
Tapinarof Nanogels as a Promising Therapeutic Approach





Abstract

1. Introduction
2. Methodology
3. Structure and Barrier Function of the Epidermis
4. General Characteristics of Psoriasis
- Erythrodermic psoriasis: The most severe form, affecting more than 90% of the skin and associated with severe inflammation, scaling, oedema, and even life-threatening complications [23].
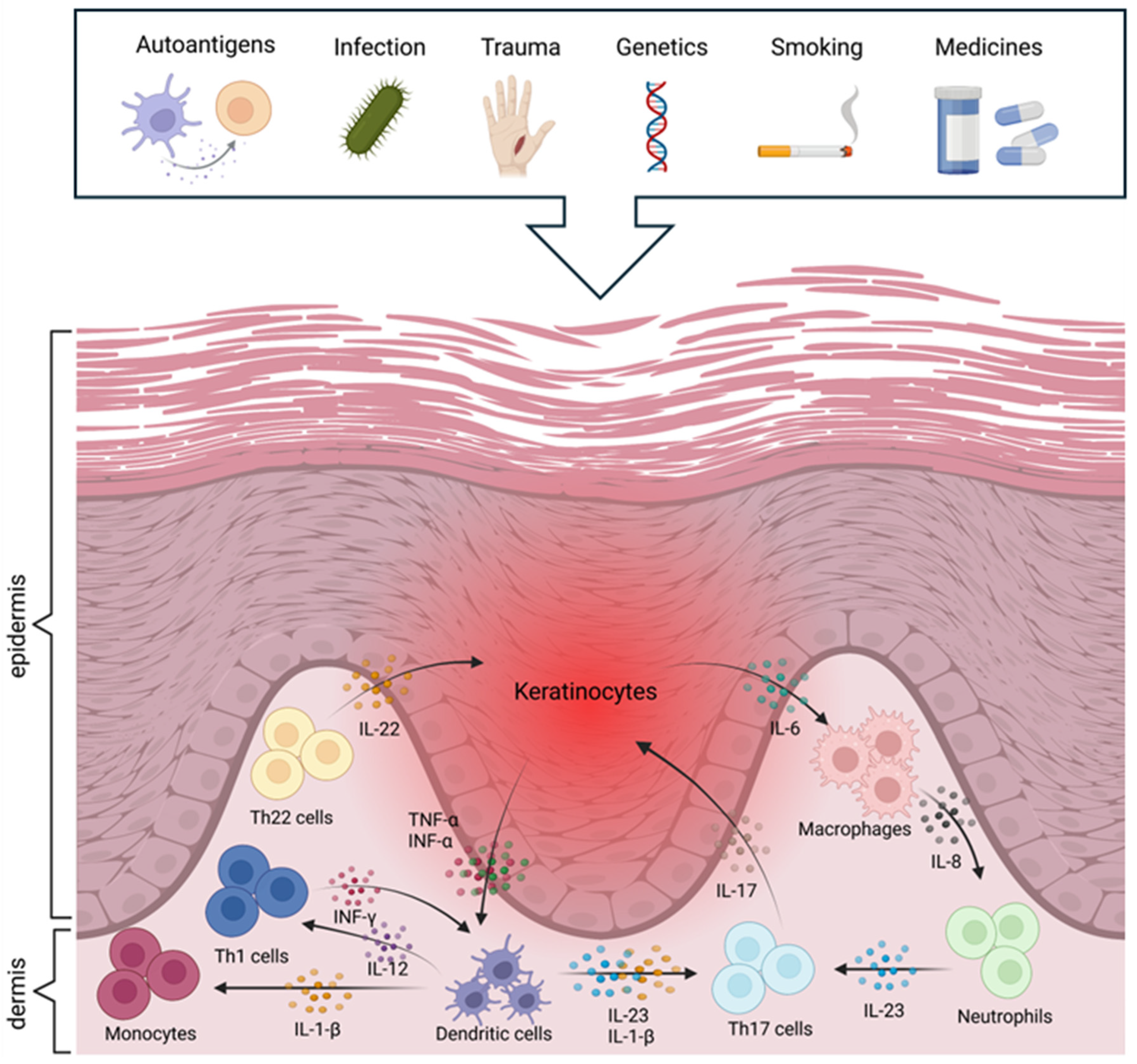
5. Immunological and Molecular Pathogenesis of Psoriasis
6. Psoriasis Therapies and Their Limitations

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Therapy | Mechanism | Adverse Effects | Examples | References |
|---|---|---|---|---|
| Corticosteroids | Inhibit the production of cytokines and reduce inflammatory mediators | Tachyphylaxis, atrophy, stretch marks, erythema | Clobetasol, betametazon, mometazon | [9,12,22,23,33] |
| Vitamin D analogues | Inhibit dendritic cell maturation, T-cell activation, and keratinocyte proliferation | Skin irritation, burning, erythema | Calcipotriene, calcitriol | [2,12,17,23,25] |
| Retinoids | Inhibit keratinocyte proliferation | Erythema, peeling, skin irritation, burning, itching | Tazarotene, tretinoin | |
| Calcineurin inhibitors | Reduce T-cell activation and the production of inflammatory cytokines (IL-2) by inhibiting the enzyme calcineurin | Skin irritation, burning, itching | Tacrolimus, pimecrolimus | [22,23,27,33,41] |
| Keratolytics | Reduce the intercellular cohesion of the stratum corneum by dissolving the intercellular cementum | Frontal headache, central nervous system symptoms, metabolic acidosis, tinnitus, nausea, vomiting | Salicylic acid | [23,42] |
| Therapy | Mechanism | Adverse Effects | Examples | References |
|---|---|---|---|---|
| Dihydrofolate reductase inhibitors | Block the proliferation of keratinocytes and immune cells by inhibiting dihydrofolate reductase | Dry skin, hair loss, liver toxicity, risk of skin cancer, nausea, infections, bone marrow suppression | Methotrexate | |
| Retinoids | Inhibit keratinocyte proliferation | Nausea, hepatotoxicity, infections, xerosis, nail and hair fragmentation, teratogenicity | Acitretin | [1,9,17,23] |
| Calcineurin inhibitors | Reduce T-cell activation and the production of inflammatory cytokines (IL-2) by inhibiting the enzyme calcineurin | Dry skin, cardiovascular and gastrointestinal problems, gingival hyperplasia, tremor, leukopenia, hepatotoxicity, nephrotoxicity, hypertension, increased immunosuppression | Cyclosporine | [1,2,6,17,41] |
| Biological therapies | Inhibit cytokines or cytokine receptors (IL-12/23 inhibitors, TNF inhibitors, IL-17 inhibitors) | Expensive, safety concerns, high risk of malignant tumours and facial paralysis | Etanercept, adalimumab, ustekinumab, infliximab | [1,2,9,23] |
| Phototherapy | Causes cell death by apoptosis, necrosis or autophagy; reduces epidermal proliferation | Melanoma, photoaging, burning, erythema, pruritus, xerosis, pain, and discomfort | Ultraviolet B light, psoralen ultraviolet A light, photodynamic therapy | [1,2,6,23,41] |
7. New Therapeutic Strategies for Psoriasis
8. Tapinarof
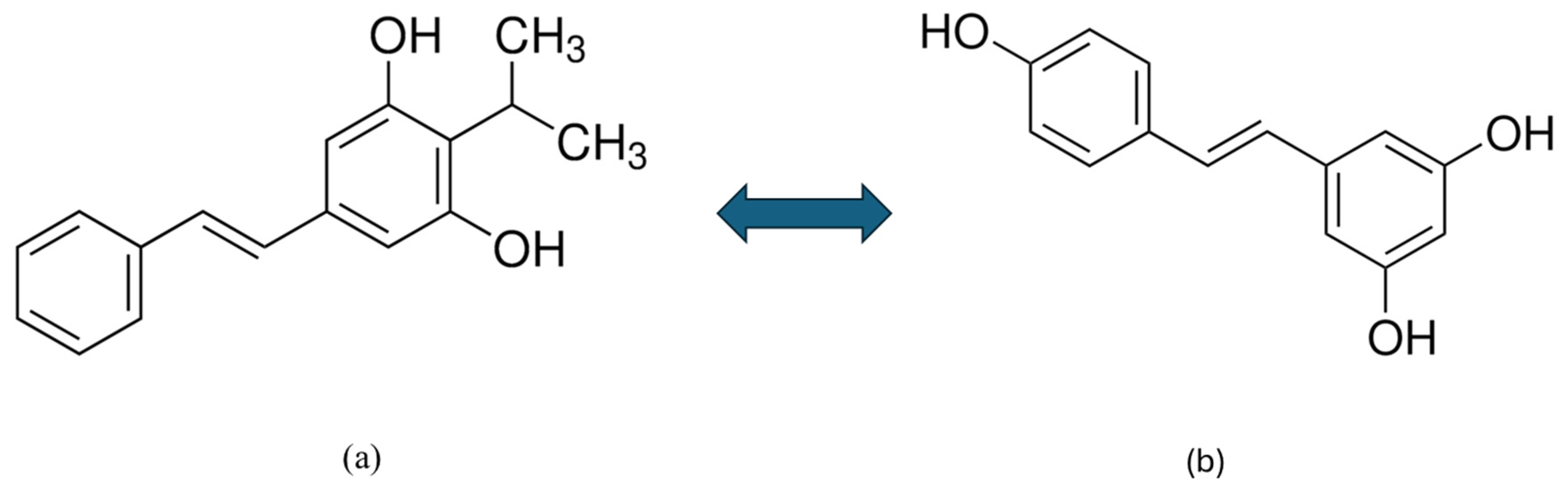
8.1. Structural Properties and Pharmacological Relevance of Tapinarof
8.2. Tapinarof as a New Nonsteroidal AhR Modulator
8.3. The Biological Origin of Tapinarof
8.4. The Role of AhR Activation and the Therapeutic Potential of Tapinarof in the Treatment of Inflammatory Skin Diseases
8.5. Results of Clinical Trials
8.5.1. Preclinical Studies
8.5.2. Clinical Studies
8.5.3. Long-Term Safety Studies
8.5.4. Pharmacokinetics
8.5.5. Side Effects
9. Nanotechnology in Dermatology
10. Nanoparticle Carriers
10.1. Nanoparticles
10.1.1. Vesicular Carriers
10.1.2. Lipid Nanoparticles
10.2. Nanofibres
10.3. Physical Carriers
10.4. Matrix Nanocarriers
11. Tapinarof Delivery Systems
11.1. Patented Tapinarof Formulations
11.2. Challenges in Formulating Tapinarof
11.3. Nanogel-Based Tapinarof Formulations
11.4. Future Directions
12. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Madawi, E.A.; Al Jayoush, A.R.; Rawas-Qalaji, M.; Thu, H.E.; Khan, S.; Sohail, M.; Mahmood, A.; Hussain, Z. Polymeric Nanoparticles as Tunable Nanocarriers for Targeted Delivery of Drugs to Skin Tissues for Treatment of Topical Skin Diseases. Pharmaceutics 2023, 15, 657. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Awasthi, R. Breakthroughs and Bottlenecks of Psoriasis Therapy: Emerging Trends and Advances in Lipid Based Nano-Drug Delivery Platforms for Dermal and Transdermal Drug Delivery. J. Drug Deliv. Sci. Technol. 2023, 84, 104548. [Google Scholar] [CrossRef]
- Siafaka, P.I.; Özcan Bülbül, E.; Okur, M.E.; Karantas, I.D.; Üstündağ Okur, N. The Application of Nanogels as Efficient Drug Delivery Platforms for Dermal/Transdermal Delivery. Gels 2023, 9, 753. [Google Scholar] [CrossRef]
- Jurel, P.; Bahadur, S.; Bajpai, M. Treatment of Chronic Plaque Psoriasis: An Overview on Current Update. Pharmacol. Res.-Rep. 2024, 2, 100004. [Google Scholar] [CrossRef]
- Biswasroy, P.; Pradhan, D.; Kar, B.; Ghosh, G.; Rath, G. Recent Advancement in Topical Nanocarriers for the Treatment of Psoriasis. AAPS PharmSciTech 2021, 22, 164. [Google Scholar] [CrossRef]
- Makuch, S.; Dróżdż, M.; Makarec, A.; Ziółkowski, P.; Woźniak, M. An Update on Photodynamic Therapy of Psoriasis—Current Strategies and Nanotechnology as a Future Perspective. Int. J. Mol. Sci. 2022, 23, 9845. [Google Scholar] [CrossRef]
- Dai, P.; Ge, X.; Sun, C.; Jiang, H.; Zuo, W.; Wu, P.; Liu, C.; Deng, S.; Yang, J.; Dai, J.; et al. A Novel Methacryloyl Chitosan Hydrogel Microneedles Patch with Sustainable Drug Release Property for Effective Treatment of Psoriasis. Macromol. Biosci. 2023, 23, 2300194. [Google Scholar] [CrossRef]
- Bodnár, K.; Fehér, P.; Ujhelyi, Z.; Bácskay, I.; Józsa, L. Recent Approaches for the Topical Treatment of Psoriasis Using Nanoparticles. Pharmaceutics 2024, 16, 449. [Google Scholar] [CrossRef]
- Zhu, B.; Jing, M.; Yu, Q.; Ge, X.; Yuan, F.; Shi, L. Treatments in Psoriasis: From Standard Pharmacotherapyto Nanotechnology Therapy. Adv. Dermatol. Allergol. 2022, 39, 460–471. [Google Scholar] [CrossRef]
- Sugumaran, D.; Yong, A.C.H.; Stanslas, J. Advances in Psoriasis Research: From Pathogenesis to Therapeutics. Life Sci. 2024, 355, 122991. [Google Scholar] [CrossRef]
- Igarashi, A.; Tsuji, G.; Fukasawa, S.; Murata, R.; Yamane, S. Tapinarof Cream for the Treatment of Plaque Psoriasis: Efficacy and Safety Results from 2 Japanese Phase 3 Trials. J. Dermatol. 2024, 51, 1269–1278. [Google Scholar] [CrossRef] [PubMed]
- Carmona-Rocha, E.; Rusiñol, L.; Puig, L. New and Emerging Oral/Topical Small-Molecule Treatments for Psoriasis. Pharmaceutics 2024, 16, 239. [Google Scholar] [CrossRef] [PubMed]
- Silverberg, J.I.; Boguniewicz, M.; Quintana, F.J.; Clark, R.A.; Gross, L.; Hirano, I.; Tallman, A.M.; Brown, P.M.; Fredericks, D.; Rubenstein, D.S.; et al. Tapinarof Validates the Aryl Hydrocarbon Receptor as a Therapeutic Target: A Clinical Review. J. Allergy Clin. Immunol. 2024, 154, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Urashima, T.; Katsuda, Y.; Yoshiuchi, H.; Ebihara, S.; Shinozaki, Y.; Kato, T.; Shimazaki, T.; Yasui, Y.; Mera, Y.; Konishi, N. Pharmacological Properties of Tapinarof in Mice as a Novel Topical Agent for Plaque Psoriasis. BPB Rep. 2024, 7, 116–122. [Google Scholar] [CrossRef]
- Saha, S. Transcutaneous Delivery of Disease Specific PI3K/Akt/mTOR Inhibitor Based Hybrid Nanoparticles in Hydrogel System for the Management of Psoriasis: Insights from in Vivo Studies. Int. J. Pharm. 2025, 627, 125325. [Google Scholar]
- Nogueira, S.; Rodrigues, M.A.; Vender, R.; Torres, T. Tapinarof for the Treatment of Psoriasis. Dermatol. Ther. 2022, 35, e15931. [Google Scholar] [CrossRef]
- Mascarenhas-Melo, F.; Carvalho, A.; Gonçalves, M.B.S.; Paiva-Santos, A.C.; Veiga, F. Nanocarriers for the Topical Treatment of Psoriasis—Pathophysiology, Conventional Treatments, Nanotechnology, Regulatory and Toxicology. Eur. J. Pharm. Biopharm. 2022, 176, 95–107. [Google Scholar] [CrossRef]
- Ahmad, M.Z.; Mohammed, A.A.; Algahtani, M.S.; Mishra, A.; Ahmad, J. Nanoscale Topical Pharmacotherapy in Management of Psoriasis: Contemporary Research and Scope. J. Funct. Biomater. 2022, 14, 19. [Google Scholar] [CrossRef]
- Yadav, T.; Yadav, H.; Raizaday, A.; Alam, M.S. The Treatment of Psoriasis via Herbal Formulation and Nanopolyherbal Formulation: A New Approach. BioImpacts 2024, 15, 30341. [Google Scholar] [CrossRef]
- Ortiz-Lopez, L.I.; Choudhary, V.; Bollag, W.B. Updated Perspectives on Keratinocytes and Psoriasis: Keratinocytes Are More Than Innocent Bystanders. Psoriasis Targets Ther. 2022, 12, 73–87. [Google Scholar] [CrossRef]
- Sieminska, I.; Pieniawska, M.; Grzywa, T.M. The Immunology of Psoriasis—Current Concepts in Pathogenesis. Clin. Rev. Allergy Immunol. 2024, 66, 164–191. [Google Scholar] [CrossRef] [PubMed]
- Lé, A.M.; Torres, T. New Topical Therapies for Psoriasis. Am. J. Clin. Dermatol. 2022, 23, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Vasowala, T.; Gharat, S.; Mhase, M.; Momin, M. Advances in Hydrogels Based Cutaneous Drug Delivery System for Management of Psoriasis. Eur. Polym. J. 2024, 202, 112630. [Google Scholar] [CrossRef]
- Aziz Hazari, S.; Kaur, H.; Karwasra, R.; Abourehab, M.A.S.; Ali Khan, A.; Kesharwani, P. An Overview of Topical Lipid-Based and Polymer-Based Nanocarriers for Treatment of Psoriasis. Int. J. Pharm. 2023, 638, 122938. [Google Scholar] [CrossRef]
- Gomes, G.S.; Frank, L.A.; Contri, R.V.; Longhi, M.S.; Pohlmann, A.R.; Guterres, S.S. Nanotechnology-Based Alternatives for the Topical Delivery of Immunosuppressive Agents in Psoriasis. Int. J. Pharm. 2023, 631, 122535. [Google Scholar] [CrossRef]
- Bissonnette, R.; Stein Gold, L.; Rubenstein, D.S.; Tallman, A.M.; Armstrong, A. Tapinarof in the Treatment of Psoriasis: A Review of the Unique Mechanism of Action of a Novel Therapeutic Aryl Hydrocarbon Receptor–Modulating Agent. J. Am. Acad. Dermatol. 2021, 84, 1059–1067. [Google Scholar] [CrossRef]
- Prabath, I.; Subramanian, S.; Rani, J. Tapinarof: A Felicitous Discovery in Psoriasis Treatment. J. Pharmacol. Pharmacother. 2022, 13, 222–228. [Google Scholar] [CrossRef]
- Assaf, J.; Sarkis, J.; Tomb, R. Tapinarof and the Future of Topical Treatments in Plaque Psoriasis. J. Am. Acad. Dermatol. 2021, 84, e283–e284. [Google Scholar] [CrossRef]
- Lin, X.; Meng, X.; Lin, J. The Role of Aryl Hydrocarbon Receptor in the Pathogenesis and Treatment of Psoriasis. J. Cutan. Med. Surg. 2024, 28, 276–286. [Google Scholar] [CrossRef]
- Shen, Q.; Liu, R.; Tan, S.; Xu, X.; Fang, J.; Li, R. Advances in Pathogenesis and Nanoparticles (NPs)-Mediated Treatment of Psoriasis. Front. Immunol. 2022, 13, 1089262. [Google Scholar] [CrossRef]
- Lee, H.-J.; Kim, M. Challenges and Future Trends in the Treatment of Psoriasis. Int. J. Mol. Sci. 2023, 24, 13313. [Google Scholar] [CrossRef] [PubMed]
- Sindrilaru, A.; Filip, A.; Scharffetter-Kochanek, K.; Crisan, D. How Can Nanoparticle-based Technologies Revolutionize the Topical Therapy in Psoriasis? Exp. Dermatol. 2020, 29, 1097–1103. [Google Scholar] [CrossRef] [PubMed]
- Grossmann, M.C.; Pixley, J.N.; Feldman, S.R. A Review of Topical Tapinarof for the Treatment of Plaque Psoriasis. Ann. Pharmacother. 2024, 58, 76–85. [Google Scholar] [CrossRef]
- Chandy, R.J.; Dao, D.-P.D.; Rivis, C.C.; Shan, D.M.; Feldman, S.R. Noncorticosteroid Topical Therapies for the Treatment of Plaque Psoriasis: A Narrative Review. J. Pharm. Technol. 2023, 39, 247–255. [Google Scholar] [CrossRef]
- Wazir, A.; O’Toole, E.A. Itching for Innovation: The Role of Aryl Hydrocarbon Receptor Agonists as a Future Therapy for Atopic Dermatitis. Clin. Exp. Dermatol. 2024, 50, llae502. [Google Scholar] [CrossRef]
- Cai, Z.; Zeng, Y.; Shi, X.; Zhang, X.; Zhu, H.; Wang, W. Benvitimod Inhibits MCM6-Meditated Proliferation of Keratinocytes by Regulating the JAK/STAT3 Pathway. J. Dermatol. Sci. 2023, 109, 71–79. [Google Scholar] [CrossRef]
- Mohd Nordin, U.U.; Ahmad, N.; Salim, N.; Mohd Yusof, N.S. Lipid-Based Nanoparticles for Psoriasis Treatment: A Review on Conventional Treatments, Recent Works, and Future Prospects. RSC Adv. 2021, 11, 29080–29101. [Google Scholar] [CrossRef]
- Armstrong, A.W.; Siegel, M.P.; Bagel, J.; Boh, E.E.; Buell, M.; Cooper, K.D.; Callis Duffin, K.; Eichenfield, L.F.; Garg, A.; Gelfand, J.M.; et al. From the Medical Board of the National Psoriasis Foundation: Treatment Targets for Plaque Psoriasis. J. Am. Acad. Dermatol. 2017, 76, 290–298. [Google Scholar] [CrossRef]
- Peppers, J.; Paller, A.S.; Maeda-Chubachi, T.; Wu, S.; Robbins, K.; Gallagher, K.; Kraus, J.E. A Phase 2, Randomized Dose-Finding Study of Tapinarof (GSK2894512 Cream) for the Treatment of Atopic Dermatitis. J. Am. Acad. Dermatol. 2019, 80, 89–98.e3. [Google Scholar] [CrossRef]
- Pareek, A.; Kumari, L.; Pareek, A.; Chaudhary, S.; Ratan, Y.; Janmeda, P.; Chuturgoon, S.; Chuturgoon, A. Unraveling Atopic Dermatitis: Insights into Pathophysiology, Therapeutic Advances, and Future Perspectives. Cells 2024, 13, 425. [Google Scholar] [CrossRef]
- Murphy, E.C.; Schaffter, S.W.; Friedman, A.J. Nanotechnology for Psoriasis Therapy. Curr. Dermatol. Rep. 2019, 8, 14–25. [Google Scholar] [CrossRef]
- Petit, R.G.; Cano, A.; Ortiz, A.; Espina, M.; Prat, J.; Muñoz, M.; Severino, P.; Souto, E.B.; García, M.L.; Pujol, M.; et al. Psoriasis: From Pathogenesis to Pharmacological and Nano-Technological-Based Therapeutics. Int. J. Mol. Sci. 2021, 22, 4983. [Google Scholar] [CrossRef] [PubMed]
- Valenzuela, F.; Flores, R. Immunogenicity to Biological Drugs in Psoriasis and Psoriatic Arthritis. Clinics 2021, 76, e3015. [Google Scholar] [CrossRef]
- Fitzgerald, T.; Zhdanava, M.; Pilon, D.; Shah, A.; Hilts, A.; Lefebvre, P.; Feldman, S.R. Long-Term Psoriasis Control with Guselkumab, Adalimumab, Secukinumab, or Ixekizumab in the USA. Dermatol. Ther. 2023, 13, 1053–1068. [Google Scholar] [CrossRef]
- Elgaard, C.D.B.; Iversen, L.; Hjuler, K.F. Guselkumab, Tildrakizumab, and Risankizumab in a Real-World Setting: Drug Survival and Effectiveness in the Treatment of Psoriasis and Psoriatic Arthritis. J. Dermatol. Treat. 2023, 34, 2133531. [Google Scholar] [CrossRef]
- Ruggiero, A.; Picone, V.; Martora, F.; Fabbrocini, G.; Megna, M. Guselkumab, Risankizumab, and Tildrakizumab in the Management of Psoriasis: A Review of the Real-World Evidence. Clin. Cosmet. Investig. Dermatol. 2022, 15, 1649–1658. [Google Scholar] [CrossRef]
- Roskoski, R. Deucravacitinib Is an Allosteric TYK2 Protein Kinase Inhibitor FDA-Approved for the Treatment of Psoriasis. Pharmacol. Res. 2023, 189, 106642. [Google Scholar] [CrossRef]
- Ahsan, S.; Degener, R.; Schlamp, M. Non-Invasive Treatments Invade the Psoriasis Pipeline. Available online: https://www.aquestconsulting.com/wp-content/uploads/2023/11/Aquest_Non-Invasive-Psoriasis-Pipeline-White-Paper-FINAL-1123.pdf (accessed on 9 March 2025).
- Bang, C.-H.; Park, C.-J.; Kim, Y.-S. The Expanding Therapeutic Potential of Deucravacitinib Beyond Psoriasis: A Narrative Review. J. Clin. Med. 2025, 14, 1745. [Google Scholar] [CrossRef]
- Truong, T.M.; Pathak, G.N.; Singal, A.; Taranto, V.; Rao, B.K. Deucravacitinib: The First FDA-Approved Oral TYK2 Inhibitor for Moderate to Severe Plaque Psoriasis. Ann. Pharmacother. 2024, 58, 416–427. [Google Scholar] [CrossRef]
- Gyldenløve, M.; Nissen, C.V.; Stave, S.D.W.; Thomsen, S.F.; Egeberg, A.; Loft, N. Oral Roflumilast in Patients with Psoriasis: A Real-World Cohort Study. Am. J. Clin. Dermatol. 2025, 26, 147–150. [Google Scholar] [CrossRef]
- Lé, A.M.; Yilmaz, O.; Luz, M.; Torres, T. Oral Roflumilast for Psoriasis: A Real-World 24-Week Prospective Cohort Study. J. Dermatol. Treat. 2025, 36, 2464107. [Google Scholar] [CrossRef] [PubMed]
- Ravindran, R.; Muralidharan, P.; Govindarajan, A. Systematizing PDE4 Inhibition in Psoriasis Treatment: Roflumilast Leads the Way. J. Young Pharm. 2025, 17, 13–18. [Google Scholar] [CrossRef]
- De Moraes-Souza, R.; Chahine Chater, R.; Pera Calvi, I.; Mesquita, Y.; Sarto, R.; Lapenda, I.; Figueiredo Pereira, L.; Moury, L.; Herranz-Pinto, P. Efficacy and Safety of Topical Roflumilast for the Treatment of Psoriasis: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Clin. Drug Investig. 2024, 44, 655–665. [Google Scholar] [CrossRef]
- Armstrong, A.W.; McConaha, J.L. Tapinarof Cream 1% Once Daily for the Treatment of Adults with Mild to Severe Plaque Psoriasis: A Novel Topical Therapy Targeting the Aryl Hydrocarbon Receptor. J. Manag. Care Spec. Pharm. 2023, 29, S1–S14. [Google Scholar]
- Orsini, D.; Assorgi, C.; Bonifati, C.; Cameli, N.; Graceffa, D.; Potestio, L.; Megna, M. Effectiveness and Safety of Risankizumab in VEry Severe Plaque Psoriasis: A Real-Life Retrospective Study (VESPA-Study). J. Dermatol. Treat. 2024, 35, 2358150. [Google Scholar] [CrossRef]
- Gordon, K.B.; Blauvelt, A.; Bachelez, H.; Coates, L.C.; Van Den Bosch, F.E.; Kaplan, B.; Koetse, W.; Ashley, D.G.; Lippe, R.; Sinvhal, R.; et al. Long-Term Safety of Risankizumab in Patients with Psoriatic Disease: A Comprehensive Analysis from Clinical Trials. Dermatol. Ther. 2024, 14, 2523–2538. [Google Scholar] [CrossRef]
- Vender, R.B.; Lynde, C.W. Certolizumab Pegol Use in the Treatment of Moderate-to-Severe Psoriasis: Real-World Data From Two Canadian Centers. J. Cutan. Med. Surg. 2022, 26, 267–273. [Google Scholar] [CrossRef]
- Lee, A.; Scott, L.J. Certolizumab Pegol: A Review in Moderate to Severe Plaque Psoriasis. BioDrugs 2020, 34, 235–244. [Google Scholar] [CrossRef]
- Coto-Segura, P.; Segú-Vergés, C.; Martorell, A.; Moreno-Ramírez, D.; Jorba, G.; Junet, V.; Guerri, F.; Daura, X.; Oliva, B.; Cara, C.; et al. A Quantitative Systems Pharmacology Model for Certolizumab Pegol Treatment in Moderate-to-Severe Psoriasis. Front. Immunol. 2023, 14, 1212981. [Google Scholar] [CrossRef]
- Turkmen, M.; Dogan, S. Certolizumab Pegol in the Treatment of Psoriasis: Real-life Data. Dermatol. Ther. 2021, 34, e14929. [Google Scholar] [CrossRef]
- Bubna, A.K.; Patil, N. Tildrakizumab in Psoriasis and Beyond. J. Dermatol. Dermatol. Surg. 2024, 28, 1–10. [Google Scholar] [CrossRef]
- Bagel, J. Biologics in Psoriasis: The Next Generation. Practical Dermatology. Available online: https://practicaldermatology.com/topics/psoriasis/biologics-in-psoriasis-the-next-generation/20807/ (accessed on 2 April 2025).
- Megna, M.; Ruggiero, A.; Tommasino, N.; Brescia, C.; Martora, F.; Cacciapuoti, S.; Potestio, L. Effectiveness and Safety of Tildrakizumab in Psoriasis Patients Who Failed Anti-IL17 Treatment: A 28-Week Real-Life Study. Clin. Cosmet. Investig. Dermatol. 2024, 17, 1037–1042. [Google Scholar] [CrossRef] [PubMed]
- Gebauer, K.; Spelman, L.; Yamauchi, P.S.; Bagel, J.; Nishandar, T.; Crane, M.; Kopeloff, I.; Kothekar, M.; Yao, S.-L.; Sofen, H.L. Efficacy and Safety of Tildrakizumab for the Treatment of Moderate-to-Severe Plaque Psoriasis of the Scalp: A Multicenter, Randomized, Double-Blind, Placebo-Controlled, Phase 3b Study. J. Am. Acad. Dermatol. 2024, 91, 91–99. [Google Scholar] [CrossRef]
- Lamb, Y.N. Guselkumab in Psoriatic Arthritis: A Profile of Its Use. Drugs Ther. Perspect. 2021, 37, 285–293. [Google Scholar] [CrossRef]
- Strober, B.; Coates, L.C.; Lebwohl, M.G.; Deodhar, A.; Leibowitz, E.; Rowland, K.; Kollmeier, A.P.; Miller, M.; Wang, Y.; Li, S.; et al. Long-Term Safety of Guselkumab in Patients with Psoriatic Disease: An Integrated Analysis of Eleven Phase II/III Clinical Studies in Psoriasis and Psoriatic Arthritis. Drug Saf. 2024, 47, 39–57. [Google Scholar] [CrossRef]
- Megna, M.; Ruggiero, A.; Martora, F.; Vallone, Y.; Guerrasio, G.; Potestio, L. Long-Term Efficacy and Safety of Guselkumab in Psoriasis Patients Who Failed Anti-IL17: A Two-Year Real-Life Study. J. Clin. Med. 2024, 13, 2691. [Google Scholar] [CrossRef]
- Blauvelt, A.; Langley, R.G.; Branigan, P.J.; Liu, X.; Chen, Y.; DePrimo, S.; Ma, K.; Scott, B.; Campbell, K.; Muñoz-Elías, E.J.; et al. Guselkumab Reduces Disease- and Mechanism-Related Biomarkers More Than Adalimumab in Patients with Psoriasis: A VOYAGE 1 Substudy. JID Innov. 2024, 4, 100287. [Google Scholar] [CrossRef]
- Puig, L. Brodalumab: The First Anti-IL-17 Receptor Agent for Psoriasis. Drugs Today 2017, 53, 283. [Google Scholar] [CrossRef]
- Lebwohl, M.G.; Armstrong, A.W.; Alexis, A.F.; Lain, E.L.; Jacobson, A.A. Efficacy of Brodalumab in Patients with Psoriasis and Risk Factors for Treatment Failure: A Review of Post Hoc Analyses. Dermatol. Ther. 2024, 14, 2709–2726. [Google Scholar] [CrossRef]
- Menter, A.; Bhutani, T.; Ehst, B.; Elewski, B.; Jacobson, A. Narrative Review of the Emerging Therapeutic Role of Brodalumab in Difficult-to-Treat Psoriasis. Dermatol. Ther. 2022, 12, 1289–1302. [Google Scholar] [CrossRef]
- Syed, Y.Y. Ixekizumab: A Review in Moderate to Severe Plaque Psoriasis. Am. J. Clin. Dermatol. 2017, 18, 147–158. [Google Scholar] [CrossRef] [PubMed]
- Reich, A.; Reed, C.; Schuster, C.; Robert, C.; Treuer, T.; Lubrano, E. Real-World Evidence for Ixekizumab in the Treatment of Psoriasis and Psoriatic Arthritis: Literature Review 2016–2021. J. Dermatol. Treat. 2023, 34, 2160196. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.; Puravath, A.P.; Orbai, A.-M. Ixekizumab for Psoriatic Arthritis: Safety, Efficacy, and Patient Selection. J. Inflamm. Res. 2021, 14, 6975–6991. [Google Scholar] [CrossRef]
- PubChem Tapinarof. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/6439522 (accessed on 9 March 2025).
- Benvitimod ≥ 98% (HPLC)|Sigma-Aldrich. Available online: https://www.sigmaaldrich.com/HU/en/product/sigma/sml3430 (accessed on 9 March 2025).
- Tapinarof|99.98%(HPLC)|AhR Agonist. Available online: https://www.selleckchem.com/products/tapinarof.html (accessed on 9 March 2025).
- Pecyna, P.; Wargula, J.; Murias, M.; Kucinska, M. More Than Resveratrol: New Insights into Stilbene-Based Compounds. Biomolecules 2020, 10, 1111. [Google Scholar] [CrossRef]
- Smith, S.H.; Jayawickreme, C.; Rickard, D.J.; Nicodeme, E.; Bui, T.; Simmons, C.; Coquery, C.M.; Neil, J.; Pryor, W.M.; Mayhew, D.; et al. Tapinarof Is a Natural AhR Agonist That Resolves Skin Inflammation in Mice and Humans. J. Investig. Dermatol. 2017, 137, 2110–2119. [Google Scholar] [CrossRef]
- Zatloukalova, M.; Hanyk, J.; Papouskova, B.; Kabelac, M.; Vostalova, J.; Vacek, J. Tapinarof and Its Structure-Activity Relationship for Redox Chemistry and Phototoxicity on Human Skin Keratinocytes. Free Radic. Biol. Med. 2024, 223, 212–223. [Google Scholar] [CrossRef]
- Shah, D.K.; Yi, D.S.; Yangxin, D.C.; Ankit, D.S. Treatment Challenges in Atopic Dermatitis with Novel Topical Therapies. J. Dermatol. Treat. 2018, 7, 136–143. [Google Scholar]
- Robbins, K.; Bissonnette, R.; Maeda-Chubachi, T.; Ye, L.; Peppers, J.; Gallagher, K.; Kraus, J.E. Phase 2, Randomized Dose-Finding Study of Tapinarof (GSK2894512 Cream) for the Treatment of Plaque Psoriasis. J. Am. Acad. Dermatol. 2019, 80, 714–721. [Google Scholar] [CrossRef]
- Hu, Y.-Q.; Liu, P.; Mu, Z.; Zhang, J.-Z. Anti-Inflammatory Effects of AhR Agonist Benvitimod in TNFα/IFNγ Stimulated HaCaT Cells and Peripheral Blood Mononuclear Cells from Patients with Atopic Dermatitis. arXiv 2022. [Google Scholar] [CrossRef]
- Zhang, J.; Cai, L.; Zheng, M. A Novel Topical Treatment for Plaque Psoriasis: Benvitimod/Tapinarof. J. Am. Acad. Dermatol. 2022, 86, e137–e138. [Google Scholar] [CrossRef]
- Keam, S.J. Tapinarof Cream 1%: First Approval. Drugs 2022, 82, 1221–1228. [Google Scholar] [CrossRef] [PubMed]
- Tian, C.; Zhang, G.; Xia, Z.; Chen, N.; Yang, S.; Li, L. Identification of Triazolopyridine Derivatives as a New Class of AhR Agonists and Evaluation of Anti-Psoriasis Effect in a Mouse Model. Eur. J. Med. Chem. 2022, 231, 114122. [Google Scholar] [CrossRef] [PubMed]
- Bissonnette, R.; Saint-Cyr Proulx, E.; Jack, C.; Maari, C. Tapinarof for Psoriasis and Atopic Dermatitis: 15 Years of Clinical Research. J. Eur. Acad. Dermatol. Venereol. 2023, 37, 1168–1174. [Google Scholar] [CrossRef]
- Ali, S.; Ion, A.; Orzan, O.A.; Bălăceanu-Gurău, B. Emerging Treatments and New Vehicle Formulations for Atopic Dermatitis. Pharmaceutics 2024, 16, 1425. [Google Scholar] [CrossRef]
- Lu, S.T.; Kelly, K.A.; Feldman, S.R. An Overview of Benvitimod for the Treatment of Psoriasis: A Narrative Review. Expert Opin. Pharmacother. 2022, 23, 327–333. [Google Scholar] [CrossRef]
- Strober, B.; Stein Gold, L.; Bissonnette, R.; Armstrong, A.W.; Kircik, L.; Tyring, S.K.; Piscitelli, S.C.; Brown, P.M.; Rubenstein, D.S.; Tallman, A.M.; et al. One-Year Safety and Efficacy of Tapinarof Cream for the Treatment of Plaque Psoriasis: Results from the PSOARING 3 Trial. J. Am. Acad. Dermatol. 2022, 87, 800–806. [Google Scholar] [CrossRef]
- Paller, A.S.; Stein Gold, L.; Soung, J.; Tallman, A.M.; Rubenstein, D.S.; Gooderham, M. Efficacy and Patient-Reported Outcomes from a Phase 2b, Randomized Clinical Trial of Tapinarof Cream for the Treatment of Adolescents and Adults with Atopic Dermatitis. J. Am. Acad. Dermatol. 2021, 84, 632–638. [Google Scholar] [CrossRef]
- Santini, G.; Bonati, L.; Motta, S. From Tapinarof to Novel AhR Modulators: Computational Drug Discovery for Psoriasis Therapeutics. Res. Sq. 2025. Preprint posted. [Google Scholar] [CrossRef]
- Dutky, S.R. Insect Microbiology. In Advances in Applied Microbiology; Umbreit, W.W., Ed.; Academic Press: Cambridge, MA, USA, 1959; Volume 1, pp. 175–200. ISBN 0065-2164. [Google Scholar]
- An Open-Label, Long-Term Extension Study to Evaluate the Safety and Efficacy of Tapinarof Cream, 1% in Subjects With Atopic Dermatitis. 2021. Available online: https://clinicaltrials.gov/study/NCT05142774 (accessed on 9 March 2025).
- Zhao, Y.; Wu, C.; Cai, L.; Mu, Z.; Liu, X.; Zhang, W.; Zhang, J. Tapinarof Inhibits Psoriatic Inflammation through Inducing Tolerogenic Dendritic Cells and Foxp3+ Tregs. Chin. Med. J. 2024, 137, 2877–2879. [Google Scholar] [CrossRef]
- Zhu, X.; Han, R.; Tian, X.; Hochgerner, M.; Li, H.; Wang, J.; Xia, J. The Opposite Effect of Tapinarof between IMQ and IL-23 Induced Psoriasis Mouse Models. Exp. Dermatol. 2024, 33, e14862. [Google Scholar] [CrossRef]
- Jett, J.E.; McLaughlin, M.; Lee, M.S.; Parish, L.C.; DuBois, J.; Raoof, T.J.; Tabolt, G.; Wilson, T.; Somerville, M.C.; DellaMaestra, W.; et al. Tapinarof Cream 1% for Extensive Plaque Psoriasis: A Maximal Use Trial on Safety, Tolerability, and Pharmacokinetics. Am. J. Clin. Dermatol. 2022, 23, 83–91. [Google Scholar] [CrossRef] [PubMed]
- A Phase 3 Study of Tapinarof for the Treatment of Plaque Psoriasis in Pediatric Subjects. 2021. Available online: https://clinicaltrials.gov/study/NCT05172726 (accessed on 9 March 2025).
- Igarashi, A.; Tsuji, G.; Murata, R.; Fukasawa, S.; Yamane, S. A Phase 2, Randomized, Double-blind, Vehicle-controlled Trial of Tapinarof Cream in Japanese Pediatric Patients with Atopic Dermatitis. J. Dermatol. 2025, 52, 247–255. [Google Scholar] [CrossRef] [PubMed]
- Simpson, E.L.; Hebert, A.A.; Browning, J.; Serrao, R.T.; Sofen, H.; Brown, P.M.; Piscitelli, S.C.; Rubenstein, D.S.; Tallman, A.M. Tapinarof Improved Outcomes and Sleep for Patients and Families in Two Phase 3 Atopic Dermatitis Trials in Adults and Children. Dermatol. Ther. 2025, 15, 111–124. [Google Scholar] [CrossRef] [PubMed]
- A Phase 3 Efficacy and Safety Study of Tapinarof for the Treatment of Moderate to Severe Atopic Dermatitis in Children and Adults. 2021. Available online: https://clinicaltrials.gov/study/NCT05032859 (accessed on 9 March 2025).
- Silverberg, J.I.; Eichenfield, L.F.; Hebert, A.A.; Simpson, E.L.; Stein Gold, L.; Bissonnette, R.; Papp, K.A.; Browning, J.; Kwong, P.; Korman, N.J.; et al. Tapinarof Cream 1% Once Daily: Significant Efficacy in the Treatment of Moderate to Severe Atopic Dermatitis in Adults and Children down to 2 Years of Age in the Pivotal Phase 3 ADORING Trials. J. Am. Acad. Dermatol. 2024, 91, 457–465. [Google Scholar] [CrossRef]
- Ghani, H.; Podwojniak, A.; Tan, I.J.; Parikh, A.K.; Sanabria, B.; Rao, B. A Comparison of the Safety and Efficacy of Tapinarof and Roflumilast Topical Therapies in the Management of Mild-to-moderate Plaque Psoriasis. Skin Res. Technol. 2024, 30, e70041. [Google Scholar] [CrossRef]
- Teva Pharmaceuticals USA. A Randomized, Double-Blind, Placebo-Controlled, Parallel-Group, Multiple-Site, Clinical Study to Evaluate the Therapeutic Equivalence of Tapinarof Cream 1% (Teva Pharmaceuticals, Inc.) with VTAMA® Tapinarof (Tapinarof) Cream 1% (Dermavant Sciences, Inc.) in Adult Patients with Plaque Psoriasis; National Library of Medicine: Bethesda, MD, USA, 2024.
- A Phase 4, Open-Label, Study to Investigate the Efficacy and Safety of VTAMA® (Tapinarof) Cream 1% in the Treatment of Plaque Psoriasis in Intertriginous Areas. 2022. Available online: https://clinicaltrials.gov/study/NCT05680740 (accessed on 9 March 2025).
- Gul, R.; Ahmed, N.; Ullah, N.; Khan, M.I.; Elaissari, A.; Rehman, A.U. Biodegradable Ingredient-Based Emulgel Loaded with Ketoprofen Nanoparticles. AAPS PharmSciTech 2018, 19, 1869–1881. [Google Scholar] [CrossRef]
- Abdellatif, A.A.H.; Alsowinea, A.F. Approved and Marketed Nanoparticles for Disease Targeting and Applications in COVID-19. Nanotechnol. Rev. 2021, 10, 1941–1977. [Google Scholar] [CrossRef]
- Yin, Y.; Hu, B.; Yuan, X.; Cai, L.; Gao, H.; Yang, Q. Nanogel: A Versatile Nano-Delivery System for Biomedical Applications. Pharmaceutics 2020, 12, 290. [Google Scholar] [CrossRef]
- Mastella, P.; Todaro, B.; Luin, S. Nanogels: Recent Advances in Synthesis and Biomedical Applications. Nanomaterials 2024, 14, 1300. [Google Scholar] [CrossRef]
- Botha, N.L.; Mushonga, P.; Onani, M.O. Review on Nanogels and Their Applications on Dermal Therapy. Polym. Polym. Compos. 2023, 31, 09673911231192816. [Google Scholar] [CrossRef]
- Gupta, V.; Mohapatra, S.; Mishra, H.; Farooq, U.; Kumar, K.; Ansari, M.; Aldawsari, M.; Alalaiwe, A.; Mirza, M.; Iqbal, Z. Nanotechnology in Cosmetics and Cosmeceuticals—A Review of Latest Advancements. Gels 2022, 8, 173. [Google Scholar] [CrossRef] [PubMed]
- Fytianos, G.; Rahdar, A.; Kyzas, G.Z. Nanomaterials in Cosmetics: Recent Updates. Nanomaterials 2020, 10, 979. [Google Scholar] [CrossRef] [PubMed]
- Sainaga Jyothi, V.G.S.; Ghouse, S.M.; Khatri, D.K.; Nanduri, S.; Singh, S.B.; Madan, J. Lipid Nanoparticles in Topical Dermal Drug Delivery: Does Chemistry of Lipid Persuade Skin Penetration? J. Drug Deliv. Sci. Technol. 2022, 69, 103176. [Google Scholar] [CrossRef]
- Aggarwal, G.; Dhawan, B.; Harikumar, S. Enhanced Transdermal Permeability of Piroxicam through Novel Nanoemulgel Formulation. Int. J. Pharm. Investig. 2014, 4, 65. [Google Scholar] [CrossRef]
- Algahtani, M.S.; Ahmad, M.Z.; Nourein, I.H.; Albarqi, H.A.; Alyami, H.S.; Alyami, M.H.; Alqahtani, A.A.; Alasiri, A.; Algahtani, T.S.; Mohammed, A.A.; et al. Preparation and Characterization of Curcumin Nanoemulgel Utilizing Ultrasonication Technique for Wound Healing: In Vitro, Ex Vivo, and In Vivo Evaluation. Gels 2021, 7, 213. [Google Scholar] [CrossRef]
- Li, N.; Qin, Y.; Dai, D.; Wang, P.; Shi, M.; Gao, J.; Yang, J.; Xiao, W.; Song, P.; Xu, R. Transdermal Delivery of Therapeutic Compounds With Nanotechnological Approaches in Psoriasis. Front. Bioeng. Biotechnol. 2022, 9, 804415. [Google Scholar] [CrossRef]
- Walunj, M.; Doppalapudi, S.; Bulbake, U.; Khan, W. Preparation, Characterization, and in Vivo Evaluation of Cyclosporine Cationic Liposomes for the Treatment of Psoriasis. J. Liposome Res. 2020, 30, 68–79. [Google Scholar] [CrossRef]
- Abu Hashim, I.; Abo El-Magd, N.; El-Sheakh, A.; Hamed, M.; Abd El-Gawad, A.E.-G. Pivotal Role of Acitretin Nanovesicular Gel for Effective Treatment of Psoriasis: Ex Vivo–in Vivo Evaluation Study. Int. J. Nanomed. 2018, 13, 1059–1079. [Google Scholar] [CrossRef]
- Vohra, P.; Varekar, S.; Shah, V. Nano-Transferosomes of Aloe-Vera and Vitamin-E for Management of Psoriasis: An Archetype in Herbal Drug Technology. Int. J. Innov. Res. Technol. 2023, 9, 876–882. [Google Scholar]
- Dadwal, N.; Amisha; Singh, D.; Singh, A. Quality-by-Design Approach for Investigating the Efficacy of Tacrolimus and Hyaluronic Acid–Loaded Ethosomal Gel in Dermal Management of Psoriasis: In Vitro, Ex Vivo, and In Vivo Evaluation. AAPS PharmSciTech 2023, 24, 220. [Google Scholar] [CrossRef]
- Serini, S.; Trombino, S.; Cassano, R.; Marino, M.; Calviello, G. Anti-Inflammatory Effects of Curcumin-Based Nanoparticles Containing α-Linolenic Acid in a Model of Psoriasis In Vitro. Nutrients 2025, 17, 692. [Google Scholar] [CrossRef] [PubMed]
- Llorente, X.; Esteruelas, G.; Bonilla, L.; Agudelo, M.G.; Filgaira, I.; Lopez-Ramajo, D.; Gong, R.C.; Soler, C.; Espina, M.; García, M.L.; et al. Riluzole-Loaded Nanostructured Lipid Carriers for Hyperproliferative Skin Diseases. Int. J. Mol. Sci. 2023, 24, 8053. [Google Scholar] [CrossRef] [PubMed]
- Tomar, Y.; Pandit, N.; Priya, S.; Singhvi, G. Evolving Trends in Nanofibers for Topical Delivery of Therapeutics in Skin Disorders. ACS Omega 2023, 8, 18340–18357. [Google Scholar] [CrossRef] [PubMed]
- Kang, N.-W.; Kim, M.-H.; Sohn, S.-Y.; Kim, K.-T.; Park, J.-H.; Lee, S.-Y.; Lee, J.-Y.; Kim, D.-D. Curcumin-Loaded Lipid-Hybridized Cellulose Nanofiber Film Ameliorates Imiquimod-Induced Psoriasis-like Dermatitis in Mice. Biomaterials 2018, 182, 245–258. [Google Scholar] [CrossRef]
- Du, H.; Liu, P.; Zhu, J.; Lan, J.; Li, Y.; Zhang, L.; Zhu, J.; Tao, J. Hyaluronic Acid-Based Dissolving Microneedle Patch Loaded with Methotrexate for Improved Treatment of Psoriasis. ACS Appl. Mater. Interfaces 2019, 11, 43588–43598. [Google Scholar] [CrossRef]
- Nguyen, T.-T.-L.; Duong, V.-A. A Review on Nanosystem-Based Delivery of Tofacitinib for Enhanced Treatment of Autoimmune Diseases and Inflammation. BioNanoScience 2024, 14, 2048–2064. [Google Scholar] [CrossRef]
- Manimaran, V.; Nivetha, R.P.; Tamilanban, T.; Narayanan, J.; Vetriselvan, S.; Fuloria, N.K.; Chinni, S.V.; Sekar, M.; Fuloria, S.; Wong, L.S.; et al. Nanogels as Novel Drug Nanocarriers for CNS Drug Delivery. Front. Mol. Biosci. 2023, 10, 1232109. [Google Scholar] [CrossRef]
- Suhail, M.; Rosenholm, J.M.; Minhas, M.U.; Badshah, S.F.; Naeem, A.; Khan, K.U.; Fahad, M. Nanogels As Drug-Delivery Systems: A Comprehensive Overview. Ther. Deliv. 2019, 10, 697–717. [Google Scholar] [CrossRef]
- Chandrashekhar, B.S. Tretinoin Nanogel 0.025% Versus Conventional Gel 0.025% in Patients with Acne Vulgaris: A Randomized, Active Controlled, Multicentre, Parallel Group, Phase IV Clinical Trial. J. Clin. Diagn. Res. 2015, 9, WC04. [Google Scholar] [CrossRef]
- Avasatthi, V.; Pawar, H.; Dora, C.P.; Bansod, P.; Gill, M.S.; Suresh, S. A Novel Nanogel Formulation of Methotrexate for Topical Treatment of Psoriasis: Optimization, in Vitro and in Vivo Evaluation. Pharm. Dev. Technol. 2016, 21, 554–562. [Google Scholar] [CrossRef]
- Kakade, P.; Patravale, V.; Patil, A.; Disouza, J. Formulation Development of Nanostructured Lipid Carrier-Based Nanogels Encapsulating Tacrolimus for Sustained Therapy of Psoriasis. Int. J. Pharm. 2024, 660, 124172. [Google Scholar] [CrossRef] [PubMed]
- Vashist, A.; Perez Alvarez, G.; Andion Camargo, V.; Raymond, A.D.; Arias, A.Y.; Kolishetti, N.; Vashist, A.; Manickam, P.; Aggarwal, S.; Nair, M. Recent Advances in Nanogels for Drug Delivery and Biomedical Applications. Biomater. Sci. 2024, 12, 6006–6018. [Google Scholar] [CrossRef] [PubMed]
- Tariq, L.; Arafah, A.; Ali, S.; Beigh, S.; Dar, M.A.; Dar, T.U.H.; Dar, A.I.; Alsaffar, R.M.; Masoodi, M.H.; Rehman, M.U. Nanogel-Based Transdermal Drug Delivery System: A Therapeutic Strategywith Under Discussed Potential. Curr. Top. Med. Chem. 2023, 23, 44–61. [Google Scholar] [CrossRef] [PubMed]
- Kraus, J.E.; Lee, J. Use of Tapinarof for the Treatment of Chronic Plaque Psoriasis. 2023. Available online: https://patents.google.com/patent/US11590088B2/en (accessed on 19 May 2025).
- Kraus, J.E.; Lee, J. Use of Tapinarof for the Treatment of Atopic Dermatitis. 2024. Available online: https://patents.google.com/patent/US11938099B2/en?oq=US11938099B2 (accessed on 19 May 2025).
- Arkin, M.; Zighelboim, M. Treatment of Ocular Diseases with Ophthalmic Tapinarof Compositions. 2021. Available online: https://patents.google.com/patent/US20210000758A1/en?oq=US20210000758A1 (accessed on 19 May 2025).
- Jain, P.; Tabolt, G.; Rubenstein, D.S.; Kalluri, H.; Catubig, R.; Roughan, B.; Buchta, R.; Bonjour, F.M.G.; Brady, B.P.; Sutcliffe, L.H. Gel, Ointment, and Foam Formulations of Tapinarof and Methods of Use 2022. U.S. Patent Application 17/533,885, 19 May 2025. [Google Scholar]
- Balogh, B.; Pető, Á.; Haimhoffer, Á.; Sinka, D.; Kósa, D.; Fehér, P.; Ujhelyi, Z.; Argenziano, M.; Cavalli, R.; Bácskay, I. Formulation and Evaluation of Different Nanogels of Tapinarof for Treatment of Psoriasis. Gels 2024, 10, 675. [Google Scholar] [CrossRef]


| Active Substance | Market Name | Application | Drug Class | Indication | FDA Approval Year | Ref. |
|---|---|---|---|---|---|---|
| Bimekizumab | Bimzelx | subcutaneous injection | IL-17A, IL-17F antagonist | moderate-to-severe plaque psoriasis | 2023 | [47,48,49] |
| Deucravacitinib | Sotyktu | oral application | TYK2 inhibitor | moderate-to-severe plaque psoriasis | 2022 | [43,47,48,49,50] |
| Roflumilast | Zoryve | topical application | PDE4 inhibitor | mild-to-severe plaque psoriasis | 2022 | [51,52,53,54] |
| Tapinarof | Vtama | topical application | AhR agonist | mild-to-severe plaque psoriasis | 2022 | [27,42,55] |
| Risankizumab | Skyrizi | subcutaneous injection | IL-23 antagonist | moderate-to-severe plaque psoriasis | 2019 | [43,44,56,57] |
| Certolizumab pegol | Cimzia | subcutaneous injection | TNF-α blocker | moderate-to-severe plaque psoriasis | 2018 | [58,59,60,61] |
| Tildrakizumab | Ilumya | subcutaneous injection | IL-23 antagonist | moderate-to-severe plaque psoriasis | 2018 | [62,63,64,65] |
| Guselkumab | Tremfya | subcutaneous injection | IL-23 antagonist | moderate-to-severe plaque psoriasis | 2017 | [43,66,67,68,69] |
| Brodalumab | Siliq | subcutaneous injection | IL-17A antagonist | moderate-to-severe plaque psoriasis | 2017 | [43,70,71,72] |
| Ixekizumab | Taltz | subcutaneous injection | IL-17A antagonist | moderate-to-severe plaque psoriasis, psoriatic arthritis | 2016 | [43,73,74,75] |
| Effect | Mechanism |
|---|---|
| Anti-inflammatory effect | Reduces the expression of Th2 cytokines (IL-4, IL-5, IL-13, IL-31) and Th17 cytokines (IL-17A, IL-17F), which are involved in the pathogenesis of psoriasis. |
| Skin barrier enhancement | Increases the expression of skin barrier proteins (filaggrin, loricrin, involucrin) and ceramide skin lipids, helping to normalise the skin barrier. |
| Antioxidant effect | Activates the Nrf2 pathway and reduces reactive oxygen species levels, contributing to the reduction in oxidative stress and the antioxidant response of the skin. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balogh, B.; Pető, Á.; Fehér, P.; Ujhelyi, Z.; Bácskay, I. Tapinarof Nanogels as a Promising Therapeutic Approach. Pharmaceutics 2025, 17, 731. https://doi.org/10.3390/pharmaceutics17060731
Balogh B, Pető Á, Fehér P, Ujhelyi Z, Bácskay I. Tapinarof Nanogels as a Promising Therapeutic Approach. Pharmaceutics. 2025; 17(6):731. https://doi.org/10.3390/pharmaceutics17060731
Chicago/Turabian StyleBalogh, Barbara, Ágota Pető, Pálma Fehér, Zoltán Ujhelyi, and Ildikó Bácskay. 2025. "Tapinarof Nanogels as a Promising Therapeutic Approach" Pharmaceutics 17, no. 6: 731. https://doi.org/10.3390/pharmaceutics17060731
APA StyleBalogh, B., Pető, Á., Fehér, P., Ujhelyi, Z., & Bácskay, I. (2025). Tapinarof Nanogels as a Promising Therapeutic Approach. Pharmaceutics, 17(6), 731. https://doi.org/10.3390/pharmaceutics17060731