
The Impact of Acute Postoperative Pain in Developing Chronic Pain after Total Knee Arthroplasty

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
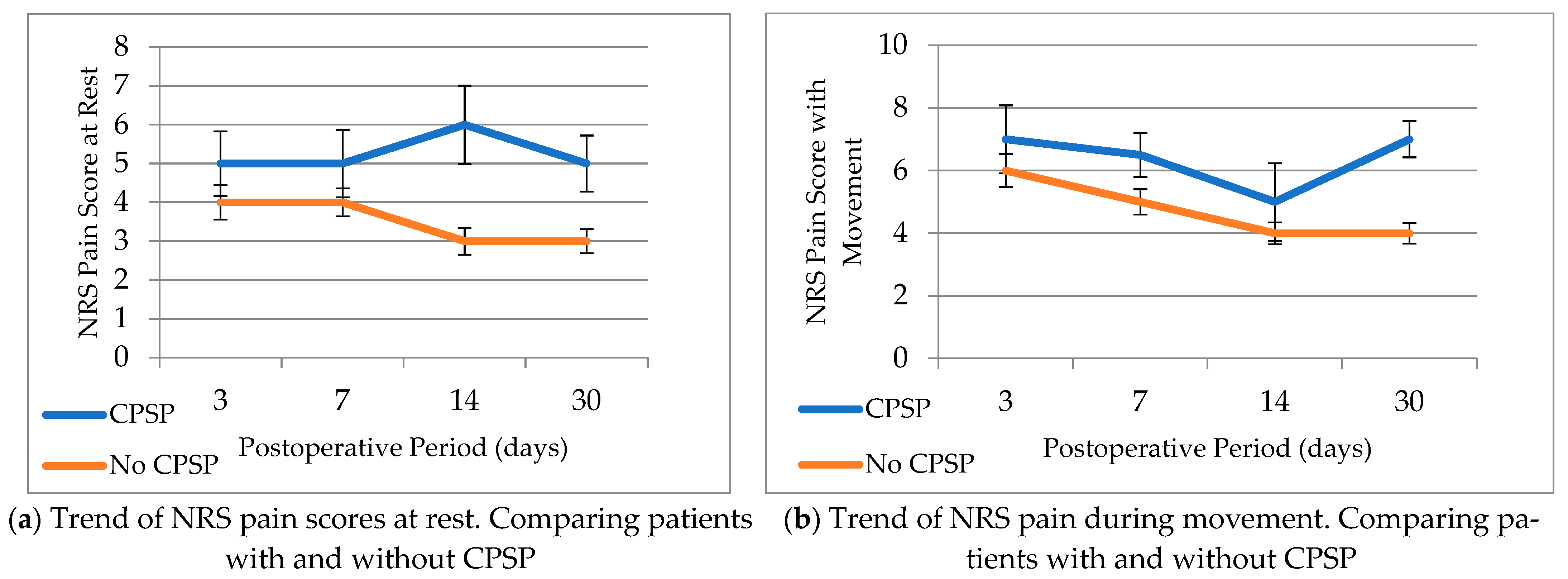
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schug, S.A.; Lavand’homme, P.; Barke, A.; Korwisi, B.; Rief, W.; Treede, R.-D. The IASP Taskforce for the Classification of Chronic Pain The IASP Classification of Chronic Pain for ICD-11: Chronic Postsurgical or Posttraumatic Pain. Pain 2019, 160, 45–52. [Google Scholar] [CrossRef]
- Rosenberger, D.C.; Pogatzki-Zahn, E.M. Chronic Post-Surgical Pain—Update on Incidence, Risk Factors and Preventive Treatment Options. BJA Educ. 2022, 22, 190–196. [Google Scholar] [CrossRef]
- Kehlet, H.; Jensen, T.S.; Woolf, C.J. Persistent Postsurgical Pain: Risk Factors and Prevention. Lancet 2006, 367, 1618–1625. [Google Scholar] [CrossRef]
- Beswick, A.D. What Proportion of Patients Report Long-Term Pain after Total Hip or Knee Replacement for Osteoarthritis? A Systematic Review of Prospective Studies in Unselected Patients. BMJ Open 2012, 2, 000435. [Google Scholar] [CrossRef]
- Jones, C.A. Health Related Quality of Life Outcomes after Total Hip and Knee Arthroplasties in a Community Based Population. J. Rheumatol. 2000, 27, 1745–1752. [Google Scholar]
- Petersen, K.K. Chronic Postoperative Pain after Primary and Revision Total Knee Arthroplasty. Clin. J. Pain 2015, 31, 1–6. [Google Scholar] [CrossRef]
- Sugiyama, Y. Prevalence of Chronic Postsurgical Pain after Thoracotomy and Total Knee Arthroplasty: A Retrospective Multicenter Study in Japan Japanese Study Group of Subacute Postoperative Pain. J. Anesth. 2018, 32, 434–438. [Google Scholar] [CrossRef]
- Noiseux, N.O. Preoperative Predictors of Pain Following Total Knee Arthroplasty. J. Arthroplast. 2014, 29, 1383–1387. [Google Scholar] [CrossRef]
- Wees, P.J. Patient-Reported Health Outcomes after Total Hip and Knee Surgery in a Dutch University Hospital Setting: Results of Twenty Years Clinical Registry. BMC Musculoskelet. Disord. 2017, 18, 97. [Google Scholar]
- Lewis, G.N. Predictors of Persistent Pain after Total Knee Arthroplasty: A Systematic Review and Meta-Analysis. Br. J. Anaesth. 2015, 114, 551–561. [Google Scholar] [CrossRef]
- Wang, J. Transition from Acute to Chronic Pain:Evaluating Risk for Chronic Postsurgical Pain. Pain Phys. 2019, 5, 479–488. [Google Scholar] [CrossRef]
- Gilron, I. Evaluating the Association between Acute and Chronic Pain after Surgery: Impact of Pain Measurement Methods. Clin. J. Pain 2017, 33, 588–594. [Google Scholar] [CrossRef]
- Woolf, C.J. Central Sensitization: Implications for the Diagnosis and Treatment of Pain. Pain 2011, 152, S2–S15. [Google Scholar] [CrossRef]
- Descalzi, G.; Ikegami, D.; Ushijima, T.; Nestler, E.; Zachariou, V.; Narita, M. Epigenetic Mechanisms of Chronic Pain. Trends Neurosci. 2015, 38, 237–246. [Google Scholar] [CrossRef]
- Inquimbert, P.; Moll, M.; Latremoliere, A.; Tong, C.-K.; Whang, J.; Sheehan, G.F.; Smith, B.M.; Korb, E.; Athié, M.C.P.; Babaniyi, O.; et al. NMDA Receptor Activation Underlies the Loss of Spinal Dorsal Horn Neurons and the Transition to Persistent Pain after Peripheral Nerve Injury. Cell Rep. 2018, 23, 2678–2689. [Google Scholar] [CrossRef]
- Carley, M.E.; Chaparro, L.E.; Choinière, M.; Kehlet, H.; Moore, R.A.; Van Den Kerkhof, E.; Gilron, I. Pharmacotherapy for the Prevention of Chronic Pain after Surgery in Adults: An Updated Systematic Review and Meta-Analysis. Anesthesiology 2021, 135, 304–325. [Google Scholar] [CrossRef]
- Rullán, P.J.; Emara, A.K.; Zhou, G.; Pasqualini, I.; Klika, A.K.; Koroukian, S.; Barsoum, W.K.; Piuzzi, N.S. National Inpatient Datasets May No Longer Be Appropriate for Overall Total Hip and Knee Arthroplasties Projections after Removal from Inpatient-Only Lists. J. Knee Surg. 2024, 37, 214–219. [Google Scholar] [CrossRef]
- Shichman, I.; Roof, M.; Askew, N.; Nherera, L.; Rozell, J.C.; Seyler, T.M.; Schwarzkopf, R. Projections and Epidemiology of Primary Hip and Knee Arthroplasty in Medicare Patients to 2040–2060. JBJS Open Access 2023, 8, e22.00112. [Google Scholar] [CrossRef]
- Lenguerrand, E. Trajectories of Pain and Function after Primary Hip and Knee Arthroplasty: The ADAPT Cohort Study. PLoS ONE 2016, 11, 0149306. [Google Scholar] [CrossRef]
- Wylde, V. 5 Year Outcomes and Survivorship of the Triathlon Total Knee Replacement: A Cohort Study. Acta Orthopædica Belg. 2017, 83, 259–267. [Google Scholar]
- Bourne, R.B. Patient Satisfaction after Total Knee Arthroplasty: Who Is Satisfied and Who Is Not? Clin. Orthop. Relat. Res. 2010, 468, 57–63. [Google Scholar] [CrossRef]
- Anderson, J.G. Functional Outcome and Patient Satisfaction in Total Knee Patients over the Age of 75. J. Arthroplast. 1996, 11, 831–840. [Google Scholar] [CrossRef]
- Dunbar, M.J. Appropriate Questionnaires for Knee Arthroplasty. Results of a Survey of 3600 Patients from The Swedish Knee Arthroplasty Registry. J. Bone Jt. Surg. Br. 2001, 83, 339–344. [Google Scholar] [CrossRef]
- Hawker, G. Health-Related Quality of Life after Knee Replacement. J. Bone Jt. Surg. Am. 1998, 80, 163–173. [Google Scholar] [CrossRef]
- Heck, D.A. Patient Outcomes after Knee Replacement. Clin. Orthop. Relat. Res. 1998, 356, 93–110. [Google Scholar] [CrossRef]
- Andersen, L.Ø.; Gaarn-Larsen, L.; Kristensen, B.B.; Husted, H.; Otte, K.S.; Kehlet, H. Subacute Pain and Function after Fast-Track Hip and Knee Arthroplasty. Anaesthesia 2009, 64, 508–513. [Google Scholar] [CrossRef]
- Wylde, V. Persistent Pain after Joint Replacement: Prevalence, Sensory Qualities, and Postoperative Determinants. Pain 2011, 152, 566–572. [Google Scholar] [CrossRef]
- Laigaard, J.; Karlsen, A.; Maagaard, M.; Rosenberg, L.K.; Creutzburg, A.; Lunn, T.H.; Mathiesen, O.; Overgaard, S. Perioperative Prevention of Persistent Pain after Total Hip and Knee Arthroplasty—Protocol for Two Systematic Reviews. Acta Anaesthesiol. Scand. 2022, 66, 772–777. [Google Scholar] [CrossRef]
- Ashoorion, V.; Sadeghirad, B.; Wang, L.; Noori, A.; Abdar, M.; Kim, Y.; Chang, Y.; Rehman, N.; Lopes, L.C.; Couban, R.J.; et al. Predictors of Persistent Post-Surgical Pain Following Total Knee Arthroplasty: A Systematic Review and Meta-Analysis of Observational Studies. Pain Med. 2023, 24, 369–381. [Google Scholar] [CrossRef]
- Lorentzen, J.S. Early Changes in Muscle Strength after Total Knee Arthroplasty. A 6-Month Follow-up of 30 Knees. Acta Orthop. Scand. 1999, 70, 176–179. [Google Scholar] [CrossRef]
- Ryu, J. Factors Influencing the Postoperative Range of Motion in Total Knee Arthroplasty. Bull. Hosp. Jt. Dis. 1993, 53, 35–40. [Google Scholar]
- Wang, D. Adductor Canal Block versus Femoral Nerve Block for Total Knee Arthroplasty: A Meta-Analysis of Randomized Controlled Trials. Sci. Rep. 2017, 7, 40721. [Google Scholar] [CrossRef]
- Guertin, J.R.; Pagé, M.G.; Tarride, J.-É.; Talbot, D.; Watt-Watson, J.; Choinière, M. Just How Much Does It Cost? A Cost Study of Chronic Pain Following Cardiac Surgery. J. Pain Res. 2018, 11, 2741–2759. [Google Scholar] [CrossRef]
- Keller, S. Validity of the Brief Pain Inventory for Use in Documenting the Outcomes of Patients with Noncancer Pain. Clin. J. Pain 2004, 20, 309–318. [Google Scholar] [CrossRef]
- Cleeland, C.S.; Ryan, K.M. Pain Assessment: Global Use of the Brief Pain Inventory. Ann. Acad. Med. Singap. 1994, 23, 129–138. [Google Scholar]
- Mendoza, T.; Mayne, T.; Rublee, D.; Cleeland, C. Reliability and Validity of a Modified Brief Pain Inventory Short Form in Patients with Osteoarthritis. Eur. J. Pain 2006, 10, 353–361. [Google Scholar] [CrossRef]
- Mendoza, T.R.; Chen, C.; Brugger, A.; Hubbard, R.; Snabes, M.; Palmer, S.N.; Zhang, Q.; Cleeland, C.S. The Utility and Validity of the Modified Brief Pain Inventory in a Multiple-Dose Postoperative Analgesic Trial. Clin. J. Pain 2004, 20, 357. [Google Scholar] [CrossRef]
- Ghoshal, A.; Bhanvadia, S.; Singh, S.; Yaeger, L.; Haroutounian, S. Factors Associated with Persistent Postsurgical Pain after Total Knee or Hip Joint Replacement: A Systematic Review and Meta-Analysis. PAIN Rep. 2023, 8, e1052. [Google Scholar] [CrossRef]
- Lavand’homme, P.M.; Grosu, I.; France, M.-N.; Thienpont, E. Pain Trajectories Identify Patients at Risk of Persistent Pain after Knee Arthroplasty: An Observational Study. Clin. Orthop. Relat. Res. 2014, 472, 1409–1415. [Google Scholar] [CrossRef]
- Buvanendran, A. Acute Postoperative Pain Is an Independent Predictor of Chronic Postsurgical Pain Following Total Knee Arthroplasty at 6 Months: A Prospective Cohort Study. Reg. Anesth. Pain Med. 2019, 44, 287–296. [Google Scholar] [CrossRef]
- Sayers, A. Rest Pain and Movement-Evoked Pain as Unique Constructs in Hip and Knee Replacements. Arthritis Care Res. 2016, 68, 237–245. [Google Scholar] [CrossRef]
- Pua, Y.H.; Ong, P.H. Association of Early Ambulation with Length of Stay and Costs in Total Knee Arthroplasty: Retrospective Cohort Study. Am. J. Phys. Med. Rehabil. 2014, 93, 962–970. [Google Scholar] [CrossRef]
- Lovelock, T.M.; Broughton, N.S. Follow-up after Arthroplasty of the Hip and Knee: Are We over-Servicing or under-Caring? Bone Jt. J. 2018; 100-B, 6–10. [Google Scholar]
- Katz, J.; Weinrib, A.Z.; Clarke, H. Chronic Postsurgical Pain: From Risk Factor Identification to Multidisciplinary Management at the Toronto General Hospital Transitional Pain Service. Can. J. Pain 2019, 3, 49–58. [Google Scholar] [CrossRef]
- Abid Azam, M.; Weinrib, A.Z.; Montbriand, J.; Burns, L.C.; McMillan, K.; Clarke, H.; Katz, J. Acceptance and Commitment Therapy to Manage Pain and Opioid Use after Major Surgery: Preliminary Outcomes from the Toronto General Hospital Transitional Pain Service. Can. J. Pain 2017, 1, 37–49. [Google Scholar] [CrossRef]
- Clarke, H.; Azargive, S.; Montbriand, J.; Nicholls, J.; Sutherland, A.; Valeeva, L.; Boulis, S.; McMillan, K.; Ladak, S.S.J.; Ladha, K.; et al. Opioid Weaning and Pain Management in Postsurgical Patients at the Toronto General Hospital Transitional Pain Service. Can. J. Pain 2018, 2, 236–247. [Google Scholar] [CrossRef]
- Teeny, S.M.; York, S.C.; Mesko, J.W.; Rea, R.E. Long-Term Follow-up Care Recommendations after Total Hip and Knee Arthroplasty: Results of the American Association of Hip and Knee Surgeons’ Member Survey. J. Arthroplast. 2003, 18, 954–962. [Google Scholar] [CrossRef]
- Follow-Up | Hip and Knee Care. Available online: https://hipknee.aahks.org/dont-take-your-new-joint-for-granted-follow-up-care/ (accessed on 13 March 2024).
- Fransen, B.L.; Hoozemans, M.J.M.; Argelo, K.D.S.; Keijser, L.C.M.; Burger, B.J. Fast-Track Total Knee Arthroplasty Improved Clinical and Functional Outcome in the First 7 Days after Surgery: A Randomized Controlled Pilot Study with 5-Year Follow-Up. Arch. Orthop. Trauma Surg. 2018, 138, 1305–1316. [Google Scholar] [CrossRef]
- Andreae, M.H.; Andreae, D.A. Regional Anaesthesia to Prevent Chronic Pain after Surgery: A Cochrane Systematic Review and Meta-Analysis. Br. J. Anaesth. 2013, 111, 711–720. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | LTFU (n = 69) | No LTFU (n = 34) | p Value |
|---|---|---|---|
| Age (mean years ± SD) | 63.5 ± 9.9 | 63.0 ± 11.6 | 0.829 |
| Sex n (%) | 0.082 | ||
| Male | 20 (29%) | 16 (47%) | |
| Female | 49 (71%) | 18 (53%) | |
| BMI kg/m2, median (IQR) | 32.9 (9.4) | 34.0 (6.4) | 0.672 |
| Length of surgery min, median (IQR) | 103.0 (44) | 96.0 (29) | 1.000 |
| NRS Pain Score at Rest, median (IQR) | |||
| POD 0 | 1.0 (6) | 1.0 (5) | 0.864 |
| POD 1 | 5.0 (3) | 4.0 (3) | 0.837 |
| POD 2 | 4.0 (4) | 4.0 (4) | 0.935 |
| POD 3 | 4.5 (2) | 5.0 (5) | 0.269 |
| POD 7 | 4.0 (3) | 5.0 (5) | 0.187 |
| POD 14 | 3.0 (3) | 3.0 (4) | 0.880 |
| POD 30 | 3.0 (4) | 3.0 (4) | 0.958 |
| NRS Pain Score with Movement, median (IQR) | |||
| POD 0 | 1.0 (5) | 1.5 (6) | 0.479 |
| POD 1 | 6.0 (3) | 5.0 (3) | 0.958 |
| POD 2 | 6.0 (3) | 4.0 (4) | 0.607 |
| POD 3 | 6.0 (3) | 6.0 (4) | 0.856 |
| POD 7 | 6.0 (3) | 6.0 (5) | 0.422 |
| POD 14 | 4.0 (3) | 4.0 (3) | 0.880 |
| POD 30 | 4.0 (5) | 4.0 (3) | 0.788 |
| Characteristics | OR (95% CI) |
|---|---|
| Age (years) | 1.03 (0.97, 1.10) |
| Female sex | 2.68 (0.54, 13.37) |
| BMI (kg/m2) | 1.03 (0.96, 1.11) |
| Morphine equivalents | |
| POD 0 | 1.010 (0.99, 1.03) |
| POD 1 | 0.997 (0.97, 1.02) |
| POD 2 | 0.997 (0.97, 1.02) |
| POD 3 | 0.957 (0.89, 1.03) |
| NRS Pain Score at Rest | |
| POD 0 | 0.99 (0.84, 1.16) |
| POD 1 | 0.99 (0.84, 1.16) |
| POD 2 | 1.11 (0.80, 1.53) |
| POD 3 | 1.52 (1.02, 2.26) ** |
| POD 7 | 1.33 (0.98, 1.79) * |
| POD 14 | 1.61 (1.10, 2.34) ** |
| POD 30 | 1.43 (0.99, 2.07) * |
| NRS Movement Pain Score | |
| POD 0 | 1.02 (0.82, 1.27) |
| POD 1 | 1.26 (0.88,1.79) |
| POD 2 | 1.07 (0.77, 1.48) |
| POD 3 | 1.14 (0.81, 1.62) |
| POD 7 | 1.14 (0.85, 1.53) |
| POD 14 | 1.18 (0.89, 1.57) |
| POD 30 | 1.51 (1.02, 2.25) |
| Interference of Activity (mean ± SD) | 7.46 ± 1.74 |
| Interference of Walking (mean ± SD) | 5.15 ± 3.08 |
| Interference of Normal Work (mean ± SD) | 6.77 ± 2.62 |
| Interference of Sleep (mean ± SD) | 3.83 ± 2.64 |
| Medication Use n (%) | |
| Opioids | 9 (13.0%) |
| Non-opioids | 4 (5.8%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Knezevic, N.N.; Syed, O.; Kabir, C.; Patel, A.; Rao Shuai, I.; Tharian, A.R. The Impact of Acute Postoperative Pain in Developing Chronic Pain after Total Knee Arthroplasty. Neurol. Int. 2024, 16, 459-469. https://doi.org/10.3390/neurolint16020034
Knezevic NN, Syed O, Kabir C, Patel A, Rao Shuai I, Tharian AR. The Impact of Acute Postoperative Pain in Developing Chronic Pain after Total Knee Arthroplasty. Neurology International. 2024; 16(2):459-469. https://doi.org/10.3390/neurolint16020034
Chicago/Turabian StyleKnezevic, Nebojsa Nick, Osman Syed, Christopher Kabir, Aisha Patel, Isabel Rao Shuai, and Antony R. Tharian. 2024. "The Impact of Acute Postoperative Pain in Developing Chronic Pain after Total Knee Arthroplasty" Neurology International 16, no. 2: 459-469. https://doi.org/10.3390/neurolint16020034
APA StyleKnezevic, N. N., Syed, O., Kabir, C., Patel, A., Rao Shuai, I., & Tharian, A. R. (2024). The Impact of Acute Postoperative Pain in Developing Chronic Pain after Total Knee Arthroplasty. Neurology International, 16(2), 459-469. https://doi.org/10.3390/neurolint16020034