
Preformulation Study of Carbamazepine Orally Disintegrating Tablets for Pediatric Patients Using Direct Compression and the SeDeM Diagram Tool: A Quality by Design Approach


 ,
,  , ,
, , 

Abstract
1. Introduction
2. Materials and Methods
2.1. Material
2.2. Methods
2.2.1. QbD Application to the Formulation Development
2.2.2. Crystal X-Ray Diffraction Method
2.2.3. Determination of Particle Size Distribution (PSD)
2.2.4. Powder Characterization Using SeDeM System
- -
- Bulk density (Da): Bulk density was determined according to monograph 2.9.34 of the Eur. Ph. [34]. Approximately 100 g of sample (or an adjusted amount to obtain a volume between 50 and 250 mL) was carefully poured into a graduated cylinder without compacting the powder. The initial volume (Vo) occupied by the sample was recorded without applying any mechanical treatment. Bulk density was then calculated using the following equation:where m is the mass (g) of the sample and Vo the initial apparent volume (mL).
- -
- Tapped density (Dc): Tapped density was measured using the same setup as for bulk density, following the procedure described in monograph 2.9.34 of the Eur. Ph. [34]. After recording the initial volume, the cylinder was tapped using an automatic volumeter (SBS Volumenometer) with 10, 500, and 1250 taps. The apparent volume was recorded after each tapping cycle. If the difference between the volumes measured after 500 and 1250 taps exceeded 2 mL, an additional 1250 taps were applied, bringing the total to 2500. The final tapped density (V1250 or V2500) was used to calculate the tapped density using the following equation:where m is the mass (g) of the sample and V1250 and V2500 are the compacted apparent volumes (mL) after 1250 and 2500 strokes, respectively.
- -
- Interparticle porosity (Ie): The interparticle porosity of the powder mixture is calculated from the following Equation (3).
- -
- Carr index (IC): This parameter is calculated using Equation (4).In both equations, Dc represents the tapped density (g/mL) and Da represents the bulk density (g/mL) of the powder mixture.
- -
- Cohesion index (Icd): This index is determined by compressing the powder, preferably using an eccentric press. Initially, the mean hardness (N) of the tablets is calculated. If the raw powder cannot be compressed, 3.5% of the standardized lubricant mixture shown in Table 1 is added.
- -
- Hausner ratio (IH): Determines the easiness of flow of the studied sample. It is calculated from Equation (5), as outlined in Section 2.9.34 of the Eur. Ph. [34].where Dc represents the tapped density (g/mL) and Da represents the bulk density (g/mL) of the powder mixture.
- -
- Angle of repose (α): The angle is determined according to the method described in Section 2.9.36 of the Eur. Ph. [35]. It represents the angle of the cone formed when the product is passed through a funnel with specific dimensions: a funnel height of 9.5 cm, an upper diameter of spout of 7.2 cm, and an inner diameter at the bottom narrow end of the spout of 1.8 cm. The funnel (ANORSA reference X5992) is positioned on a stand 20 cm above the tablet surface, centered on a millimeter grid sheet where two intersecting lines mark the center. The narrow end of the funnel nozzle is capped and leveled with the sample by running a spatula along the funnel sides. Upon removing the stopper, the powder falls onto the millimeter sheet. The four radii at the base of the cone are measured using a sliding caliper, and their mean value (r) is calculated. Additionally, the height (h) of the cone is measured. Finally, the tangent of the cone angle (α) is determined using Equation (6).where h is cone height and r is the average value of the four radii.
- -
- Powder flow (t″): This parameter, expressed in seconds and tenths of a second per 100 g of sample, was determined according to the method described in Section 2.9.16 of the Eur. Ph. [36]. The flowability was assessed by measuring the time required for a powder to flow through a standardized funnel. The equipment used included an ANORSA funnel (reference X7705), a metal stand with a clamp, and a stopwatch. The funnel’s orifice was initially sealed with paper, and 100 g of sample was poured into the funnel. Once filled, the paper plug was removed, and the time taken for the entire sample to flow through the funnel was recorded using the stopwatch. The procedure was repeated three times, and the average of the three measurements was reported as the result.
- -
- Loss on drying (%HR): This parameter is determined according to the method outlined in Section 2.2.32 in the Eur. Ph. [37]. The sample is dried in an oven at 105 °C ± 2 °C until a constant weight is obtained.
- -
- Hygroscopicity (%H): This parameter quantifies the percentage increase in sample weight after exposure to a humidifier set at a relative humidity of 76% (±2%) and a temperature of 22 °C ± 2 °C for 24 h.
- -
- Particle size < 50 mcm (%Pf): The percentage of fine particles (<50 µm) is determined using a sieve test following the general method 2.9.12 of the Eur. Ph. [38]. The reported value represents the percentage of particles that pass through a 0.05 mm sieve when vibrated for 10 min at speed 10 (CISA® vibrator).
- -
- Homogeneity index (Iθ): This index is calculated according to the general method 2.9.12 of the Eur. Ph. [38] for particle size determination by means of the sieve test. The grain size of a 100 g sample is measured by subjecting a sieve stack to vibration for 10 min at the speed of 10 (CISA vibrator). The percentage of product retained in each sieve is calculated, and the amount that passes through the 0.05 mm sieve is measured. The sieve sizes used are 0.355 mm, 0.212 mm, 0.100 mm, and 0.05 mm. Equation (7), described in previous works [10,11], is applied.where:
- Iθ: Relative homogeneity index. Particle size homogeneity in the range of the fractions studied.
- Fm: Percentage of particles in the majority range.
- Fm − 1: Percentage of particles in the range immediately below the majority range.
- Fm + 1: Percentage of particles in the range immediately above the majority range.
- n: Order number of the fraction studied under a series, with respect to the major fraction.
- dm: Mean diameter of the particles in the major fraction.
- dm − 1: Mean diameter of the particles in the fraction of the range immediately below the majority range.
- dm + 1: Mean diameter of the particles in the fraction of the range immediately above the majority range.
- -
- Parametric profile index (IPP). This index represents the mean value of all calculated parameters, with an acceptability limit set at r ≥ 5.
- -
- Good compression index (IGC). This index is calculated from Equation (8), where f is the reliability factor, determined by the ratio of polygon area to circle area. A GCI value greater than 5 is necessary to permit direct compression processing.where IPP is the parametric profile index and f is the reliability limit for IPP would be equal to or higher than 5. f can be calculated by using Equation (9).
2.2.5. Formulation Design Under the SeDeM Perspective
2.2.6. Blends Preparation
2.2.7. Tablet Preparation
2.2.8. Tablet Characterization
2.2.9. Product Characterization: Initial Risk Assessment
3. Results and Discussion
3.1. Carbamazepine Characterization
3.2. Excipient Characterization
3.3. Compressibility Approach
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tolou-Ghamari, Z.; Zare, M.; Habibabadi, J.M.; Najafi, M.R. A quick review of carbamazepine pharmacokinetics in epilepsy from 1953 to 2012. J. Res. Med. Sci. 2013, 18, S81–S85. [Google Scholar] [PubMed]
- Canadell-Heredia, R.; Suñé-Pou, M.; Nardi-Ricart, A.; Pérez-Lozano, P.; Suñé-Negre, J.; García-Montoya, E. Formulation and development of paediatric orally disintegrating carbamazepine tablets. Saudi Pharm. J. 2022, 30, 1612–1622. [Google Scholar] [CrossRef] [PubMed]
- NICE (National Institute For health and Care Excellence UK). 2012 Clinical Guideline (CG137). Epilepsies: Diagnosis and Management. Available online: https://www.nice.org.uk/guidance/cg137 (accessed on 15 January 2025).
- Ali, A.A.; Charoo, N.A.; Abdallah, D.B. Pediatric drug development: Formulation considerations. Drug Dev. Ind. Pharm. 2014, 40, 1283–1299. [Google Scholar] [CrossRef] [PubMed]
- Mistry, P.; Batchelor, H.; SPaeDD-UK project (Smart Paediatric Drug Development-UK). Evidence of acceptability of oral paediatric medicines: A review. J. Pharm. Pharmacol. 2017, 69, 361–376. [Google Scholar] [CrossRef]
- WHO. Carbamazepine in Childhood Epilepsy. October 2006; pp. 1–13. Available online: https://es.scribd.com/document/357200264/Carbamazepin (accessed on 11 December 2024).
- Comoglu, T.; Dilek Ozyilmaz, E. Orally disintegrating tablets and orally disintegrating mini tablets–novel dosage forms for pediatric use. Pharm. Dev. Technol. 2019, 24, 902–914. [Google Scholar] [CrossRef]
- Canadell-Heredia, R. Desarrollo de Comprimidos Bucodispersables de Carbamazepine de Uso Pediátrico. Ph. D. Thesis, University of Barcelona, Barcelona, Spain, 2023. [Google Scholar]
- Food and Drug Administration. Anticonvulsant Medications: U.S FDA Administration-Approved Indications and Dosages for Use in Pediatric Patients. 2015. Available online: https://www.cms.gov/medicare-medicaid-coordination/fraud-prevention/medicaid-integrity-education/pharmacy-education-materials/downloads/ac-pediatric-factsheet11-14.pdf (accessed on 12 February 2025).
- Gunda, R.K.; Kumar, J.N.S.; Satyanarayana, V.; Batta, S.; Harika, C.M. Formulation development and evaluation of Carbamazepine fast dissolving tablets. J. Pharm. Res. 2016, 10, 216–225. [Google Scholar]
- Comoglu, T. Formulation and Evaluation of Carbamazepine Fast Disintegrating Tablets. Pharm. Ind. 2010, 72, 150–158. [Google Scholar]
- Negre, J.M.S.; Carreras, M.R.; García, R.F.; Pérez, C.H.; Roura, R.R.; Montoya, E.G.; Carmona, M.M.; Lozano, P.P.; Grau, J.R.T. Nueva metodología de preformulación galénica para la caracterización de sustanciasen relacióna su viabilidad para la compresión: Diagrama SeDeM. Cienc. Tecnol. Pharm. 2005, 15, 125–136. [Google Scholar]
- Perez-Lozano, P.; Suñe-Negre, J.M.; Miñarro, M.; Roig, M.; Fuster, R.; García-Montoya, E.; Hernández, C.; Ruhi, R.; Ticó, J.R. A new expert system (SeDeM Diagram) for control batch powder formulation and preformulation drug products. Eur. J. Pharm. Biopharm. 2006, 64, 351–359. [Google Scholar] [CrossRef]
- Aguilar-Díaz, J.; García-Montoya, E.; Pérez-Lozano, P.; Suñé-Negre, J.M.; Miñarro, M.; Ticó, J.R. SeDeM expert system a new innovator tool to develop pharmaceutical forms. Drug Dev. Ind. Pharm. 2014, 40, 363–9045. [Google Scholar] [CrossRef]
- Suñé-Negre, J.M.; Pérez-Lozano, P.; Roig, M.; Fuster, R.; Hernández, C.; Ruhí, R.; García-Montoya, E.; Miñarro, M.; Ticó, J.R. Optimization of parameters of the SeDeM Diagram Expert System: Hausner index (IH) and relative humidity (%RH). Eur. J. Pharm. Biopharm. 2011, 79, 464–472. [Google Scholar] [CrossRef] [PubMed]
- Aguilar-Díaz, J.E.; García-Montoya, E.; Pérez-Lozano, P.; Suñe-Negre, J.M.; Miñarro, M.; Ticó, J.R. The use of the SeDeM Diagram expert system to determine the suitability of diluents–disintegrants for direct compression and their use in formulation of ODT. Eur. J. Pharm. Biopharm. 2009, 73, 414–423. [Google Scholar] [CrossRef]
- Suñe-Negre, J.M.; Perez-Lozano, P.; Miñarro, M.; Roig, M.; Fuster, R.; Hernández, C.; Ruhí, R.; García-Montoya, E.; Ticó, J.R. Application of the SeDeM Diagram and a new mathematical equation in the design of direct compression tablet formulation. Eur. J. Pharm. Biopharm. 2008, 69, 1029–1039. [Google Scholar] [CrossRef] [PubMed]
- Swamy, P.V.; Shahidulla, S.M.; Shirsand, S.B.; Hiremath, S.N.; Ali, Y. Orodispersible tablets of Carbamazepine prepared by direct compression method using 32 full factorial design. J. Pharm. Sci. 2008, 7, 1–5. [Google Scholar]
- Comoglu, T.; Dogan, A.; Comoglu, S.; Basci, N. Formulation and Evaluation of Diclofenac Potassium Fast Disintegrating Tablets and Their Clinical Application in Migraine Patients. Drug Dev. Ind. Pharm. 2011, 37, 260–267. [Google Scholar] [CrossRef]
- Perissutti, B.; Rubessa, F.; Moneghini, M.; Voinovich, D. Formulation Design of Carbamazepine Fast-Release Tablets Prepared by Melt Granulation Technique. Int. J. Pharm. 2003, 256, 53–56. [Google Scholar] [CrossRef]
- Mishra, S.M.; Rohera, B.D. An integrated, quality by design (QbD) approach for design, development and optimization of orally disintegrating tablet formulation of carbamazepine. Pharm. Dev. Technol. 2017, 22, 889–903. [Google Scholar] [CrossRef]
- Suñé-Negre, J.M.; Roig, M.; Fuster, R.; Hernández, C.; Ruhí, R.; García-Montoya, E.; Pérez-Lozano, P.; Miñarro, M.; Ticó, J.R. New classification of directly compressible (DC) excipients in function of the SeDeM Diagarm Expert System. Int. J. Pharm. 2014, 470, 15–27. [Google Scholar] [CrossRef]
- Aguilar-Díaz, J.E.; García-Montoya, E.; Suñe-Negre, J.M.; Pérez-Lozano, P.; Miñarro, M.; Ticó, J.R. Predicting orally disintegrating tablets formulations of ibuprophen tablets: An application of the new SeDeM-ODT expert system. Eur. J. Pharm. Biopharm. 2012, 80, 638–648. [Google Scholar] [CrossRef]
- Saurí, J.; Millán, D.; Suñé-Negre, J.M.; Pérez-Lozano, P.; Sarrate, R.; Fàbregas, A.; Carrillo, C.; Miñarro, M.; Ticó, J.R.; García-Montoya, E. The use of the SeDeM diagram expert system for the formulation of Captopril SR matrix tablets by direct compression. Int. J. Pharm. 2014, 461, 38–45. [Google Scholar] [CrossRef]
- Suñe-Negre, J.; García Montoya, E.; Perez-Lozano, P.; Edward Aguilar-Díaz, J.; Roig, M.; Fuster, R.; Miñarro, M.; Ticó, J. SeDeM Diagram: A New Expert System for the Formulation of drugs in Solid form. In Expert System for Human, Materials and Automation; InTechOpen: Rijeka, Croatia, 2011; pp. 17–34. [Google Scholar]
- Suñe Negre, J.; Roig, M.; Fuster, R.; García Montoya, E.; Perez-Lozano, P.; Edward Aguilar-Díaz, J.; Miñarro, M.; Ticó Grau, J. SeDeM Diagram: An expert system for preformulation, characterization and optimization of tablets obtained for direct compression. In Formulation Tools for Pharmaceutical Development; Woodhead Publishing: Cambridge, UK, 2013; pp. 109–135. [Google Scholar]
- Aguilar, J.E.; García-Montoya, E.; Pérez-Lozano, P.; Suñé-Negre, J.M.; Miñarro-Carmona, M.; Ticó-Grau, J.R. New SeDeM-ODT expert system: An expert system for formulation of orodispersible tablets obtained by direct compression. In Formulation Tools for Pharmaceutical Development; Woodhead Publishing: Sawston, UK, 2013; pp. 137–154. [Google Scholar] [CrossRef]
- Dai, S.; Xu, B.; Shi, G.; Liu, J.; Zhang, Z.; Shi, X.; Qiao, Y. SeDeM expert system for directly compressed tablet formulation: A review and new perspectives. Powder Technol. 2019, 342, 517–527. [Google Scholar] [CrossRef]
- Roque, F. Paediatric Medicines: Formulation Considerations. Arch. Pharm. Pharm. Sci. 2017, 1, 24–27. [Google Scholar]
- Rietnales, D.A.V.; Kozarewicz, P.; Aylward, B.; Vries, R.D.; Egberts, T.C.G.; Rademaker, C.M.A.; Schobben, A.F.A.M. Paediatric Drug Development and Formulation Design—A European Perspective. AAPS PharmSciTech. 2017, 18, 241–249. [Google Scholar] [PubMed]
- EMA; CHMP; ICH. ICH Q8 (R2) Pharmaceutical Development. 2014. Available online: https://www.ema.europa.eu/en/ich-q8-r2-pharmaceutical-development-scientific-guideline (accessed on 12 February 2025).
- EMA; CHMP; ICH. ICH Q9 Quality Risk Management. 2023. Available online: https://www.ema.europa.eu/en/ich-q9-quality-risk-management-scientific-guideline (accessed on 13 February 2025).
- European Pharmacopoeia 11.3. 2.9.31. Particle Size Analysis by Laser Light Diffraction. 2019. Available online: https://pheur.edqm.eu/app/11-2/content/11-2/20931E.htm?highlight=on&terms=particle&terms=particle-size%20distribution&terms=distribution&terms=particle%20size&terms=size%20distribution&terms=size&terms=particle-size (accessed on 14 March 2025).
- European Pharmacopoeia 11.3. 2.9.34. Bulk Density and Tapped Density of Powders. 2019. Available online: https://pheur.edqm.eu/app/11-3/content/default/20934E.htm (accessed on 14 March 2025).
- European Pharmacopoeia 11.2. 2.9.36. Powder Flow. Available online: https://pheur.edqm.eu/app/11-2/content/default/20936E.htm (accessed on 14 March 2025).
- European Pharmacopoeia 11.2. 2.9.16. Flowability. 2008. Available online: https://pheur.edqm.eu/app/11-2/content/default/20916E.htm (accessed on 23 March 2025).
- European Pharmacopoeia 11.3. 2.2.32. Loss on Drying. 2019. Available online: https://pheur.edqm.eu/app/11-3/content/default/20232E.htm (accessed on 23 March 2025).
- European Pharmacopoeia 11.3. 2.9.12. Sieve Test. 2022. Available online: https://pheur.edqm.eu/app/11-3/content/default/20912E.htm (accessed on 12 March 2025).
- Hamman, H.; Hamman, J.; Wessels, A.; Scholtz, J.; Steenekamp, J. Development of multiple-unit pellet system tablets by employing the SeDeMexpert diagram system II: Pellets containing different active pharmaceutical ingredients. Pharm. Dev. Technol. 2018, 24, 1–12. [Google Scholar]
- Rowe, R.C.; Sheskey, P.J.; Owen, S.C. Handbook of Pharmaceutical Excipients, 6th ed.; Pharmaceutical Press: London, UK, 2006. [Google Scholar]
- European Pharmacopoeia 11.3. 2.9.5. Uniformity of Mass of Single-dose Preparations. 2023. Available online: https://pheur.edqm.eu/app/11-3/content/default/20905E.htm (accessed on 12 February 2025).
- European Pharmacopoeia 11.3. 2.9.8. Resistance to Crushing of Tablets. 2008. Available online: https://pheur.edqm.eu/app/11-3/content/default/20908E.htm (accessed on 14 February 2025).
- European Pharmacopoeia 11.3. 2.9.7. Friability of Uncoated Tablets. 2024. Available online: https://pheur.edqm.eu/app/11-3/content/default/20907E.htm (accessed on 15 February 2025).
- European Pharmacopoeia 11.3. 2.9.1. Disintegration of Tablets and Capsules. 2022. Available online: https://pheur.edqm.eu/app/11-3/content/default/20901E.htm (accessed on 17 February 2025).
- Database Drugs.com. Carbamazepine Dosage. Available online: www.drugs.com/dosage/carbamazepine.html (accessed on 15 January 2019).
- Yu, L.X.; Amidon, G.; Khan, M.A.; Hoag, S.W.; Polli, J.; Raju, G.K.; Woodcock, J. Understanding Pharmaceutical Quality by Design. AAPS J. 2014, 16, 771–783. [Google Scholar] [CrossRef]
- Yu, L.X. Pharmaceutical quality by design: Product and process development, understanding, and control. Pharm. Res. 2007, 25, 781–791. [Google Scholar] [CrossRef]
- Yu, L.X.; Lionberger, R.; Olson, M.C.; Johnston, G.; Buehler, G.; Winkle, H. Quality by design for generic drugs. Pharm. Technol. 2009, 33, 122–127. [Google Scholar]
- Lionberger, R.A.; Lee, S.L.; Lee, L.; Raw, A.; Yu, L.X. Quality by design: Concepts for ANDAs. AAPS J. 2008, 10, 268–276. [Google Scholar] [CrossRef]
- Zhang, L.; Mao, S. Application of quality by design in the current drug development. Asian J. Pharm. Sci. 2017, 12, 1–8. [Google Scholar] [CrossRef]
- Khatri, S.; Saini, S.; Gurubalaji, G.K.; Gangawat, K. Pharmaceutical QbD: Concepts for Drug Product Development. Int. J. Pharm. Sci. Rev. Res. 2014, 26, 84–91. [Google Scholar]
- Wadke, D.A.; Serajuddin, A.T.M.; Jacobson, H. Preformulation testing. In Pharmaceutical Dosage Forms–Tablets; Routledge: London, UK, 1989; Volume 1, pp. 1–73. [Google Scholar]
- FDA, (Food and Drug Administration). Draft guidance for industry. ANDAs Pharm. Solid. Polymorphism. Chem. Manuf. Control. Inf. 2005, 2, 264–269. [Google Scholar]
- ICH. ICH Harmonised Tripartite Guideline, Pharmaceutical Development Q8 (R2). ICH Harmon Tripart Guid. 2009, 8, 1–28. [Google Scholar]
- Snider, D.A.; Addicks, W.; Owens, W. Polymorphism in generic drug product development. Adv. Drug Deliv. 2004, 56, 391–395. [Google Scholar] [CrossRef] [PubMed]
- Raw, A.S.; Furness, M.S.; Gill, D.S.; Adams, R.C.; Holcombe, F.O.; Yu, L.X. Regulatory considerations of pharmaceutical solid polymorphism in Abbreviated New Drug Applications (ANDAs). Adv. Drug Deliv. Rev. 2004, 56, 397–414. [Google Scholar] [CrossRef]
- Censi, R.; Di Martino, P. Polymorph impact on the bioavailability and stability of poorly soluble drugs. Molecules 2015, 20, 18759–18776. [Google Scholar] [CrossRef]
- Grzesiak, A.L.; Lang, M.; Kim, K.; Matzger, A.J. Comparision of the four anhydrous polymorphs of carbamazepine and the crystal structure of form I. J. Pharm. Sci. 2003, 92, 2260–2271. [Google Scholar] [CrossRef]
- Campiñez, M.D.; Casas, M.; Caraballo, I. Characterization of the Ability of Carbamazepine for Processing It through Direct Compression Applying the New Expert System SeDeM. Int. J. Clin. Pharmacol. Pharmacother. 2016, 1, 105. [Google Scholar] [CrossRef]
- Rowe, R.C.; Sheskey, P.J.; Quinn, M.E. Handbook of Pharmaceutical Excipients, 7th ed.; Rowe, R.C., Sheskey, P.J., Quinn, M.E., Eds.; Pharmaceutical Press: London, UK, 2009; ISBN 978-0-85369-792-3. [Google Scholar]
- Sipos, E.; Oltean, A.R.; Szabó, Z.-I.; Rédai, E.-M.; Nagy, G.D. Application of SeDeM expert systems in preformulation studies of pediatric ibuprofen ODT tablets. Acta Pharm. 2017, 67, 237–246. [Google Scholar] [CrossRef]
- Jung, D.E.; Yu, R.; Yoon, J.-R.; Eun, B.-L.; Kwon, S.-H.; Lee, Y.-J.; Eun, S.-H.; Lee, J.-S.; Kim, H.-D.; Nam, S.-O.; et al. Neuropsychological effects of levetiracetam and carbamazepine in children with focal epilepsy. Neurol. J. 2015, 84, 2312–2319. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Components | Percentage (%) |
|---|---|
| Talc | 2.36 |
| Aerosil® 200 | 0.14 |
| Magnesium stearate | 1.00 |
| Parameter | Symbol | Unit | Equation | Acceptable Ranges | Equation to Convert Values to SeDeM Radius Values |
|---|---|---|---|---|---|
| Bulk density | Da | g/mL | Da = m/V0 | 0–1 | 10 v |
| Tapped density | Dc | g/mL | Dc = m/V1250 Dc = m/V2500 | 0–1 | 10 v |
| Interparticle porosity | Ie | - | Ie = (Dc – Dc)/(Dc × Da) | 0–1.2 | 10 v/1.2 |
| Carr index | IC | % | IC = ((Dc − Da)/Dc) × 100 | 0–50 | v/5 |
| Cohesion index | Icd | N | Experimental | 0–200 | v/20 |
| Hausner index | IH | - | IH = Dc/Da | 3–1 | (30–10 v)/2 |
| Angle of repose | α | ° | Experimental | 50–0 | 10–(v/5) |
| Powder flow | t″ | s | Experimental | 20–0 | 10–(v/2) |
| Loss on drying | %HR | % | Experimental | 10–0 | 10-v |
| Hygroscopicity | %H | % | Experimental | 20–0 | 10–(v/2) |
| Particles < 50 µm | %Pf | µ | Experimental | 50–0 | 10–(v/5) |
| Homogeneity index | Iϴ | - | Iϴ = Fm/(100 + ΔFmn) | 0–0.02 | 500 v |
| Mixture | Components | Percentage for Compressibility Radius 5.0 | Percentage for Compressibility Radius 4.5 | Percentage for Compressibility Radius 4.0 | Percentage for Compressibility Radius 3.5 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| F1 | F2 | F3 | F4 | F5 | F6 | F7 | F8 | F9 | F10 | F11 | F12 | F13 | F14 | F15 | F16 | ||
| Mixture 1 | Carbamazepine | 26.70 | 28.97 | 7.23 | 20.59 | 43.48 | 45.20 | 28.69 | 38.84 | 60.26 | 61.44 | 50.15 | 57.08 | 77.04 | 77.67 | 71.61 | 75.33 |
| L-HPC LH11 | 69.80 | - | - | - | 53.02 | - | - | - | 36.24 | - | - | - | 19.46 | - | - | - | |
| L-HPC NBD022 | - | 67.53 | - | - | - | 51.30 | - | - | - | 35.06 | - | - | - | 18.83 | - | - | |
| PARTECK® ODT | - | - | 89.27 | - | - | - | 67.81 | - | - | - | 46.35 | - | - | - | 24.89 | - | |
| PROSOLV® ODT | - | - | - | 75.91 | - | - | - | 57.66 | - | - | - | 39.42 | - | - | - | 21.17 | |
| Talc | 2.36 | 2.36 | 2.36 | 2.36 | 2.36 | 2.36 | 2.36 | 2.36 | 2.36 | 2.36 | 2.36 | 2.36 | 2.36 | 2.36 | 2.36 | 2.36 | |
| Aerosil® | 0.14 | 0.14 | 0.14 | 0.14 | 0.14 | 0.14 | 0.14 | 0.14 | 0.14 | 0.14 | 0.14 | 0.14 | 0.14 | 0.14 | 0.14 | 0.14 | |
| Mixture 2 | Magnesium stearate | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| QTPP Elements | Target |
|---|---|
| Dosage form | Orally disintegrating tablets |
| Route of administration | Oral |
| Dosage strength | 50 mg |
| Shape | Tablet diameter < 7 mm |
| Disintegration time | Not more than 3 min |
| Pediatric population | Aged 6 years or older |
| CQA | Polymorph (Shape) | Particle Size (Distribution) | Moisture | Disintegrant | Lubricant |
|---|---|---|---|---|---|
| Blend | |||||
| Flow | M | H | L | H | H |
| Compression | |||||
| Hardness | H | M | L | H | M |
| Friability | H | M | L | H | M |
| Disintegration | L | L | L | H | L |
| Final risk | H | M | L | H | M |
| Carbamazepine | L-HPC L-H11 | L-HPC NBD022 | PARTECK® ODT | PROSOLV® ODT | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Incidence Factor | Parameter | Symbol | Units | Radius Value | Incidence | Radius Value | Incidence | Radius Value | Incidence | Radius Value | Incidence | Radius Value | Incidence |
| Dimensions | Bulk density | Da | g/mL | 5.84 | 6.44 | 3.84 | 4.68 | 3.52 | 4.52 | 5.28 | 5.74 | 6.19 | 7.01 |
| Tapped density | Dc | g/mL | 7.02 | 5.52 | 5.51 | 6.20 | 7.82 | ||||||
| Compressibility | Interparticle porosity | Ie | - | 2.39 | 2.92 | 6.61 | 5.90 | 8.55 | 6.00 | 2.34 | 4.91 | 2.81 | 5.66 |
| Carr index | IC | % | 3.36 | 6.09 | 7.22 | 2.97 | 4.17 | ||||||
| Cohesion index | Icd | N | 3.00 | 4.99 | 2.22 | 9.42 | 10.00 | ||||||
| Flowability/Powder flow | Hausner index | IH | - | 8.99 | 7.28 | 7.81 | 3.00 | 7.18 | 3.42 | 9.13 | 7.30 | 8.69 | 7.26 |
| Angle of repose | α | ° | 4.69 | 1.19 | 3.10 | 4.60 | 5.09 | ||||||
| Powder flow | t | s | 8.17 | 0.00 | 0.00 | 8.17 | 8.00 | ||||||
| Lubricity/Stability | Loss on drying | %HR | % | 9.67 | 9.81 | 3.10 | 4.93 | 6.02 | 4.95 | 8.12 | 8.90 | 6.18 | 7.98 |
| Hygroscopicity | %H | % | 9.95 | 4.77 | 3.89 | 9.69 | 9.78 | ||||||
| Lubricity/Dosage | Particles < 50 µm | %Pf | µ | 7.80 | 4.53 | 0.00 | 3.00 | 0.00 | 3.83 | 7.40 | 4.63 | 2.57 | 3.66 |
| Homogeneity index | Iϴ | - | 1.25 | 6.00 | 7.65 | 1.85 | 4.75 | ||||||
| Good compression index (IGC) | 5.72 | 4.12 | 4.35 | 5.96 | 6.03 | ||||||||
| Target Radius | Formulation | Mean Weight (mg) | Mean Hardness (N) | Tablet Diameter (mm) |
|---|---|---|---|---|
| 5 | F1 | 187.6 | 147.7 | 9 |
| F2 | 172.9 | 159.9 | 9 | |
| F3 | 697.6 | 331.8 | 13 | |
| F4 | 250.0 | 230.5 | 9 | |
| 4.5 | F5 | 160.9 | 121.9 | 8 |
| F6 | 112.0 | 113.4 | 8 | |
| F7 | 172.7 | 48.0 | 8 | |
| F8 | 131.3 | 78.3 | 8 | |
| 4.0 | F9 | 83.0 | 77.0 | 6 |
| F10 | 82.7 | 73.2 | 6 | |
| F11 | 101.5 | 55.4 | 6 | |
| F12 | 88.4 | 21.2 | 6 | |
| 3.5 | F13 | 67.0 | 62.5 | 5 |
| F14 | 62.8 | 24.8 | 5 | |
| F15 | 69.9 | 27.6 | 5 | |
| F16 | 68.1 | 37.4 | 5 |
| Formula | Hausner Ratio | Mean Hardness (N) | Friability (%) | Disintegration (s) | Tablet Diameter (mm) |
|---|---|---|---|---|---|
| F13 | 1.36 | 62.5 | 0.89 | 50 | 5 |
| F14 | 1.32 | 24.8 | 0.38 | 45 | 5 |
| F15 | 1.19 | 27.6 | 0.89 | 103 | 5 |
| F16 | 1.23 | 37.4 | 1.00 | 420 | 5 |
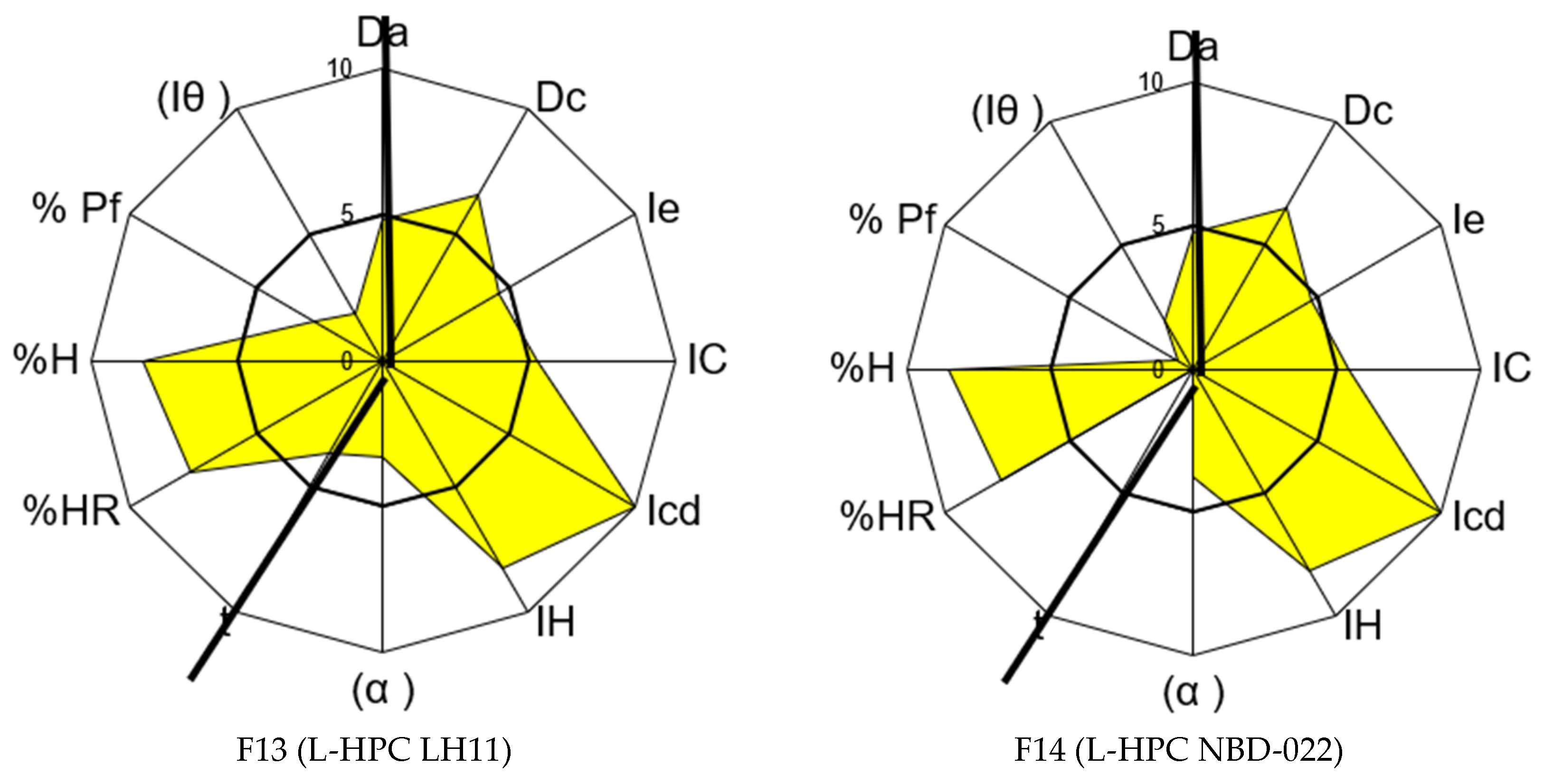
| Formulation 13 | Formulation 14 | ||||||
|---|---|---|---|---|---|---|---|
| Incidence factor | Parameter | Symbol | Units | Radius Value | Incidence | Radius Value | Incidence |
| Dimensions | Bulk density | Da | g/mL | 4.84 | 5.72 | 4.73 | 5.61 |
| Tapped density | Dc | g/mL | 6.59 | 6.49 | |||
| Compressibility | Interparticle porosity | Ie | - | 4.58 | 6.63 | 4.78 | 6.73 |
| Carr index | IC | % | 5.31 | 5.42 | |||
| Cohesion index | Icd | N | 10.00 | 10.00 | |||
| Flowability/Powder flow | Hausner index | IH | - | 8.19 | 5.05 | 8.14 | 3.97 |
| Angle of repose | (α) | ° | 3.30 | 3.76 | |||
| Powder flow | t | s | 3.67 | 0.00 | |||
| Lubricity/Stability | Loss on drying | %HR | % | 7.63 | 7.94 | 7.77 | 8.16 |
| Hygroscopicity | %H | % | 8.24 | 8.55 | |||
| Lubricity/Dosage | Particles < 50 µm | %Pf | µ | 2.69 | 2.27 | 0.62 | 1.28 |
| Homogeneity index | Iϴ | - | 1.85 | 1.95 | |||
| Good compression Index | ICG | - | - | 5.31 | - | 4.94 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Canadell-Heredia, R.; Rouaz-El-Hajoui, K.; Franco-Piedrahita, N.; Pérez-Lozano, P.; Suñé-Pou, M.; Suñé-Negre, J.M.; García-Montoya, E. Preformulation Study of Carbamazepine Orally Disintegrating Tablets for Pediatric Patients Using Direct Compression and the SeDeM Diagram Tool: A Quality by Design Approach. Pharmaceutics 2025, 17, 624. https://doi.org/10.3390/pharmaceutics17050624
Canadell-Heredia R, Rouaz-El-Hajoui K, Franco-Piedrahita N, Pérez-Lozano P, Suñé-Pou M, Suñé-Negre JM, García-Montoya E. Preformulation Study of Carbamazepine Orally Disintegrating Tablets for Pediatric Patients Using Direct Compression and the SeDeM Diagram Tool: A Quality by Design Approach. Pharmaceutics. 2025; 17(5):624. https://doi.org/10.3390/pharmaceutics17050624
Chicago/Turabian StyleCanadell-Heredia, Ricard, Khadija Rouaz-El-Hajoui, Natalia Franco-Piedrahita, Pilar Pérez-Lozano, Marc Suñé-Pou, Josep María Suñé-Negre, and Encarna García-Montoya. 2025. "Preformulation Study of Carbamazepine Orally Disintegrating Tablets for Pediatric Patients Using Direct Compression and the SeDeM Diagram Tool: A Quality by Design Approach" Pharmaceutics 17, no. 5: 624. https://doi.org/10.3390/pharmaceutics17050624
APA StyleCanadell-Heredia, R., Rouaz-El-Hajoui, K., Franco-Piedrahita, N., Pérez-Lozano, P., Suñé-Pou, M., Suñé-Negre, J. M., & García-Montoya, E. (2025). Preformulation Study of Carbamazepine Orally Disintegrating Tablets for Pediatric Patients Using Direct Compression and the SeDeM Diagram Tool: A Quality by Design Approach. Pharmaceutics, 17(5), 624. https://doi.org/10.3390/pharmaceutics17050624