psychological Corporation: San Antonio, TX, USA, 1982. [Google Scholar]
- Soroker, N. Hebrew Western Aphasia Battery; Loewenstein Hospital Rehabilitation Center: Ra’anana, Israel, 1997. [Google Scholar]
- Raven, J.C.; Court, J.H. Colored Progressive Matrices; HK Lewis: London, UK, 1962. [Google Scholar]
- Raven, J.C. Raven’s Progressive Matrices and Vocabulary Scales; Oxford University Press: Oxford, UK, 1998. [Google Scholar]
- Jaeggi, S.M.; Buschkuehl, M.; Perrig, W.J.; Meier, B. The concurrent validity of the N-back task as a working memory measure. Memory 2010, 18, 394–412. [Google Scholar] [CrossRef]
- Scheibel, R.S.; Pearson, D.A.; Faria, L.P.; Kotrla, K.J.; Aylward, J.; Bachevalier, J.; Levin, H.S. An fMRI study of executive functioning after severe diffuse TBI. Brain Inj. 2003, 17, 919–930. [Google Scholar] [CrossRef] [PubMed]
- Ghasemi, A.; Zahediasl, S. Normality tests for statistical analysis: A guide for non-statisticians. Int. J. Endocrinol. Metab. 2012, 10, 486–489. [Google Scholar] [CrossRef] [PubMed]
- Morgan, C.J. Use of proper statistical techniques for research studies with small samples. Am. J. Physiol. Lung Cell. Mollecular Physiol. 2017, 313, L873–L877. [Google Scholar] [CrossRef] [PubMed]
- Fucetola, R.; Connor, L.T.; Strube, M.J.; Corbetta, M. Unravelling nonverbal cognitive performance in acquired aphasia. Aphasiology 2009, 23, 1418–1426. [Google Scholar] [CrossRef]
- Cohen, H.; Scherzer, P.; Viau, R.; Voss, P.; Lepore, F. Working memory for braille is shaped by experience. Commun. Integr. Biol. 2011, 4, 227–229. [Google Scholar] [CrossRef]
- Harris, J.A.; Miniussi, C.; Harris, I.M.; Diamond, M.E. Transient storage of a tactile memory trace in primary somatosensory cortex. J. Neurosci. 2002, 22, 8720–8725. [Google Scholar] [CrossRef]
- Ku, Y.; Zhao, D.; Bodner, M.; Zhou, Y.D. Cooperative processing in primary somatosensory cortex and posterior parietal cortex during tactile working memory. Eur. J. Neurosci. 2015, 42, 1905–1911. [Google Scholar] [CrossRef]
- Zhao, D.; Zhou, Y.D.; Bodner, M.; Ku, Y. The causal role of the prefrontal cortex and somatosensory cortex in tactile working memory. Cereb. Cortex 2018, 28, 3468–3477. [Google Scholar] [CrossRef]
- Marinelli, C.V.; Spaccavento, S.; Craca, A.; Marangolo, P.; Angelelli, P. Different Cognitive Profiles of Patients with Severe Aphasia. Behav. Neurol. 2017, 2017, 3875954. [Google Scholar] [CrossRef]
- Paulraj, S.R.; Schendel, K.; Curran, B.; Dronkersa, N.F.; Baldo, J.V. Role of the left hemisphere in visuospatial working memory. J. Neurolinguistics 2018, 48, 122–141. [Google Scholar] [CrossRef]
- Lacey, E.H.; Skipper-kallal, L.M.; Xing, S.; Fama, M.E.; Turkeltaub, P.E. Mapping Common Aphasia Assessments to Underlying Cognitive Processes and Their Neural Substrates. Neurorehabilit. Neural Repair 2017, 31, 442–450. [Google Scholar] [CrossRef] [PubMed]
- Wager, T.D.; Smith, E.E. Neuroimaging studies of working memory: A meta-analysis. Cogn. Affect. Behav. Neurosci. 2003, 3, 255–274. [Google Scholar] [CrossRef] [PubMed]
- Lezak, M.D.; Howieson, D.B.; Bigler, E.D.; Tranel, D. Neuropsychological Assessment; Oxford University Press: New York, NY, USA, 2012. [Google Scholar]
- Miyake, A.; Friedman, N.P.; Emerson, M.J.; Witzki, A.H.; Howerter, A.; Wager, T.D. The Unity and Diversity of Executive Functions and Their Contributions to Complex “Frontal Lobe” Tasks: A Latent Variable Analysis. Cogn. Psychol. 2000, 41, 49–100. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Group | No. | Sex | Age | Education (Years) | Time After Stroke (Months) |
|---|---|---|---|---|---|
| Aphasia patients | 1 | Male | 71 | 16 | 14 |
| 2 | Male | 45 | 14 | 30 | |
| 3 | Male | 62 | 12 | 66 | |
| 4 | Male | 65 | 15 | 24 | |
| 5 | Male | 58 | 18 | 3 | |
| 6 | Male | 37 | 15 | 24 | |
| 7 | Male | 68 | 12 | 8 | |
| 8 | Male | 50 | 12 | 20 | |
| 9 | Male | 63 | 19 | 36 | |
| 10 | Male | 64 | 12 | 24 | |
| 11 | Male | 61 | 15 | 120 | |
| 12 | Male | 60 | 17 | 10 | |
| 13 | Female | 27 | 16 | 30 | |
| 14 | Female | 78 | 15 | 8 | |
| Controls | 1 | Male | 40 | 17 | -- |
| 2 | Male | 49 | 15 | -- | |
| 3 | Male | 67 | 18 | -- | |
| 4 | Male | 47 | 12 | -- | |
| 5 | Male | 57 | 16 | -- | |
| 6 | Male | 44 | 16 | -- | |
| 7 | Male | 65 | 20 | -- | |
| 8 | Male | 35 | 17 | -- | |
| 9 | Male | 33 | 17 | -- | |
| 10 | Male | 37 | 20 | -- | |
| 11 | Male | 42 | 17 | -- | |
| 12 | Male | 53 | 15 | -- | |
| 13 | Male | 47 | 14 | -- | |
| 14 | Female | 74 | 16 | -- | |
| 15 | Female | 46 | 16 | -- |
| Variable | Aphasia Patients (n = 14) | Control Group (n = 15) |
|---|---|---|
| Age (years) | 57.78 (13.7) | 49.06 (12.12) |
| Education (years) | 14.78 (2.55) | 16.40 (2.06) |
| Tactual Span forward | 3.28 (0.72) | 5.53 (1.41) |
| Visuospatial Span forward | 3.92 (1.68) | 5.73 (1.71) |
| Tactual Span backward | 3.00 (0.78) | 5.13 (1.73) |
| Visuospatial Span backward | 3.50 (1.40) | 5.53 (1.06) |
| 1-back task (ms.) | 0.78 (0.19) | 0.55 (0.17) |
| RCMT (intellectual ability) | 32.28 (10.99) | 34.40 (1.63) |
| Time since stroke (months) | 29.78 (30.37) | ---- |
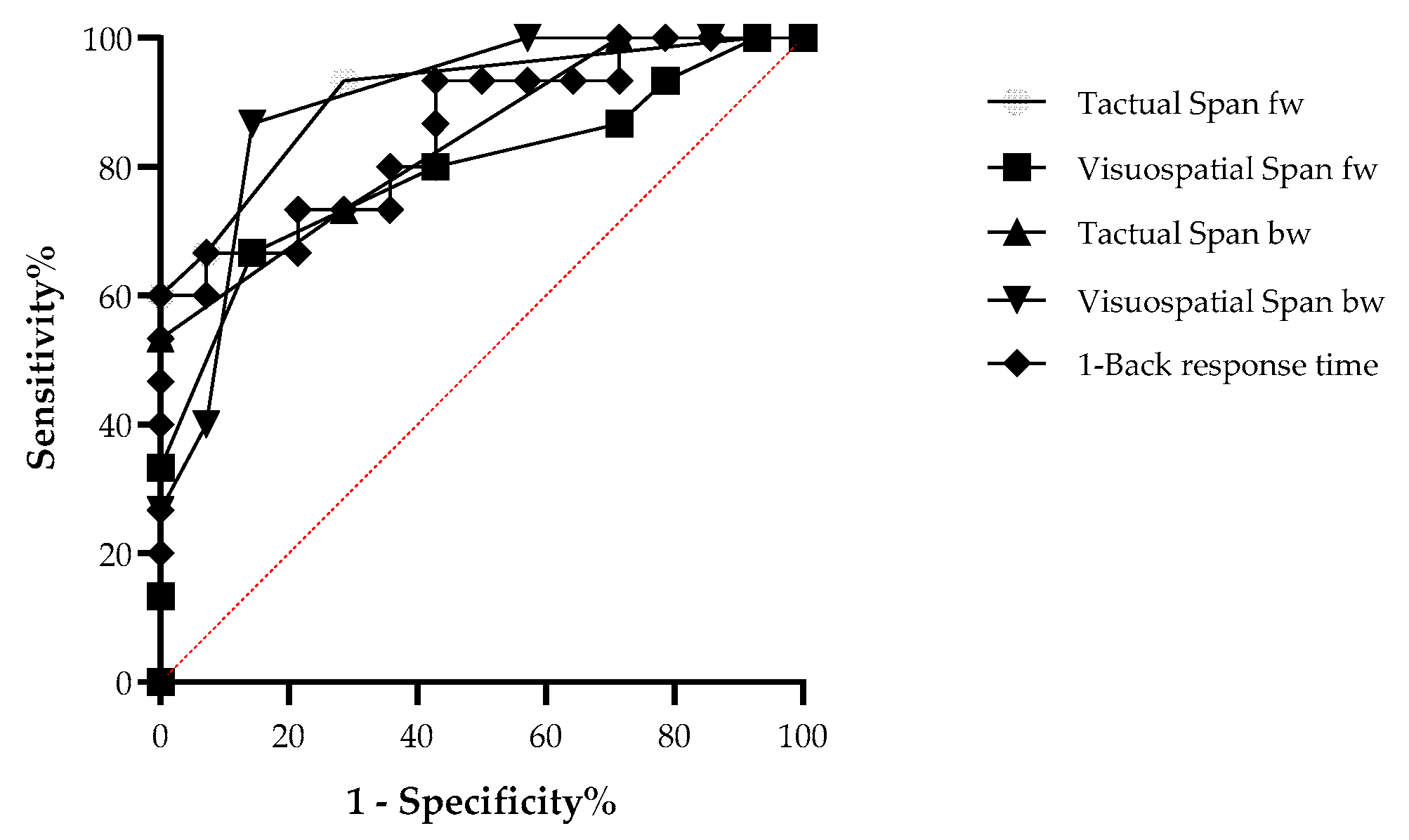
| Measure | Sensitivity (%) | Specificity (%) | AUC | 95% CI | Cut-Off Score |
|---|---|---|---|---|---|
| TS fw | 92.9 | 66.7 | 0.91 (0.05) | [0.80, 1.00] | 4.5 |
| VS fw | 85.7 | 66.7 | 0.79 (0.08) | [0.62, 0.96] | 5.5 |
| TS bw | 71.4 | 73.3 | 0.83 (0.07) | [0.69, 0.98] | 3.5 |
| VS bw | 85.7 | 86.7 | 0.89 (0.06) | [0.77, 1.00] | 4.50 |
| 1-Back task | 85.7 | 73.3 | 0.81 (0.08) | [0.66, 0.97] | 0.62 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heled, E.; Levi, O.; Strobinsky, E.; Zeilig, G. Non-Verbal Working Memory in Post-Stroke Motor Aphasia: A Pilot Study Using the Tactual Span. Neurol. Int. 2025, 17, 58. https://doi.org/10.3390/neurolint17040058
Heled E, Levi O, Strobinsky E, Zeilig G. Non-Verbal Working Memory in Post-Stroke Motor Aphasia: A Pilot Study Using the Tactual Span. Neurology International. 2025; 17(4):58. https://doi.org/10.3390/neurolint17040058
Chicago/Turabian StyleHeled, Eyal, Ohad Levi, Elana Strobinsky, and Gabi Zeilig. 2025. "Non-Verbal Working Memory in Post-Stroke Motor Aphasia: A Pilot Study Using the Tactual Span" Neurology International 17, no. 4: 58. https://doi.org/10.3390/neurolint17040058
APA StyleHeled, E., Levi, O., Strobinsky, E., & Zeilig, G. (2025). Non-Verbal Working Memory in Post-Stroke Motor Aphasia: A Pilot Study Using the Tactual Span. Neurology International, 17(4), 58. https://doi.org/10.3390/neurolint17040058