

Evaluation of Age Based-Sleep Quality and Fitness in Adolescent Female Handball Players


 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Anthropometric Measurements
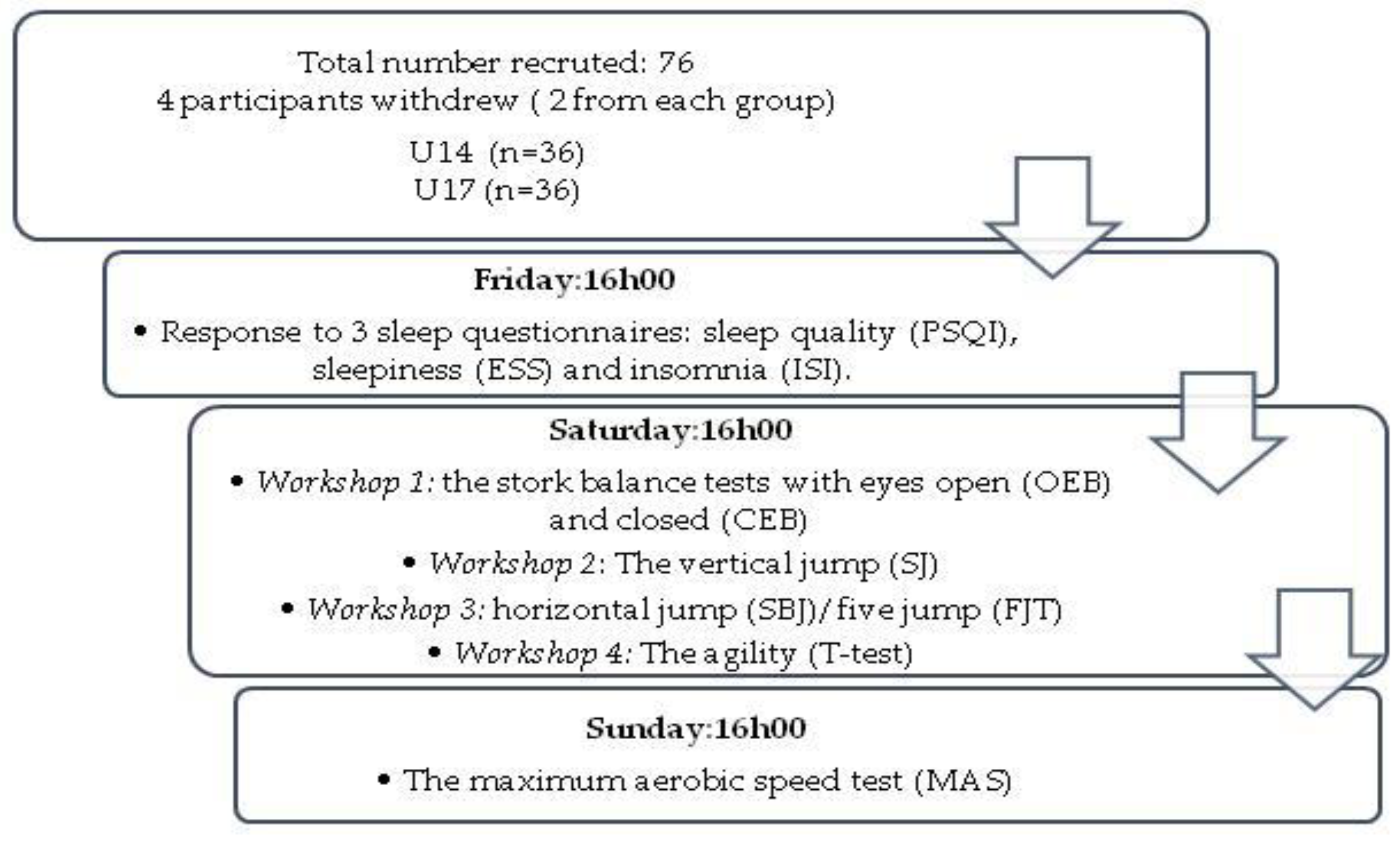
2.3. Procedure
- Day1:
- Day2:
2.3.1. Stork Balance Test
2.3.2. Squat Jump (SJ)
2.3.3. The Standing Broad Jump or the Horizontal Jump (SBJ)
2.3.4. Five Jump Test (FJT)
2.3.5. The Agility t Test
2.3.6. VAMEVAL Test
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Daneshjoo, A.; Hoseinpour, A.; Sadeghi, H.; Kalantari, A.; Behm, D.G. The Effect of a Handball Warm-Up Program on Dynamic Balance among Elite Adolescent Handball Players. Sports 2022, 10, 18. [Google Scholar] [CrossRef] [PubMed]
- Gioftsidou, A.; Malliou, P.; Sofokleous, P.; Pafis, G.; Beneka, A.; Godolias, G. The Effects of Balance Training on Balance Ability in Handball Players. Exerc. Qual. Life 2012, 4, 15–22. [Google Scholar] [CrossRef]
- Ljubica, M.; Bjelica, B.; Aksović, N.; Cicović, V.; D’Onofrio, R. Estimation of Explosive Power of Lower Extremities in Handball. Ital. J. Sport. Rehabil. Posturol. 2021, 10, 2507–2617. [Google Scholar]
- Oxyzoglou, N.; Kanioglou, A.; Rizos, S.; Mavridis, G.; Kabitsis, C. Muscular Strength and Jumping Performance after Handball Training versus Physical Education Program for Pre-Adolescent Children. Percept. Mot. Ski. 2007, 104 Pt 2, 1282–1288. [Google Scholar] [CrossRef] [PubMed]
- Karcher, C.; Buchheit, M. On-Court Demands of Elite Handball, with Special Reference to Playing Positions. Sport. Med. 2014, 44, 797–814. [Google Scholar] [CrossRef] [PubMed]
- Spasic, M.; Krolo, A.; Zenic, N.; Delextrat, A.; Sekulic, D. Reactive Agility Performance in Handball; Development and Evaluation of a Sport-Specific Measurement Protocol. J. Sport. Sci. Med. 2015, 14, 501–506. [Google Scholar]
- Camacho-Cardenosa, A.; Camacho-Cardenosa, M.; Brazo-Sayavera, J. Endurance Assessment in Handball: A Systematic Review. Eur. J. Hum. Mov. 2019, 43, 13–39. [Google Scholar]
- Wagner, H.; Finkenzeller, T.; Würth, S.; von Duvillard, S.P. Individual and Team Performance in Team-Handball: A Review. J. Sport. Sci. Med. 2014, 13, 808–816. [Google Scholar]
- Zech, A.; Venter, R.; de Villiers, J.E.; Sehner, S.; Wegscheider, K.; Hollander, K. Motor Skills of Children and Adolescents Are Influenced by Growing up Barefoot or Shod. Front. Pediatr. 2018, 6, 115. [Google Scholar] [CrossRef]
- Trecroci, A.; Longo, S.; Perri, E.; Iaia, F.M.; Alberti, G. Field-Based Physical Performance of Elite and Sub-Elite Middle-Adolescent Soccer Players. Res. Sport. Med. 2019, 27, 60–71. [Google Scholar] [CrossRef]
- Waldron, M.; Murphy, A. A Comparison of Physical Abilities and Match Performance Characteristics among Elite and Sub-elite Under-14 Soccer Players. Pediatr. Exerc. Sci. 2013, 25, 423–434. [Google Scholar] [CrossRef]
- Trajković, N.; Sporiš, G.; Krističević, T.; Madić, D.M.; Bogataj, Š. The Importance of Reactive Agility Tests in Differentiating Adolescent Soccer Players. Int. J. Environ. Res. Public Health 2020, 17, 3839. [Google Scholar] [CrossRef] [PubMed]
- Srhoj, V.; Rogulj, N.; Zagorac, N.; Katić, R. A New Model of Selection in Women’s Handball. Coll. Antropol. 2006, 30, 601–605. [Google Scholar] [PubMed]
- Lloyd, R.S.; Oliver, J.L.; Faigenbaum, A.D.; Myer, G.D.; De Ste Croix, M.B.A. Chronological Age vs. Biological Maturation: Implications for Exercise Programming in Youth. J. Strength Cond. Res. 2014, 28, 1454–1464. [Google Scholar] [CrossRef] [PubMed]
- Greier, K.; Drenowatz, C.; Ruedl, G.; Kirschner, W.; Mitmannsgruber, P.; Greier, C. Physical Fitness across 11- to 17-Year-Old Adolescents: A Cross-Sectional Study in 2267 Austrian Middle- and High-School Students. Adv. Phys. Educ. 2019, 9, 258–269. [Google Scholar] [CrossRef]
- Vink, E.E.; van Coeverden, S.C.C.M.; van Mil, E.G.; Felius, B.A.; van Leerdam, F.J.M.; Delemarre-van de Waal, H.A. Changes and Tracking of Fat Mass in Pubertal Girls. Obesity 2010, 18, 1247–1251. [Google Scholar] [CrossRef]
- Drake, C.; Nickel, C.; Burduvali, E.; Roth, T.; Jefferson, C.; Pietro, B. The Pediatric Daytime Sleepiness Scale (PDSS): Sleep Habits and School Outcomes in Middle-School Children. Sleep 2003, 26, 455–458. [Google Scholar]
- Chasens, E.R.; Sereika, S.M.; Weaver, T.E.; Umlauf, M.G. Daytime Sleepiness, Exercise, and Physical Function in Older Adults. J. Sleep Res. 2007, 16, 60–65. [Google Scholar] [CrossRef]
- Strand, L.B.; Laugsand, L.E.; Wisløff, U.; Nes, B.M.; Vatten, L.; Janszky, I. Insomnia Symptoms and Cardiorespiratory Fitness in Healthy Individuals: The Nord-Trøndelag Health Study (HUNT). Sleep 2013, 36, 99–108. [Google Scholar] [CrossRef]
- Colrain, I.M.; Baker, F.C. Changes in Sleep as a Function of Adolescent Development. Neuropsychol. Rev. 2011, 21, 5–21. [Google Scholar] [CrossRef]
- Carskadon, M.A.; Acebo, C.; Richardson, G.S.; Tate, B.A.; Seifer, R. An Approach to Studying Circadian Rhythms of Adolescent Humans. J. Biol. Rhythm. 1997, 12, 278–289. [Google Scholar] [CrossRef] [PubMed]
- Crowley, S.J.; Acebo, C.; Carskadon, M.A. Sleep, Circadian Rhythms, and Delayed Phase in Adolescence. Sleep Med. 2007, 8, 602–612. [Google Scholar] [CrossRef]
- Moore, M.; Meltzer, L.J. The Sleepy Adolescent: Causes and Consequences of Sleepiness in Teens. Paediatr. Respir. Rev. 2008, 9, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Sadeh, A.; Dahl, R.E.; Shahar, G.; Rosenblat-Stein, S. Sleep and the Transition to Adolescence: A Longitudinal Study. Sleep 2009, 32, 1602–1609. [Google Scholar] [CrossRef] [PubMed]
- Johnson, E.O.; Roth, T.; Schultz, L.; Breslau, N. Epidemiology of DSM-IV Insomnia in Adolescence: Lifetime Prevalence, Chronicity, and an Emergent Gender Difference. Pediatrics 2006, 117, e247–e256. [Google Scholar] [CrossRef] [PubMed]
- Roberts, R.E.; Roberts, C.R.; Duong, H.T. Chronic Insomnia and Its Negative Consequences for Health and Functioning of Adolescents: A 12-Month Prospective Study. J. Adolesc. Health 2008, 42, 294–302. [Google Scholar] [CrossRef]
- Carvalho, A.S.; Fernandes, A.P.; Gallego, A.B.; Vaz, J.A.; Vega, M.S. The Relation of Sports with Sleep Quality and Anthropometric Measures at Secondary Schools. J. Sport Health Res. 2019, 11, 91–106. [Google Scholar]
- Harriss, D.J.; Atkinson, G. Update—Ethical Standards in Sport and Exercise Science Research. Int. J. Sport. Med. 2011, 32, 819–821. [Google Scholar] [CrossRef]
- Tanner, J.M.; Whitehouse, R.H. Clinical Longitudinal Standards for Height, Weight, Height Velocity, Weight Velocity, and Stages of Puberty. Arch. Dis. Child. 1976, 51, 170–179. [Google Scholar] [CrossRef]
- Chtourou, H.; Souissi, N. The Effect of Training at a Specific Time of Day: A Review. J. Strength Cond. Res. 2012, 26, 1984–2005. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A New Instrument for Psychiatric Practice and Research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef] [PubMed]
- Morin, C.M. Insomnia: Psychological Assessment and Management; Guilford Press: New York, NY, USA, 1993; pp. xvii, 238. [Google Scholar]
- Johns, M.W. A New Method for Measuring Daytime Sleepiness: The Epworth Sleepiness Scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [PubMed]
- Racil, G.; Ben Ounis, O.; Hammouda, O.; Kallel, A.; Zouhal, H.; Chamari, K.; Amri, M. Effects of High vs. Moderate Exercise Intensity during Interval Training on Lipids and Adiponectin Levels in Obese Young Females. Eur. J. Appl. Physiol. 2013, 113, 2531–2540. [Google Scholar] [CrossRef]
- Sopa, I.S.; Szabo, D.A. Testing agilityand balance in volleyball game. Discobolul Phys. Educ. Sport Kinetother. J. 2015, XII, 167–174. [Google Scholar]
- Bosco, C.; Luhtanen, P.; Komi, P.V. A Simple Method for Measurement of Mechanical Power in Jumping. Eur. J. Appl. Physiol. Occup. Physiol. 1983, 50, 273–282. [Google Scholar] [CrossRef]
- Saint-Maurice, P.F.; Laurson, K.R.; Kaj, M.; Csányi, T. Establishing Normative Reference Values for Standing Broad Jump Among Hungarian Youth. Res. Q. Exerc. Sport. 2015, 86 (Suppl. 1), S37–S44. [Google Scholar] [CrossRef] [PubMed]
- Chamari, K.; Chaouachi, A.; Hambli, M.; Kaouech, F.; Wisløff, U.; Castagna, C. The Five-Jump Test for Distance as a Field Test to Assess Lower Limb Explosive Power in Soccer Players. J. Strength Cond. Res. 2008, 22, 944–950. [Google Scholar] [CrossRef]
- Jlid, M.C.; Coquart, J.; Maffulli, N.; Paillard, T.; Bisciotti, G.N.; Chamari, K. Effects of in Season Multi-Directional Plyometric Training on Vertical Jump Performance, Change of Direction Speed and Dynamic Postural Control in U-21 Soccer Players. Front. Physiol. 2020, 11, 374. [Google Scholar] [CrossRef]
- Kuipers, H.; Verstappen, F.T.; Keizer, H.A.; Geurten, P.; van Kranenburg, G. Variability of Aerobic Performance in the Laboratory and Its Physiologic Correlates. Int. J. Sport. Med. 1985, 6, 197–201. [Google Scholar] [CrossRef]
- Pugh, L.G. Oxygen Intake in Track and Treadmill Running with Observations on the Effect of Air Resistance. J. Physiol. 1970, 207, 823–835. [Google Scholar] [CrossRef]
- Shephard, R.J. A Nomogram to Calculate the Oxygen-Cost of Running at Slow Speeds. J. Sport. Med. Phys. Fit. 1969, 9, 10–16. [Google Scholar]
- Davenne, D. Activité physique et sommeil chez les seniors. Médecine Du Sommeil 2015, 12, 181–189. [Google Scholar] [CrossRef]
- Rasekhi, S.; Pour Ashouri, F.; Pirouzan, A. Effects of Sleep Quality on the Academic Performance of Undergraduate Medical Students. Health Scope 2016, 5, e31641. [Google Scholar] [CrossRef]
- Bruce, E.S.; Lunt, L.; McDonagh, J.E. Sleep in Adolescents and Young Adults. Clin. Med. 2017, 17, 424–428. [Google Scholar] [CrossRef] [PubMed]
- Bel, S.; Michels, N.; Vriendt, T.D.; Patterson, E.; Cuenca-García, M.; Diethelm, K.; Gutin, B.; Grammatikaki, E.; Manios, Y.; Leclercq, C.; et al. Association between self-reported sleep duration and dietary quality in European adolescents. Br. J. Nutr. 2013, 110, 949–959. [Google Scholar] [CrossRef] [PubMed]
- Ferranti, R.; Marventano, S.; Castellano, S.; Giogianni, G.; Nolfo, F.; Rametta, S.; Matalone, M.; Mistretta, A. Sleep Quality and Duration Is Related with Diet and Obesity in Young Adolescent Living in Sicily, Southern Italy. Sleep Sci. 2016, 9, 117–122. [Google Scholar] [CrossRef]
- Figueiro, M.G. Delayed Sleep Phase Disorder: Clinical Perspective with a Focus on Light Therapy. Nat. Sci. Sleep. 2016, 8, 91–106. [Google Scholar] [CrossRef]
- Chen, Y.; Cui, Y.; Chen, S.; Wu, Z. Relationship between Sleep and Muscle Strength among Chinese University Students: A Cross-Sectional Study. J. Musculoskelet. Neuronal Interact. 2017, 17, 327–333. [Google Scholar]
- Knowles, O.E.; Drinkwater, E.J.; Urwin, C.S.; Lamon, S.; Aisbett, B. Inadequate Sleep and Muscle Strength: Implications for Resistance Training. J. Sci. Med. Sport 2018, 21, 959–968. [Google Scholar] [CrossRef]
- Morasso, P.G.; Sanguineti, V. Ankle Muscle Stiffness Alone Cannot Stabilize Balance during Quiet Standing. J. Neurophysiol. 2002, 88, 2157–2162. [Google Scholar] [CrossRef]
- Ahrberg, K.; Dresler, M.; Niedermaier, S.; Steiger, A.; Genzel, L. The Interaction between Sleep Quality and Academic Performance. J. Psychiatr. Res. 2012, 46, 1618–1622. [Google Scholar] [CrossRef] [PubMed]
- Avni, N.; Avni, I.; Barenboim, E.; Azaria, B.; Zadok, D.; Kohen-Raz, R.; Morad, Y. Brief Posturographic Test as an Indicator of Fatigue. Psychiatry Clin. Neurosci. 2006, 60, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Gomez, S.; Patel, M.; Berg, S.; Magnusson, M.; Johansson, R.; Fransson, P.A. Effects of Proprioceptive Vibratory Stimulation on Body Movement at 24 and 36h of Sleep Deprivation. Clin. Neurophysiol. 2008, 119, 617–625. [Google Scholar] [CrossRef] [PubMed]
- Nakano, T.; Araki, K.; Michimori, A.; Inbe, H.; Hagiwara, H.; Koyama, E. Nineteen-Hour Variation of Postural Sway, Alertness and Rectal Temperature during Sleep Deprivation. Psychiatry Clin. Neurosci. 2001, 55, 277–278. [Google Scholar] [CrossRef] [PubMed]
- Cerrah, A.O.; Bayram, İ.; Yildizer, G.; Uğurlu, O.; Şïmşek, D.; Ertan, H. Effects of functional balance training on static and dynamic balance performance of adolescent soccer players. Int. J. Sport Exerc. Train. Sci.—IJSETS 2016, 2, 73–81. [Google Scholar] [CrossRef][Green Version]
- Rusek, W.; Adamczyk, M.; Baran, J.; Leszczak, J.; Inglot, G.; Baran, R.; Pop, T. Is There a Link between Balance and Body Mass Composition in Children and Adolescents? Int. J. Environ. Res. Public Health 2021, 18, 10449. [Google Scholar] [CrossRef]
- Caballero, C.; Barbado, D.; Urbán, T.; García-Herrero, J.A.; Moreno, F.J. Functional Variability in Team-Handball Players during Balance Is Revealed by Non-Linear Measures and Is Related to Age and Expertise Level. Entropy 2020, 22, 822. [Google Scholar] [CrossRef]
- Kolimechkov, S.; Petrov, L.; Alexandrova, A. Alpha-fit test battery norms for children and adolescents from 5 to 18 years of age obtained by a linear interpolation of existing european physical fitness references. Eur. J. Phys. Educ. Sport Sci. 2019, 5. [Google Scholar] [CrossRef]
- Thomas, E.; Petrigna, L.; Tabacchi, G.; Teixeira, E.; Pajaujiene, S.; Sturm, D.J.; Sahin, F.N.; Gómez-López, M.; Pausic, J.; Paoli, A.; et al. Percentile Values of the Standing Broad Jump in Children and Adolescents Aged 6-18 Years Old. Eur. J. Transl. Myol. 2020, 30, 9050. [Google Scholar] [CrossRef]
- Chung, L.M.Y.; Chow, L.P.Y.; Chung, J.W.Y. Normative Reference of Standing Long Jump Indicates Gender Difference in Lower Muscular Strength of Pubertal Growth. Health 2013, 5, 6. [Google Scholar] [CrossRef]
- Ramírez-Vélez, R.; Martínez, M.; Correa-Bautista, J.E.; Lobelo, F.; Izquierdo, M.; Rodríguez-Rodríguez, F.; Cristi-Montero, C. Normative Reference of Standing Long Jump for Colombian Schoolchildren Aged 9–17.9 Years: The FUPRECOL Study. J. Strength Cond. Res. 2017, 31, 2083–2090. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Sepúlveda, J.A.; Ramírez-Vélez, R.; Correa-Bautista, J.E.; Izquierdo, M.; García-Hermoso, A. Physical Fitness and Anthropometric Normative Values among Colombian-Indian Schoolchildren. BMC Public Health 2016, 16, 962. [Google Scholar] [CrossRef] [PubMed]
- Beunen, G.; Thomis, M. Muscular Strength Development in Children and Adolescents. Pediatr. Exerc. Sci. 2000, 12, 174–197. [Google Scholar] [CrossRef]
- Eisenmann, J.C.; Malina, R.M. Age- and Sex-Associated Variation in Neuromuscular Capacities of Adolescent Distance Runners. J. Sport. Sci. 2003, 21, 551–557. [Google Scholar] [CrossRef] [PubMed]
- Vänttinen, T.; Blomqvist, M.; Nyman, K.; Häkkinen, K. Changes in Body Composition, Hormonal Status, and Physical Fitness in 11-, 13-, and 15-Year-Old Finnish Regional Youth Soccer Players during a Two-Year Follow-Up. J. Strength Cond. Res. 2011, 25, 3342–3351. [Google Scholar] [CrossRef]
- Racil, G.; Coquart, J.; Elmontassar, W.; Haddad, M.; Goebel, R.; Chaouachi, A.; Amri, M.; Chamari, K. Greater Effects of High- Compared with Moderate-Intensity Interval Training on Cardio-Metabolic Variables, Blood Leptin Concentration and Ratings of Perceived Exertion in Obese Adolescent Females. Biol. Sport 2016, 33, 145–152. [Google Scholar] [CrossRef]
- Welde, B.; Morseth, B.; Handegård, B.H.; Lagestad, P. Effect of Sex, Body Mass Index and Physical Activity Level on Peak Oxygen Uptake Among 14-19 Years Old Adolescents. Front. Sport. Act. Living 2020, 2, 78. [Google Scholar] [CrossRef]
- Berthoin, S.; Baquet, G.; Mantéca, F.; Lensel-Corbeil, G.; Gerbeaux, M. Maximal Aerobic Speed and Running Time to Exhaustion for Children 6 to 17 Years Old. Pediatr. Exerc. Sci. 1996, 8, 234–244. [Google Scholar] [CrossRef]


{kind=link}
| Group | U14 N = 36 | U17 N = 36 |
|---|---|---|
| PS (II–III/IV–V) Height (m) | 15/21 1.64 ± 0.04 | 17/19 1.67 ± 0.05 * |
| Body mass (kg) | 57.83 ± 5.79 | 59.21 ± 6.16 * |
| Body mass index (kg m−2) | 21.49 ± 1.52 | 21.22 ± 1.63 * |
| Body fat (%) | 24.45 ± 1.5 | 22.27 ± 1.3 |
| Lean body mass (kg) | 43.95 ± 2.7 | 46.18 ± 3.1 * |
| Group | PSQI | ISI | ESS |
|---|---|---|---|
| Group U14 | 5.44 ± 1.576 | 7.19 ± 2.649 | 6.36 ± 1.91 |
| Group U17 | 5.47 ± 1.540 | 7.50 ± 2.49 | 6.31 ± 1.89 |
| Variables | Group U14 | Group U17 | Average of the 2 Groups |
|---|---|---|---|
| PSQI ≥ 5 | 61.1% | 63.8% | 62.45% |
| PSQI < 5 | 38.9% | 36.2% | 37.55% |
| ISI ≥ 11 | 8.3% | 8.4% | 8.35% |
| ISI < 11 | 91.7% | 91.6% | 91.65% |
| ESS > 8 | 19.4% | 22.3% | 20.85% |
| ESS < 8 | 80.6% | 77.7% | 79.15% |
| Group | OEB | CEB | SJ | SBJ | FJT | t-Test | VAMEVAL |
|---|---|---|---|---|---|---|---|
| U14 | 11.01 ± 8.52 | 2.88 ± 0.86 | 24.8 ± 5.38 | 1.59 ± 0.20 | 9.12 ± 0.54 | 12.8± 1.11 | 12.2 ± 1.35 |
| U17 | 10.49 ± 9.75 | 2.24 ± 1.11 | 28.5 ± 4.04 | 1.66 ± 0.20 | 8.90 ±0.98 | 11.7 ** ± 0.59 | 12.69 * ± 0.91 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guembri, M.A.; Racil, G.; Dhouibi, M.-A.; Coquart, J.; Souissi, N. Evaluation of Age Based-Sleep Quality and Fitness in Adolescent Female Handball Players. Int. J. Environ. Res. Public Health 2023, 20, 330. https://doi.org/10.3390/ijerph20010330
Guembri MA, Racil G, Dhouibi M-A, Coquart J, Souissi N. Evaluation of Age Based-Sleep Quality and Fitness in Adolescent Female Handball Players. International Journal of Environmental Research and Public Health. 2023; 20(1):330. https://doi.org/10.3390/ijerph20010330
Chicago/Turabian StyleGuembri, Mohamed Alaeddine, Ghazi Racil, Mohamed-Ali Dhouibi, Jeremy Coquart, and Nizar Souissi. 2023. "Evaluation of Age Based-Sleep Quality and Fitness in Adolescent Female Handball Players" International Journal of Environmental Research and Public Health 20, no. 1: 330. https://doi.org/10.3390/ijerph20010330
APA StyleGuembri, M. A., Racil, G., Dhouibi, M.-A., Coquart, J., & Souissi, N. (2023). Evaluation of Age Based-Sleep Quality and Fitness in Adolescent Female Handball Players. International Journal of Environmental Research and Public Health, 20(1), 330. https://doi.org/10.3390/ijerph20010330