
Incorporation of Mometasone Furoate into a Cyclodextrin Metal-Organic Framework to Optimize Nasal Administration

 ,
, 
Abstract

1. Introduction
2. Materials and Methods
2.1. Materials
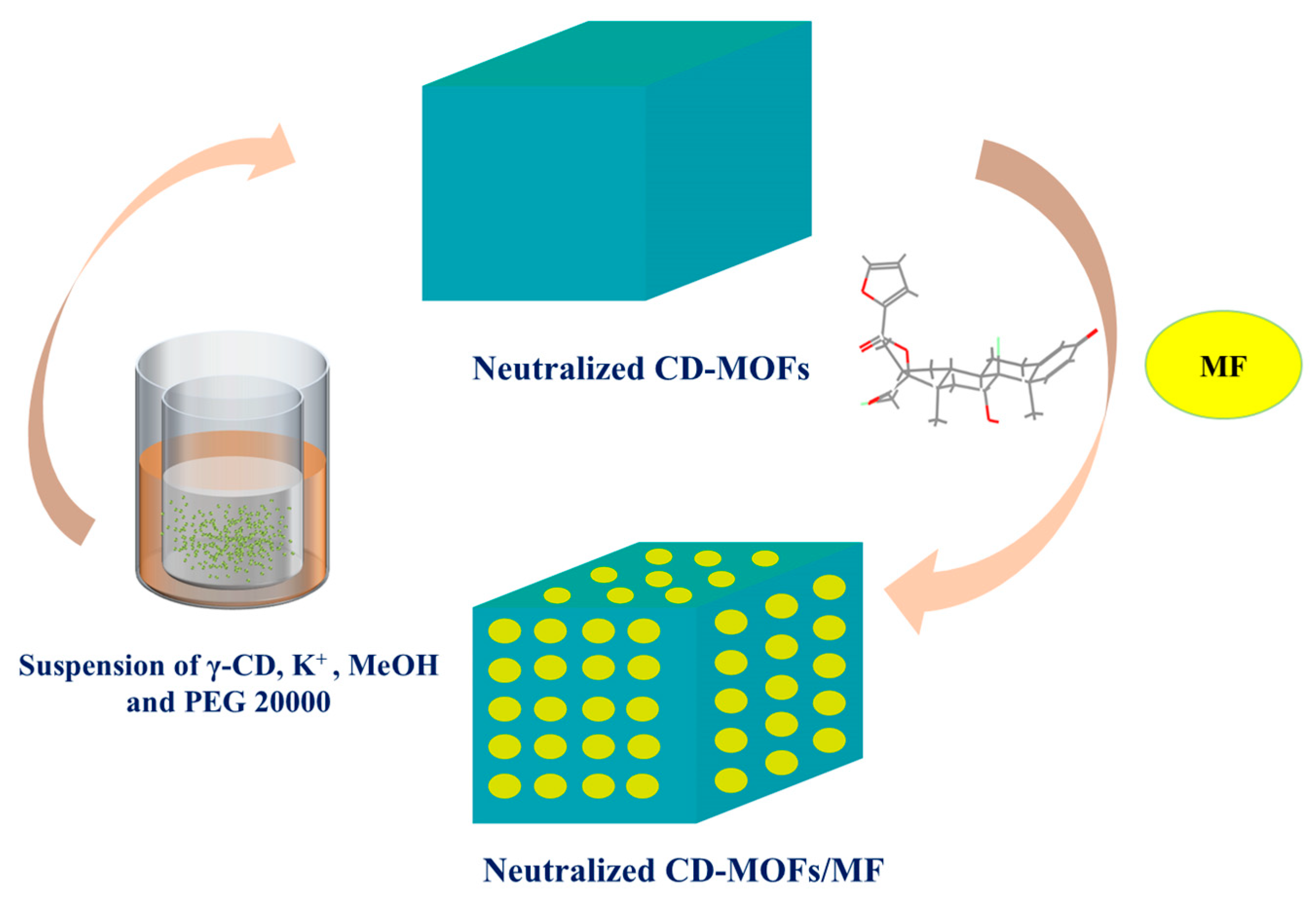
2.2. Synthesis of CD-MOFs
2.3. Characterization of CD-MOFs
2.4. Drug Loading of MF into CD-MOFs
2.5. Morphology and Other Characterizations of MF@MOF
2.6. Solubility Studies In Vitro
2.7. In Vitro Release Study of MF@MOF
2.8. Application of 3D Biomimetic Human Nasal Cavity Models
3. Results
3.1. Morphology and Characterization of CD-MOFs
3.2. Optimization of Drug Loading Conditions
3.3. Characterization of MF@MOF
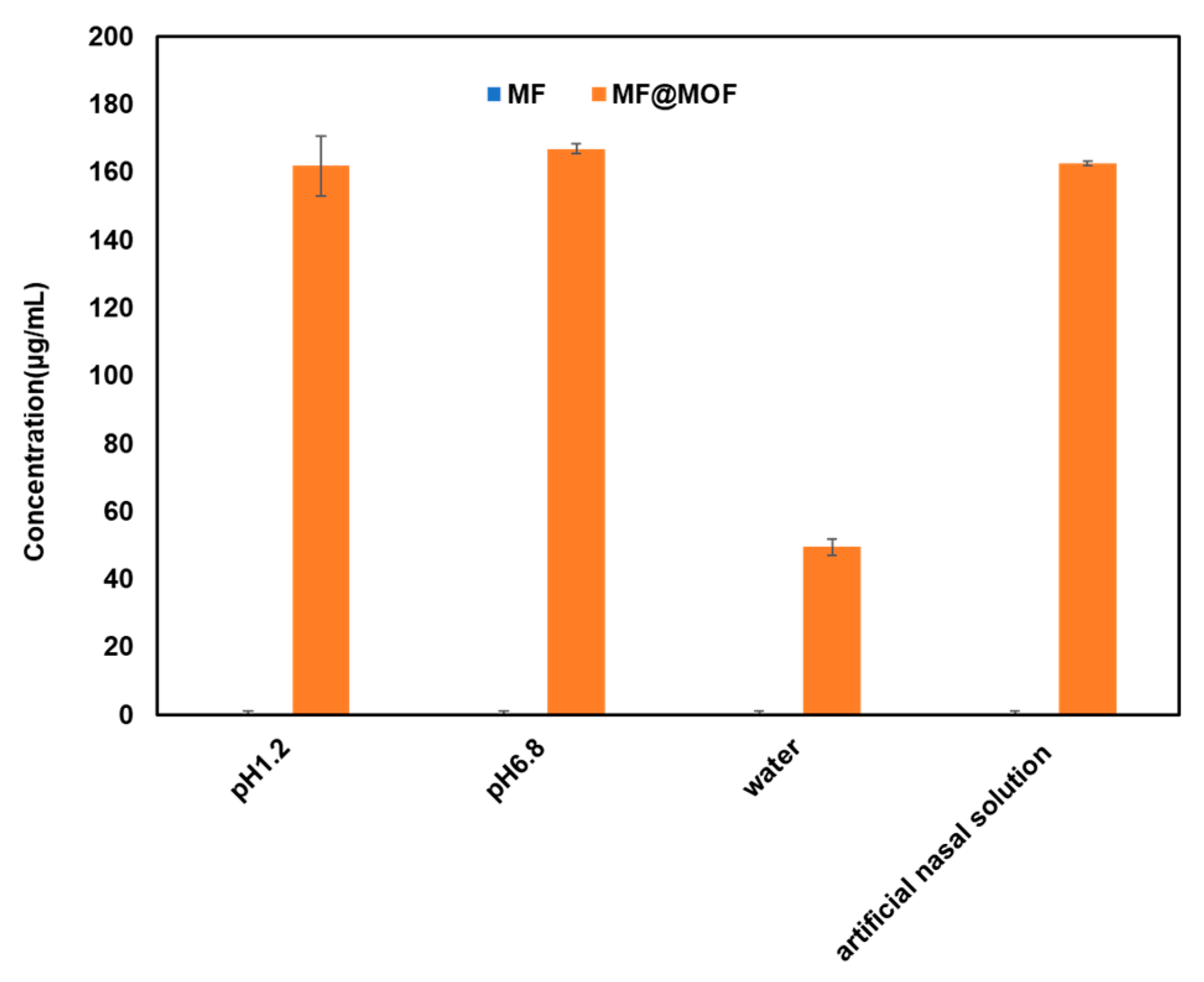
3.4. Enhanced Solubility of MF@MOF
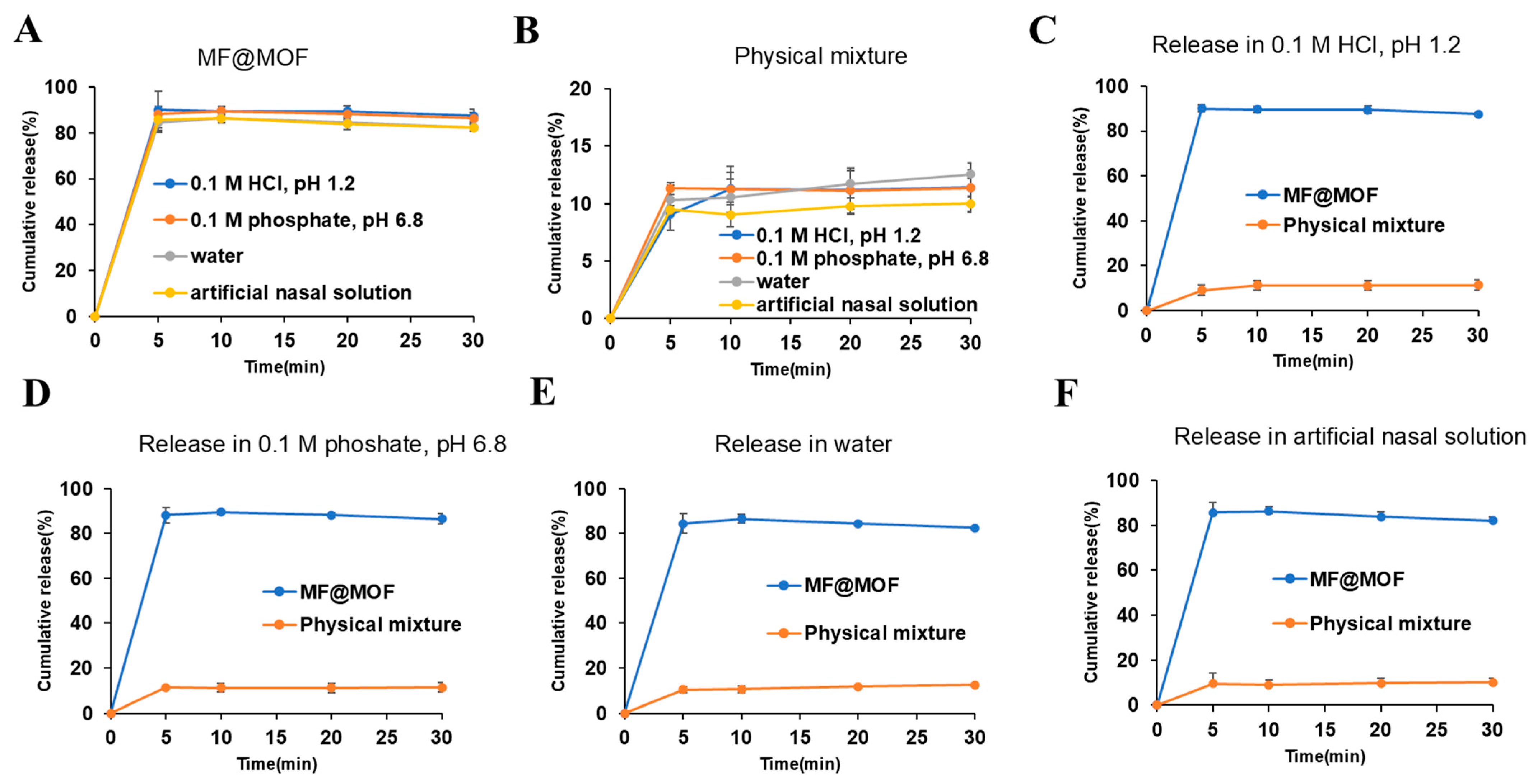
3.5. In Vitro Evaluation of Drug Release
3.6. Deposition of MF Powder in a 3D Biomimetic Human Nasal Cavity Model
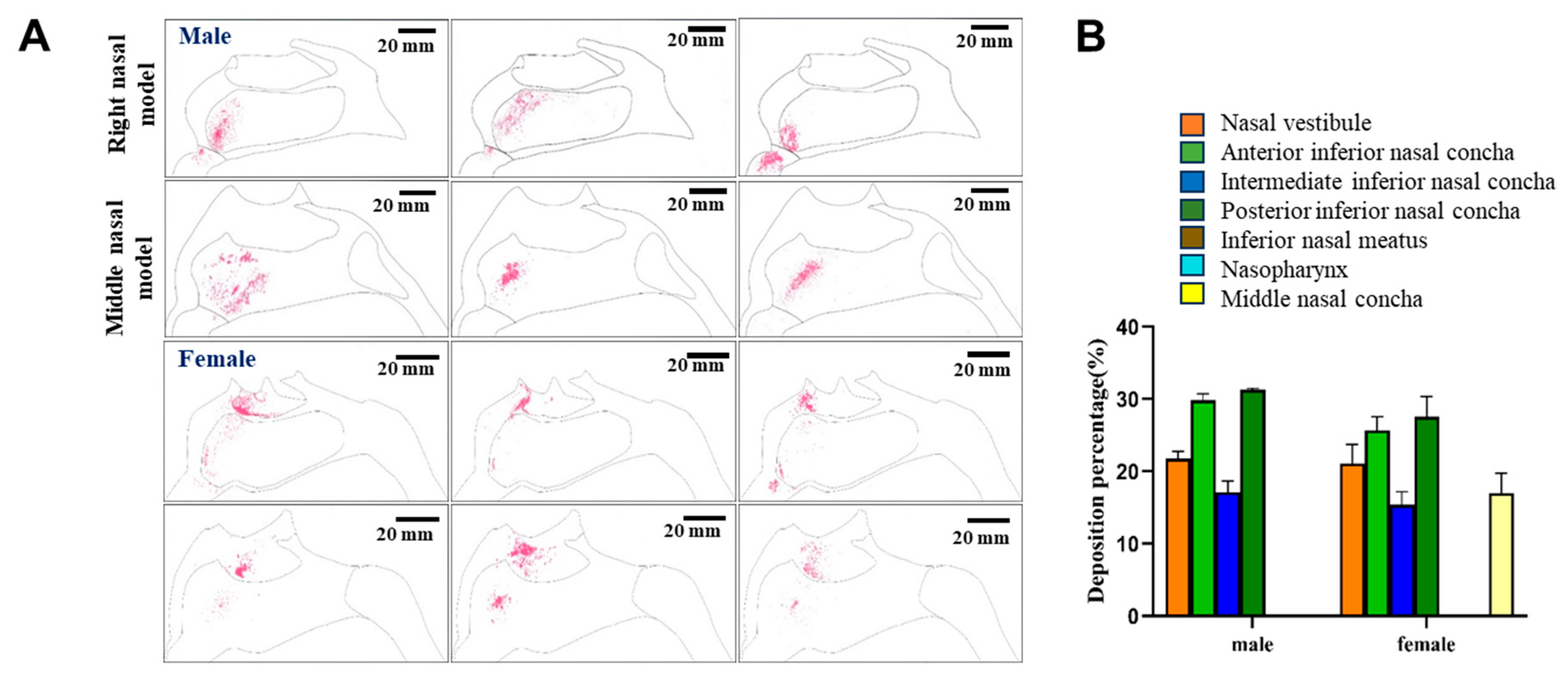
3.6.1. Delivery of MF@MOF with a Nozzle Angle of 45°
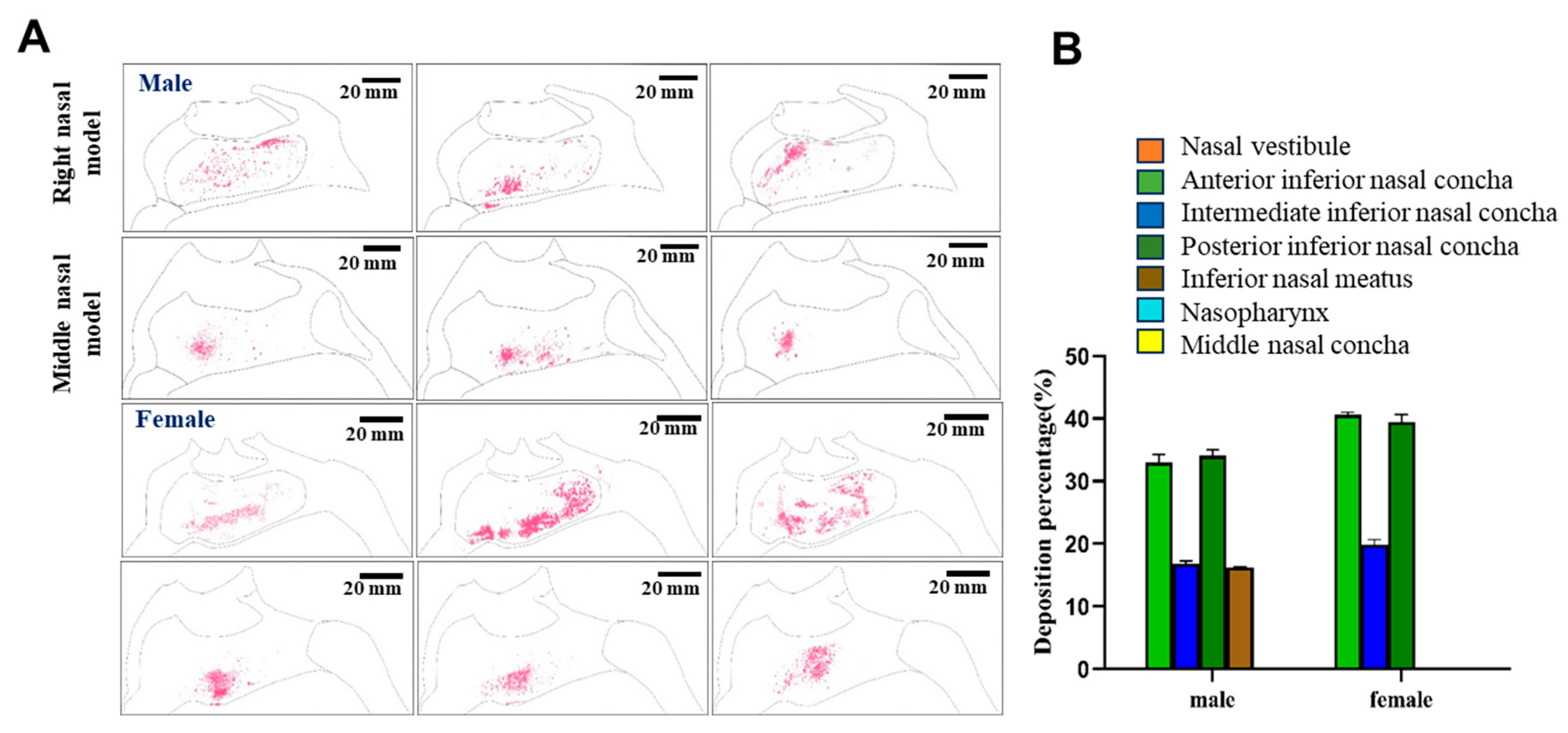
3.6.2. Delivery of MF@MOF with a Nozzle Angle of 30°
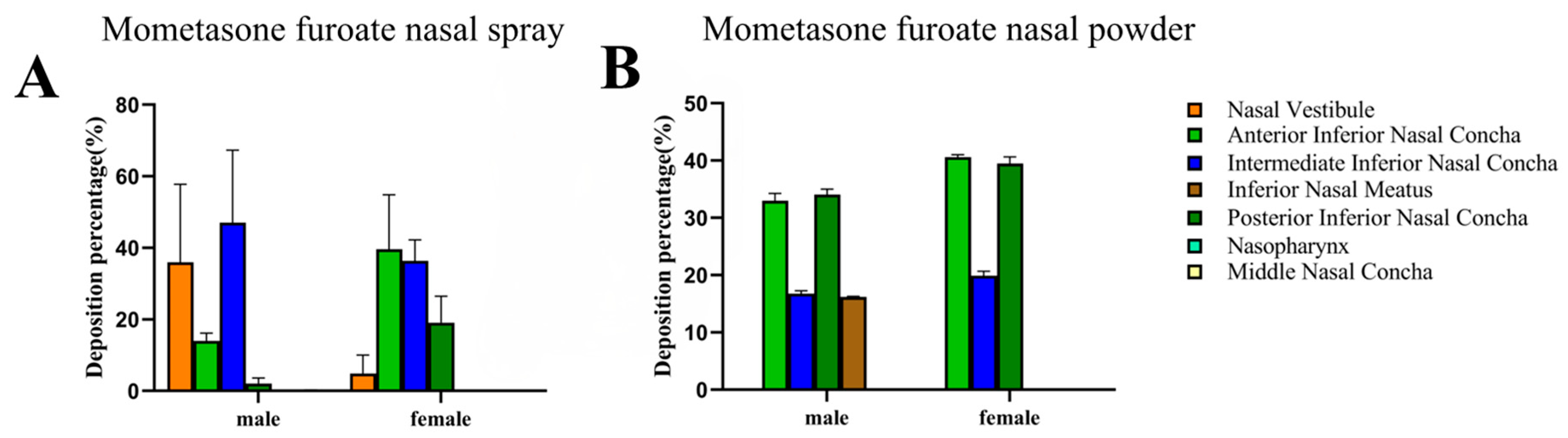
3.6.3. Comparison of Delivery of MF@MOF to That of a Commercial MF Nasal Spray
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| MF | Mometasone furoate |
| CD-MOF | Cyclodextrin metal-organic framework |
| CRS | Chronic rhinosinusitis |
| γ-CD | γ-Cyclodextrin |
| 3DP | Three-dimensional printing |
| SEM | Scanning electron microscopy |
| SR-FTIR | Synchrotron radiation Fourier transform infrared spectroscopy |
| PXRD | Powder X-ray diffraction |
| TGA | Thermogravimetric analysis |
References
- Fokkens, W.J.; Lund, V.J.; Hopkins, C. European Position Paper on Rhinosinusitis and Nasal Polyps. Rhinology 2020, 58, 1–464. [Google Scholar] [CrossRef] [PubMed]
- Wahid, N.W.; Smith, R.; Clark, A. The socioeconomic cost of chronic rhinosinusitis study. Rhinology 2020, 58, 112–125. [Google Scholar] [CrossRef]
- Halawi, A.M.; Smith, S.S.; Chandra, P.K. Chronic rhinosinusitis: Epidemiology and cost. Allergy Asthma Proc. 2013, 34, 328–334. [Google Scholar] [CrossRef]
- Zlotnik, A.; Yoshie, O. Chemokines: A new classification system and their role in immunity. Immunity 2000, 12, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Hildenbrand, T.; Milger-Kneidinger, K.; Baumann, I.; Weber, R. The Diagnosis and Treatment of Chronic Rhinosinusitis. Dtsch. Arztebl. Int. 2024, 121, 643–653. [Google Scholar] [CrossRef]
- Schweickart, V.L.; Epp, A.; Raport, C.J. CCR11 is a functional receptor for the monocyte chemoattractant protein family of chemokines. J. Biol. Chem. 2000, 275, 9550–9556. [Google Scholar] [CrossRef] [PubMed]
- Hughes, C.E.; Nibbs, R.J.B. A guide to chemokines and their receptors. FEBS J. 2018, 285, 2944–2971. [Google Scholar] [CrossRef]
- Lui, J.T.; Rudmik, L. Case Definitions for Chronic Rhinosinusitis in Administrative Data: A Systematic Review. Am. J. Rhinol. Allergy 2015, 29, 146–151. [Google Scholar] [CrossRef]
- Editorial Board. Definition, classification and treatment of chronic rhinosinusitis. Chin. J. Otorhinolaryngol. Head Neck Surg. 2005, 10, 18–31. [Google Scholar]
- Ragab, S.M.; Lund, V.J.; Scadding, G. Evaluation of the medical and surgical treatment of chronic rhinosinusitis: A prospective, randomised, controlled trial. Laryngoscope 2004, 114, 923–930. [Google Scholar] [CrossRef]
- Yang, Q.M. Rational use of glucocorticoids. J. Pract. Med. Tech. 2007, 22, 2995–2997. [Google Scholar]
- He, Y.Z.; Yi, W.; Suino-Powell, K. Structures and mechanism for the design of highly potent glucocorticoids. Cell Res. 2014, 24, 713–726. [Google Scholar] [CrossRef] [PubMed]
- Benet, L.Z.; Broccatelli, F.; Oprea, T.I. BDDCS applied to over 900 drugs. AAPS J. 2011, 13, 519–547. [Google Scholar] [CrossRef]
- Li, H.; Lv, N.; Li, X. Composite CD-MOF nanocrystals-containing microspheres for sustained drug delivery. Nanoscale 2017, 9, 7454–7463. [Google Scholar] [CrossRef]
- Chen, X.; Guo, T.; Zhang, K. Simultaneous improvement to solubility and bioavailability of active natural compound isosteviol using cyclodextrin metal-organic frameworks. Acta Pharm. Sin. B 2021, 11, 2914–2923. [Google Scholar] [CrossRef]
- Fairen-Jimenez, D.; Colón, Y.J.; Farha, O.K. Understanding excess uptake maxima for hydrogen adsorption isotherms in frameworks with rht topology. Chem. Commun. 2012, 48, 10496–10498. [Google Scholar] [CrossRef]
- Lee, J.; Farha, O.K.; Roberts, J. Metal-organic framework materials as catalysts. Chem. Soc. Rev. 2009, 38, 1450–1459. [Google Scholar] [CrossRef]
- Meek, S.T.; Greathouse, J.A.; Allendorf, M.D. Metal-Organic Frameworks: A Rapidly Growing Class of Versatile Nanoporous Materials. Adv. Mater. 2011, 23, 249–267. [Google Scholar] [CrossRef] [PubMed]
- Silberstein, S.; Winner, P.K.; McAllister, P.J. Early Onset of Efficacy and Consistency of Response Across Multiple Migraine Attacks From the Randomized COMPASS Study: AVP-825 Breath Powered Exhalation Delivery System (Sumatriptan Nasal Powder) vs. Oral Sumatriptan. Headache 2017, 57, 862–876. [Google Scholar] [CrossRef]
- Pires, A.; Fortuna, A.; Alves, G. Intranasal drug delivery: How, why and what for? J. Pharm. Pharm. Sci. 2009, 12, 288–311. [Google Scholar] [CrossRef]
- Cunha, S.; Amaral, M.H.; Lobo, J.M.S. Lipid Nanoparticles for Nasal/Intranasal Drug Delivery. Crit. Rev. Ther. Drug Carr. Syst. 2017, 34, 257–282. [Google Scholar] [CrossRef]
- Thomann-Harwood, L.J.; Kaeuper, P.; Rossi, N. Nanogel vaccines targeting dendritic cells: Contributions of the surface decoration and vaccine cargo on cell targeting and activation. J. Control. Release 2013, 166, 95–105. [Google Scholar] [CrossRef]
- Bahamondez-Canas, T.F.; Cui, Z.R. Intranasal immunization with dry powder vaccines. Eur. J. Pharm. Biopharm. 2018, 122, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Varshosaz, J.; Sadrai, H.; Heidari, A. Nasal delivery of insulin using bioadhesive chitosan gels. Drug Deliv. 2006, 13, 31–38. [Google Scholar] [CrossRef]
- Costantino, H.R.; Illum, L.; Brandt, G. Intranasal delivery: Physicochemical and therapeutic aspects. Int. J. Pharm. 2007, 337, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Costa, C.; Moreira, J.N.; Amaral, M.H. Nose-to-brain delivery of lipid-based nanosystems for epileptic seizures and anxiety crisis. J. Control. Release 2019, 295, 187–200. [Google Scholar] [CrossRef] [PubMed]
- Costa, C.P.; Moreira, J.N.; Sousa Lobo, J.M. Intranasal delivery of nanostructured lipid carriers, solid lipid nanoparticles and nanoemulsions: A current overview of in vivo studies. Acta Pharm. Sin. B 2021, 11, 925–940. [Google Scholar] [CrossRef]
- Shrewsbury, S.B. The Upper Nasal Space: Option for Systemic Drug Delivery, Mucosal Vaccines and “Nose-to-Brain”. Pharmaceutics 2023, 15, 1720. [Google Scholar] [CrossRef]
- Lv, Y.; Zhang, D.; Zhang, C. Research progress in nasal drug delivery. Tianjin J. Tradit. Chin. Med. 2014, 31, 766–768. [Google Scholar]
- Bao, T.T.; Zhang, Q.; Wu, W.Z. Advances in nasal powder aerosol research. World Clin. Drugs 2019, 40, 287–292. [Google Scholar]
- Stansbury, J.W.; Idacavage, M.J. 3D printing with polymers: Challenges among expanding options and opportunities. Dent. Mater. 2016, 32, 54–64. [Google Scholar] [CrossRef]
- Boetker, J.; Water, J.J.; Aho, J. Modifying release characteristics from 3D printed drug-eluting products. Eur. J. Pharm. Sci. 2016, 90, 47–52. [Google Scholar] [CrossRef]
- Trenfield, S.J.; Goyanes, A.; Telford, R. 3D printed drug products: Non-destructive dose verification using a rapid point-and-shoot approach. Int. J. Pharm. 2018, 549, 283–292. [Google Scholar] [CrossRef] [PubMed]
- Khaled, S.A.; Alexander, M.R.; Wildman, R.D. 3D extrusion printing of high drug loading immediate release paracetamol tablets. Int. J. Pharm. 2018, 538, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Wadher, K.; Trivedi, R.; Wankhede, N. 3D printing in pharmaceuticals: An emerging technology full of challenges. Ann. Pharm. Fr. 2021, 79, 107–118. [Google Scholar] [CrossRef]
- Shao, X.Y. Development of H102 Peptide Nasal Spray for Alzheimer’s Disease. Master’s Thesis, Fudan University, Shanghai, China, 2013. [Google Scholar]
- Muwaffak, Z.; Goyanes, A.; Clark, V. Patient-specific 3D scanned and 3D printed antimicrobial polycaprolactone wound dressings. Int. J. Pharm. 2017, 527, 161–170. [Google Scholar] [CrossRef]
- Smaldone, R.A.; Forgan, R.S.; Furukawa, H. Metal-organic frameworks from edible natural products. Angew. Chem. Int. Ed. 2010, 49, 8630–8634. [Google Scholar] [CrossRef] [PubMed]
- Su, J.; Liu, Y.; Sun, H. Visualization of nasal powder distribution using biomimetic human nasal cavity model. Acta Pharm. Sin. B 2024, 14, 392–404. [Google Scholar] [CrossRef]
- Zheng, Y.; Cui, L.; Lu, H. Nose to Brain: Exploring the Progress of Intranasal Delivery of Solid Lipid Nanoparticles and Nanostructured Lipid Carriers. Int. J. Nanomed. 2024, 19, 12343–12368. [Google Scholar] [CrossRef]
- Zeng, M.; Long, X.B.; Cui, Y.H.; Liu, Z. Comparison of efficacy of mometasone furoate versus clarithromycin in the treatment of chronic rhinosinusitis without nasal polyps in Chinese adults. Am. J. Rhinol. Allergy 2011, 25, 203–207. [Google Scholar] [CrossRef]
- Shelley, H.; Babu, R.J. Role of Cyclodextrins in Nanoparticle-Based Drug Delivery Systems. J. Pharm. Sci. 2018, 107, 1741–1753. [Google Scholar] [CrossRef] [PubMed]
- Şeker, B.; Açar, G.; Çiçekcibaşı, A.E.; Aydoğdu, D. Morphometric analysis of sphenopalatine foramen on computed tomography images with clinical significance. Surg. Radiol. Anat. 2022, 44, 1521–1529. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Solvent | MF/CD-MOF Ratio, % (w/w) | Loading Efficiency, % (w/w) |
|---|---|---|
| Acetone | 4.55 | 4.22 |
| 5.88 | 5.36 | |
| 8.70 | 8.23 | |
| 4.55 | 4.46 | |
| Ethyl acetate | 5.88 | 5.57 |
| 8.70 | 8.63 | |
| 4.55 | 4.25 | |
| Anhydrous ethanol | 5.88 | 5.63 |
| 8.70 | 8.21 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, J.; Guo, Y.; Liu, Y.; Gao, Q.; Wang, S.; Wu, L.; Wang, C.; Ren, X.; Zhang, J. Incorporation of Mometasone Furoate into a Cyclodextrin Metal-Organic Framework to Optimize Nasal Administration. Pharmaceutics 2025, 17, 788. https://doi.org/10.3390/pharmaceutics17060788
Li J, Guo Y, Liu Y, Gao Q, Wang S, Wu L, Wang C, Ren X, Zhang J. Incorporation of Mometasone Furoate into a Cyclodextrin Metal-Organic Framework to Optimize Nasal Administration. Pharmaceutics. 2025; 17(6):788. https://doi.org/10.3390/pharmaceutics17060788
Chicago/Turabian StyleLi, Jie, Yuhua Guo, Yan Liu, Qingfang Gao, Siwen Wang, Li Wu, Caifen Wang, Xiaohong Ren, and Jiwen Zhang. 2025. "Incorporation of Mometasone Furoate into a Cyclodextrin Metal-Organic Framework to Optimize Nasal Administration" Pharmaceutics 17, no. 6: 788. https://doi.org/10.3390/pharmaceutics17060788
APA StyleLi, J., Guo, Y., Liu, Y., Gao, Q., Wang, S., Wu, L., Wang, C., Ren, X., & Zhang, J. (2025). Incorporation of Mometasone Furoate into a Cyclodextrin Metal-Organic Framework to Optimize Nasal Administration. Pharmaceutics, 17(6), 788. https://doi.org/10.3390/pharmaceutics17060788