
Future Possible Changes in Medically Underserved Areas in Japan: A Geographic Information System-Based Simulation Study



{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics Statements
2.2. Study Design
2.3. Definition and Analysis
3. Results
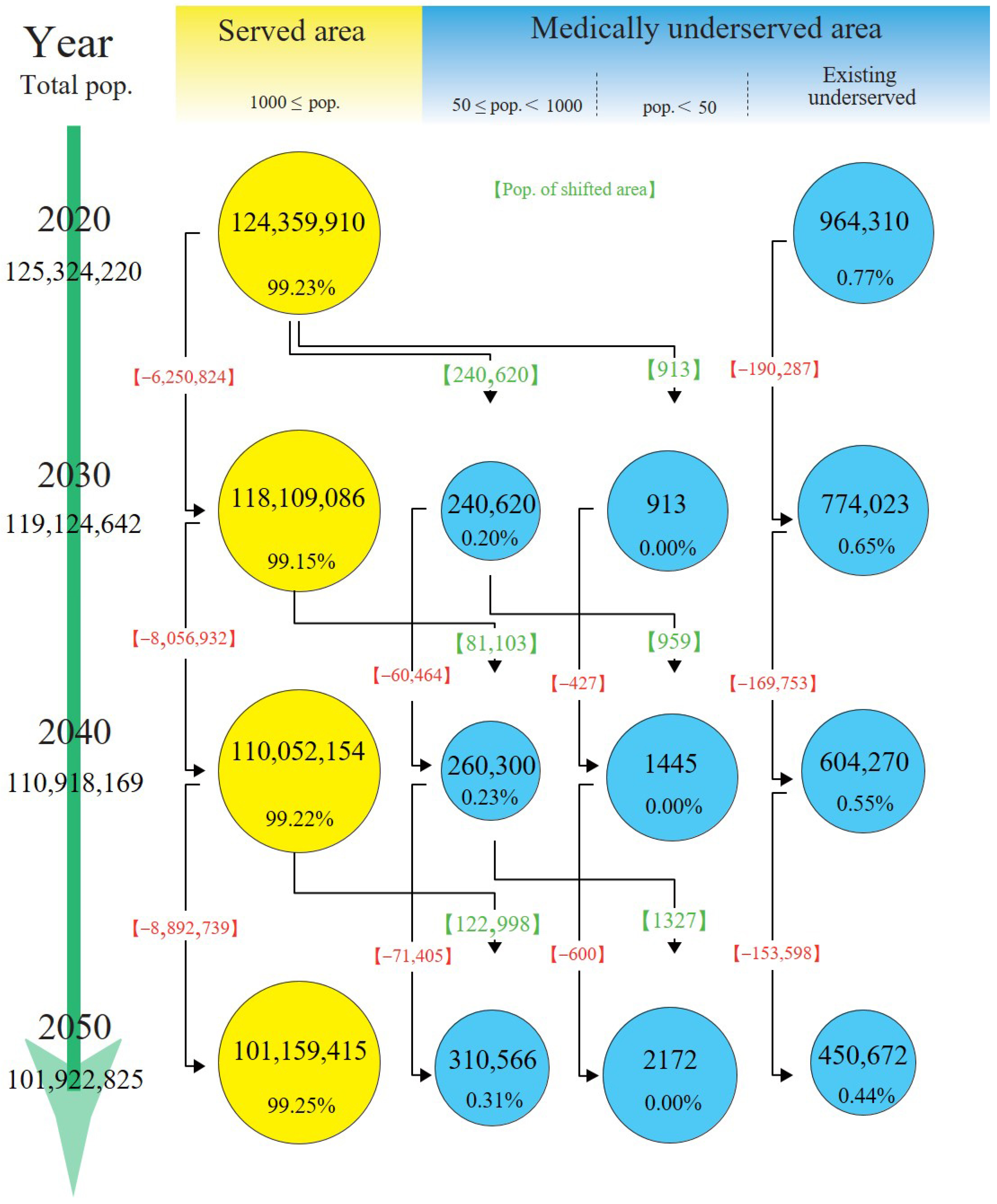
3.1. Population Trends
3.2. Land Area Trends
3.3. Estimated Number of Medical Institutions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations, Department of Economic and Social Affairs. World Population Prospects. 2019. Available online: https://population.un.org/wpp/publications/files/wpp2019_highlights.pdf (accessed on 16 January 2024).
- Grau, H.R.; Aide, M. Globalization and land-use transitions in Latin America. Ecol. Soc. 2008, 13, 16. [Google Scholar] [CrossRef]
- Karcagi Kováts, A.; Katona Kovács, J. Factors of population decline in rural areas and answers given to them identified in strategies. Stud. Agric. Econ. 2012, 114, 49–56. [Google Scholar] [CrossRef]
- Lim, A.; Asher, M.I.; Ellwood, E.; Ellwood, P.; Exeter, D.J. How are ‘urban’ and ‘rural’ defined in publications regarding asthma and related diseases. Allergol. Immunopathol. 2014, 42, 157–161. [Google Scholar] [CrossRef]
- Diaz, A.; Pawlik, T.M. Rural surgery and status of the rural workplace: Hospital survival and economics. Surg. Clin. North Am. 2020, 100, 835–847. [Google Scholar] [CrossRef] [PubMed]
- Brundell, K.; Vasilevski, V.; Farrell, T.; Sweet, L. Rural maternity and media discourse analysis: Framing new narratives. Aust. J. Rural Health 2023, 31, 395–407. [Google Scholar] [CrossRef] [PubMed]
- Meade, Z.S.; Li, H.W.; Allison, H.; Bhatia, M.B.; Joplin, T.S.; Simon, C.; Darkwa, L.; Keung, C.; McDow, A.D. Demographics and medical school exposures to rural health influence future practice. Surgery 2022, 172, 1665–1672. [Google Scholar] [CrossRef]
- Randle, T.; Garg, A.; Mago, V.; Choudhury, S.; Ohle, R.; Strasser, R.; Moore, S.W.; Kernick, A.; Savage, D.W. Staffing rural emergency departments in Ontario: The who, what and where. Can. J. Rural Med. 2023, 28, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Cabinet Office Japan. Annual Report on the Ageing Society [Summary] FY2021. Available online: https://www8.cao.go.jp/kourei/english/annualreport/2021/pdf/2021.pdf (accessed on 16 January 2024).
- Digital National Land Information. Available online: https://nlftp.mlit.go.jp/ksj/gml/datalist/KsjTmplt-mesh1000h30.html (accessed on 16 January 2024).
- Ministry of Health, Labour and Welfare. Labour and Welfare White Paper 2020 Edition, Health and Medical Services. Available online: https://www.mhlw.go.jp/english/wp/wp-hw13/dl/02e.pdf (accessed on 16 January 2024).
- Kashima, S.; Inoue, K.; Matsumoto, M.; Takeuchi, K. Non-physician communities in Japan: Are they still disadvantaged. Rural Remote Health 2014, 14, 2907. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare. Measures for Health and Medical Services in Remote Areas. Available online: https://www.mhlw.go.jp/web/t_doc?dataId=00ta6714&dataType=1&pageNo=1 (accessed on 16 January 2024). (In Japanese)
- Ministry of Health, Labour and Welfare. About Rural Medical Care. Available online: https://www.mhlw.go.jp/stf/newpage_20900.html (accessed on 16 January 2024).
- Teraura, H.; Kotani, K.; Sato, E.; Koike, S. The attributes of physicians assigned to rural clinics designated for areas without physicians in Japan. Tohoku J. Exp. Med. 2023, 261, 273–281. [Google Scholar] [CrossRef]
- Wang, F. Why public health needs GIS: A methodological overview. Ann. GIS 2020, 26, 1–12. [Google Scholar] [CrossRef]
- Nykiforuk, C.I.; Flaman, L.M. Geographic information systems (GIS) for health promotion and public health: A review. Health Promot. Pract. 2011, 12, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Rushton, G. Public health, GIS, and spatial analytic tools. Annu. Rev. Public Health 2003, 24, 43–56. [Google Scholar] [CrossRef]
- Boulos, M.N. Towards evidence-based, GIS-driven national spatial health information infrastructure and surveillance services in the United Kingdom. Int. J. Health Geogr. 2004, 3, 1. [Google Scholar] [CrossRef] [PubMed]
- Guagliardo, M.F. Spatial accessibility of primary care: Concepts, methods and challenges. Int. J. Health Geogr. 2004, 3, 3. [Google Scholar] [CrossRef] [PubMed]
- Sanati, N.A.; Sanati, M. Growing interest in use of geographic information systems in health and healthcare research: A review of PubMed from 2003 to 2011. JRSM Short Rep 2013, 4, 2042533313478810. [Google Scholar] [CrossRef] [PubMed]
- Shaw, N.; McGuire, S. Understanding the use of geographical information systems (GIS) in health informatics research: A review. J. Innov. Health Inform. 2017, 24, 940. [Google Scholar] [CrossRef] [PubMed]
- Leosari, Y.; Uelmen, J.A.; Carney, R.M. Spatial evaluation of healthcare accessibility across archipelagic communities of Maluku Province, Indonesia. PLoS Glob. Public Health 2023, 3, e0001600. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T.; Nakamura, A.; Mukuda, K.; Harada, M.; Kotani, K. Potential accessibility scores for hospital care in a province of Japan: GIS-based ecological study of the two-step floating catchment area method and the number of neighborhood hospitals. BMC Health Serv. Res. 2017, 17, 438. [Google Scholar] [CrossRef] [PubMed]
- McGrail, M.R. Spatial accessibility of primary health care utilising the two step floating catchment area method: An assessment of recent improvements. Int. J. Health Geogr. 2012, 11, 50. [Google Scholar] [CrossRef] [PubMed]
- Cervigni, F.; Suzuki, Y.; Ishii, T.; Hata, A. Spatial accessibility to pediatric services. J. Community Health 2008, 33, 444–448. [Google Scholar] [CrossRef]
- Doi, S.; Inoue, T.; Ide, H.; Nakamura, T.; Fujita, S.; Suzuki, T.; Takabayashi, K. Using geographic information systems to simulate patient access areas. Stud. Health Technol. Inform. 2014, 205, 1120–1124. [Google Scholar] [PubMed]
- Calovi, M.; Seghieri, C. Using a GIS to support the spatial reorganization of outpatient care services delivery in Italy. BMC Health Serv. Res. 2018, 18, 883. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Koike, S.; Matsumoto, M. Effect and significance of incorporating access in estimating the number of required physicians: Focus on differences in population density in the target area. Int. J. Health Geogr. 2021, 20, 21. [Google Scholar] [CrossRef] [PubMed]
- Institute for Health Economics and Policy. Publications. Available online: https://www.ihep.jp/publications/other/?y=2018 (accessed on 16 January 2024). (In Japanese).
- Hori, K.; Saito, O.; Hashimoto, S.; Matsui, T.; Akter, R.; Takeuchi, K. Projecting population distribution under depopulation conditions in Japan: Scenario analysis for future socio-ecological systems. Sustain. Sci. 2021, 16, 295–311. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.P.; Bentham, G.; Horwell, C. Health service accessibility and deaths from asthma. Int. J. Epidemiol. 1999, 28, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Freitas, P.F.; Drachler, M.L.; Leite, J.C.; Marshall, T. Inequalities in cesarean delivery rates by ethnicity and hospital accessibility in Brazil. Int. J. Gynaecol. Obstet. 2009, 107, 198–201. [Google Scholar] [CrossRef]
- Ambroggi, M.; Biasini, C.; Del Giovane, C.; Fornari, F.; Cavanna, L. Distance as a barrier to cancer diagnosis and treatment: Review of the literature. Oncologist 2015, 20, 1378–1385. [Google Scholar] [CrossRef] [PubMed]
- Jarosławski, S.; Jarosławska, B.; Błaszczyk, B.; Auqier, P.; Toumi, M. Health-related quality of life of patients after ischaemic stroke treated in a provincial hospital in Poland. J. Mark. Access Health Policy 2020, 8, 1775933. [Google Scholar] [CrossRef] [PubMed]
- O’Meara, P.F.; Kendall, D.; Kendall, L. Working together for a sustainable urgent care system: A case study from south eastern Australia. Rural Remote Health 2004, 4, 312. [Google Scholar] [CrossRef]
- Ministry of Health and Long Term Care. Northern Physician Retention Initiative. Available online: https://www.ontario.ca/document/northern-health-programs/northern-physician-retention-initiative (accessed on 16 January 2024).
- Cherry, J.J.; Rich, W.C.; McLennan, P.L. Telemedicine in remote Australia: The Royal Flying Doctor Service (RFDS) Medical Chest Program as a marker of remote health. Rural Remote Health 2018, 18, 4502. [Google Scholar] [CrossRef]
- Teraura, H.; Iguchi, S.; Maeda, T.; Koike, S.; Matsumoto, M.; Haruyama, S.; Kotani, K. The use of information and communication technology in Japanese rural clinics. J. Rural Med. 2021, 16, 298–300. [Google Scholar] [CrossRef] [PubMed]
- Saint Onge, J.M.; Smith, S. Demographics in Rural Populations. Surg. Clin. North Am. 2020, 100, 823–833. [Google Scholar] [CrossRef] [PubMed]
- Kotani, K. The framework for modern community medicine in Japan. Biosci. Trends 2023, 17, 322–324. [Google Scholar] [CrossRef] [PubMed]
- Lehtonen, O. Population grid-based assessment of the impact of broadband expansion on population development in rural areas. Telecomm. Policy 2020, 44, 102028. [Google Scholar] [CrossRef] [PubMed]
- Townsend, L.; Sathiaseelan, A.; Fairhurst, G.; Wallace, C. Enhanced broadband access as a solution to the social and economic problems of the rural digital divide. Local Econ. 2013, 28, 580–595. [Google Scholar] [CrossRef]
- Eurostat. Fertility Statistics: France with the Highest and Malta with the Lowest Total Fertility Rate in 2022. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Fertility_statistics#France_with_the_highest_and_Malta_with_the_lowest_total_fertility_rate_in_2022 (accessed on 8 April 2024).
- United Nations Expert Group Meeting on Policy Reponses to Low Fertility. The Influence of Family Policies on Fertility in France. Available online: https://www.eastwestcenter.org/publications/the-influence-family-policies-fertility-in-france#:~:text=French%20family%20policies%20have%20evolved,workforce%20participation%20of%20both%20parents (accessed on 8 April 2024).
- Song, P.; Tang, W. The community-based integrated care system in Japan: Health care and nursing care challenges posed by super-aged society. Biosci. Trends 2019, 13, 279–281. [Google Scholar] [CrossRef]
- Hasegawa, T.; Matsumoto, K.; Onishi, R.; Hirata, K. Social and health sector reform towards 2040 in Japan. Public Adm. Policy Asia-Pacific J. 2020, 23, 259–271. [Google Scholar] [CrossRef]
- Children and Families Agency, Government of Japan. Outline of the Act Establishing the Children and Families Agency (Act No. 75 of 2022). Available online: https://www.cfa.go.jp/en/act-establishing-the-CFA-en/ (accessed on 8 April 2024).
- Cabinet Secretariat. Regional Empowerment for Japan’s Growth. Available online: https://www.japan.go.jp/regions/_userdata/pdf/A4_12P.pdf (accessed on 8 April 2024).



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakamura, A.; Satoh, E.; Suzuki, T.; Koike, S.; Kotani, K. Future Possible Changes in Medically Underserved Areas in Japan: A Geographic Information System-Based Simulation Study. J. Mark. Access Health Policy 2024, 12, 118-127. https://doi.org/10.3390/jmahp12020010
Nakamura A, Satoh E, Suzuki T, Koike S, Kotani K. Future Possible Changes in Medically Underserved Areas in Japan: A Geographic Information System-Based Simulation Study. Journal of Market Access & Health Policy. 2024; 12(2):118-127. https://doi.org/10.3390/jmahp12020010
Chicago/Turabian StyleNakamura, Akihisa, Eiji Satoh, Tatsuya Suzuki, Soichi Koike, and Kazuhiko Kotani. 2024. "Future Possible Changes in Medically Underserved Areas in Japan: A Geographic Information System-Based Simulation Study" Journal of Market Access & Health Policy 12, no. 2: 118-127. https://doi.org/10.3390/jmahp12020010
APA StyleNakamura, A., Satoh, E., Suzuki, T., Koike, S., & Kotani, K. (2024). Future Possible Changes in Medically Underserved Areas in Japan: A Geographic Information System-Based Simulation Study. Journal of Market Access & Health Policy, 12(2), 118-127. https://doi.org/10.3390/jmahp12020010