
Product Development of High-Dose Ambroxol HCl Capsules for an n-of-1 Clinical Trial Involving Dutch Patients with Gaucher Disease Type 3

 , , ,
, , ,
Abstract

1. Introduction
2. Materials and Methods
2.1. Raw Materials and Chemicals
2.2. Production of Validation Batches AMB Capsules
2.3. Product Specifications
2.4. Analytical Methods
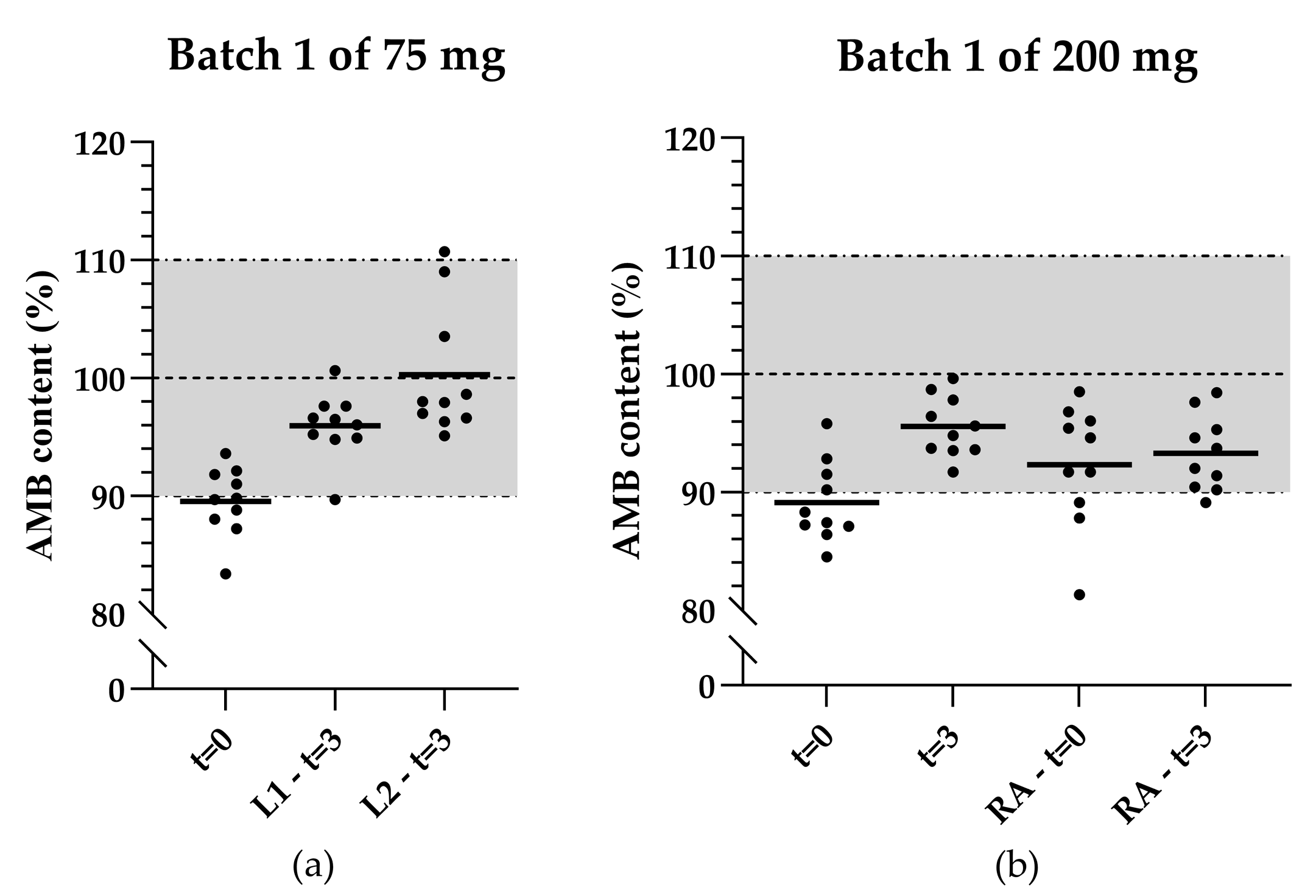
2.5. Stability Study
2.6. Out-of-Expectiation Investigation
2.6.1. Properties of AMB API
2.6.2. Error and Variations in Analytical Method
3. Results
3.1. In-Process Controls of the Produced AMB Formulations
3.1.1. The Initial Formulations
3.1.2. The Optimized Formulation
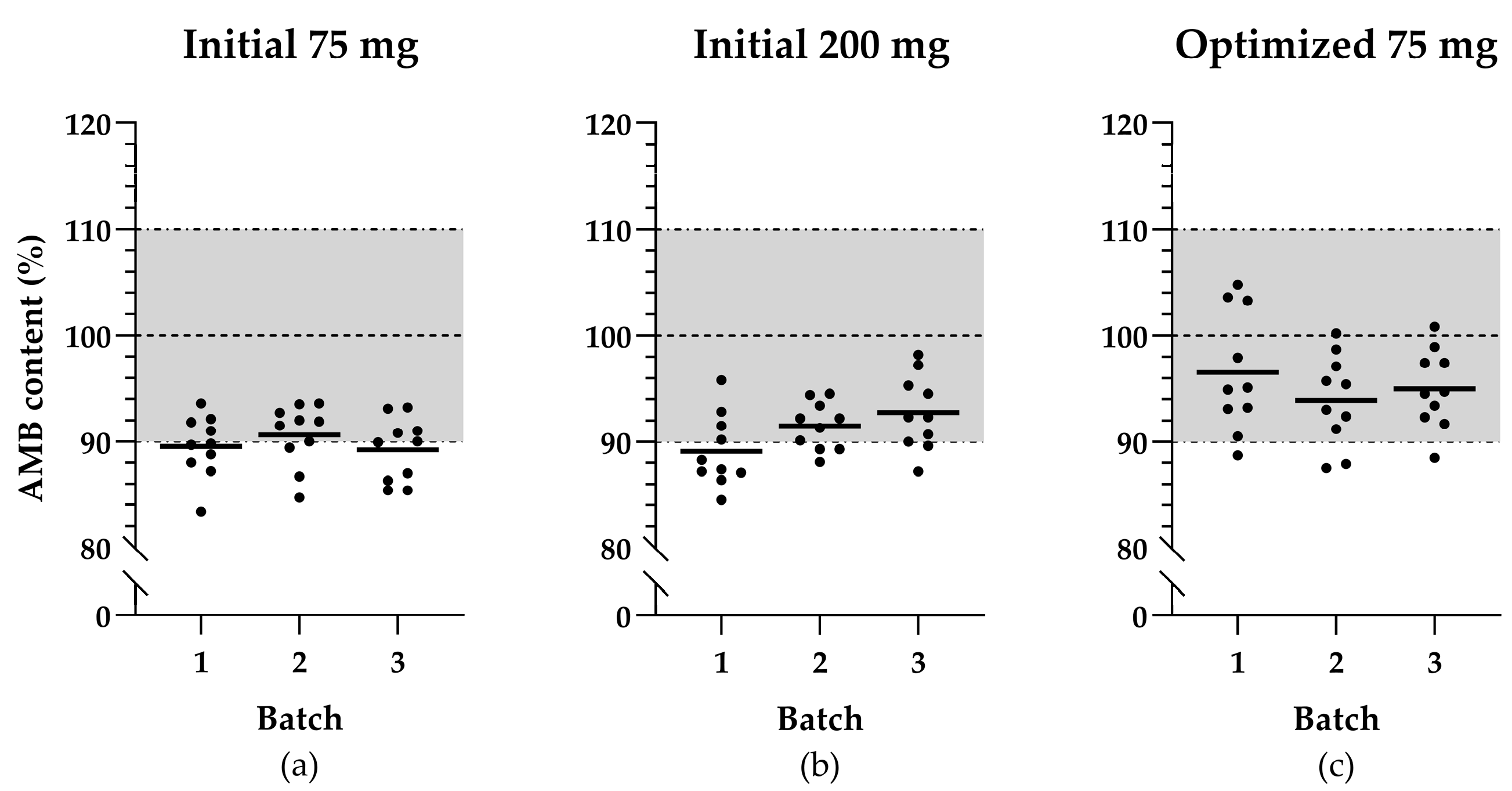
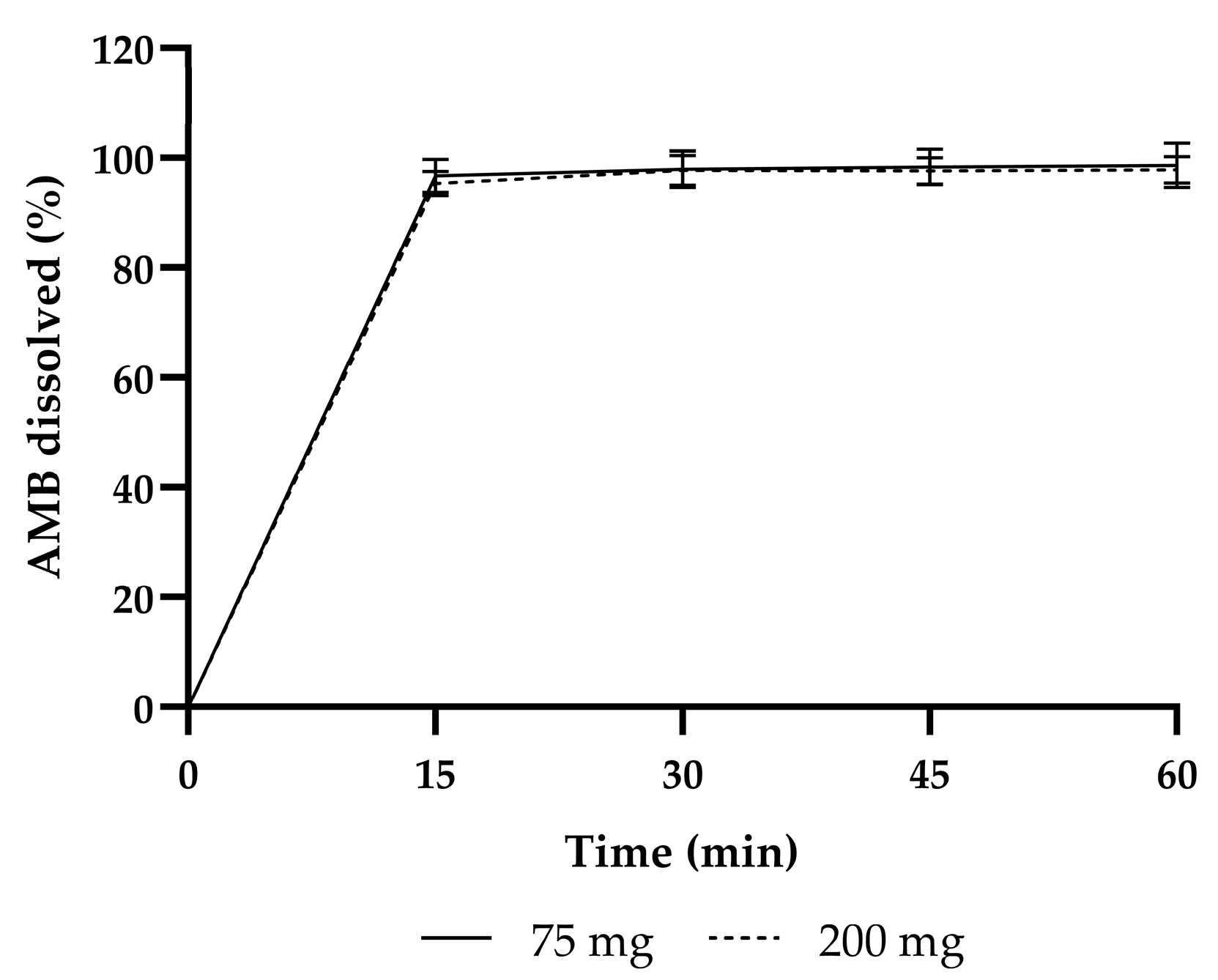
3.2. Product Validation
3.2.1. Product Validation of the Initial Formulations
3.2.2. Product Validation of the Optimized 75 mg Formulation
3.3. Out-of-Expectation Investigation
3.3.1. Hygroscopicity of AMB
3.3.2. Error and Variations in Analysis Method
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brady, R.O. Gaucher’s disease: Past, present and future. Baillieres Clin. Haematol. 1997, 10, 621–634. [Google Scholar] [CrossRef] [PubMed]
- Charrow, J.; Andersson, H.C.; Kaplan, P.; Kolodny, E.H.; Mistry, P.; Pastores, G.; Rosenbloom, B.E.; Scott, C.R.; Wappner, R.S.; Weinreb, N.J.; et al. The Gaucher registry: Demographics and disease characteristics of 1698 patients with Gaucher disease. Arch. Intern. Med. 2000, 160, 2835–2843. [Google Scholar] [CrossRef] [PubMed]
- Grabowski, G.A. Phenotype, diagnosis, and treatment of Gaucher’s disease. Lancet 2008, 372, 1263–1271. [Google Scholar] [CrossRef] [PubMed]
- Stirnemann, J.; Belmatoug, N.; Camou, F.; Serratrice, C.; Froissart, R.; Caillaud, C.; Levade, T.; Astudillo, L.; Serratrice, J.; Brassier, A.; et al. A Review of Gaucher Disease Pathophysiology, Clinical Presentation and Treatments. Int. J. Mol. Sci. 2017, 18, 441. [Google Scholar] [CrossRef] [PubMed]
- Leonart, L.P.; Fachi, M.M.; Böger, B.; Silva, M.R.D.; Szpak, R.; Lombardi, N.F.; Pedroso, M.L.A.; Pontarolo, R. A Systematic Review and Meta-analyses of Longitudinal Studies on Drug Treatments for Gaucher Disease. Ann. Pharmacother. 2023, 57, 267–282. [Google Scholar] [CrossRef] [PubMed]
- Roshan Lal, T.; Sidransky, E. The Spectrum of Neurological Manifestations Associated with Gaucher Disease. Diseases 2017, 5, 10. [Google Scholar] [CrossRef] [PubMed]
- Maegawa, G.H.; Tropak, M.B.; Buttner, J.D.; Rigat, B.A.; Fuller, M.; Pandit, D.; Tang, L.; Kornhaber, G.J.; Hamuro, Y.; Clarke, J.T.; et al. Identification and characterization of ambroxol as an enzyme enhancement agent for Gaucher disease. J. Biol. Chem. 2009, 284, 23502–23516. [Google Scholar] [CrossRef] [PubMed]
- Charkhand, B.; Scantlebury, M.H.; Narita, A.; Zimran, A.; Al-Hertani, W. Effect of Ambroxol chaperone therapy on Glucosylsphingosine (Lyso-Gb1) levels in two Canadian patients with type 3 Gaucher disease. Mol. Genet. Metab. Rep. 2019, 20, 100476. [Google Scholar] [CrossRef] [PubMed]
- Aries, C.; Lohmöller, B.; Tiede, S.; Täuber, K.; Hartmann, G.; Rudolph, C.; Muschol, N. Promising Effect of High Dose Ambroxol Treatment on Neurocognition and Motor Development in a Patient With Neuropathic Gaucher Disease 2. Front. Neurol. 2022, 13, 907317. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.M.; Yum, M.S.; Heo, S.H.; Kim, T.; Jin, H.K.; Bae, J.S.; Seo, G.H.; Oh, A.; Yoon, H.M.; Lim, H.T.; et al. Pharmacologic properties of high-dose ambroxol in four patients with Gaucher disease and myoclonic epilepsy. J. Med. Genet. 2020, 57, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Ramadža, D.P.; Zekušić, M.; Žigman, T.; Škaričić, A.; Bogdanić, A.; Mustać, G.; Bošnjak-Nađ, K.; Ozretić, D.; Ohno, K.; Fumić, K.; et al. Early initiation of ambroxol treatment diminishes neurological manifestations of type 3 Gaucher disease: A long-term outcome of two siblings. Eur. J. Paediatr. Neurol. 2021, 32, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Ciana, G.; Dardis, A.; Pavan, E.; Da Riol, R.M.; Biasizzo, J.; Ferino, D.; Zanatta, M.; Boni, A.; Antonini, L.; Crichiutti, G.; et al. In vitro and in vivo effects of Ambroxol chaperone therapy in two Italian patients affected by neuronopathic Gaucher disease and epilepsy. Mol. Genet. Metab. Rep. 2020, 25, 100678. [Google Scholar] [CrossRef] [PubMed]
- Chu, S.Y.; Chien, C.C.; Hwu, W.L.; Wang, P.J.; Chien, Y.H. Early initiation of high-dose oral ambroxol in combination with enzyme replacement therapy in a neuropathic Gaucher infant. Blood Cells Mol. Dis. 2020, 81, 102402. [Google Scholar] [CrossRef] [PubMed]
- Pawlinski, L.; Malecki, M.T.; Kiec-Wilk, B. The additive effect on the antiepileptic treatment of ambroxol in type 3 Gaucher patient. The early observation. Blood Cells Mol. Dis. 2018, 68, 192–193. [Google Scholar] [CrossRef] [PubMed]
- Narita, A.; Shirai, K.; Itamura, S.; Matsuda, A.; Ishihara, A.; Matsushita, K.; Fukuda, C.; Kubota, N.; Takayama, R.; Shigematsu, H.; et al. Ambroxol chaperone therapy for neuronopathic Gaucher disease: A pilot study. Ann. Clin. Transl. Neurol. 2016, 3, 200–215. [Google Scholar] [CrossRef] [PubMed]
- den Hollander, B.; Le, H.L.; Swart, E.L.; Bikker, H.; Hollak, C.E.M.; Brands, M.M. Clinical and preclinical insights into high-dose ambroxol therapy for Gaucher disease type 2 and 3: A comprehensive systematic review. Mol. Genet. Metab. 2024, 143, 108556. [Google Scholar] [CrossRef] [PubMed]
- Zorginstituut Nederland. Farmacotherapeutisch Kompas: Ambroxol. Available online: https://www.farmacotherapeutischkompas.nl/bladeren/preparaatteksten/a/ambroxol (accessed on 7 March 2025).
- European Pharmacopoeia Commission. Ambroxol Hydrochloride (1489), 11th ed.; Quality of Medicines & HealthCare of the Council of Europe (EDQM): Strasbourg, France, 2022. [Google Scholar]
- European Pharmacopoeia Commission. Colloidal Anhydrous Silica (0434), 11th ed.; Quality of Medicines & HealthCare of the Council of Europe (EDQM): Strasbourg, France, 2022. [Google Scholar]
- European Pharmacopoeia Commission. Lactose Monohydrate (0187), 11th ed.; Quality of Medicines & HealthCare of the Council of Europe (EDQM): Strasbourg, France, 2022. [Google Scholar]
- European Commission. Detailed Commission Guidelines on Good Manufacturing Practice for Investigational Medicinal Products for Human Use, Pursuant to the Second Subparagraph of Article 63(1) of Regulation (EU) No 526/2014. Available online: https://health.ec.europa.eu/document/download/a0b206a0-5788-406b-9e20-e0525b16e712_en?filename=guideline_adopted_1_en_act_part1_v3.pdf (accessed on 28 October 2024).
- KNMP. Capsules. Available online: https://kennisbank.knmp.nl/article/LNA-procedures_bereiding/Toedieningsvormen/capsulespoeders/B061.html (accessed on 18 October 2024).
- International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH). ICH Harmonised Tripartite Guideline: Specifications: Test Procedures and Acceptance Criteria for New Drug Substances and New Drug Products: Chemical Substances (Q6A). Available online: https://database.ich.org/sites/default/files/Q6A%20Guideline.pdf (accessed on 16 August 2024).
- European Pharmacopoeia Commission. Pharmaceutical Preparations (2619), 11th ed.; Quality of Medicines & HealthCare of the Council of Europe (EDQM): Strasbourg, France, 2022. [Google Scholar]
- European Pharmacopoeia Commission. Capsules (0016), 11th ed.; Quality of Medicines & HealthCare of the Council of Europe (EDQM): Strasbourg, France, 2022. [Google Scholar]
- Committee for Medicinal Products for Human Use (CHMP). Guideline on the Requirements for Chemical and Pharmaceutical Quality Documentation Concerning Investigational Medicinal Products in Clinical Trials. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-requirements-chemical-and-pharmaceutical-quality-documentation-concerning-investigational-medicinal-products-clinical-trials-revision-2_en.pdf (accessed on 24 October 2024).
- European Pharmacopoeia Commission. Appendix XII C: Consistency of Formulated Preparations (2.9.5), 11th ed.; Quality of Medicines & HealthCare of the Council of Europe (EDQM): Strasbourg, France, 2022. [Google Scholar]
- International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH). ICH Topic Q1A (R2) Stability Testing of New Drug Substances and Products. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/ich-q-1-r2-stability-testing-new-drug-substances-and-products-step-5_en.pdf (accessed on 18 October 2024).
- Ministerie van Algemene Zaken. Besluit Geneesmiddelenwet. Available online: https://wetten.overheid.nl/BWBR0021672/2018-08-01 (accessed on 16 August 2024).
- Oussoren, C.; Bolhuis, G. 26 Oraal vast. In Recepteerkunde: Product en Beereiding van Geneesmiddelen, 5th ed.; Bohn Stafleu van Loghum: Houten, The Netherlands, 2009; pp. 569–592. [Google Scholar]
- Cyske, Z.; Gaffke, L.; Rintz, E.; Wiśniewska, K.; Węgrzyn, G.; Pierzynowska, K. Molecular mechanisms of the ambroxol action in Gaucher disease and GBA1 mutation-associated Parkinson disease. Neurochem. Int. 2024, 178, 105774. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Initial Product Validation 75 mg | Initial Product Validation 200 mg | Optimized Product Validation 75 mg | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Tests | Acceptance Limit | Batch 1 | Batch 2 | Batch 3 | Batch 1 | Batch 2 | Batch 3 | Batch 1 | Batch 2 | Batch 3 |
| Identity | Complies | Complies | Complies | Complies | Complies | Complies | Complies | Complies | Complies | Complies |
Related substances (%)
| <0.1 <0.3 | <0.1 <0.3 | <0.1 <0.3 | <0.1 <0.3 | <0.1 <0.3 | <0.1 <0.3 | <0.1 <0.3 | <0.1 <0.3 | <0.1 <0.3 | <0.1 <0.3 |
| Mean content (% of labelled content) | 90–110% | 89.5 | 90.6 | 89.2 | 89.1 | 91.5 | 92.7 | 96.5 | 93.9 | 95.0 |
| Uniformity of dosage units (Content Uniformity) | AV ≤ 15.0 | 16.0 | 15.0 | 16.5 | 17.6 | 12.4 | 14.2 | 14.5 | 14.9 | 12.4 |
| Dissolution | ≥80% at 30 min | 100.5% | 97.2% | 96.0% | 96.5% | 99.4% | 97.3% | 95.0% | 99.5% | 96.3% |
Microbiology
| <103 CFU/g <102 CFU/g Absent | <10 <10 Absent | <10 <10 Absent | <10 <10 Absent | <10 <10 Absent | <10 <10 Absent | <10 <10 Absent | <10 <10 Absent | <10 <10 Absent | <10 <10 Absent |
| Dose | Batch | Batch Size Meeting IPC (Caps) | Number of Portions Failed IPC | Capsule Content * (mg) | Mean Weight Deviation * (%) (<±3.0%) | RSD * (%) (75 mg: <4.0% 200 mg: <3.0%) |
|---|---|---|---|---|---|---|
| 75 mg (initial) | 1 | 1400 | 0 | 222.6 ± 14.3 | −0.52 ± 0.70 | 2.23 ± 0.49 |
| 2 | 900 | 1 † | 206.7 ± 10.0 | −1.25 ± 0.59 | 2.38 ± 0.80 | |
| 3 | 800 | 2 † | 199.0 ± 5.0 | −0.14 ± 1.38 | 2.58 ± 0.33 | |
| 200 mg (initial) | 1 | 1100 | 3 † | 303.8 ± 9.6 | −1.19 ± 0.45 | 2.13 ± 0.30 |
| 2 | 800 | 1 † | 298.4 ± 3.6 | −1.37 ± 0.86 | 2.52 ± 0.41 | |
| 3 | 800 | 1 † | 328.0 ± 23.9 | −0.06 ± 1.21 | 1.56 ± 0.28 | |
| 75 mg (optimized) | 1 | 1000 | 0 | 259.1 ± 2.6 | −0.94 ± 1.00 | 2.37 ± 0.54 |
| 2 | 1000 | 0 | 262.9 ± 1.1 | −1.73 ± 0.53 | 1.64 ± 0.45 | |
| 3 | 1000 | 0 | 284.4 ± 1.8 | −1.94 ± 0.62 | 1.86 ± 0.41 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Le, H.L.; Bouwhuis, N.; Hollak, C.E.M.; Wilhelm, A.J.; Gerards, A.-L.E.; Bijleveld, Y.A.; Swart, E.L. Product Development of High-Dose Ambroxol HCl Capsules for an n-of-1 Clinical Trial Involving Dutch Patients with Gaucher Disease Type 3. Pharmaceutics 2025, 17, 417. https://doi.org/10.3390/pharmaceutics17040417
Le HL, Bouwhuis N, Hollak CEM, Wilhelm AJ, Gerards A-LE, Bijleveld YA, Swart EL. Product Development of High-Dose Ambroxol HCl Capsules for an n-of-1 Clinical Trial Involving Dutch Patients with Gaucher Disease Type 3. Pharmaceutics. 2025; 17(4):417. https://doi.org/10.3390/pharmaceutics17040417
Chicago/Turabian StyleLe, Hoang Lan, Natalja Bouwhuis, Carla E. M. Hollak, Abraham J. Wilhelm, Anne-Loes E. Gerards, Yuma A. Bijleveld, and Eleonora L. Swart. 2025. "Product Development of High-Dose Ambroxol HCl Capsules for an n-of-1 Clinical Trial Involving Dutch Patients with Gaucher Disease Type 3" Pharmaceutics 17, no. 4: 417. https://doi.org/10.3390/pharmaceutics17040417
APA StyleLe, H. L., Bouwhuis, N., Hollak, C. E. M., Wilhelm, A. J., Gerards, A.-L. E., Bijleveld, Y. A., & Swart, E. L. (2025). Product Development of High-Dose Ambroxol HCl Capsules for an n-of-1 Clinical Trial Involving Dutch Patients with Gaucher Disease Type 3. Pharmaceutics, 17(4), 417. https://doi.org/10.3390/pharmaceutics17040417