
Mobile Application for Real-Time Food Plan Management for Alzheimer Patients through Design-Based Research


Abstract
1. Introduction
2. Related Work
3. Materials and Methods
3.1. Design-Based Approach
- The application should be intuitive and easy to use;
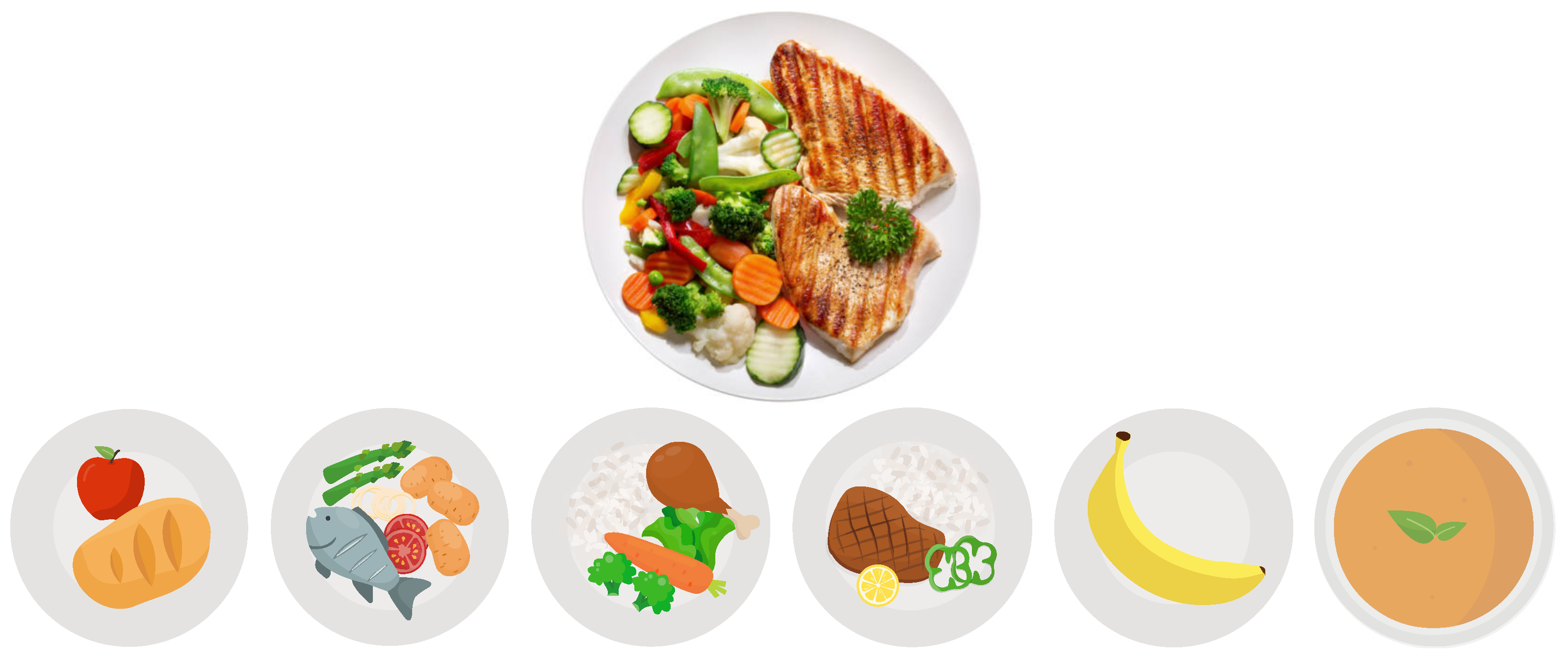
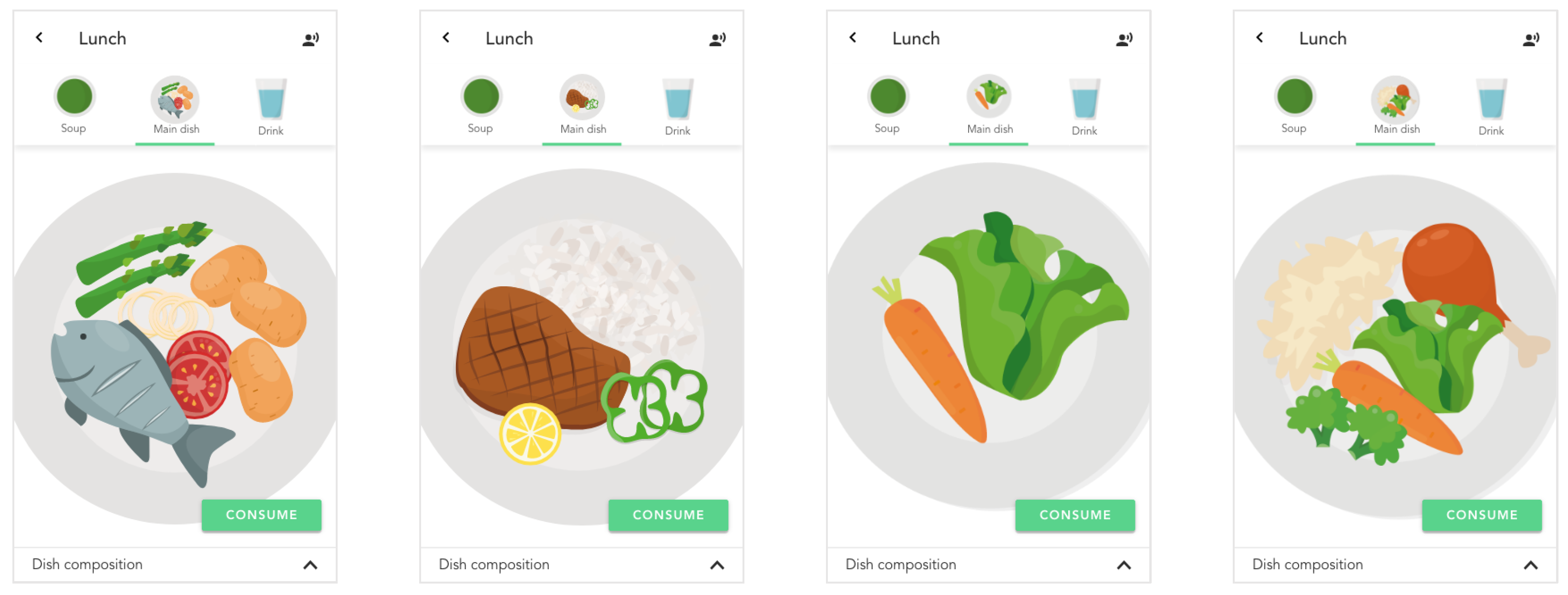
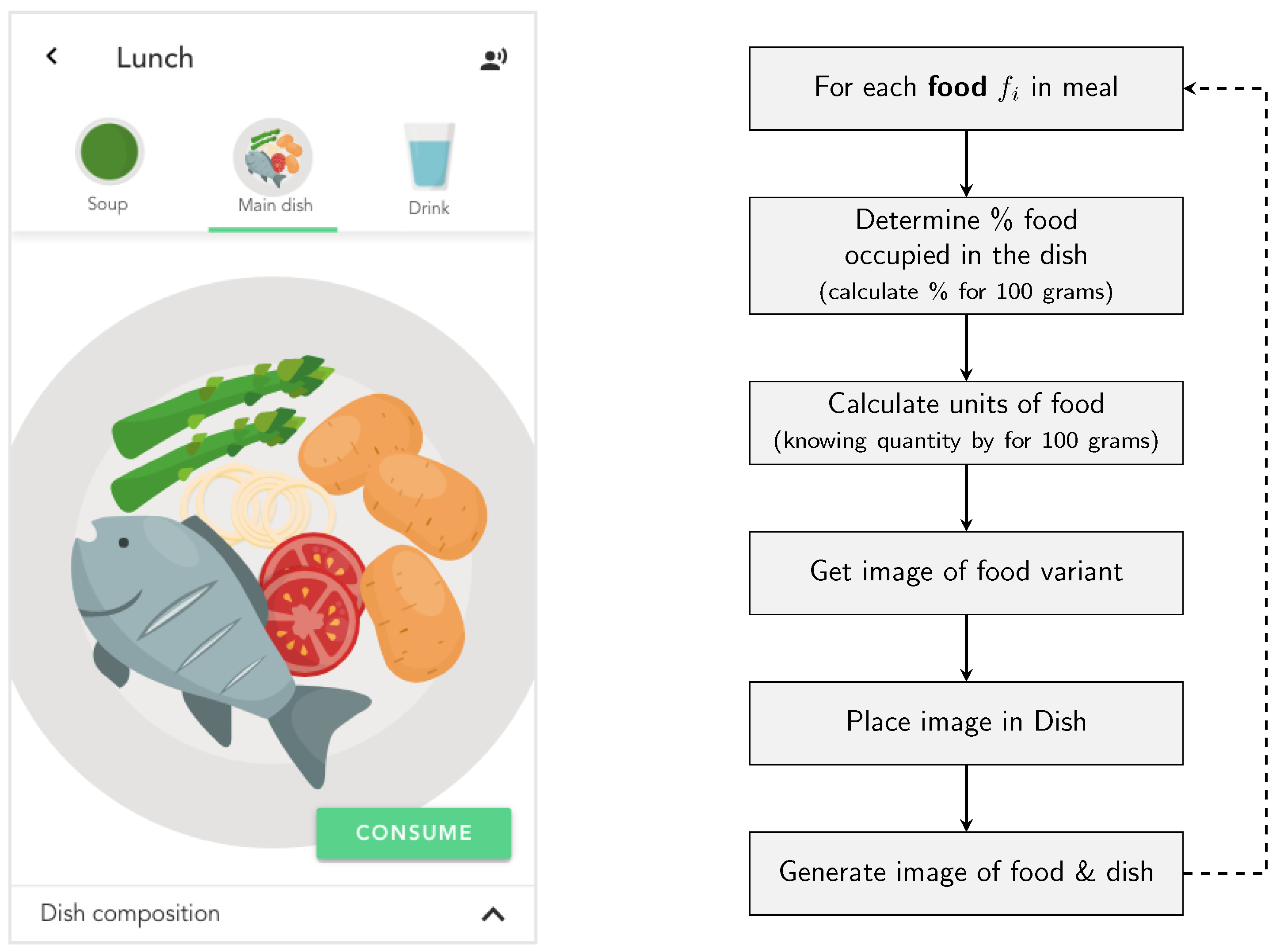
- The application should map the real concept of what a meal is and use visual markers for better identification of components;
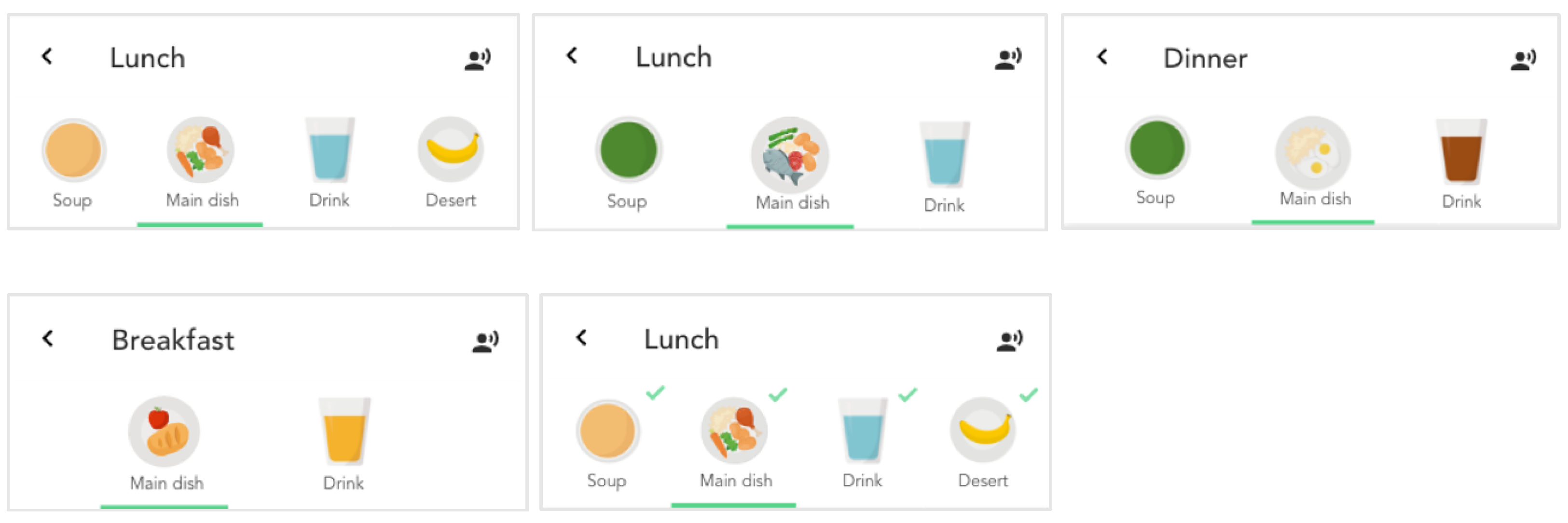
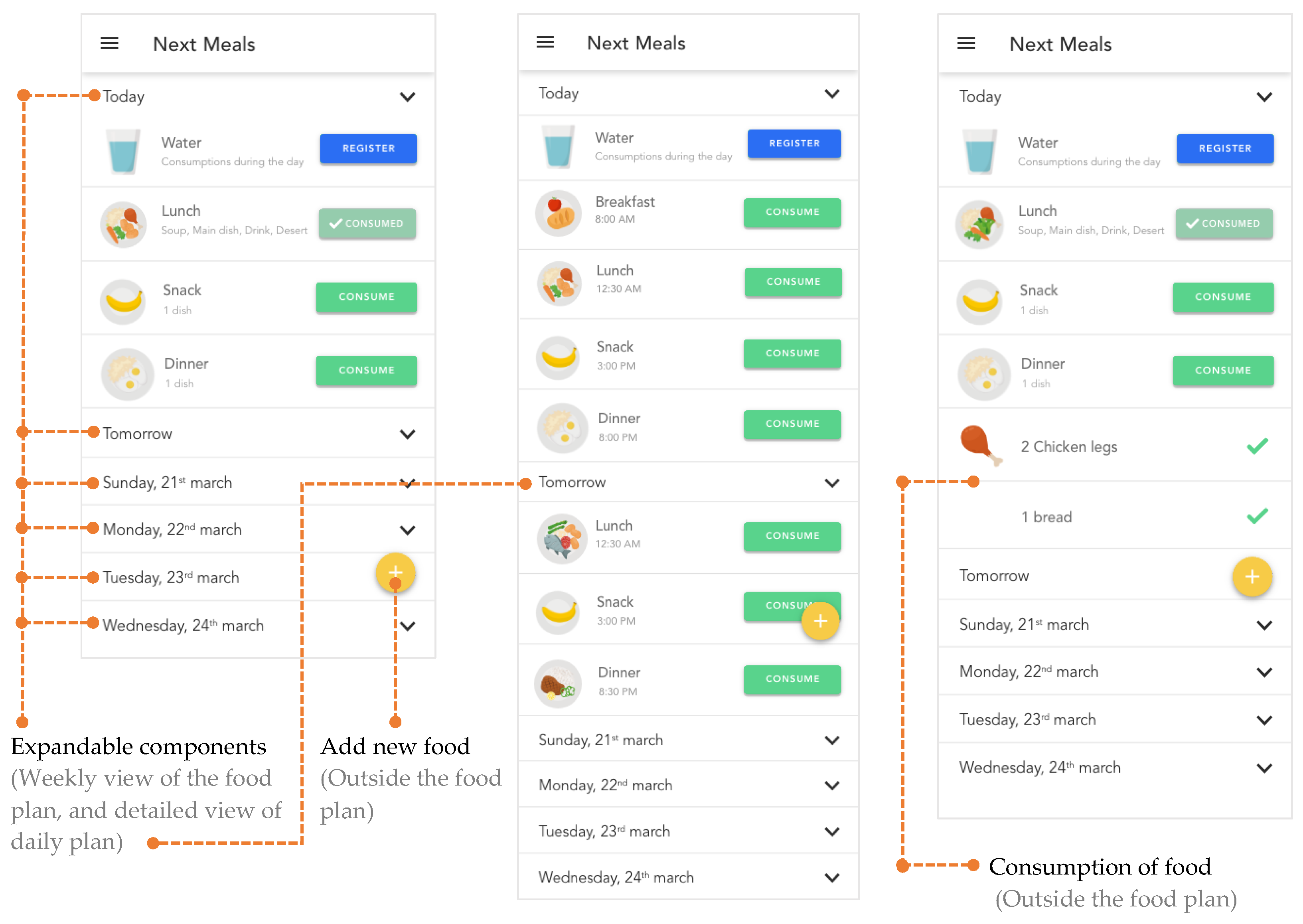
- Make available a weekly list of meals provided by the nutritionist so that the caregiver or patient can plan and anticipate the meals for that week;
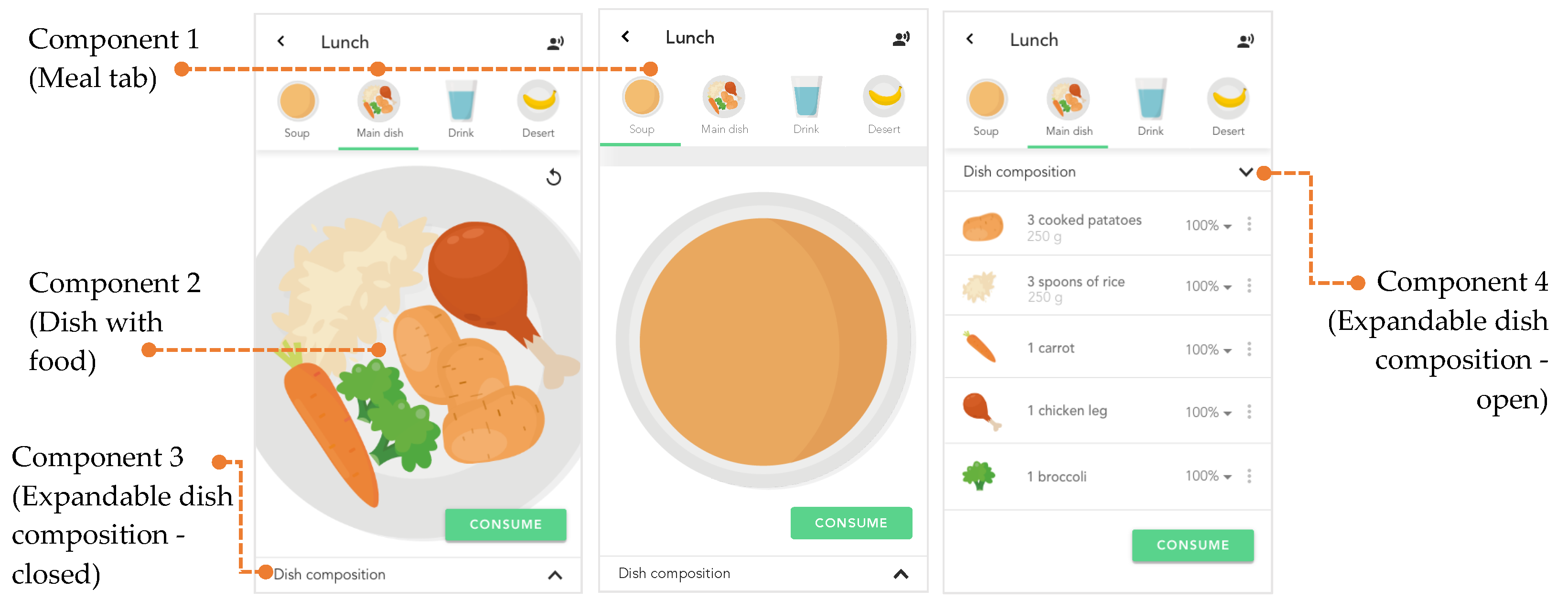
- Provide a detailed view of each meal and use visual markers for each food;
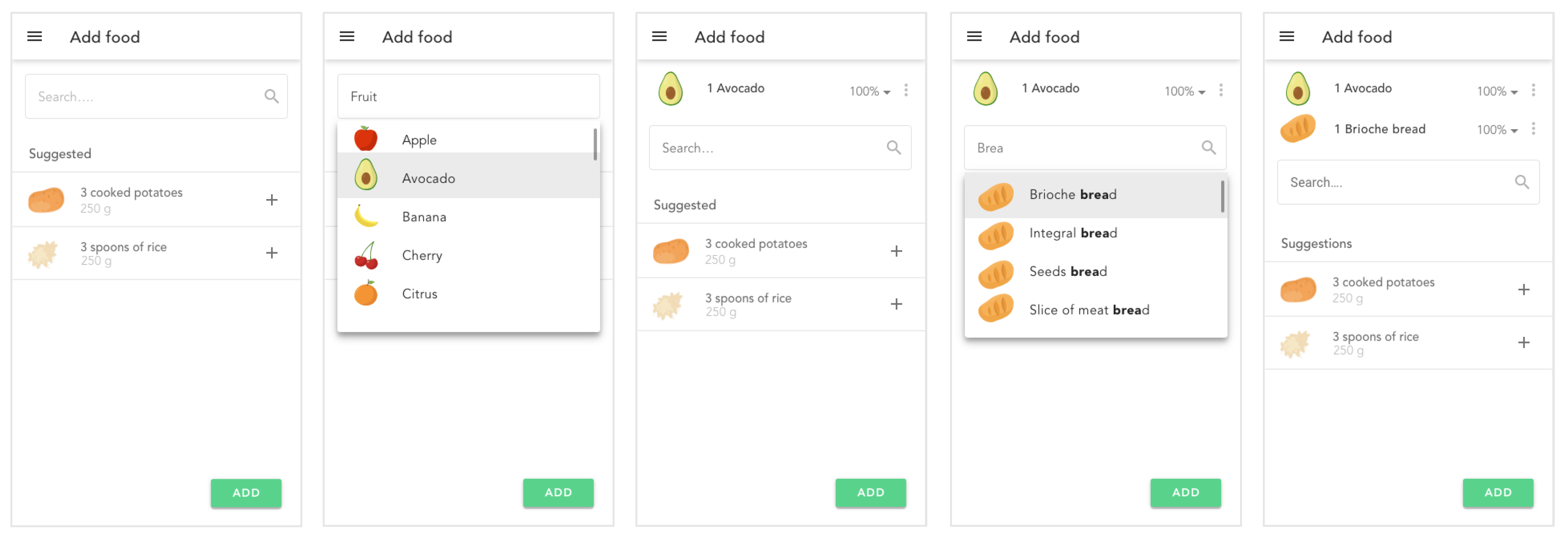
- Allow the change of food in a meal for an equivalent (with the same nutritional value);
- Register the consumption of macro-nutrients, micro-nutrients, and water consumed in each meal of the food plan;
- Provide the user with information on discrepancies between the defined nutrients and real consumption through statistics;
- Push notifications for scheduled meals.
3.2. Participants and Tasks
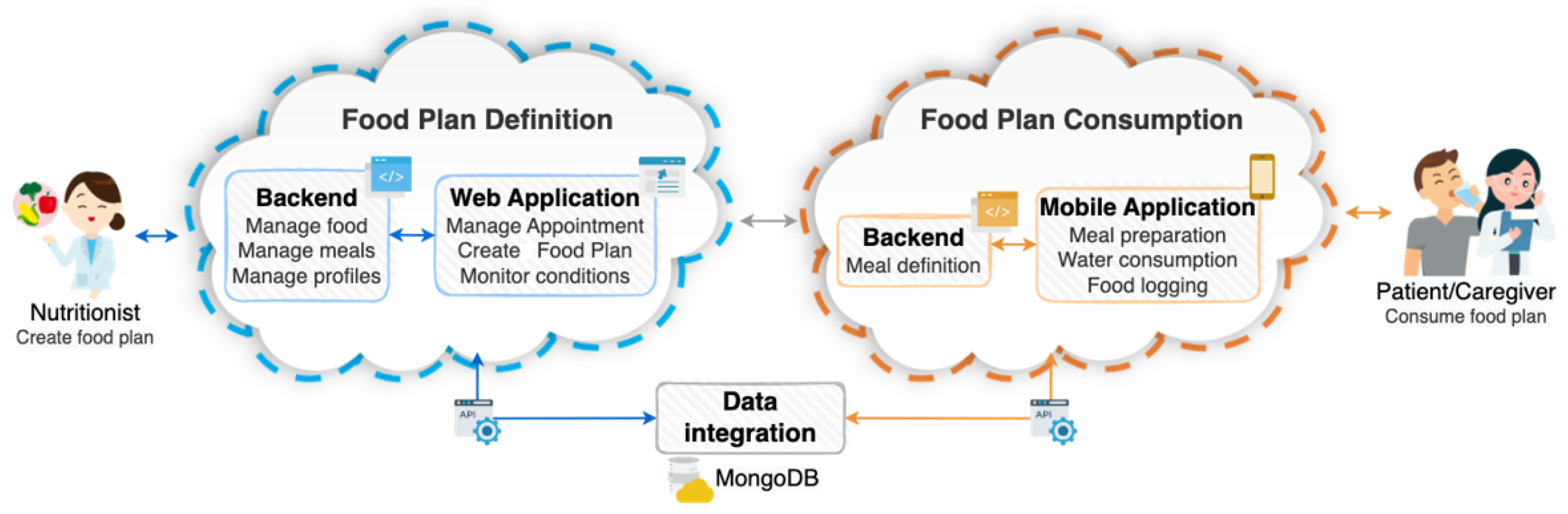
3.3. System Architecture
4. Application Features
4.1. Mapping Real World Food Plans
4.2. Components
4.2.1. Import Meal
4.2.2. Weekly View of Food Plan
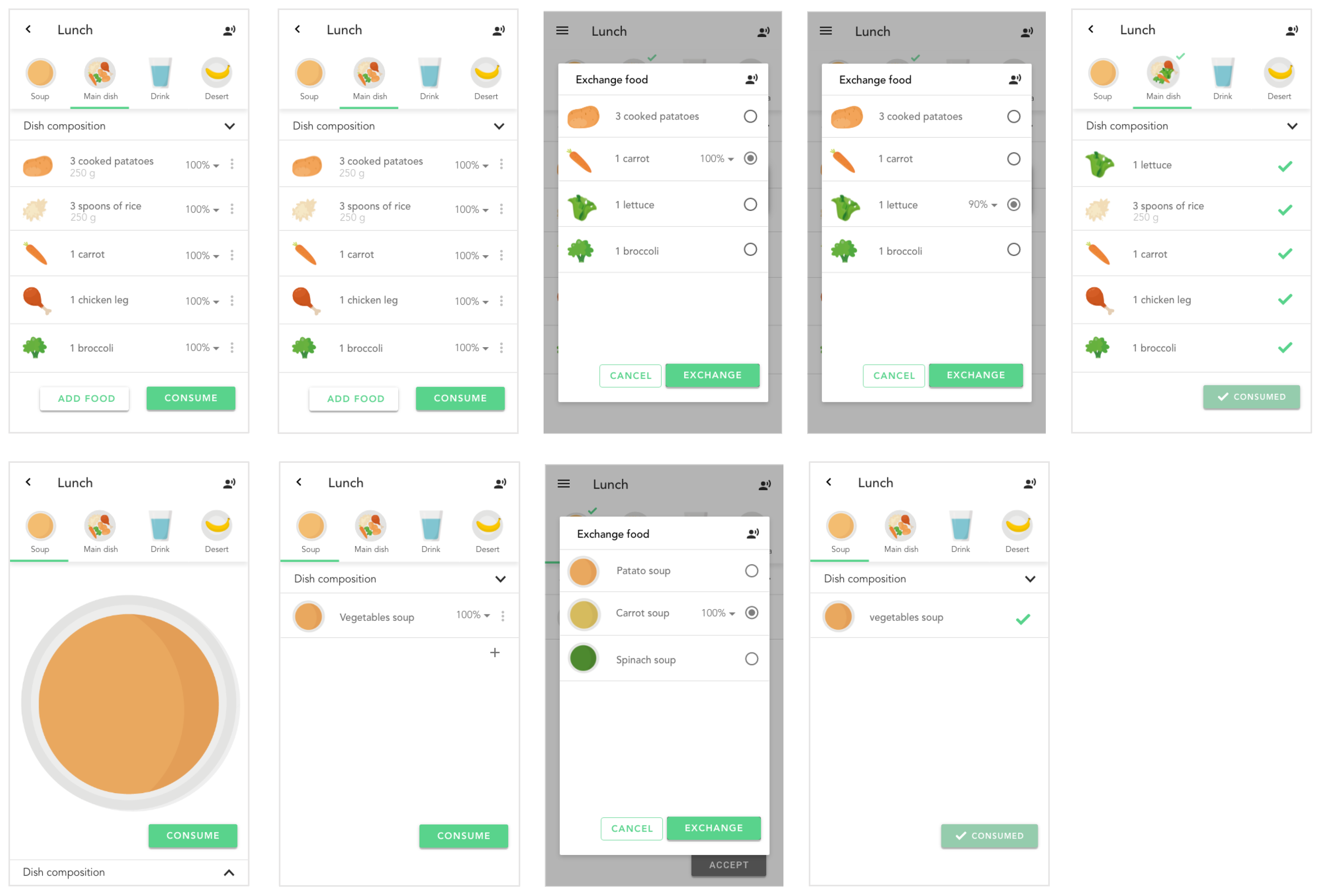
4.2.3. Operations on Food and Meal
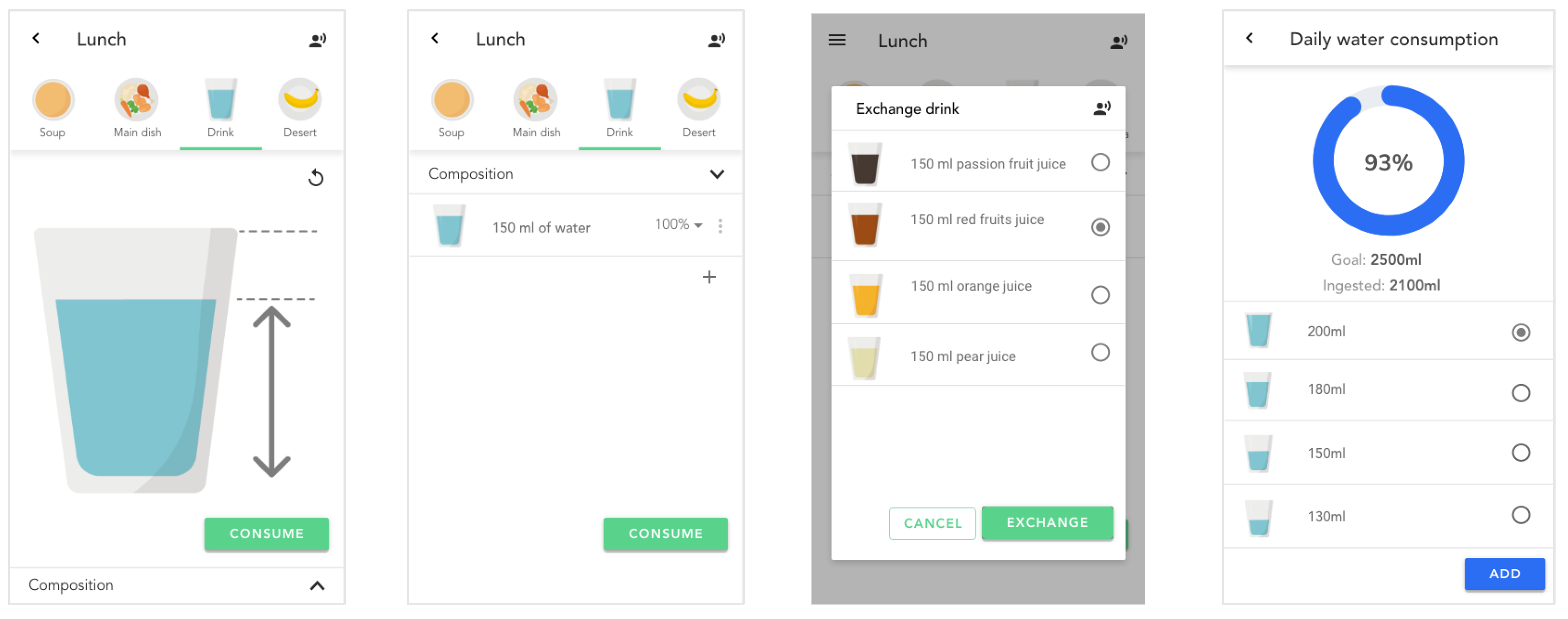
4.2.4. Water Consumption
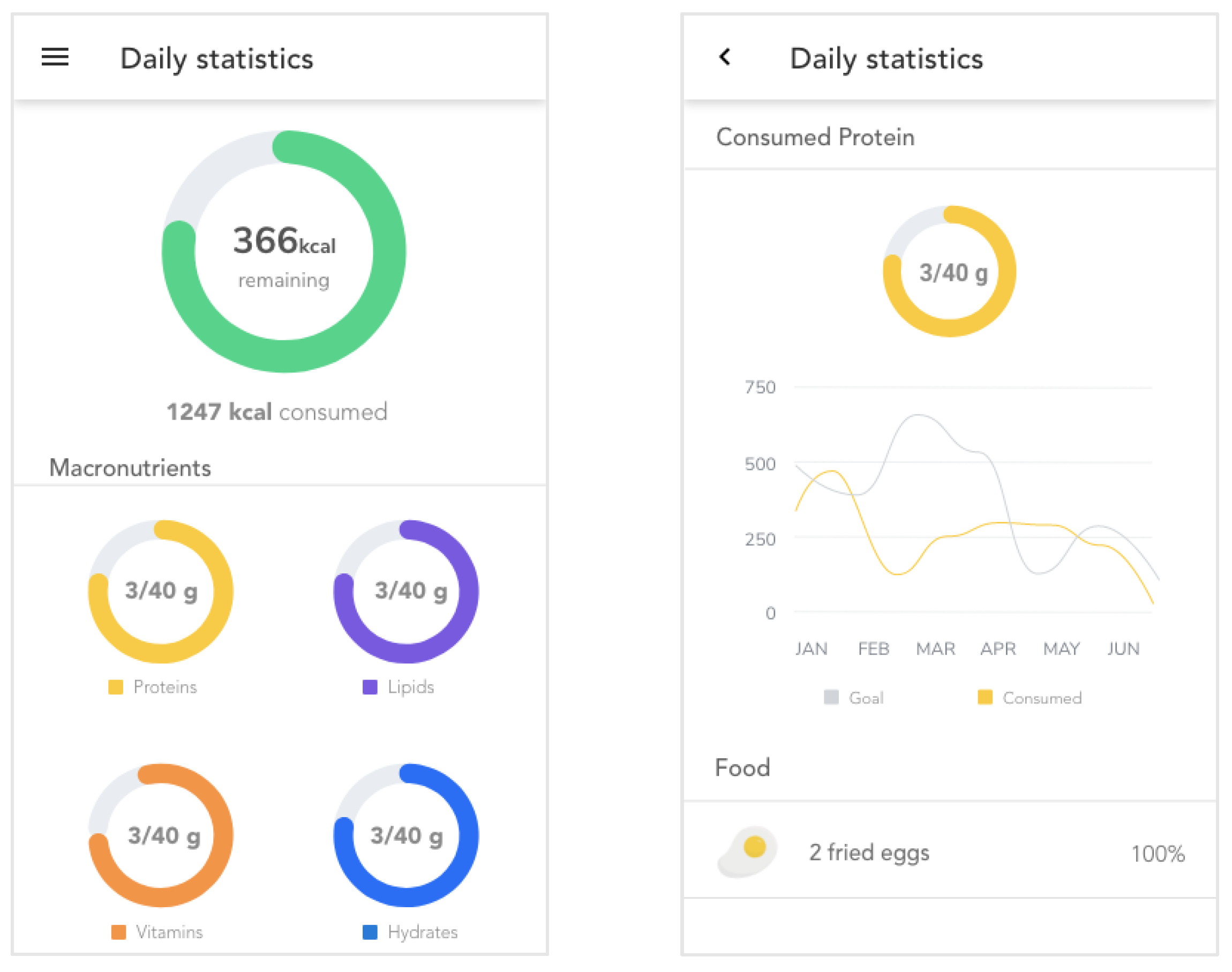
4.2.5. Macronutrients Statistics
5. Evaluation
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
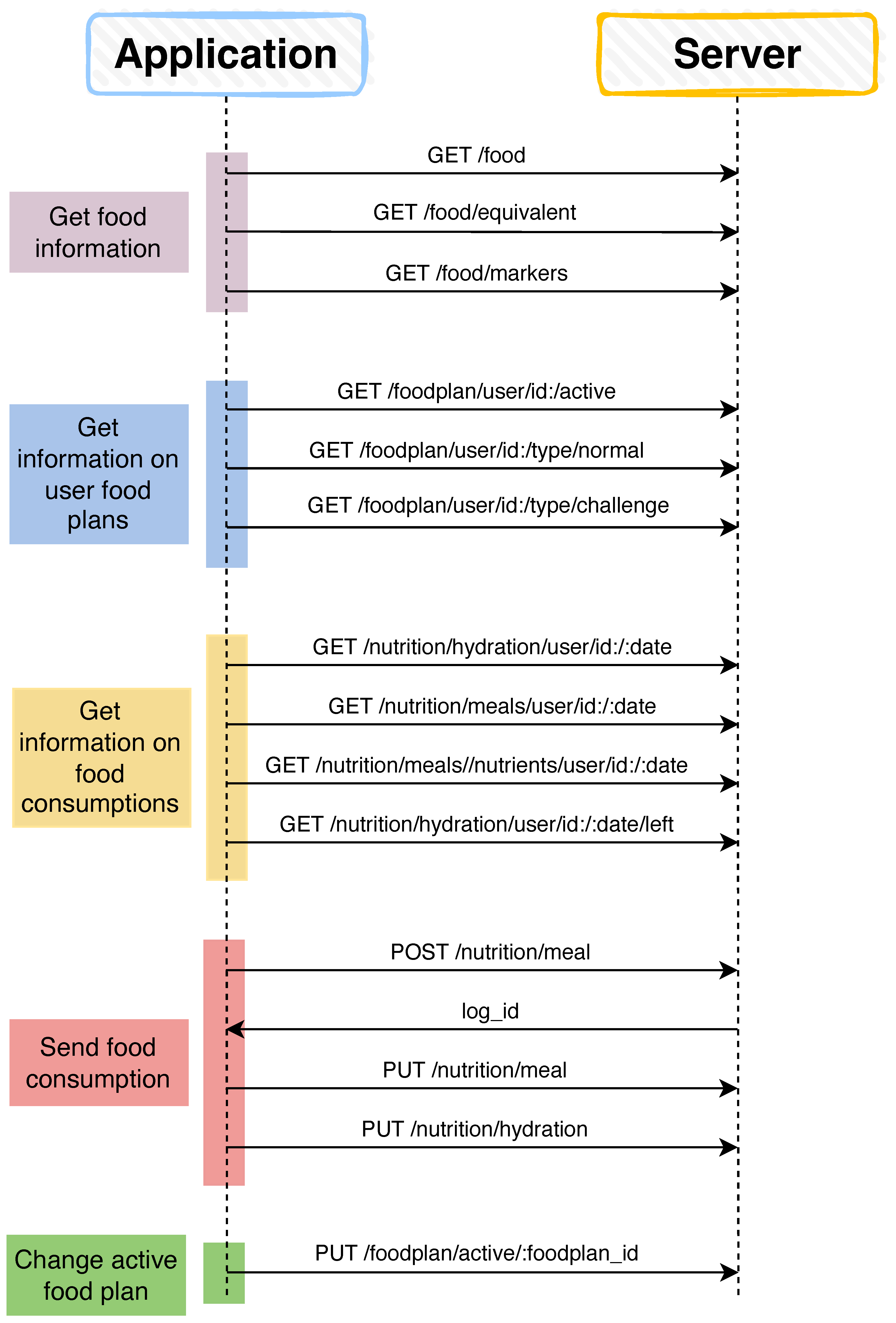
Appendix A. List of Server Requests

Appendix B. Categories and Contexts of Food Products

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Fruits | ||||||||
| Star fruit | Banana | Persimmon | Apple | Avocado | Cherry | Pomegranate | Peach | Strawberry |
 |  |  |  |  |  |  |  |  |
| Lemon | Fig | Raspberry | Pumpkin | Melon | Quince | Citrus | Grapes | Mango |
 |  |  |  |  |  |  |  |  |
| Papaya | Pineapple | Plum | Kiwi | Watermelon | Pear | Tomato | ||
 |  |  |  |  |  |  | ||
| Drinks | ||||||||
| Water | Natural Juices | Coffee | Wine | Beer | Carbonated Drinks | Milk | Tea | |
 |  |  |  |  |  |  |  | |
| Deserts and sweet food | ||||||||
| Pudding | Ice-cream | Cake | Chocolate | Cookie | Gelatin | Cream | Jam | |
 |  |  |  |  |  |  |  | |
| Vegetables | ||||||||
| Artichoke | Peas | Turnip | Peeper | Salad | Cucumber | Radish | Asparagus | |
 |  |  |  |  |  |  |  | |
| Carrot | Broccoli | Courgette | Garlic | Eggplant | Onion | Mushroom | ||
 |  |  |  |  |  |  | ||
| Proteins | ||||||||
| Sausage | Salty meat | Poultry meat | Meat | Finger food | Egg | Fish | ||
 |  |  |  |  |  |  | ||
| Other categories | ||||||||
| Dry fruits | Beans | Truffle | Soup | Cinnamon | Tofu | |||
 |  |  |  |  |  | |||
| Carbohydrates | ||||||||
| Pasta | Rice | Cereals | Potato | Bread | ||||
 |  |  |  |  | ||||
| Milk derivatives | ||||||||
| Yogurt | Cheese | Butter | ||||||
 |  |  | ||||||
| 200% | 150% | 100% | 75% | 50% | 25% |
 |  |  |  |  |  |
 |  |  |  |  |  |
 |  |  |  |  |  |
 |  |  |  |  |  |
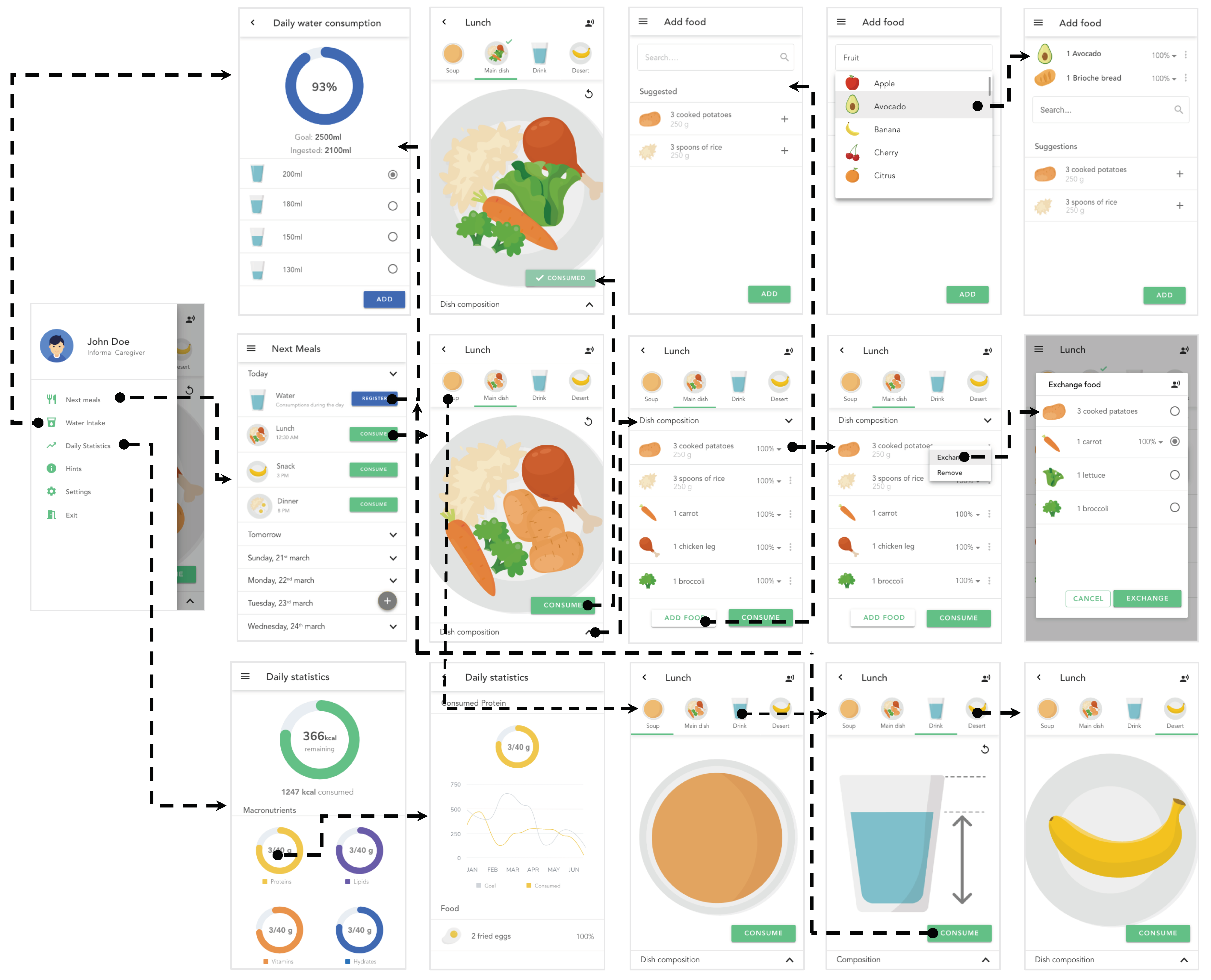
Appendix C. Navigation Scheme

References
- Association, A. 2016 Alzheimer’s disease facts and figures. Alzheimer’s Dement. 2016, 12, 459–509. [Google Scholar] [CrossRef] [PubMed]
- Spijker, A.; Vernooij-Dassen, M.; Vasse, E.; Adang, E.; Wollersheim, H.; Grol, R.; Verhey, F. Effectiveness of Nonpharmacological Interventions in Delaying the Institutionalization of Patients with Dementia: A Meta-Analysis. J. Am. Geriatr. Soc. 2008, 56, 1116–1128. [Google Scholar] [CrossRef] [PubMed]
- Hebert, L.E.; Weuve, J.; Scherr, P.A.; Evans, D.A. Alzheimer disease in the United States (2010–2050) estimated using the 2010 census. Neurology 2013, 80, 1778–1783. [Google Scholar] [CrossRef]
- Hung, Y.N.; Kadziola, Z.; Brnabic, A.J.; Yeh, J.F.; Fuh, J.L.; Hwang, J.P.; Montgomery, W. The epidemiology and burden of Alzheimer’s disease in Taiwan utilizing data from the National Health Insurance Research Database. Clin. Outcomes Res. 2016, 8, 387–395. [Google Scholar] [CrossRef]
- Walker, A.J.; Pratt, C.C.; Eddy, L. Informal Caregiving to Aging Family Members: A Critical Review. Fam. Relations 1995, 44, 402–411. [Google Scholar] [CrossRef]
- Guay, C.; Auger, C.; Demers, L.; Mortenson, W.B.; Miller, W.C.; Gélinas-Bronsard, D.; Ahmed, S. Components and Outcomes of Internet-Based Interventions for Caregivers of Older Adults: Systematic Review. J. Med. Internet Res. 2017, 19, e313. [Google Scholar] [CrossRef] [PubMed]
- Adelman, R.D.; Tmanova, L.L.; Delgado, D.; Dion, S.; Lachs, M.S. Caregiver Burden: A Clinical Review. JAMA 2014, 311, 1052–1060. [Google Scholar] [CrossRef]
- Zarit, S.H.; Todd, P.A.; Zarit, J.M. Subjective Burden of Husbands and Wives as Caregivers: A Longitudinal Study1. Gerontologist 1986, 26, 260–266. [Google Scholar] [CrossRef]
- Roberts, C.A.; Geryk, L.L.; Sage, A.J.; Sleath, B.L.; Tate, D.F.; Carpenter, D.M. Adolescent, caregiver, and friend preferences for integrating social support and communication features into an asthma self-management app. J. Asthma 2016, 53, 948–954. [Google Scholar] [CrossRef]
- Chiarini, G.; Ray, P.; Akter, S.; Masella, C.; Ganz, A. mHealth Technologies for Chronic Diseases and Elders: A Systematic Review. IEEE J. Sel. Areas Commun. 2013, 31, 6–18. [Google Scholar] [CrossRef]
- Donevant, S.B.; Estrada, R.D.; Culley, J.M.; Habing, B.; Adams, S.A. Exploring app features with outcomes in mHealth studies involving chronic respiratory diseases, diabetes, and hypertension: A targeted exploration of the literature. J. Am. Med Infor. Assoc. 2018, 25, 1407–1418. [Google Scholar] [CrossRef] [PubMed]
- Coorey, G.M.; Neubeck, L.; Mulley, J.; Redfern, J. Effectiveness, acceptability and usefulness of mobile applications for cardiovascular disease self-management: Systematic review with meta-synthesis of quantitative and qualitative data. Eur. J. Prev. Cardiol. 2020, 25, 505–521. [Google Scholar] [CrossRef]
- Lee, J.A.; Choi, M.; Lee, S.A.; Jiang, N. Effective behavioral intervention strategies using mobile health applications for chronic disease management: A systematic review. BMC Med. Inform. Decis. Mak. 2018, 18, 12. [Google Scholar] [CrossRef] [PubMed]
- Grossman, M.R.; Zak, D.K.; Zelinski, E.M. Mobile Apps for Caregivers of Older Adults: Quantitative Content Analysis. JMIR Mhealth Uhealth 2018, 6, e162. [Google Scholar] [CrossRef] [PubMed]
- Miller, G. The Smartphone Psychology Manifesto. Perspect. Psychol. Sci. 2012, 7, 221–237. [Google Scholar] [CrossRef]
- European Comission. Green Paper on Mobile Health (“mHealth”). Available online: https://digital-strategy.ec.europa.eu/en/library/green-paper-mobile-health-mhealth (accessed on 25 April 2023).
- Stanford/VA Alzheimer’s Center. Geriatric Depression and Dementia Scale. Available online: https://med.stanford.edu/svalz/apps.html (accessed on 25 April 2023).
- Lumos Labs, Inc. Lumosity. Available online: https://www.lumosity.com/en/ (accessed on 25 April 2023).
- Dakim, Inc. Dakim Brain Fitness. Available online: https://www.dakim.com (accessed on 25 April 2023).
- Elevate Labs. Elevate—Brain Training and Brain Games. Available online: https://elevateapp.com (accessed on 25 April 2023).
- AngelSense. GPS Tracker for Elderlys. Available online: https://www.angelsense.com/gps-tracker-for-elderly/ (accessed on 25 April 2023).
- Metalert. GPS SmartSole. Available online: https://www.gpssmartsole.com (accessed on 25 April 2023).
- Chaudhry, B.M. Health is fine if pills are on time. Mhealth 2016, 2, 40. [Google Scholar] [CrossRef]
- Cunha, C.A.S.; Duarte, R.P. Multi-Device Nutrition Control. Sensors 2022, 22, 2617. [Google Scholar] [CrossRef]
- Honor Care Network. Help for Alzheimers Families. Available online: https://www.helpforalzheimersfamilies.com (accessed on 25 April 2023).
- K. Burns et al. Care4Dementia App. Available online: https://dementiaresearch.org.au/resources/zz-app-care4dementia/ (accessed on 25 April 2023).
- AppInst Ltd. Dementia Emergency. Available online: https://apps.apple.com/us/app/dementia-emergency/id1072396675 (accessed on 25 April 2023).
- American Red Cross. Emergency App. Available online: https://www.redcross.org/get-help/how-to-prepare-for-emergencies/mobile-apps.html (accessed on 25 April 2023).
- Sanvello Health 2022 ©. Home—Sanvello. Available online: https://www.sanvello.com (accessed on 25 April 2023).
- Evans, D. MyFitnessPal. Br. J. Sport. Med. 2017, 51, 1101–1102. [Google Scholar] [CrossRef]
- Levinson, C.A.; Fewell, L.; Brosof, L.C. My Fitness Pal calorie tracker usage in the eating disorders. Eat. Behav. 2017, 27, 14–16. [Google Scholar] [CrossRef]
- FatSecret. FatsecretPlatform API. Available online: https://platform.fatsecret.com/api/ (accessed on 25 April 2023).
- Tredrea, M.S.; Dalbo, V.J.; Scanlan, A.T. Lifesum: Easy and effective dietary and activity monitoring. Br. J. Sport. Med. 2017, 51, 1042. [Google Scholar] [CrossRef]
- Livestrong. MyPlate Calorie Counter. Available online: https://www.livestrong.com/myplate/ (accessed on 25 April 2023).
- Corcoran, K. Fooducate. Available online: https://www.fooducate.com/ (accessed on 25 April 2023).
- Willett, W.C. The Mediterranean diet: Science and practice. Public Health Nutr. 2006, 9, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Dohan, M.; Tan, J. Lose It! Int. J. Healthc. Inf. Syst. Inform. (IJHISI) 2011, 6, 60–65. [Google Scholar] [CrossRef]
- Fitnow, Inc. Lose It! Available online: https://www.loseit.com/ (accessed on 25 April 2023).
- US Department of Agriculture. Start Simple with My Plate. Available online: https://www.myplate.gov/resources/tools/startsimple-myplate-app (accessed on 25 April 2023).
- MedHelp. My Diet Diary. Available online: https://www.medhelp.org/land/calorie-counter-app (accessed on 25 April 2023).
- GetFit Apps. GetFit Calorie Counter. Available online: https://getfitapps.com/ (accessed on 25 April 2023).
- Hendawi, R.; Li, J.; Alian, S. ADDietCoach: A Personalized Virtual Diet Coach for Alzheimer’s Disease. Int. J.-Health Med. Commun. (IJEHMC) 2021, 12, 1–18. [Google Scholar] [CrossRef]
- Nielsen, J. Usability Engineering; Morgan Kaufmann: Burlington, MA, USA, 1994. [Google Scholar]
- ISO I. 9241-210; 2019 Ergonomics of Human-System Interaction. Part 210: Human-Centred Design for Interactive Systems. ISO: Geneva, Switzerland, 2019. Available online: https://www.iso.org/standard/77520.html (accessed on 2 March 2023).
- Virzi, R.A. Refining the Test Phase of Usability Evaluation: How Many Subjects Is Enough? Hum. Factors 1992, 34, 457–468. [Google Scholar] [CrossRef]
- Rieman, J.; Franzke, M.; Redmiles, D. Usability Evaluation with the Cognitive Walkthrough. In Proceedings of the Conference Companion on Human Factors in Computing Systems (CHI ’95), Denver, CO, USA, 7–11 May 1995; Association for Computing Machinery: New York, NY, USA, 1995; pp. 387–388. [Google Scholar] [CrossRef]
- Mahatody, T.; Sagar, M.; Kolski, C. State of the Art on the Cognitive Walkthrough Method, Its Variants and Evolutions. Int. J. Hum.–Comput. Interact. 2010, 26, 741–785. [Google Scholar] [CrossRef]
- Schrepp, M.; Thomaschewski, J.; Hinderks, A. Construction of a benchmark for the user experience questionnaire (UEQ). Int. J. Interact. Multimed. Artif. Intell. 2017, 4, 40–44. [Google Scholar] [CrossRef]
- Boivie, I.; Åborg, C.; Persson, J.; Löfberg, M. Why usability gets lost or usability in in-house software development. Interact. Comput. 2003, 15, 623–639. [Google Scholar] [CrossRef]
- Neale, D.C.; Carroll, J.M. Chapter 20—The Role of Metaphors in User Interface Design. In Handbook of Human-Computer Interaction, 2nd ed.; Helander, M.G., Landauer, T.K., Prabhu, P.V., Eds.; North-Holland: Amsterdam, The Netherlands, 1997; pp. 441–462. [Google Scholar] [CrossRef]
- Reese, G. Cloud Application Architectures: Building Applications and Infrastructure in the Cloud; O’Reilly Media, Inc.: Sebastopol, CA, USA, 2009. [Google Scholar]
- Lit. LitElement. Available online: https://lit.dev (accessed on 25 April 2023).
- MongoDB. Available online: https://www.mongodb.com/ (accessed on 25 April 2023).
- Dan Abramov and the Redux Documentation Authors. Redux—A Predictable State Container for JS Apps. Available online: https://redux.js.org/ (accessed on 25 April 2023).
- Johnson, J.; Henderson, A. Conceptual Models: Begin by Designing What to Design. Interactions 2002, 9, 25–32. [Google Scholar] [CrossRef]
- Camelon, K.M.; Hadell, K.; Jamsen, P.T.; Ketonen, K.J.; Kohtamaki, H.M.; Makimatilla, S.; Tormala, M.L.; Valve, R.H. The Plate Model: A Visual Method of Teaching Meal Planning. J. Am. Diet. Assoc. 1998, 98, 1155–1158. [Google Scholar] [CrossRef] [PubMed]
- Bostock, M.; Ogievetsky, V.; Heer, J. D3 Data-Driven Documents. IEEE Trans. Vis. Comput. Graph. 2011, 17, 2301–2309. [Google Scholar] [CrossRef]
- Bostock, M. Zoomable Circle Packing. Available online: https://observablehq.com/@d3/zoomable-circle-packing (accessed on 25 April 2023).
- Rashid, A.M.; Albert, I.; Cosley, D.; Lam, S.K.; McNee, S.M.; Konstan, J.A.; Riedl, J. Getting to Know You: Learning New User Preferences in Recommender Systems. In Proceedings of the Proceedings of the 7th International Conference on Intelligent User Interfaces (IUI ’02), San Francisco, CA, USA, 13–16 January 2002; Association for Computing Machinery: New York, NY, USA, 2002; pp. 127–134. [Google Scholar] [CrossRef]
- Fürnkranz, J.; Hüllermeier, E. Preference Learning and Ranking by Pairwise Comparison. In Preference Learning; Fürnkranz, J., Hüllermeier, E., Eds.; Springer: Berlin/Heidelberg, Germany, 2011; pp. 65–82. [Google Scholar] [CrossRef]
- Noah, S.A.; Abdullah, S.N.; Shahar, S.; Abdul-Hamid, H.; Khairudin, N.; Yusoff, M.; Ghazali, R.; Mohd-Yusoff, N.; Shafii, N.S.; Abdul-Manaf, Z. DietPal: A Web-Based Dietary Menu-Generating and Management System. J. Med. Internet Res. 2004, 6, e4. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Pérez, J.M.; Miranda, G.; Segredo, E.; León, C.; Rodríguez-León, C. Application of Multi-Objective Evolutionary Algorithms for Planning Healthy and Balanced School Lunches. Mathematics 2021, 9, 80. [Google Scholar] [CrossRef]













| MyFitnessPal [30,31] | MyPlate Calorie Counter [34] | Fooducate [35] | FatSecret [32] | Start Simple with My Plate [39] | My Diet Diary [40] | GetFit [41] | Lose It! [37,38] | ADDietCoach [42] | Lifesum [33] | |
|---|---|---|---|---|---|---|---|---|---|---|
| Meal plan tracking | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Intended for the older age group | ✓ | |||||||||
| Designed for people with health concerns | ✓ | ✓ | ✓ | |||||||
| Records water consumption | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Records food/nutrients ingested | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Control amounts of food/nutrients | ✓ | ✓ | ✓ | ✓ | ||||||
| Meal listing | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Provides statistics | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Meal consultation | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Allows food exchange for equivalents | ||||||||||
| Allows to add food | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Interface design quality | ↗ | ↗ | ↑ | ↑ | ↘ | ↓ | ↗ | ↑ | ↓ | ↑ |
| Real time nutritionist feedback |
| No. | Task | Process |
|---|---|---|
| 1 | Register the consumption of 130 mL of water outside the food plan | Grab a cup of water, fill it with the amount |
| 2 | For lunch, check which food will be consumed, of the prescribed food plan from the nutritionist | Identify a meal in a list and see the food that it contains |
| 3 | Exchange the food corn in the lunch for another equivalent | In the preparation of food, an ingredient is missing. It needs to be exchanged |
| 4 | Remove broccoli from the meal | Lunch contains broccoli, which are not of the interest of the patient. They are to be removed |
| 5 | Add lettuce to a meal | The patient loves lettuce. It must be added to the dish. |
| 6 | Register the consumption of the lunch | Check the dish to identify the amount of food consumed |
| 7 | Reduce the amount of food in a dish to 50% | A prescribed food was not completely ingested |
| 8 | Add an ice cream as an extra meal | The patient really wants an ice cream. Give it to him |
| 9 | The food plan for the day is complete. See if all the macronutrients were ingested | Ingestion of all (or parts) of food from the meals |
| 10 | Check the lunch in two days | In the prescribed food plan, see the food that composes the lunch |
| No. | Task | Average Time (Seconds) |
|---|---|---|
| 1 | Register the consumption of 130 mL of water outside the food plan | 2.3 |
| 2 | For lunch, check which food will be consumed, of the prescribed food plan from the nutritionist | 3.5 |
| 3 | Exchange the food corn in the lunch for another equivalent | 3.6 |
| 4 | Remove broccoli from the meal | 3.6 |
| 5 | Add lettuce to a meal | 8.6 |
| 6 | Register the consumption of the lunch | 1.2 |
| 7 | Reduce the amount of food in a dish to 50% | 4.8 |
| 8 | Add an ice cream as an extra meal | 8.6 |
| 9 | The food plan for the day is complete. See if all the macronutrients were ingested | 1.2 |
| 10 | Check the lunch in two days | 2.3 |
| Confidence Intervals (p = 0.05) per Scale | ||||||
|---|---|---|---|---|---|---|
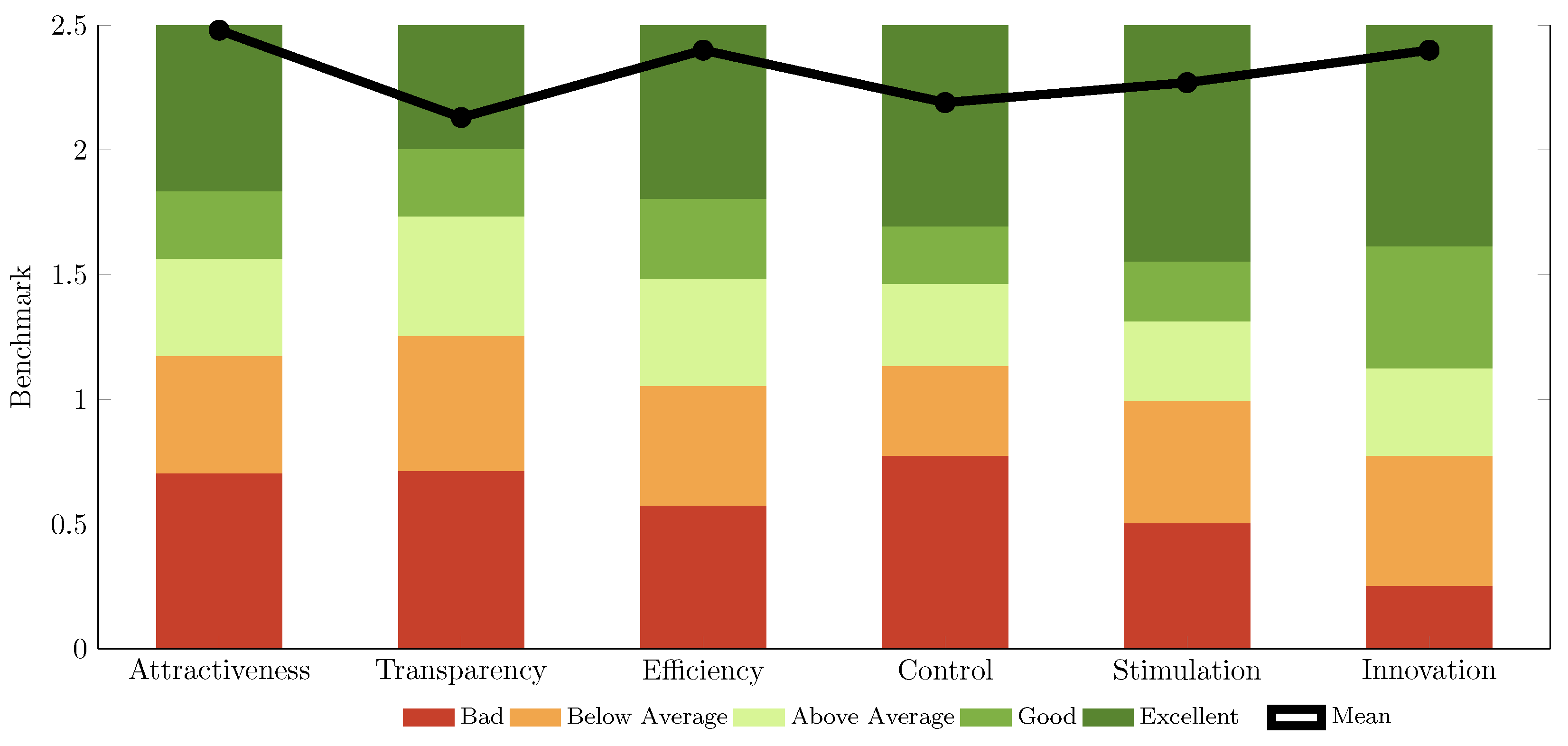
| Scale | Mean | Std. Dev. | Confidence | Confidence Interval | Rating | |
| Attractiveness | 2.48 | 0.20 | 0.10 | 2.38 | 2.58 | Excellent |
| Perspicuity | 2.13 | 0.42 | 0.20 | 1.92 | 2.33 | Excellent |
| Efficiency | 2.59 | 0.26 | 0.13 | 2.47 | 2.72 | Excellent |
| Dependability | 2.19 | 0.25 | 0.12 | 2.07 | 2.31 | Excellent |
| Stimulation | 2.27 | 0.45 | 0.22 | 2.04 | 2.49 | Excellent |
| Novelty | 2.48 | 0.40 | 0.20 | 2.29 | 2.68 | Excellent |
| Pragmatic and Hedonic Quality | |
|---|---|
| Attractiveness | 2.48 |
| Pragmatic Quality | 2.30 |
| Hedonic Quality | 2.38 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duarte, R.P.; Cunha, C.A.S.; Alves, V.N.N. Mobile Application for Real-Time Food Plan Management for Alzheimer Patients through Design-Based Research. Future Internet 2023, 15, 168. https://doi.org/10.3390/fi15050168
Duarte RP, Cunha CAS, Alves VNN. Mobile Application for Real-Time Food Plan Management for Alzheimer Patients through Design-Based Research. Future Internet. 2023; 15(5):168. https://doi.org/10.3390/fi15050168
Chicago/Turabian StyleDuarte, Rui P., Carlos A. S. Cunha, and Valter N. N. Alves. 2023. "Mobile Application for Real-Time Food Plan Management for Alzheimer Patients through Design-Based Research" Future Internet 15, no. 5: 168. https://doi.org/10.3390/fi15050168
APA StyleDuarte, R. P., Cunha, C. A. S., & Alves, V. N. N. (2023). Mobile Application for Real-Time Food Plan Management for Alzheimer Patients through Design-Based Research. Future Internet, 15(5), 168. https://doi.org/10.3390/fi15050168