
Cytotoxic and Immunomodulatory Effects of Hypericin as a Photosensitizer in Photodynamic Therapy Used on Skin Cell Cultures

 , , ,
, , ,  ,
,  and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Chemicals
2.2. Cell Cultures
2.3. Fluorescence Microscopy
2.4. Photodynamic Therapy
2.5. MTT Assay
2.6. Cytokines Measurements
2.7. Statistical Analysis
3. Results
3.1. Fluorescence Microscopy
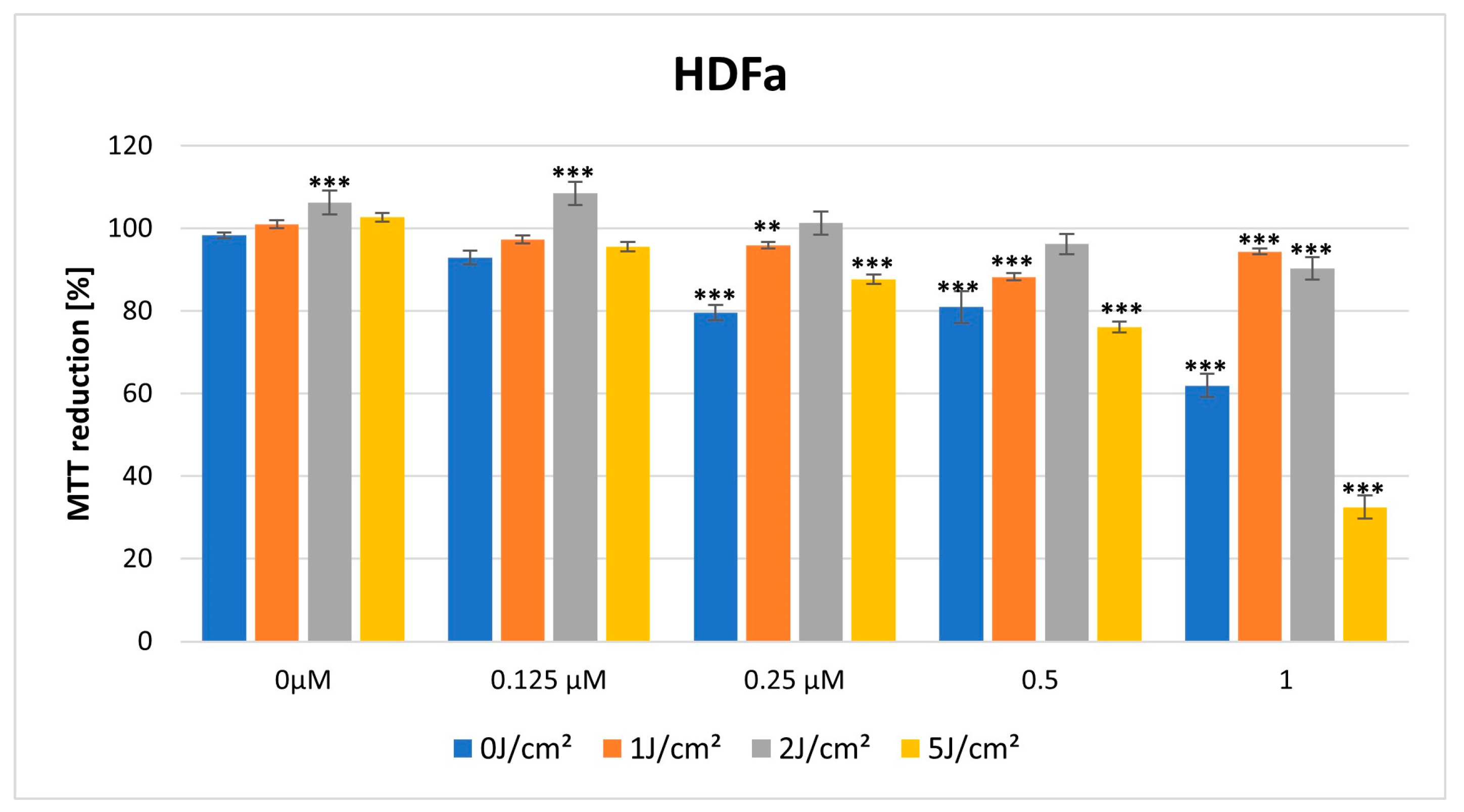
3.2. MTT Cytotoxicity Assay
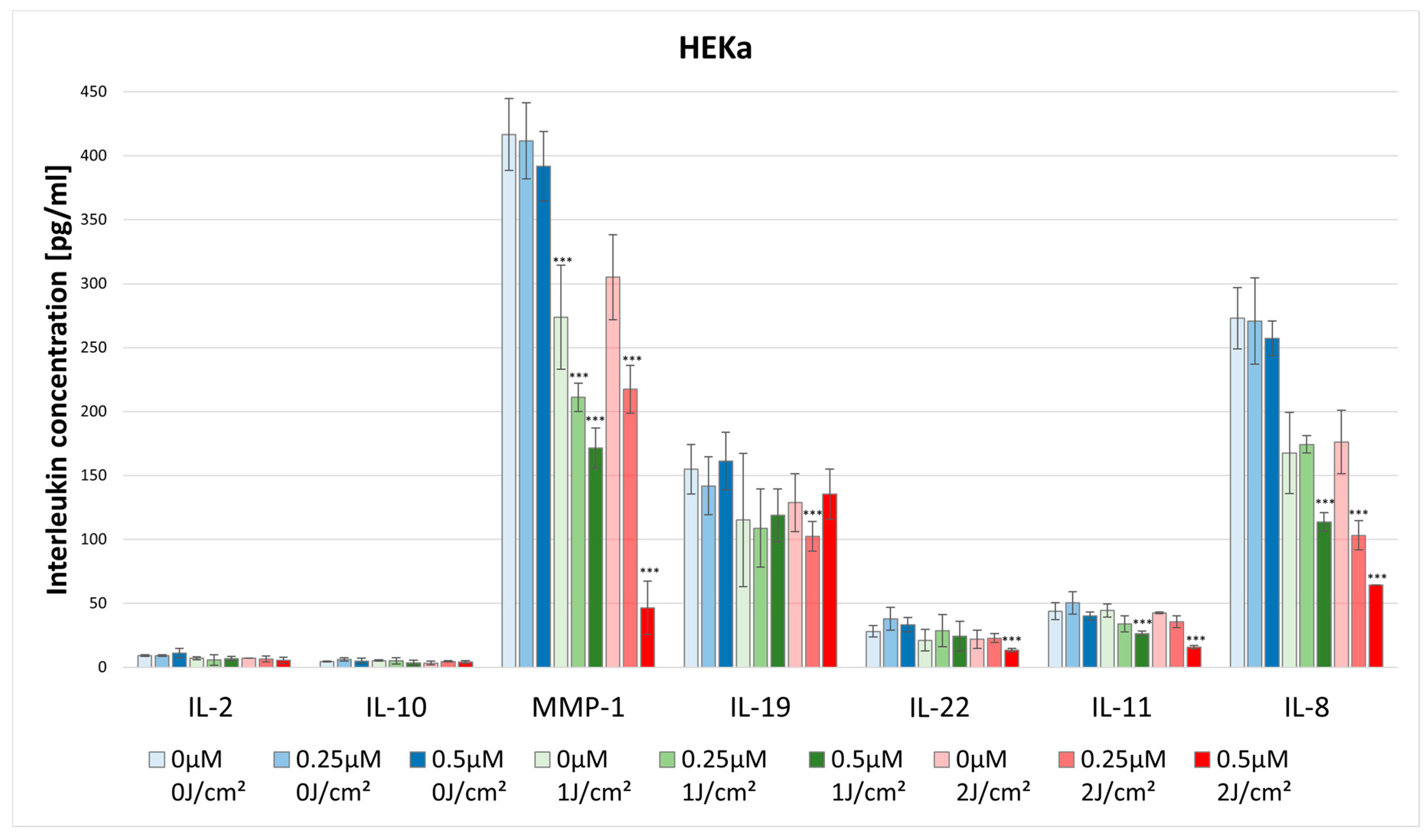
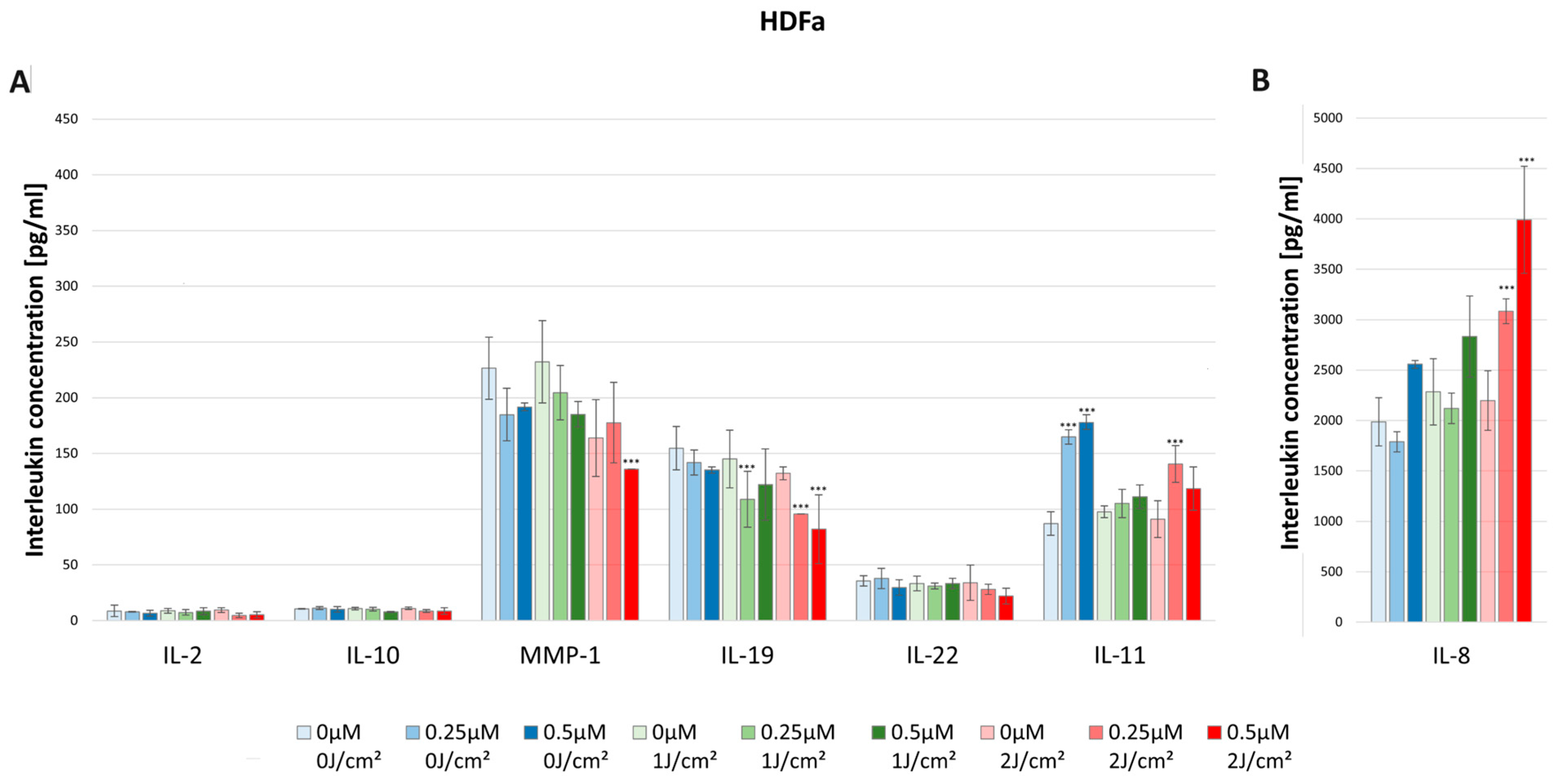
3.3. Effect of HY–PDT on the Secretory Activity of IL-2, IL-10, MMP-1, IL-19, IL-22, IL-11, and IL-8
3.3.1. IL-2
3.3.2. IL-8
3.3.3. IL-10
3.3.4. MMP-1
3.3.5. IL-19
3.3.6. IL-22
3.3.7. IL-11
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Agostinis, P.; Vantieghem, A.; Merlevede, W.; de Witte, P.A. Hypericin in cancer treatment: More light on the way. Int. J. Biochem. Cell Biol. 2002, 34, 221–241. [Google Scholar] [CrossRef] [PubMed]
- Theodossiou, T.A.; Hothersall, J.S.; De Witte, P.A.; Pantos, A.; Agostinis, P. The multifaceted photocytotoxic profile of hypericin. Mol. Pharm. 2009, 6, 1775–1789. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Gao, L.; Hu, J.; Wang, C.; Hagedoorn, P.L.; Li, N.; Zhou, X. Hypericin: Source, determination, separation, and properties. Sep. Purif. Rev. 2020, 51, 1–10. [Google Scholar] [CrossRef]
- Doroshenko, A.; Tomkova, S.; Kozar, T.; Stroffekova, K. Hypericin, a potential new BH3 mimetic. Front. Pharmacol. 2022, 13, 991554. [Google Scholar] [CrossRef] [PubMed]
- Kiesslich, T.; Krammer, B.; Plaetzer, K. Cellular mechanisms and prospective applications of hypericin in photodynamic therapy. Curr. Med. Chem. 2006, 13, 2189–2204. [Google Scholar] [CrossRef] [PubMed]
- Sanovic, R.; Verwanger, T.; Hartl, A.; Krammer, B. Low dose hypericin-PDT induces complete tumor regression in BALB/c mice bearing CT26 colon carcinoma. Photodiagn. Photodyn. Ther. 2011, 8, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Wölfle, U.; Seelinger, G.; Schempp, C.M. Topical application of St. John’s wort (Hypericum perforatum). Planta Med. 2014, 80, 109–120. [Google Scholar] [CrossRef] [PubMed]
- Ng, Q.X.; Venkatanarayanan, N.; Ho, C.Y. Clinical use of Hypericum perforatum (St John’s wort) in depression: A meta-analysis. J. Affect. Disord. 2017, 210, 211–221. [Google Scholar] [CrossRef]
- Allison, R.R.; Moghissi, K. Photodynamic therapy (PDT): PDT mechanisms. Clin. Endosc. 2013, 46, 24–29. [Google Scholar] [CrossRef]
- Plaetzer, K.; Krammer, B.; Berlanda, J.; Berr, F.; Kiesslich, T. Photophysics and photochemistry of photodynamic therapy: Fundamental aspects. Lasers Med. Sci. 2009, 24, 259–268. [Google Scholar] [CrossRef]
- Kwiatkowski, S.; Knap, B.; Przystupski, D.; Saczko, J.; Kędzierska, E.; Knap-Czop, K.; Kotlińska, J.; Michel, O.; Kotowski, K.; Kulbacka, J. Photodynamic therapy—Mechanisms, photosensitizers and combinations. Biomed. Pharmacother. 2018, 106, 1098–1107. [Google Scholar] [CrossRef] [PubMed]
- Agostinis, P.; Berg, K.; Cengel, K.A.; Foster, T.H.; Girotti, A.W.; Gollnick, S.O.; Hahn, S.M.; Hamblin, M.R.; Juzeniene, A.; Kessel, D.; et al. Photodynamic therapy of cancer: An update. CA Cancer J. Clin. 2011, 61, 250–281. [Google Scholar] [CrossRef] [PubMed]
- Wachowska, M.; Muchowicz, A.; Demkow, U. Immunological aspects of antitumor photodynamic therapy outcome. Cent. Eur. J. Immunol. 2015, 40, 481–485. [Google Scholar] [CrossRef] [PubMed]
- Oniszczuk, A.; Wojtunik-Kulesza, K.A.; Oniszczuk, T.; Kasprzak, K. The potential of photodynamic therapy (PDT)-Experimental investigations and clinical use. Biomed. Pharmacother. 2016, 83, 912–929. [Google Scholar] [CrossRef]
- Reginato, E.; Wolf, P.; Hamblin, M.R. Immune response after photodynamic therapy increases anti-cancer and anti-bacterial effects. World J. Immunol. 2014, 4, 1–11. [Google Scholar] [CrossRef]
- Dougherty, T.J.; Gomer, C.J.; Henderson, B.W.; Jori, G.; Kessel, D.; Korbelik, M.; Moan, J.; Peng, Q. Photodynamic therapy. J. Natl. Cancer Inst. 1998, 90, 889–905. [Google Scholar] [CrossRef]
- Allison, R.R.; Moghissi, K. Oncologic photodynamic therapy: Clinical strategies that modulate mechanisms of action. Photodiagn. Photodyn. Ther. 2013, 10, 331–341. [Google Scholar] [CrossRef] [PubMed]
- Yang, D.; Lei, S.; Pan, K.; Chen, T.; Lin, J.; Ni, G.; Liu, J.; Zeng, X.; Chen, Q.; Dan, H. Application of photodynamic therapy in immune-related diseases. Photodiagn. Photodyn. Ther. 2021, 34, 102318. [Google Scholar] [CrossRef]
- Sitnik, T.M.; Hampton, J.A.; Henderson, B.W. Reduction of tumour oxygenation during and after photodynamic therapy in vivo: Effects of fluence rate. Br. J. Cancer 1998, 77, 1386–1394. [Google Scholar] [CrossRef]
- Dong, X.; Zeng, Y.; Zhang, Z.; Fu, J.; You, L.; He, Y.; Hao, Y.; Gu, Z.; Yu, Z.; Qu, C.; et al. Hypericin-mediated photodynamic therapy for the treatment of cancer: A review. J. Pharm. Pharmacol. 2021, 73, 425–436. [Google Scholar] [CrossRef]
- Saw, C.L.; Heng, P.W.; Olivo, M. Potentiation of the photodynamic action of hypericin. J. Environ. Pathol. Toxicol. Oncol. 2008, 27, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, T.; Ohta, N.; Yamazaki, I.; Song, P.S. Excited-state properties of hypericin: Electronic spectra and fluorescence decay kinetics. J. Phys. Chem. 1993, 97, 7870–7875. [Google Scholar] [CrossRef]
- Kubin, A.; Wierrani, F.; Burner, U.; Alth, G.; Grünberger, W. Hypericin--the facts about a controversial agent. Curr. Pharm. Des. 2005, 11, 233–253. [Google Scholar] [CrossRef] [PubMed]
- Ehrenberg, B.; Anderson, J.L.; Foote, C.S. Kinetics and yield of singlet oxygen photosensitized by hypericin in organic and biological media. Photochem. Photobiol. 1998, 68, 135–140. [Google Scholar] [CrossRef]
- Koren, H.; Schenk, G.M.; Iindra, R.H.; Alth, G.; Ebermann, R.; Kubin, A.; Koderhold, G.; Kreitner, M. Hypericin in phototherapy. J. Photochem. Photobiol. B Biol. 1996, 36, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Alecu, M.; Ursaciuc, C.; Hãlãlãu, F.; Coman, G.; Merlevede, W.; Waelkens, E.; de Witte, P. Photodynamic treatment of basal cell carcinoma and squamous cell carcinoma with hypericin. Anticancer Res. 1998, 18, 4651–4654. [Google Scholar]
- Sharman, W.M.; Allen, C.M.; van Lier, J.E. Photodynamic therapeutics: Basic principles and clinical applications. Drug Discov. Today 1999, 4, 507–517. [Google Scholar] [CrossRef]
- Lavie, G.; Meruelo, D.; Aroyo, K.; Mandel, M. Inhibition of the CD8+ T cell-mediated cytotoxicity reaction by hypericin: Potential for treatment of T cell-mediated diseases. Int. Immunol. 2000, 12, 479–486. [Google Scholar] [CrossRef]
- Dirschka, T.; Radny, P.; Dominicus, R.; Mensing, H.; Brüning, H.; Jenne, L.; Karl, L.; Sebastian, M.; Oster-Schmidt, C.; Klövekorn, W.; et al. Photodynamic therapy with BF-200 ALA for the treatment of actinic keratosis: Results of a multicentre, randomized, observer-blind phase III study in comparison with a registered methyl-5-aminolaevulinate cream and placebo. Br. J. Dermatol. 2012, 166, 137–146. [Google Scholar] [CrossRef]
- Kim, E.J.; Mangold, A.R.; DeSimone, J.A.; Wong, H.K.; Seminario-Vidal, L.; Guitart, J.; Appel, J.; Geskin, L.; Lain, E.; Korman, N.J.; et al. Efficacy and safety of topical hypericin photodynamic therapy for early-stage cutaneous T-cell Llymphoma (Mycosis fungoides): The FLASH phase 3 randomized clinical trial. JAMA Dermatol. 2022, 158, 1031–1039. [Google Scholar] [CrossRef]
- Liu, W.T.; Wang, H.T.; Yeh, Y.H.; Wong, T.W. An update on recent advances of photodynamic therapy for primary cutaneous lymphomas. Pharmaceutics 2023, 15, 1328. [Google Scholar] [CrossRef]
- Rook, A.H.; Wood, G.S.; Duvic, M.; Vonderheid, E.C.; Tobia, A.; Cabana, B. A phase II placebo-controlled study of photodynamic therapy with topical hypericin and visible light irradiation in the treatment of cutaneous T-cell lymphoma and psoriasis. J. Am. Acad. Dermatol. 2010, 63, 984–990. [Google Scholar] [CrossRef]
- Conrado, P.C.V.; Vaine, A.A.; Arita, G.S.; Sakita, K.M.; Gonçalves, R.S.; Caetano, W.; de Souza, M.; Baesso, M.L.; Malacarne, L.C.; Razzolini, E.; et al. Promising onychomycosis treatment with hypericin-mediated photodynamic therapy: Case reports. Photodiagn. Photodyn. Ther. 2023, 42, 103498. [Google Scholar] [CrossRef]
- Galinari, C.B.; Biachi, T.P.; Gonçalves, R.S.; Cesar, G.B.; Bergmann, E.V.; Malacarne, L.C.; Kioshima Cotica, É.; Bonfim-Mendonça, P.S.; Svidzinski, T.I.E. Photoactivity of hypericin: From natural product to antifungal application. Crit. Rev. Microbiol. 2023, 49, 38–56. [Google Scholar] [CrossRef]
- Choi, Y.M.; Adelzadeh, L.; Wu, J.J. Photodynamic therapy for psoriasis. J. Dermatol. Treat. 2015, 26, 202–207. [Google Scholar] [CrossRef]
- Marek-Jozefowicz, L.; Nedoszytko, B.; Grochocka, M.; Żmijewski, M.A.; Czajkowski, R.; Cubała, W.J.; Slominski, A.T. Molecular mechanisms of neurogenic inflammation of the skin. Int. J. Mol. Sci. 2023, 24, 5001. [Google Scholar] [CrossRef]
- Morgner, B.; Tittelbach, J.; Wiegand, C. Induction of psoriasis- and atopic dermatitis-like phenotypes in 3D skin equivalents with a fibroblast-derived matrix. Sci. Rep. 2023, 13, 1807. [Google Scholar] [CrossRef]
- Su, Z.; Zeng, Y.P. Dupilumab-associated psoriasis and psoriasiform manifestations: A scoping review. Dermatology 2023, 239, 646–657. [Google Scholar] [CrossRef]
- Navarro-Triviño, F.; Alcantara-Luna, S.; Domínguez-Cruz, J.; Galán-Gutiérrez, M.; Ruiz-Villaverde, R.; Pereyra-Rodriguez, J.J.; Armario-Hita, J.C. Upadacitinib for moderate to severe atopic dermatitis. Immunotherapy 2023, 15, 799–808. [Google Scholar] [CrossRef]
- Turchin, I.; Bourcier, M. The role of interleukins in the pathogenesis of dermatological immune-mediated diseases. Adv. Ther. 2022, 39, 4474–4508. [Google Scholar] [CrossRef]
- Rathod, D.G.; Muneer, H.; Masood, S. Phototherapy. In StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2024. [Google Scholar]
- Kurz, B.; Berneburg, M.; Bäumler, W.; Karrer, S. Phototherapy: Theory and practice. J. Dtsch. Dermatol. Ges. 2023, 21, 882–897. [Google Scholar] [CrossRef]
- Ding, Y.N.; Ding, H.Y.; Li, H.; Yang, R.; Huang, J.Y.; Chen, H.; Wang, L.H.; Wang, Y.J.; Hu, C.M.; An, Y.L.; et al. Photosensitive small extracellular vesicles regulate the immune microenvironment of triple negative breast cancer. Acta Biomater. 2023, 167, 534–550. [Google Scholar] [CrossRef]
- Grundmann, S.A.; Beissert, S. Modern aspects of phototherapy for atopic dermatitis. J. Allergy 2012, 2012, 121797. [Google Scholar] [CrossRef]
- Ruscitti, P.; Esposito, M.; Di Cola, I.; Pellegrini, C.; De Berardinis, A.; Mastrangelo, M.; Gianneramo, C.; Barile, A.; Fargnoli, M.C.; Cipriani, P. Cytokine profile characterization of naïve patients with psoriasis and psoriatic arthritis: Implications for a pathogenic disease continuum. Front. Immunol. 2023, 14, 1229516. [Google Scholar] [CrossRef]
- Numerof, R.P.; Asadullah, K. Cytokine and anti-cytokine therapies for psoriasis and atopic dermatitis. BioDrugs 2006, 20, 93–103. [Google Scholar] [CrossRef]
- Woźniak, M.; Nowak-Perlak, M. Hypericin-based photodynamic therapy displays higher selectivity and phototoxicity towards melanoma and squamous cell cancer compared to normal keratinocytes in vitro. Int. J. Mol. Sci. 2023, 24, 16897. [Google Scholar] [CrossRef]
- Popovic, A.; Wiggins, T.; Davids, L.M. Differential susceptibility of primary cultured human skin cells to hypericin PDT in an in vitro model. J. Photochem. Photobiol. B 2015, 149, 249–256. [Google Scholar] [CrossRef]
- Zhang, Y.; Su, J. Interleukin-2 family cytokines: An overview of genes, expression, signaling and functional roles in teleost. Dev. Comp. Immunol. 2023, 141, 104645. [Google Scholar] [CrossRef]
- Yuan, Y.; Kolios, A.G.A.; Liu, Y.; Zhang, B.; Li, H.; Tsokos, G.C.; Zhang, X. Therapeutic potential of interleukin-2 in autoimmune diseases. Trends Mol. Med. 2022, 28, 596–612. [Google Scholar] [CrossRef]
- Matsushima, K.; Shichino, S.; Ueha, S. Thirty-five years since the discovery of chemotactic cytokines, interleukin-8 and MCAF: A historical overview. Proc. Jpn. Acad. Ser. B Phys. Biol. Sci. 2023, 99, 213–226. [Google Scholar] [CrossRef]
- Larisch, P.; Verwanger, T.; Linecker, M.; Krammer, B. The interrelation between a pro-inflammatory milieu and fluorescence diagnosis or photodynamic therapy of human skin cell lines. Photodiagn. Photodyn. Ther. 2014, 11, 91–103. [Google Scholar] [CrossRef] [PubMed]
- Safarini, O.A.; Keshavamurthy, C.; Patel, P. Calcineurin inhibitors. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Ke, Y.; Li, B.Z.; Nguyen, K.; Wang, D.; Wang, S.; Young, C.D.; Wang, X.J. IL-22RA2 Is a SMAD7 target mediating the alleviation of dermatitis and psoriatic phenotypes in mice. J. Investig. Dermatol. 2023, 143, 2243–2254.e2210. [Google Scholar] [CrossRef] [PubMed]
- Wölfle, U.; Haarhaus, B.; Schempp, C.M. Amarogentin displays immunomodulatory Effects in Human Mast Cells and Keratinocytes. Mediat. Inflamm. 2015, 2015, 630128. [Google Scholar] [CrossRef] [PubMed]
- Steadman, T.; O’Reilly, S. Elevated interleukin-11 in systemic sclerosis and role in disease pathogenesis. J. Dermatol. 2023, 50, 1255–1261. [Google Scholar] [CrossRef] [PubMed]
- O’Reilly, S. Interleukin-11 and its eminent role in tissue fibrosis: A possible therapeutic target. Clin. Exp. Immunol. 2023, 214, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Keskin, E.S.; Keskin, E.R.; Öztürk, M.B.; Çakan, D. The effect of MMP-1 on wound healing and scar formation. Aesthetic Plast. Surg. 2021, 45, 2973–2979. [Google Scholar] [CrossRef] [PubMed]
- Oka, T.; Sugaya, M.; Takahashi, N.; Nakajima, R.; Otobe, S.; Kabasawa, M.; Suga, H.; Miyagaki, T.; Asano, Y.; Sato, S. Increased interleukin-19 expression in cutaneous T-cell lymphoma and atopic dermatitis. Acta Derm.-Venereol. 2017, 97, 1172–1177. [Google Scholar] [CrossRef] [PubMed]
- Ge, G.; Shang, J.; Gan, T.; Chen, Z.; Pan, C.; Mei, Y.; Long, S.; Wu, A.; Wang, H. Psoriasis and leprosy: An arcane relationship. J. Inflamm. Res. 2023, 16, 2521–2533. [Google Scholar] [CrossRef]
- Krupka-Olek, M.; Bożek, A.; Kawczyk-Krupka, A. The immunological and allergen profiles of patients with atopic dermatitis or psoriasis. Medicina 2022, 58, 367. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krupka-Olek, M.; Bożek, A.; Czuba, Z.P.; Kłósek, M.; Cieślar, G.; Kawczyk-Krupka, A. Cytotoxic and Immunomodulatory Effects of Hypericin as a Photosensitizer in Photodynamic Therapy Used on Skin Cell Cultures. Pharmaceutics 2024, 16, 696. https://doi.org/10.3390/pharmaceutics16060696
Krupka-Olek M, Bożek A, Czuba ZP, Kłósek M, Cieślar G, Kawczyk-Krupka A. Cytotoxic and Immunomodulatory Effects of Hypericin as a Photosensitizer in Photodynamic Therapy Used on Skin Cell Cultures. Pharmaceutics. 2024; 16(6):696. https://doi.org/10.3390/pharmaceutics16060696
Chicago/Turabian StyleKrupka-Olek, Magdalena, Andrzej Bożek, Zenon P. Czuba, Małgorzata Kłósek, Grzegorz Cieślar, and Aleksandra Kawczyk-Krupka. 2024. "Cytotoxic and Immunomodulatory Effects of Hypericin as a Photosensitizer in Photodynamic Therapy Used on Skin Cell Cultures" Pharmaceutics 16, no. 6: 696. https://doi.org/10.3390/pharmaceutics16060696
APA StyleKrupka-Olek, M., Bożek, A., Czuba, Z. P., Kłósek, M., Cieślar, G., & Kawczyk-Krupka, A. (2024). Cytotoxic and Immunomodulatory Effects of Hypericin as a Photosensitizer in Photodynamic Therapy Used on Skin Cell Cultures. Pharmaceutics, 16(6), 696. https://doi.org/10.3390/pharmaceutics16060696